Embed Size (px)
Citation preview
Amie Martin OTR/L
PRACTICAL SOLUTIONS TO
REHAB DEMENTIA CARE PART 1
PROMOTING EACH PERSON’S BEST ABILITY TO FUNCTION
Intro to the cognitive disabilities model of care
The Dementia Problem
Aging population
Growing need for dementia care
Efficient, practical & compassionate service is more important than ever before
Age related changes impacting function
Physical changes in strength,
coordination, energy levels
Digestive and excretory system changes
Medications may have side effects that impact appetite, alertness, or physical functioning
Immune system changes
Chronic Pain
Sensory loss
Sleep problems
MORE Difficulties In Dementia
Decreased attention/concentration to complete a task. Easily distracted.
Reduced hunger/thirst awareness, dysphagia, aversion to textures
Disorientation to time, spatial awareness
Reduced ability to communicate
Intolerance to excessive stimulation
Confusion about what is expected
Inability to sequence through multiple steps
Feelings of loss (of self, of the familiar, of security…)
Who is at risk?
Any patient with a condition : • That impacts blood flow
• That effects glucose levels
• That reduces oxygen levels
• That requires multiple medications
• That effects nutrient absorption
• That causes sleep impairment
• That leads to chronic pain
• That is accompanied by depression
Vascular Dementia
Represents 20% of dementia cases
Characterized by neurological signs and
systematic progression of symptoms
Early gait changes
Risk factors are HTN and CAD
“An Interdisciplinary Dementia Program Model for Long Term Care,” Kim Warhol, OTR/L, Topics in Geriatric Rehabilitation Vol20, No.1, pp.59-71 2005 Lippincott Williams & Wilkins, Inc.
Amie Martin OTR/L
Dementia with Lewy Bodies
Accounts for 20% of dementia cases
Early signs are not memory problems, but
difficulties with attention, logic, time, and
spatial thinking.
Often show fluctuations in cognition not
seen in other types
Characterized in first year by
parkinsonian movement, visual
hallucinations, and early gait changes.
“An Interdisciplinary Dementia Program Model for Long Term Care,” Kim Warhol, OTR/L, Topics in Geriatric Rehabilitation Vol20, No.1, pp.59-71 2005 Lippincott Williams & Wilkins, Inc.
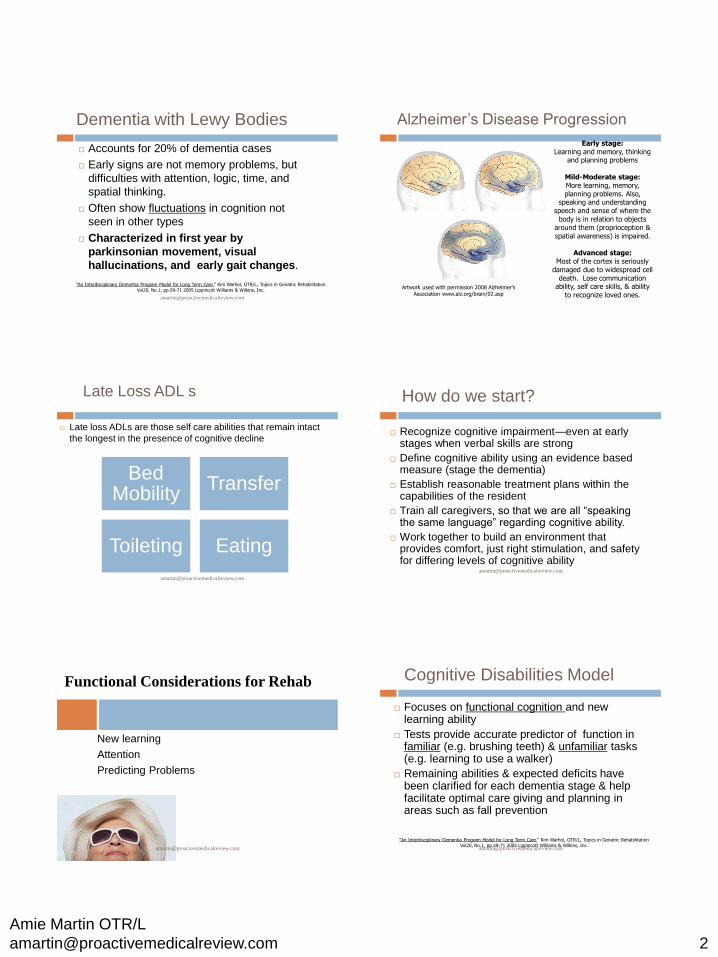
Alzheimer’s Disease Progression
Early stage: Learning and memory, thinking
and planning problems
Mild-Moderate stage: More learning, memory, planning problems. Also,
speaking and understanding speech and sense of where the
body is in relation to objects around them (proprioception & spatial awareness) is impaired.
Advanced stage:
Most of the cortex is seriously damaged due to widespread cell
death. Lose communication ability, self care skills, & ability
to recognize loved ones. Artwork used with permission 2008 Alzheimer’s
Association www.alz.org/brain/02.asp
Late Loss ADL s
Late loss ADLs are those self care abilities that remain intact
the longest in the presence of cognitive decline
Bed Mobility
Transfer
Toileting Eating
How do we start?
Recognize cognitive impairment—even at early stages when verbal skills are strong
Define cognitive ability using an evidence based measure (stage the dementia)
Establish reasonable treatment plans within the capabilities of the resident
Train all caregivers, so that we are all “speaking the same language” regarding cognitive ability.
Work together to build an environment that provides comfort, just right stimulation, and safety for differing levels of cognitive ability
Functional Considerations for Rehab
New learning
Attention
Predicting Problems
Cognitive Disabilities Model
Focuses on functional cognition and new learning ability
Tests provide accurate predictor of function in familiar (e.g. brushing teeth) & unfamiliar tasks (e.g. learning to use a walker)
Remaining abilities & expected deficits have been clarified for each dementia stage & help facilitate optimal care giving and planning in areas such as fall prevention
“An Interdisciplinary Dementia Program Model for Long Term Care,” Kim Warhol, OTR/L, Topics in Geriatric Rehabilitation Vol20, No.1, pp.59-71 2005 Lippincott Williams & Wilkins, Inc.
Amie Martin OTR/L
What is the ACLS and RTI?
ACL=Allen Cognitive Level Screen
Presenting an unfamiliar task to determine how the resident problem solves and follows directions
RTI=Routine Task Inventory
Categorizes ADL performance based on caregiver
observation of routine activities.
These tests are based on the research of Claudia Allen & colleagues that has been ongoing since the early 1970s. Studies support the use of these tools to measure cognitive change, analyze activity performance, and develop reasonable treatment goals that promote meaningful activity within the patient’s capacity to function.
Abilities are analyzed based on:
What they will pay attention to
Motor control expectations
Communication ability
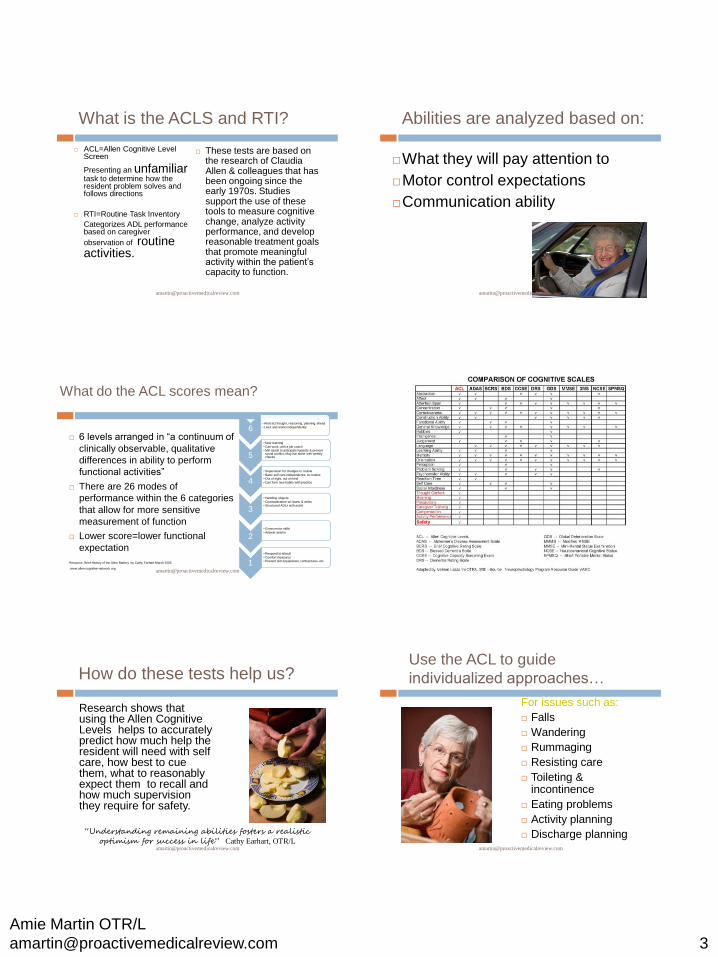
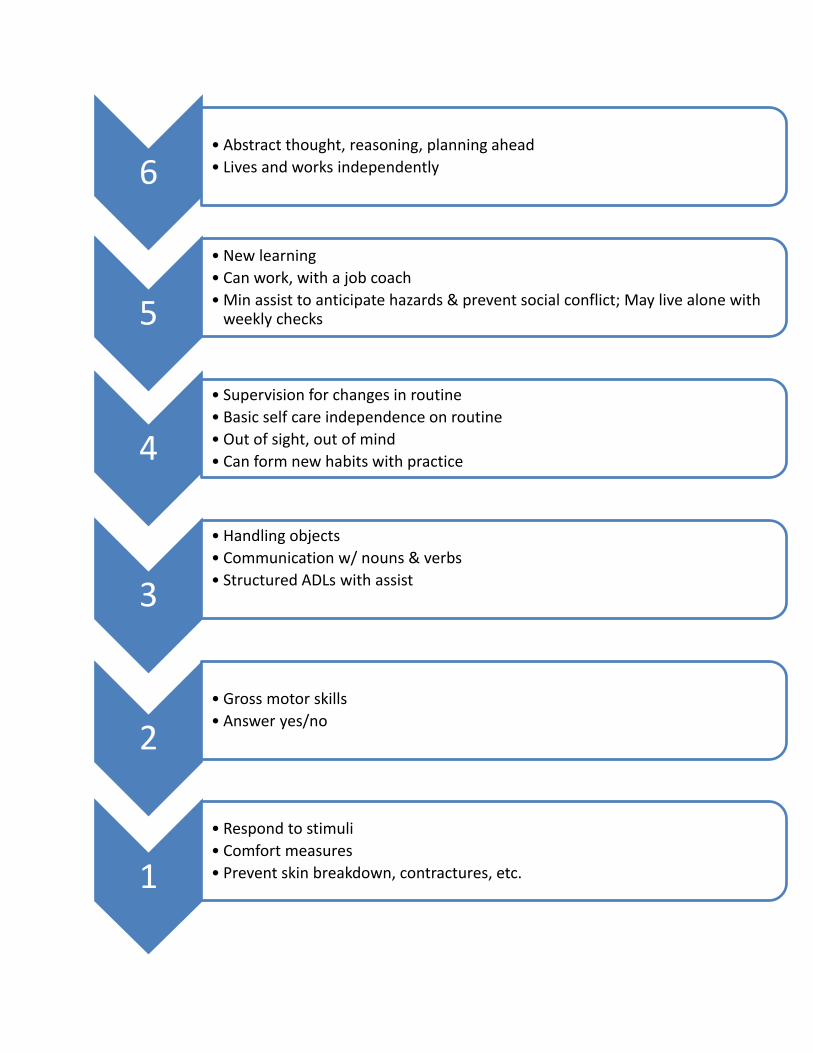
What do the ACL scores mean?
6 levels arranged in “a continuum of
clinically observable, qualitative
differences in ability to perform
functional activities”
There are 26 modes of
performance within the 6 categories
that allow for more sensitive
measurement of function
Lower score=lower functional
expectation
Resource: Brief History of the Allen Battery by Cathy Earhart March 2005
www.allen-cognitive-network.org
6 • Abstract thought, reasoning, planning ahead
• Lives and works independently
5
• New learning
• Can work, with a job coach • Min assist to anticipate hazards & prevent social conflict; May live alone with weekly checks
4
• Supervision for changes in routine
• Basic self care independence on routine • Out of sight, out of mind
• Can form new habits with practice
3
• Handling objects
• Communication w/ nouns & verbs • Structured ADLs with assist
2 • Gross motor skills
• Answer yes/no
1
• Respond to stimuli
• Comfort measures • Prevent skin breakdown, contractures, etc.
How do these tests help us?
Research shows that using the Allen Cognitive Levels helps to accurately predict how much help the resident will need with self care, how best to cue them, what to reasonably expect them to recall and how much supervision they require for safety.
“Understanding remaining abilities fosters a realistic
optimism for success in life” Cathy Earhart, OTR/L [email protected]
Use the ACL to guide
individualized approaches…
For issues such as:
Falls
Wandering
Rummaging
Resisting care
Toileting & incontinence
Eating problems
Activity planning
Discharge planning
Amie Martin OTR/L
Provide “just right” structure
Activities that are age
appropriate and individualized
based on abilities, interests,
and needs
Environment & interaction
that reduces anxiety, allows
residents to maintain control
in areas that they can
Structure without sameness
or lack of purpose in their day
Steps to achieve this goal
Use an objective means of
identifying remaining
cognitive ability and self
care potential
Train staff on how to offer
the “just right challenge” for
each resident in our care
How about some examples…
2.4 will walk aimlessly/wander avoiding barriers
that are above the knee, but may trip over
something left on the floor
Resists confinement. Tries to escape.
Eats and drinks with set up and mod assist to
initiate / sustain actions. Needs 2-3xs the usual
time to eat.
2.6 may disrobe if uncomfortable in clothes
Level 3 Examples
3.0 may need you to put the washcloth or fork in
their hand to remind them to start the task. May try
to climb over side rails in bed or need you to
actively encourage them to rest if they pace the
halls. May need extra time to adjust from sitting to
standing. May clog up the toilet using too much
toilet paper.
Level 4 examples
4.4 may be left alone for part of the day with someone to remove safety hazards and solve minor problems AND a procedure for calling help if needed
Will pay attention to the environment 3-4 feet around them
May initiate coming to the table at routine times or make self a sandwich. May not be able to eat and converse at the same time. May recognize well learned special diets.
4.6 may live alone with daily checks and help with bills and housework.
Amie Martin OTR/L
Care is more compassionate!
We do not set goals higher than the
resident can reasonably attain
Care is more individualized!
We can offer the types of activities that
residents will predictably enjoy
Care involves less trial & error!
We can communicate in
ways residents will best
understand
We can reduce behaviors
by offering appropriate
challenges & stimulation
opportunities
Care is more efficient!
We have a functional means of communicating across caregivers the level of care required
We can coordinate the activity calendar based on the cognitive levels represented
Changes in cognitive function can be objectively measured &
documented
Putting it all together
Lets review a sample
patient program
Case Study 1: Fred
92 y/o with frequent falls at home where he was
ambulatory in the house without AD.
History of dementia, Parkinson’s, arthritis, chronic
back pain, depression. New admit from home.
Interventions:
PT/OT with cognitive screening and fall risk assessment.
ACLS/RTI score: 3.8
OT: cognitive assessment, ADL program with consistent routine, bathroom transfers, environmental modification (grab bar, raised toilet,) activities program guidance, staff education
PT: assess & grade personal fall risk factors, balance activities, strengthening, back pain management, transfer training with walker, posture, restorative exercise & walk to dine program
Amie Martin OTR/L
Other Interventions for Fred
Develop routine: In 3 weeks, finds way to & from DR and begins walk to dine program.
Performs basic ADLs with prompts to start and items set up in plain site and in order to be
used/put on. Plan for slow pace and cues to “keep going.“
Activities should be structured throughout the day to provide a calm yet sensory rich environment and avoid excessive “sitting.” Often enjoys meaningful music from own era, seated stretching and exercise, walks, people watching, repetitive tasks (polishing, sanding, folding, sorting) and basic crafts
Scheduled toileting: Toilets with SBA for the transfer and occasional cues for thorough
hygiene. He may not ask for help if he needs to go between scheduled times.
Safety: Does not consistently “remember” safety precautions for transfers, but after
consistent drilling of proper walker use has formed a new motor habit over time. Provide
consistent task order and the same simple cues across caregivers to reinforce safe
transitional movements/transfers/ambulation.
Environment: Nightlights, no bed rails, tub seat, removal of items from floor, removal of
unstable furniture due to tendency to furniture walk
Finding the individual’s
“Just Right Challenge”
Therapy referral from nursing based on a change in condition or identified deficit
Therapy evaluation, objective cognitive assessment, and treatment plan based on findings
Individualized FMP or restorative program development with staff training on recommendations and cognitive level findings
Nursing/restorative follows through with FMP or restorative program and consults with therapy if changes in the program are needed prior to the quarterly screening
Intervention Cycle
Change in Status/Skilled
Need
Rehab Intervention
FMP/RNP referral
Maintenance Program
Quarterly Screens
Proactive Medical Review & Consulting, LLC
Join us for the next sessions:
Session 2: April 9 (Assessment)
April 10-15 Complete self study lab practice of assessments with
online videos
Session 3 : April 16 (Application in treatment)
Session 4: April 23 (Interventions) Certificates will be issued after session 4 with cumulative hours of
sessions attended. All sessions will be recorded. Contact Holly at HTS
regarding accessing recorded sessions.
6 • Abstract thought, reasoning, planning ahead
• Lives and works independently
5
• New learning
• Can work, with a job coach
• Min assist to anticipate hazards & prevent social conflict; May live alone with weekly checks
4
• Supervision for changes in routine
• Basic self care independence on routine
• Out of sight, out of mind
• Can form new habits with practice
3
• Handling objects
• Communication w/ nouns & verbs
• Structured ADLs with assist
2 • Gross motor skills
• Answer yes/no
1
• Respond to stimuli
• Comfort measures
• Prevent skin breakdown, contractures, etc.

![N RESERVOIR - Luray Caverns Airport · 896 894 892 892 892 894 896 899 900 900 899 901 899 power dam road future relocated state route 652 [ i ] proposed papi (2l) [ i ] (4l) [u]](https://img.pdfslide.us/doc/110x75/5ac1d2de7f8b9a357e8d23bd/n-reservoir-luray-caverns-894-892-892-892-894-896-899-900-900-899-901-899-power.jpg)

















![Curso Assembler Pic 892[1]](https://img.pdfslide.us/doc/110x75/544ed1c6af7959d91e8b4cd9/curso-assembler-pic-8921.jpg)