Embed Size (px)
Citation preview

Afa0010
7'ý AIDA 1 6 SCAO-AN
.0-4
IL Reproduced FromBest Available Copy ~
,Do9oW4Q 6

Research Issues inSimulator Sickness:Proceedings of a Workshop
Michael E. McCauley, EditorCommittee on Human FactorsCommission on Behavioral and Social Sciences and EducationNational Research Council
NATIONAL ACADEMY PRESSWashington. D.C. 1984

NOTTCE: The project that is the subject of this report wasapproved by the Governing board of the National ResearchCouncil, whose members are drawn from the councils of theNational Academy of Sciences, the National Academy ofEngineering, and th% Institute uf Medicine. The members of thecommittee responsible for the report werc chosen for theirspecial competence@ and with resard for appropriate balance.
This report has been reviewed by a group other than theauthors according to proccdures approved by a Report ReviewCommit-ee consisting of members of the National Academy ofSciences, the National Academ, of gngineering, and the Instituteof Medicine.
The National Research Council was established by the NationalAcademy of Sciences in 19l6 to associate the broad community ofscience and technology with the Academy's purposes of furtherintiknowledge ind of advising the federal government. The Counciloperates in accordance with general policies determined by theAcademy under tne authority of its congressional charter of1863, wt-ich establishes the Academy as a private, nonprofit,self-governing membership corporation. The Council has become
, the principal operating agency of both the National Academy ofSciences and the National Academy of Engineering in the conductof their services to the government, the public, and thescientific and engineering communities. It is administeredjointly by both Academies and the Institute of Medicine. TheNational Academy of Engineering and the Institute of Medicinewere established in 1964 and 1970, respectively, under thecharter of the National Academy of Sciences.
The Committee on Human Factors in the Commission on Behavioral
and Social Sciencus and Edication is sponsored jointly by theAir Force Office of Scientific Research, the Army ResearchInstitute for the Behavioral and :ocial 3ciences, the Office ofNaval Research, the National Aeronautics anI SpaceAdministration, and the National Science Foundation.
This work relat,'s to Department of the navy ContractN00014-81-C-0017 issued by *he Office of Naval Research underContract Authority NR 196-167. However, the content does notnecessarily reflect the position or the policy of thegovernment, and no official endorsement saiould be inferred.
The United States government has at lsast a royalty-free.notoexclusive and irrevo.able license thro ghout the wcrld forgovernment purposes to publish, translates reproduce, deliver,perform, dispose of, and to authorize others so to do, all or
any portion of this work.
Is a o i Ht 0 i

I
WORKSHOP ON SIMULATOR SICKNESS
HERSCHEL W. LEIBOWITZ (Chair), Department of Psychology,Pennsylvanii State University
ALAN J. BENSON, Royal Air Force Institute of AviationMedicine, Farnborough, Hants, U.K.
JOHN G. CASALI, Vehicle Simulation Laboratory, VirginiaPolytechnic Institite and State University
MALCOLM H. COHEN, Biomedical Research Division, NASAAmes Research Center, Moffet Field, Calif.
SHELDON H. EBENHOLTZ, Department of Psychology.University of Wisconsin
LAWRENCE H. FRANK, Naval Training Equipment Center.Orlando, Fla.
KENT GILLINGHAM, USAF SA/IVNB, Brooks Air Force Base,Tex.
FREDERICK Z. GUEDRY, Naval Aerospace Medical ResearchLaboratory, Pensacola, Fla.
CHARLES W. HUTCWiINS, U.S. Naval Postgraduate School,Monterey, Calif.
ROBERT S. KELLOGG, University of Dayton ResearchInstitute, Williams Air Force Base, Ariz.
ROBERT S. KENNEDY, Essex Corporation, Orlando, Fla.JAMES 1. LACKNER, Department of Psychology, Brandeis
University
MICHAEL Z. McCAULEY, Monterey Technologies, Inc.,Carmel, Calif.
GRANT B. McNAUGHTON, Norton Air Force Base, Calif.KEN 9. MONEY, Defense and Civil Institute of
Environmental Medicine, Downsviev, Ont.ROBERT POST, Department of Psychology, University of
California, Davis
i i | l i .

JOHN D. SINACORI, John R. Sinscori Associate3, Nonttrey,Calif.
EDWARD A. STARK, Link Flight/Simulator Divisiou, SingerCompany, Binghamton, N.Y.
DANIEL J. WEINTRJAUB, Human Periormance Center.University of Michigae
ROBERT H. WRI•HT, U.S. Army Raeee-ch Institute, FortRucker, Ala.
ROBERT T. HENNESSY, Workshop OrganizerJEANNE RICHARDS, Administrao,.ve Secretary
Acoession For
fNTIS G.A&IDTIC T'.F flUnanu.w-.nced e0Jit i.icrl........
Di striut ion/
Availabtility CodoeAv'ill and/or
Dist
iv

CO:!MITTEE ON HUM1AN FACIO.S
RICH1ARD W. PEW (Chair), Bolt Beranek & Newman Inc.,Cambridge, Ma33.
NA:CY S. ANDERSON, Department of Psychology, Universityof Maryland
ALP11C:SE CHAPANIS, Communications Research, Inc.,Ealtimore, Md.
BARUCH FISCHROFF, Decision Research (a branch ofPerceptronics, Inc.), Eugene, Ore.
IRWIN L. GOLDSTEIN, Department of Psychology, Universityof Maryland
JULIAN HOCHBERG, Department of Psychology, ColumbiaUniversity
K.H. EBERHARD KROEN1ER, Ergonomics Laboratory, VirginiaPolytechnic Institute and State University
TUCIAS K. LA11DAUER, Bell Laboratories, Murray Hill, N.J.JUDITA R*.IT'iA1 OLSON, School of Business Administration,
University of MichiganTk1,'uIS h. SHERIDAN, Department of Mechanical Engineering,
",laoaachusetts Institute of TechnologyROBERT C. WILLIGES, Department of Industrial Engineering
and Operations R,.search, Virginia PolytechnicInstitute and State University
STANLEY DEUTSCH, Study DirectorJEANKIIE RICiL%\RDS, Administrative Secretary
S...... .. V

CONTENTS
PREFACE xi
INTRODUCTION
INCIDENCE AND PREVALENCE 4
S IMULATOR CHARACTERISTICS
Visual Systems, 8Lags, 10Motion Systems, 12Other Motion Cueing Devices, 15Comment on Visual and Motion Systens, 15Designing a Flight Simulator, 16Design Characteristics of Automobile
Simulators, 19
THEORIES OF MOTION SICKNESS AND ADAPTATION 22
Sensory Conflict Theory, 25Adaptation Studies, 30Oculomotor Adaptive Systems, 33Comments on Theories of Motion Sickness, 41
RECOMMENDED COUNTERMEASURES FOR EXISTING SIMULATORS 43
It
vii
•nn n

RECO••ENDATIONS FOR RESEARCH 48
Problem Definition, 48
Theory/Model Development, 49Methodology, 50Determination of Causes and Processes, 51Evaluation of Candidate Countermeasures, 53
APPENDIX: POTENTIAL CONTRIBUTORS TO SIMULATORSICKNESS 55
REFERENCES 59
viii

TABLES AND FIGURES
Table I Major Studies of Simulator Sickness 5Table 2 Types of Sensory Conflict 31Table 3 Recommended Countermeasures for Current
Simulators 44
Figure I A Comparison Between MIL-STD 1472CVomiting Criteria and a ProjectedEnvelope for Lesser Symptomatology 14
Figure 2 Cross-Coupled Semicircular CanalStimuli 29
Figure 3 Etiology of Uotion Sickness 30Figure 4 Vergence and Accommodation Control
Systems 36Figure 5 Vector Analysis of the Conditions
Productive of Increased Gain, Reversed
Gain, and Directional Shifts in theVestibular-Ocular Reflex 38
ix

PREFACE
The Committee on Human Factors was established in
October 1980 by the Commission on Behavioral and SocialSciences and Education of the National Research Council
in response to a request by the Office of Naval Research,the Air Force Office of Scientific Researchland theArmy Research Institute for the Behavioral and SocialSciences. In addition, its sponsors currently includethe National Aeronautics and Space Administration andthe Nation&l Science Foundation. The committee'sobjectives are to provide new perspectives ontheoretical and methodological issues, identify basicresearch needed to expand and strengthen the'scientificbasis of human factors, and to attract scientists bothwithin and outside the field to perform the neoededresearch. Its overall goal is to provide a dolidfoundation of research as a base on which effectivehuman factors practices can build.
Human factors issues arise in every domain in which
people interact with the preducts of a technologicalsociety. To perform its role effectively, the committeedrawn on experts from a wide range of scientific andengineering disciplines, including specialists in thefields of psychology, engineering, biomechanics,cognitive sciences, machine intelligence, cmputersciences, sociology, and human factors engineering.Experts in additional disciplines also participate inthe working groups, workshops, and symposia organized bythe committee. Each of these disciplines contributes tothe basic data, theory, and methods needed to improve I
i- A
**POP,

the scientific basiw of human f2ctors.Simulat.3" sickneas, the experience of symptoms
similar to motion sickness, has occurred frequently incivilian and military flight training simulators and, ia
some cases, has persisted or arisen several hoers aftera simulator sessirmn. The syndrome 4a of concern tosimulator designers tnd users, incl.ding simulatordevelopers, flight instructors, tra.ning and operitional
personnel, aerospace physicians, physiologists,
psychologists, and, cf course, pilot".It is important t. beir in mind .iiat simulator
sickness may be a special case of sijtial dise-orientation, or at least result frown the same bic
mechanisms. Spatial orientation ii a fundamenLalbiological function that incorporates posture,
locomotion, and kerwvedge of one's position in space.As such, it is of continuing inter'o-L to a wide spectrum
of scientists concerned with its un,,erly.rng nscnanisms,individual differences, pathology, .nd developftentalaspects. Thus, the study of simula''or sickness isvaluable not only from the point of view nf simulatorsbut also in terms of the contributirn it way make to themore general phenomenon of spatial orientation.
Recognizing the potential importance of the problem,the Naval Training Equipment Center, the Army ResearchInstitute, and the Air Force School of AerospaceMedicine asked the Committee on Human Factors toidentify current information and ti recommend researchaimed at the development of ,:cuntermeasures. Thecosemittee convened a three-day workshop September 26-28,
1983, at the Naval Postgrad.iate School in Monterey,California, to: (1) review available information on the
nature and severity of the symptoms oi simulator sict-ness, their frequency, and circumstances of ocarrence;(2) identify its likely etiology and contributingfactors, such as simulator design characteristics andtraining methods; (3) assess the efficacy of cairrentavailable counterveastires to the effects of s.sulatorsickness; (4) assess whether its occurrence io anindication of deficiencies in simulators that way
adversely affect the transfer of learning, operationalpetformance, or safety; and (M) recmend research andother courses of action necessary t- eliminate the
problem of simulator sickness.Nineteen experts in one or more of the following
fields participated in the workshop: onption sickness,vestibular dynamics, visual procezres, wimnlator
'ii
I

sic.kness, and :3imulator dessign and use. This report orthe proceedings reflucts the discuxai:n that toýk placeanc the group's recommrier-Ations for res3arch. It isba.ied on audio recordingd )i the wzorkshop, backgroundposition par-ers provided W.' the participants in advanctof the meeti-g, presenc.t'ons at the meeting, andcomments on a preliminsry draft. In a number ofsoctions of the report.. -tributio~i is givon to indicatethat the section reflect- the thinking of un ipdividualparticipant. Most participants made comment4 ;n tbeAraft report, which %ere incorporated into .he texr. Wehave attempted to re~lect the workshop issues and thethinting of the participants as accurately as posfible.
A background pap;er 1 repared by Rcbert S. Kennedy andLawrenc(e H. Frank, "A Te,,iew of Moticn Sickneas WithSpecial Reference to Sitmator Sickness," provided areview of existing infotaption for the dtliber•tin's oftho workshop participants. The paper, which is availablefroa the Committee or ljnr Factors, describes thephenomenon of motion sickness ard presents arioustheories concer-ing its etiology and responsecharacteristics.
It should be noted that the workshop participantssupport the use of flLgnt. simulators for training. Ourdiscussions of simulator sickness do not imply anindictment of simulators. Our ;ntent is rather t3strive for progrese iii :he design and aiVplication ofsimulators through understanding. As technologyadvances, continued advances are also necessary in thehuman/machine interface.
A related study on simulation has recently beencompleted by a special working grur of the Committee onHuman Factorn The worting group's report is scheduledfor release early in 1935.
In addition to the uorkshop pacticipantu, a numberof people contributed it. importint ways to the successof the study. Michael L. McCauley did a fine job asPditor of the prcceedings report. Robert T. Hennessy,the committee's study director in 1983, and workshopparticipants Robert Kenn#dy and Larry F.'ank effectivelyplanned and organized the workshop. Cecald S. Kelecki,of the Office of Naval Research, Alfred K. Fregly, ofthe Air Force Office of Scientilic Rese4rch, and RooertM. Sasmor, of the Army Research Institute for theBehavioral and Social Sciences, providen importantassistance in organizing and supporting this effort.Charles W. Hutchins hosted the meeting )n behalf of the
xiii
- - 1*~~~ -___________ -3

%ava1 postgraduate School; his hospitAlitY and horl *or%
in prepaifng the t.filites for the workshop are
,inctrely appreciaCed. Stanley Deutsch, the commttCC'
study director, made valuable contributiotS in
ortaoilinl and drafting the report. Christine L.
1cShane, editor of the Comiesion on Behavioral and
Sociat Sciences and Education, was extrcueal helpful in
improving its style, orsetitation, and clarity. Ann G.
polvinate, administrstive assooiate of the ComiSssioo,
end Jeanne Richards, the committee's administative
*,crotery, provided extensive secretarial and
edministrative support.
Herschel W. Leiboitx, Chair
Worksho;' on Research Issues in
Simulator Sickness
liv

INTRODUCTION
Simulator sickness is a term used to describe thediverse signs or symptoms tiat have been experienced byflight crew* during or after a training session in a
Slight simuletor. The phenomenon has been described aspolygenic and polysymptomatic; symptoms incl%de nausea,dizziness, spinning senhstinne, visual flashbacks, motordyskinesia, confusion, and drowsiness (Frank et al.,1983). Observable evidence (signs) of simulatorsickness include pallor, cold sweating, and emesis.
Motion sickness is a general term for aconstellation of symptoms and signs, generally adverse,due to exposure to abrupt, periodic, or unnaturalaccelerations. Simulator sickness is a special case ofmotion sickness that may be due to these accelerativeforces or may be cauned by visual motion cues withoutactual movement of the subject (Crampton and Young,1953; Dichgans and Brandt, 1973).
Although some scientiits have objected to the ternsimulator sickness because the constellation of effectsassociated with it would be described better as asyndrome than a sickness, most of the workshopparticipants concurred with the use of the term becauseit is idiomatic, similar to terms for other subsets ofmotion sickness such as sea sickness, car sickness, andspace sickness. (The National Aeronautic and SpaceAdministration has adopted the term space adaptationsynd'ome--Homick, 1982; Hicogossian and Parker, 1982).
Simulator sickness has been experienced by pilots,copilots, and other crew members in flight simulators aswell as by drivers and passengers in automobilesimulators. The workshop emphasized simulator sickness
II IIIj/

2
related to flight simulators, but pertinent evidencerelated to automobile simulator* was also discussed. Inall documented cases of simulator sickness, a visualdirpLay of vehicle dynamics has been involved.
Simulator sickness occurs in both fined- and motion-base simulators. It occurs during the simulator flight,immediately afterward, and many hours later. Thephenomenon was first reported in connection with ahelicopter simulator (Navron and Butler, 1957; Miller.nd Goodsoi, 1958), but it has occurred in patrol,
transport, and fighter/attack aircraft simulators aswell. The highest incidence (88 percent) has beenreported in an air combat maneuvering (ACl) simulatorduring fixed-base operations, in which high visualacceleration maneuvers are common (Kellogg et al., 1980).
Experienced aviators and test pilots seea to be moresusceptible to simulator sickness than inexperiencedtrainees. This fact seems surprising, but it is
consonant with the sost common explanation of the causeof simulator sickness, i.e., intersensory conflict. The
sensory conflict hypothesis suggests that experiencedaviators have a well-established neural store
representing the relationships among manual controlactions, visual dynamics, and the orientation and
inertial senses subserved by the vestibular/proprioceptive systems. Inexperienced aviators do nothave such a well-established neurophysiological"expectancy" for these relationships. To the extentthat the simulator violates the sensory expectancies, aconflict exists.
Simulator sickness may be of operational
significance because of four kinds of problems:
I. Compromised Training. Symptoms experienced inthe simulator may compromise training through distractionand decreased motivation. Behaviors learned in the
simulator to avoid symptoms (e.g., not looking out thewindow, reducing head movements, avoiding aggressivesaneuvers) may be inappropriate for flight.
2. Decreased Simulator Use. Because of theunpleasant symptoms and aftereffects, simulator userssay be reluctant to return for subsequent trainingsessions. They also may have reduced confidence in thetraining they receive from the simulator.
3. Ground Safety. Aftereffects, such asdisequilibrium, could be potentially hazardous for userswhen exiting the simulator or driving home.

3
4. Flight Safety. No direct evidence exists for arelationship between simulator sickness aftereffects andaccident probability. However, from the scientificliterature on perceptual adaptation, one could predictthat adaptation to a simulator's rearranged perceptualdynamics would be counterproducti t in flight. Indeed,
anecdotal reports from the Royal Air Force in the early1970s indicate that flight instructors claimed increasedsusceptibility to disorientation In flight hours after asimulator sassion.
This report covers the topics that were discussed indetail at the three-day workshop. It begins with anaccount of the major studies of simulator sickness andwhat we know about its incidenLe and prevalence. Thenext secticn describes the televant design heracter-istics of simulators: it begins by describiig some o!the characteristics of simulators and their operatorsthat may be involved in simulator sickness, includingvisual systems, lags, motiort systems, and other motion
cueing devices; it then discusses design problemsspecific to flight simulators and those specific to
automobile simulators. Theories o! motion sickness andadaptation are dealt with in the following section, and
sensory conflict theory emerges as the most plausibleexplanation for the phenomenon of motion sickness. Thereport then makes a number of practical suggestions foravoiding the effects of simulator sickness in the
equipment currently in use, although these counter-measures remain to be validated. It ends with a summaryof the recomnendations for research that surfacedthroughout the workshop.
It is important to note that the workshop did notreview the relationship of space sickness (or spaceadaption syndrome) to simulator sickness. This omissionwas deliberate, largely due to the fact that therelationship between motion sickness in a one-gravity
environment and the space adaptation syndrome is poorlyunderstood at this t-.me. In studies by NASA there wasgreat difficulty in ptedicting susceptibility to spacesickness using tests performed in one-gravityenvironments. Even incidents of motion sickness inprovocative one-gravity environments prior to spaceflight were not useful in predicting incidents of spaceadaptation syndrome (Nicogossian and Parker, 1982).
/

INCIDENCE AM3 PREVALENCE*
The overall incidence of simulatur sickness in flighcsimulators across the armed services is unknown, evftnthough the problem was first reported nearly 30 yearsago. There are suggestions, however, that the incidenceis increasing. Pilots tend not to talk about suchproblems as simulator sickness, so we may be under-estimating the probim. As new video systems becomeoperational in simulators and in aircraft, inforestionabout simulator sickness and motion perception maybecome even more important.This section is a brief review of the docwuaentedevidence of simulator sickness. For a more completereview, see Kennedy et al. (1983) and Frank et al.(1983). In addition, Puig (1970, 1971) has reviewed thetheoretical basis for disorientation and sickness insimulation.
Table I summarizes the major studies that have beenmade of simulator sickness. The studies by Havron andButler (1957) and Miller and Goodson (1958, 1960), thefirst published reports of simulator sickness, found asubstantial incidence (72 percent) of symptoms amongusers of the Navy's 2-FH-2 Rover Trainer. An interestingfinding from the Miller and Goodson work, as previouslynoted, is that "the more experienced instructors seemedto be those most susueptible to unpleasant sensations."Other findings of note were that "the more violentmaneuvers were found Lo produce a greater degree of
*This section was drafted from the workshop presentationby Lawrence H. Frank.
4

)5
a A
o0 UD 0 'A * U0a
10 ý o 0% 0l 4 1 e PC%. e4O Q 3'~~ . N r
V 4 u
C C4 C1
- .4 cc.4
1.U)U 0- 4 C4 C4 N -.4g.4 a
UIt
C- *Oa Q a C
t.. Va to v dU
soI. - .. . w I
3U 0 0
-3 4 t.Of a4 r- 410w w o c
0. u . pi I
aw

6
f'otion sickness.' Instructors have reported that theyarA more prone to become sick when sitting as apassenger . . . than when they are actually 'flying' thesimulator" (Miller and Goodson, 1960:210). Miller andGoodson (1958) also reported the occurrence of delayedeffects in an instructor pilot who became "so badlydisoriented in the simulator that he was later forced tostop his car, get out, and walk around in order toregain his bearings enough to continue driving" (p. 9).
Sinacori (1967) studied simulation techniques forveLical short takeoff and landing (VSTOL) flight.Using only one test pilot, he was able to report:
Pilot vertigo was induced as the time duration of aparticular flight increased. Vertigo was especiallyannoying to the pilot during attitude reversals orhovering. The pilot felt he could do better withcockpit motion teso .%. . Pilot vertigo may becaused by the confl'ct betwejn the sometimes "fair"visual cues arquired doring attempted hover and thehighly trained kinesthetic sensations which are
expected but not felt because the cockpit is fixed.Inadvertent pilot head motions were observedfrequently.
Kellogg et &l. (1980) studied simulator sicknessduring fixed-base operations in the Air Force Simulator )for Air to Air Combat (SAAC). which has a wide field of
view. The 48 pilots surveyed were undergoing an intenseexposure--a high acceleration environment (impliedvisually) during 550 ACM engagements over 5 tays,averaging a total of 12 hours of exposure for eachpilot. More than 87 percent of the pilots surveyed
reported some symptoms of simulator sickness, primarilynausea. Symptoms were most prevalent in the first Zvwdays. Pilots reported visual flashbacks, sometimes 8-10hours after exposure; these included sensations ofclimbing and turning while watching TV and experiencingan inversion of the visual field while lying down.
In a study for the Canadian Defence and CivilInstitute of Environmental Kedcine., Money (1980)investigated reports of simulator-sickness in the AuroraCP 140 FDS (analogous to the U.S. Navy's P-3 Orion)* Hefound that 44 percent of the pilots reported symptoms,ranging from clight discomfort to mild nausea. Thesymptoms were usually experienced only in the first oneor two simltator exercises. Subsequent exercises weresymptomr-frea, presumably due to habituation.
_______l____________

7
McGuinness, Bouwman, and Forbes (1981) investigatedthe incidence of simulator sickness among 66 air crew inthe Navy's F-4/F-14 Air Combat Maneuvering Simulator(ACMS),.the 2E6, and reported an overall incidence of 27
percent. However, the more experienced air crews, thosewith more than 1.500 lifetime flight hours, had anincidence of 50 percent, whiLe those with less than1,500 hours had an incidence of 18 percent. Pilots hada greater incidence than Radar Intercept Officera (RIO&or "backseaters") with incidences of 36 percent and 15percent, respectively. There were no reports of visualflashbacks in the 2E6. Dizziness was the most frequentsymptom, followed by vertigo, disorientation, "leans,"and nausea.
Franic (1981) reported that approximately IC percentof those using the Navy's F-14 simulator, the 2F112,experienced symptoms of simulator sickness and thatapproximately 48 percent of those sampled in the E-2Csimulator, the 2F11O, experienced symptoms. In the2F110, several of the pilots commented that the visuaIstreaming that occurred during turns-while-taxiing wasparticularly disconcerting.
Crosby and Kennedy (1982) found that flightengineers were having problems in the P-3C simulator,the 2F87. They found that the flight engineer wasviewing the independent CRT/CGI displays of the pilotand the copilot from 30 degrees off-axis. Measures ofpostural equilibrium in walking and standing, which havebeen used previously as indices of vestibular disruption(Fregly, 1974), indicated significant decrements in 50percent of the flight engineers after a normal four-hour
exposure in the simulator. Occluding the flightengineer's view of the pilot's and copilot's displayseliminated the postural equilibrium problems.
Frank and Crosby (1982) investigated the CH-46E
helicopter simulator, the 2F117, while it was in thefinal stages of development and production. Theyreported some tendency for symptoms of simulatorsickness and suggested that a more rigorous study beconducted after the 2FI17 is introduced to the fleet.
From the brief review given above it is clear that a
constelletion of effects have been found in air crewsduring or after exposure to flight simulation. These
effecte include the classic Gigns and symptoms of motionsickness and phenomena associated with perceptual
adaptation. The overall incidence and severity of theproblem across a broad spectrum of flight simulators,
however, has not been established.
• ÷ ~ .

SIMULATOR CHARACTERISTICS
A large number of simulator and ooerator characteristicsare nuspected of playing a role in simulator sickness.The wo~kshop participants generated a long list of them,which provided an initial structure for discussion.Limitations of time at the workshop allowed only a fewof these characteristics to be discussed in detail.However, as a potential guide to other investigators,the complete list appears as an appendix to this report.
This section presents the discussions that tookplace on visual systems, time lags, motion systems, andother motion cueing devices. It also incorporatesworkshop presentarions on the design of a particularflight simulator with its attendant problems andproblems involved in automobile simulators.
Visual Systems
Several types of visual systems have been used in flightsimulators, the major ones being point-light source,model boazd, and computer-generated imagery (CGI).Cases of simulator sickness have bees documented in CGIand point-light source visual systems, but they sees tobe less frequent in model board systems.
One of the important variables for simulatorsickness is the field of view (FOV) of the visual system.An estimated range of horizontal FOV for flightsimulators 's 40-360 deg, depending on the purposes ofthe simulation. For example, the Navy's Night CarrierLanding Trainer (NCLT, 2F103) has a relatively narrowFOV, approximately 40 deg. In contrast, ACl simulators,
8
S.. .....

9
such as the Air Force SAAC anA the Navy's ACKS, havewide FOVs, in excess of 300 deg.
Research by Leibowitz et &1. (1982) has suggestedthe importance of the ambient visual system in processingdynamic and orientation information. The general findingwith respect to retinal location is that infor-r.ti-on atthe peripheral retina is a more powerful determinant ofspatial orientation effects than is information at thecentral retina. This is confoundtd, however, by sub-tended angle; things usually get larger in the peripherybecause one is moving forward. So perhaps it would bemore accurate to say that larger things affect orien-tation more than smaller things.
Thus, w ider FOV would provide more stimulation forthe ambient system, resulting in a more compellingvisual display of motion. This enhanced sense of visualmotion may contribute to more conflict with vestijularinputs, which are relatively impoverished in thesimulator.
The SAAC has s mosaic of eight electronic screensthat surround the canopy of an P-4 cockpit, yielding a296 x 180 degree (H x V) FOY. Anecdotal reports suggestthat disorientation and symptomatology occur with thefull eight-window display, but not with three windows.Also, a compelling illusion of tilt was perceived withthe eight-window display when a flight scenario wasfrozen in a 45-deg angle of bank.
A study by Reason and Diaz (1971), however, found noincrease in the incidence of sickness in an automobilesimulator as the FOV was increased from 45 to 90 deg.More research is needed on FOY.
Scene detail is another variable that may beimportant in the genesis of simulator oickness. Greaterscene detail provides the human visual system with moreinformation about spatial dynamics, presumably sharpeningthe perception of motion and generating greater conflictwith the vestibular inputs. The effects of scene detail,however, have not been investigated systematically.
Lags in the temporal presentation of the visual"display have been suggested as a contributing factor insinulator sickness. This issue is discussed more fullyin the section below on lags.
There has been some suggestion that the detailedprocess of writing a visual display across the screenmay be registered by the human visual system, if notperceived consciously. According to one estimate, atypical time period for writing the video image is
r
* --

10
approximately 16 msec. In several simulators, e.g., theAdvanced Simulator for Pilot Training (ASPT) and SAAC,
the video images are written in different directions onadjacent windows. This may create an unusual visualstimulus of simultaneous movement in different directionsin adjacent locations. It is possible that these kinds
of effects may contribute either to symptoms of simulatorsickness or to the visual aftereffects that have beenreported. The same problem of multidirectional videowriting is likely in the new area-of-intecest simulatordisplays, in which one display is contained within alarger one, their video images being written indifferent directions.
Some simulators have visual systems with a 2:1interlace system in which the video imagery is updatedby the computer at 30 Hz but the display is updated at60 Hz. With this type of system it is inevitable thatmoving targets create double images, which may createillusory movement and other problems, Luch as a strobiugeffect. The contribution of these effects to simulatorsickness is unknown.
Other features of visual displays have been cited aspotential contributors to the problem. Opticaldistortiona were mentioned by Miller and Goodson (1958)as a probaole contributing factor in simulator sickess.Poor resolution, flicker, and off-axis viewing also havebeen implicated (Frank et al., 1983).
As new video displays become operational inaircraft, it will be p&rticularly important to ensurethat the visual dynamics provided in the simulator arecompatible with those experienced in the aircraft. Forexample, a helmet-mounted TV diaplay will be included inone cf. the weapon systems on the Army's new gurtship, the64 Apache. Research on visually coupled systems shouldinclude questions of perceptual aftereffects in thesimulator and the aircraft.
Eventually, three-dimensional visual displays arelikely to be introduced. The study of motion perception,perceptual adaptation and aftereffects will be even moreimportant when three-dimensional displays becomeoperational in simulation.
Lags
Temporal incongruities may exist in the presentation ofmotion information in the simulator. Time lags may

Il
occur in the visual system (Crane, 1983), the motionbase, or both (Ricard et al., 1976; Ricard and Puig,1977; Semple et al., 1980).
Lags should be defined with reference to thetemporal relationships found in the aircraft as well asto the usual description of total time. As an example,suppose that 50 maec elapsed bet'een a rilot's rollinput with the stick and the beginning of the aircraft.roll. Given the same input in a simulator, realisticestimates of lags might be 250 msec before the visualsystem begins to respond and 350 msec for the motionbase. There are thus several sources of error for thehighly tuned noural store of the experianced pilot: a200 msec lag in the visual, a 300 msec lag in theinertial, and a 100 msec discrepancy between the two.This is a complex problem, because there probably is nota constant optimal lag time. Puig (1970) has pointedout that the optimal lag time is likely to be a functionof the intensity of the stimulus (i.e., the level ofacceleration).
Moreover, lag is just one index of the fidelity ofdynamic information. The accelerative responses of thevisual and inertial systems should not only begin at the
proper time, but follow the rise time and amplitudecharacteristics with reasonable fidelity.
Experienced pilots have learned a set of temporaland spatial patterns in the aircraft related to controlstick inputs and the re..dltant visual, vestibular, andproprioceptive feedback of acceleration information. Inthe simulator, they are confronted with a new set oftemporal and spatial patterns, i.e., lags, rise times,washout, etc. This discrepancy is probably the mainsource of simulator sickness.
We gain more insight into this problem byconaidering the differing dynamics of the visual andvestibular sensory systems in the perception of motion.Retinal receptors signal position and velocity of avisual target, from which acceleration may beperceptually derived. In contrast, the otoLiths (in
j company with sonaesthetic mechanoreceptora) aresensitive to linear acceleration and rate of change ofacceleration (jerk) and hence give information aboutbody movement that is phase-advanced on that provided bythe visual system. Sensory integration of thesegravireceptor signals is required in order to perceive
- - • transiant linear velocity and displacement. Accordingto Benson (1978), the semicircular canals signal, for
w.
: .. .. ll I I J I I I I II .J I I 1 I _ I I I . . . . II I .. . ..

12
transient angular movements, the angular velocity of thehead and provide cues that allow the change in angularposition or angular acceleration to be perceived byintegration or differentiation of the afferent signalwithin the central nervous system. The implication ofthese differitig sensory dynamics is cnat sensory
conflict is likely to be the greater if mechanicalmovement of the simulator (and hence the operator) lagsvisual movement of the visual display than if the motionsystem leads the visual.
Why are more experienced pilots more susceptible tosickness? Perhaps only people who are very susceptibleto motion sickness are likely to have a problem whenthey are inexperienced, but as experience is acquired,the less susceptible pilots also may bw affected. Thisinformation is important to simulator designers, becausethey can aim their design at the experieiuce level of theuser6. Highly expvrienced pilots may not tolerate asmuch error between visual and motion cues. Withinexperienced students, however, high transfer oftraining may require a less exacting simulation.
A simulator (particularly the motion base) cannot
reproduce the acceleration waveforms of the aircraftexactly. Whct degree of departure from the nominalacceleration waveforms is acceptable? The answer is notentirely known. It depends in part on human visual andvestibular processes as influenced by simulator
characteristics and the experience of the user, both inthe aircraft and the simulator. This is certainly anarea for further research that could have an effect onsimulator sickness, the transfer of training, andsimulator design guidelines.
mNotion Systems
The majority of today's military flight simulators havea motion base. The number of axes of motion varies fromone to six, although six is most common. The typicalmotion base is hydraulically driven and has a maxiwmuangular displacement of 32 deg and a maximum linear(translational) displacement of about I m. Because ofthe displacement limitations, motion systems are drivenby command signals using washout algorithms that permithigh fidelity of movement initiation, with subsequentdiminution of the motion response even though theaccelerations associated with the maneuver (and implied

13
by the visual display) continue. The importance oftuning the washout algorithms is diBCuased in thesection on designing a flight simulator.
The responsiveness ot a gocd motion base providesvestibular and proprioceptive cues to motion for subtleaircraft maneuvers. In very extreme mane-Avert, such asthose required in air-to-air combat, the moti,3n base hasthe hopeless task of ke-eping up with sustained high-gravity turns and rapid roll rates. It has been reportedthat the Air Force air combat simulator (SAA) had amotion base that was t*ventually disengaged because ofits ineffectiveness (Seever& and Makinney, 1979). TheNavy's 2E6 air combat simulator is also fixeO-base(HcGuinness et al., 1981). Despite good designcharacteristics and periodic calibration, the etfective-ness of a motion base is likely to be limitea insimulators intended for scenarios with high-acceleration
maneuvers.Frank et al. (1983) have emphasized the importance
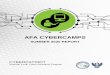
of simulator resonant frequency as a possiblecontributory factor to simulator sickness. It is knownthat symptome are greatest at a frequency resonance ofabout 0.2 Hz (McCauley and Kennedy, 1976; Money, 1970).Hence, it would appear advisable to avoid this very lowfrequency range at the trainee's sitting position inbuilding simulators. Frank et al. (1983:7-8) describe acase in point, which appears as Figure 1:
(The figure) prisents a compmrison between MilitaryStandard 1472C tMIL-STD 1472C, 1981) vibration
protection limits, projected envelopes fox lessersymptomatology, %nd the SAAC fi.equency spectrum.The two solid lines are from V'IL-STD 1472 andrepresent the 90% protection limits for an 8-hourvibracion exposure. The solid U-shaped Line,representing the exposure limit for below I Hz, isbased on a criterion of frank emesis. The solidline, representing the exposure limit for above 1SFz is based upon a criterion of fatigue-decreasedproficiency. The criteria for these two differ as aresult of the large quantity of data generated onthe effects of vibration on human performance above
curtently insufficient to reach hard conclusions for
eXpq sures to very low frequency vibrations (i.e.,bel w I Hz). The limits for below I Hz, then,should be viewed as conservative, since it can be
V_

14
'~~ j %AI4?Y £6OfAW%
*1 I /
e4,~~ MI T1 A I t's 6,1S(w
//
StJ -Ii WITII•AtOft of A5
043 eINIT At tIM? ONti %VMPIOIM
/ /7 . NO
031%-
,,M~ W1(10 l:'% ,¥ .. ...
020
Ole .... ...
o 0 416 / IW ioI.a
rplioulftcy (W KAMgo
FIGURE 1 A Comsparison Betveen MIL-STD 1472C VomnitingCriteria and a Projected Envelope for LesserSymptomatology.
Source: Frani, et al. (1983).
predicted that decrement's in performance can beexpected to' occur before euesis. Consequently,the heavy-dashed line represents our estimation ofwhere 50 of the population i!. exhibit at leastor- srptoi of simulator or motion sickness (e.g.,pallor). The light-dashed line is our estimationof where at least one post-effect will occur.Mot- trat the tolerance limits for each of theseenvelopes shift upward, coincident with thespectrum for normal locomotion. Note, also,
Crieri an a rojcte Eneloe fr deeaS~sptc~~o~o'I

15
that the lowest thresholds correrpond to thoseenergy -egions that are most associated with motionsickness. . . .
The SAAC spectrum depicted in (the figure]was replotted from Hartman (1976). This mappingreveals quite clearly that the resonant frequency ofthe SAAC inertial system intersects our estimatedtolerance envelopes and, therefore, may be conduciveto simulator sickness. Indeed, Hartman and Hatsellreported incidence rates for spatial disorientation,eye strain, tiredness, headache and nausea of 52%,50%, 38%, 32%, and 14%, respecti'vely.
It is readily apparent from the figure thatsimulator resonant frequency is o)f critical saliency,relative to simulator sickness; and that simulatorsshould be designed with these envelopes in mind.
Other Mttion Cueing Devices
In addition to a motion base, G-seats, G-suits, helmetloaders, and other devices have been used in flightsimulators to provide pseudo-inertial cues to the pilot.The cueing algorithms for these devices require furtherdevelopmcnt to ensure that the proper temporal patternsare achieved relative to the vision and motion basesystems.
G-seats may be pneumatic or hydraulic. Thepneumatic seats have longer lag times, which must be.ompensated for if they are to provide useful motion
cies. G-seats also change the locition of the pilot'sheaed, a feature that combines with voluntary headmovement to change the point of regard of the visualdisplay. These variables have not been thoroughlystudied with respect to the pilot's perception of motionfrom the display or the potential discrepancies relativeto the aircraft.
Comment on Visual and Motion Systems
In summary, the characteristics of both visual displaysand motion systems for simulation present problems, notonly with regard to simulator sickness, but in thelarger context of the selection and counication ofmotion information to support learning and optimizetransfer of training.
IOwl',

16
Designing a Flight Simulator*
In 1965 the Northrup Corporation was committed tobuilding a flight simulator to study the problems ofaerodynamics and flight control for vertical shorttake-off and landing aircraft. The concepts forbuilding a simulator then were not much different thanwhen Miller and Goodson first reported simulatorsickness in 1958, according to the DeFlores Principle;i.e., the pilot sat in a fixed platform surrounded by aspherical screen with about a 12-ft radius. At the topcenter was a point-light source that provided a screenluminance of about I ft-Lambert. Features on a glassplate below the light were projected onto the screen asshadows. The plate was servo-driven under the light tosimulate the progress of the aircraft over the ground.
Field of view is the first factor identified as
important in simulator sickness as discussed above.Both size and shape are relevant aspects of FOV. TheNorthrup simulator had a FOV of about 200 by 60 degrees,which is equivalent to abouc 28 percent of a completesphere. Such a large field is quite compelling to thepilot.
The X-14 aircraft at Edwards Air Force Base was usedas a validation aircraft for the simulator. It had T-34wings and tail and a "home-made" fuselage with an opencockpit and two J85 engines. The project team atNorthrup tried to design the simulator so that the pilot
ratings of flight handling characteristics would beequivalent for the simulator and the X-14. They werealso interested in the test pilot's (N - 1) subjectiveimpressions of workload.
One of the first things they looked for was theability to maintain a hover. There was a goodcorrespondence between the performance of the aircraftand the simulator for the hover. The visual display andthe control characteristics seemed quite adequate.
Scene detail became an issue as they attempted toput features on the glass plate for the visual display.The raw number of stimuli that represent the real world,probably an important factor in simulator sickness, isrepresented as the number of patch boundaries in theluminance distribution. oere are metrics for thisfactor.
*This section was drafted f om the workshop presentation
by John B. Sinacori.
i .. . .. . . ., | ,,

17
When they tried the second maneuver, the lateral-quick-stop, the test pilot complained about stomachawareness and nausea. After about 10-20 minutes ofperforming lateral-quick-stops, the pilot had to take abreak to avoid being sick.
The pilot felt that these effects would go away ifhe had a motion base. Bolstered by discussions vittexperts such as Fred Guedry and an introduction to theconcept of sensory conflict (discussed below), theyacquired a motion base. It had 3 df, pitch, roll, andyaw with ÷/- 12 deg angular displacement--and notranslatory motion. The visual system was capable ofabout +/- 30 deg, so some type of washout was required.The motion base would initially follow a rollacceleration, for example, and then drift back, eventhough the aircraft was still at the full roll attitude.So a motion base with washout was considered as a way to
reduce the conflict between the visual and vestibularinputs that occur in a fixed-base simulator. Washout isa compromise: it does not produce the full motionenvironment of flight, but it provides more cues than afixed-base simulator.
Designing the washoat required a bit of trial anderror. A 12 deg roll would be followed closely by themotion base, but for larger rolls, the washout wouldbegin to reduce the response. On the basis of the workof Guedry, they knew tbat the tCte constant of thesemicircular canals was ov the order of 10 sec, so L;%eyguessed that the critical time conviant for the washoutwould be somewhere bet&ween I sec and infinity (which isequivalent to no timi constatnt--a 1:1 motion case).They swept through the :ime constants in the simulatorwith the test pilot giving his opinions about thesimulation characteristics. With an acceleration timeconstant of 2-3 sec (2-3 deg/sec/sec), the visual andmotion systems were quite acceptable to the pilot. Withtime constants less than 2 sec, he reported nausea andrelated problems, such as in the fixed-basemodes- Therewas also the tendency for the pilot to overcontrol, bothin fixed-base and short time constants. Longer timeconstants created other problems, because, wbiie theroll was accurate, the linear acceleration was absent inthe simulator (but -repent in the aircraft).
Although the tendency toward sickness was greatlyreduced with a time constant of 2-3 sec, some tracesremained. This may have been due to visual distortions,as mentioned by Miller and Goodson (1958), who evaluated
... .ll'l - WI N"III I

18
a helicopter simulator with a similar type of visualsystem.
Head movements are another subtle but importantfactor. Pilots in the simulator tended to roll theirheads back toward the upright in a roll maneuver, perhaps,in an attempt to maintain a stable visual image. Laterit was verified that the pilots did the same thing whenflying the helicopter. With the simulator in the fixed-base mode, the pilots again tried to decrease the angleof the horiton. but in this case the head movement was inthe opposite direction--with the roll rather thanagainst it.
Overall, approximately 75 percent of the experiencedpilots who flew the simulator in the fixed-base mode hadproblems with sickness. With the moving base, only about10 percent indicated any symptoms. Anecdotal evidencesuggests that these conditions may have the oppositeeffects on inexperienced pilots. The simulator operator/technician learned to "fly" the simulator in the fixed-base mone. Subsequently, when the motion base was added,he experienced symptoms of sickness. The implication isthat his prior adaptation to the sensory conflict
conditions in the fixed-base mode made him susceptibleto sickness when the visual and vestibular sources ofmotion information were rearranged by adding the motio~nbase.
A device like this simulator would be a good toolfor renearch on simulator sickness. One of the lessonsto be learned from this experience was that, in thisparticular situation, a washout time constant of 2-3sec, which is considerably less than the washout timeconstant of the semicircular canals (about 10 sec),seemed sufficient to reduce sensory conflict to generallytolerable levels. One might guess that a siwaulator timeconstant that matches the sensory one would be best, butit may be that as one increases the time constant toward10 sec, the intravestibulaz conflict (canals versus theotoliths) are magnified. The best goal may be a per-ceptual realism rather than a physical realism in thesimulation.
The changes in manual control performance thatoccurred as & result of the motion base were very small.Simulator design must take into account both petformanceand sickness.
Working on the visual systems will probably help toreduce the incidence of sioulator sickness. Using amotion base and manipulating the acceleration time
#WOO,-

19
constant shiould not be construed as the solution to thesimulator sickness problem, although they worked in thisparticular case, with a certain type of aircraft, certainmanouvers, etc. In cases of more extreme mane.vers,alleviation of siinulator sizkness by "beefing up" themotion base would be a very impractical approach. Amotion base is not a quick fix to the simulator sickressproblem.
Tilt is another feature on many motion-basesimulators, used to simulate linear acceleration. It isimportant to be very careful of this technique becausethe human senses are very good at perceiving tilt forwhat it is--a change in pitch attitude rather than atranslatory acceleration. According to Guedry, theotolith system provides both a position signal, i.e.,
static tilt relative to gravity, and a transient (phasic)response to change in position relative to gravity.Horizontal linear acceleration, within certain frequencyand magnitude limits, are perceived as linear velocity
rather than tilt, probably because the transient otolithsignal is unaccompanied by a complementary semicircularcanal signal.
Design Characteristics of Automobile Simulators*
There are many parallel issues in the design of drivingsimulators and flight simulators. Due largely to their
custom-made nature, high cost, and the large drivingpopulation, most driving simulators have been research
tools rather than training devices. Several years agoit became apparent that research using a number ofdifferent driving simulators was hindered by thesubjects' experiences of symptoms akin to motionsickness after even brief exposures (Reason and Diaz,1971). The incidence of sickness in research drivingsimulators is difficult to document; however, in severalcases symptoms have been quite overt and subjects havevoluntarily ended driving trials due to imminent emesi.
The basic concepts of the sensory conflict theory(discussed in a later section) seem to apply to theproblem of simulator sickness in driving simulators.Closed-loop delay, over and above normal vehicle
*This 4ection waj drafted from the workshop presentation
by John G. Casali.
£ ,tm

20
dynamics delay, soems to be particularly important.Historically, driving simulators have tended to haveless computational power for the vehicle dynamics anddisplay systems than flight simulators. And the motion-base systems have in many instances been cruder thanthose used for flight simulation, although this ischanging of late. For these reasons, there have some-times been closed-loop lags in the system that areperceptible to the drivers, which may contribute to cueexpectancy couflicts and also degrade vehicular control.
Automobile simulators also face the same problem oftilt. Certain automobile simsulators have used oversizeroll and pitch motions to simulate lateral and longi-tudinal transactions, respectively. Instances of driverdiscomfort and manual control difficulties have beenreported for several of these devices. Apparently thevestibular system is not easily fooled into believingthat tilt (angular position) is equivalent to a linearacceleration. A potential conflict say arise when thesubject perceives the motion as rotational, when themotion cue that is anticipated in response to controlinput is primarily translational.
In an attempt to catalogue simulator characteristicsthat potentially contribute to simulator sickca.s, itwas found that subjects in about 10 of a total of 25driving simulators had reported motion sickness. Bothfixed- and motion-base simulators were represented aoongthose with symptoms.
Casali and Wierwille (1980) performed a completefactorial experimental study of driving simulatorsickness using a modified version of the Virginia Techsimulator. This device includes a CGI 50 dog(horizontal) FOV, sonochrcme display of a two-lanehighway, a 4 df motion base (does not include pitch andheave), and a full sound system. The lateral translationcue was replaced with an oversizad roll cue, and a 300meet pure delay with smoothing in the closed-loopdynamics was Prtificially introduced. The subjects'view of the surrounding room was occluded by a narrow,boxlike cab. All these "degraded" simulator variableshad some negative effects, either in increasing vehiclecontrol problems or inducing mild symptoms of sickness.They found no profound cases of simulator sickness,however, from sore than 1,000 subjects in variousstudies.
A test of field dependence was used to match subjectsin the study. They found no relationship between this
rA

21
measure and motion sickness, contrary to previous resultsreported by Barrett and Thornton (1968), who found thatextremely field-independent subjects were more sus-ceptible to sickness than field-dependent subjects in adriving simulator. However, Barrett and Thornton alioreported more severe symptoms of sickness in theirexperimental trials than Casali and Wierwille found intheir study, perhaps accounting for the differentresults o! field dependence.
Because of the multivariable nature of drivingsimulator s*ckness, it is difficult to design researchthat will allow enough variables o be included in afactorial design to allow proper assessment of theinteractinns. This same problem applies to studies offlight simulators.
I /

THEORIES OF MOTION SICKNESS AND ADAPTATION
A theoretical understanding of the physiology andetiology of motion sickness is iwportant in solving theproblems associated itith simulator sickness. The work-shop participants reviewed some of the more prominenttheories that have been suggested on the phy3iologicalfactors involved. This section opens with an overviewof motion sickness as an adaptive response to thestimulation of the vestibular system.* It thendiscusses sensory conflict theory, the most persuasiveargument lo date. Next it describes studies ofadaptation to rearranged senscry inputs, illustratinghow people adjust to the conflicting message* from thevisual and vestibuler systems. It then describesadaptive changes in oculomotor systems. The sectionends with some comrents on theories of motion sicknessand some questions for further research.
The Greek word naus means ship and that is theorigin of the words nausea and nautical. It was oncethought that the sea brought about sickness by acting onthe stomach; it was some time before it was known thatmotion rather than the sea itself causes sickness. In1882 William James reported that motion causes sicknessby acting on the vestibular apparatus rather than thestomach (James, 1832). The term motion sickness is
*This overview was dr&fted from the workshop
presentation of Ken E. 11onny; for a ccmpreh naivt rcvi-twof notion sickness, see 11oney (1970), o • n(1975), Denson (1973), end Kennedy and !Fatik
22

23
usually defined as sickness caused by notion.Treisman (1977) addressed the evolutionary
significance of the emetic 'esponse of motion sickness:How could vomiting in response to a dynamic environmentcontribute to the survival of the species? He suggestedthat the significance of the emetic response was in theexpulsion of ingested toxins from the body. That is,vomiting occurs because the brain interprets thestimulus as if it were a poison.
Treisman's "poison theory" provides the basis forMoney's view of motion sickness, that it is theactivation, by motion, of the vestibular mechanisms thatnormally facilitate the emetic response to poisons. Thisview implies that motion sickness is a response to thestimulation of the vestibular system and that it involvesthe unnatural activation of a normal physiologicalmechanism, i.e., vomiting in response to poison.
It is well known that central vestibular units canbe driven by stimulating the ambient visual system(Waespe and Henn, 1977, 1978). Therefore, it is notsurprising that the vestibular mechanisms can beactivated by visual stimulation, as they are in simulatorsickness. It is also well known that in the absence ofthe vestibular system, motion sickness cannot occur.Someone who does not have a vestibular apparatus isabsolutely imune to wition sickness and, presumably, tosimulator sickness sr well, although this has not beendemonstrated directly.
The absence of motion sickness !in subjects without avestibular system has been i' wnstrated many times, inboth human and animal subjects. In a classic study oflabyrinthine defect!ve subjects (Lbs) aboard a ship inthe North Atlantic, all of the experimenters and thecrew got sick, but the LWs did not,(Kennedy et al.,1968). They were terrified and praying, but not sick.This experiment also dealt L blow to the notion thatan xiety gives rise to motion sickness; at least it doesnot in LDs. There is also no reason to think thatanxiety plays a major role in simulator sickness.
Money and Chiung (1983) tested the hypothesis thatthe surgical removal of the vestibular system shouldleave an animal with a defective response to poisons--which is one of the four physiological functions of theinner ear (i.e., I-earing, body balance, control of eyeftovcments, and the emetic response to poisons). Theemetic response of dogs to poisons was measured beforeand after surgical ra'ioval of the inner ear. The poisons

24
used in the study included lobeline, nicotine,apomorphine, and pilocarpine. The results of the study.ere that the dogs no longer vomited in response tomotion and that their emetic response to several poisonswas greatly reduced. For several other poisons, theemetic response was not reduced. There are a number ofsechanistis by which poisons can induce vomiting, and thevestibular system seems to be active only in some ofthem.
Money and Cheung concluded that there is a normalvestibular facilitation of the emetic response tocertain poisons. This supports the view of motionsickness given above, that stresses the central role ofthe vestibular system and at the same time indicatesthat it results from an activation, by motion, of anormal response. 4otion sickness is q normal responseboth for a wide variety of species when confronted withcertain conditions of real (or visually mediated)motion. We all use the term motion sickness, but it isnot really sickness: it is a normal physiologicalresponse. (There are, of course, dozens of mechanismswhereby vomiting can occur, and motion sickness is justone of them).
Treisman's poison theory gives credence to thesensory conflict or sensory mismatch theory of motionsickness (described in detail below), which is a usefulway to think about the problem of motion sickness andcan provide s meaningful framework for research.
rie evolutionary survival value of a physiologicalmechanism such as that suggested by Treismen issigoificant. It is accessible by stimulatian arisingfrom peculiar motions--motions that exceed the normaldynamic limits of the vestibular system. When exposedto such motion, the vestibular systcm therefore sendsinformation that it false (or distorted). The brainthen recognizes these inputs as false because they are Iin conflict with other information about motion fromvision, from another part of the vestibular system, orfrom proprioception. The result is notion sickness. Itis the false information from the vestibular system thatbecomes the stimulus for the brain's vomiting center. 1
II
j
$ U -ss

25
Sensory Conflict Theory*
A good starting point in understanding the role of
sensory conflict in motion sickness and simulatorsickness is to consider sensory inputs from the
vestibular, visual, and proprioceptor systems in natural
movements in everyday conditions. Children spend yearsperfecting control of eye, head, and limb movements,first crawling, then walking and running. With
maturation and practice, control of motion becomes
skillful and hence largely automatic.In the normal adult, the vestibular system works in
close coa rdination with the visual system to stabilize
the eyes relative to selected earth-targets during
"walking, running, and turning movements, and the three
systems work in close harmony in maintaining control ofmotion daring locomotion. Typically, most of thiscoordination occurs automatically and without conscious
awareness--until something goes wrong, e.g., a partial
unilateral loss of vestibular function. An afflicted
individual will be quite disturbed and acutely aware of
the challenge to his or her control of movement. Blurredvision (oscillopsis) uill probably result from turningthe head and nausea and vomiting from persisting inmoving about. However, by moving about with care, in
time the disturbing symptoms usually will disappear ashe or she adjusts to the new sensory inputs that occurduring movement.
In some respects the normal adult moving about on
the earth is like a skilled pilot, using skillsdeveloped over the years in controlling whole-bodymotion relative to the earth. The pilot, whose lifedepends on the skilled control of motion of the aircraft,
becomes an integral part of the motion control-loop ofthe aircraft. With experience the sensory feedback fromcontrol actions is used as an important part of the
control loop, and, as in any skilled perceptual-motor
control performance, the relations between controlactions and the unique feedback induced by the forces
and torques of flight recede from conscious awareness(i.e., the feedback is used autotatically). Only
deviations from expected sequences of sensory feedbackachieve conscious awareness and are assessed as potential
indicators for corrective actions.
"*Thi6 section was adapted from the workshop presentation
of Frederick E. Guedry.

s6
A quotation from Helvill Jones (1974:874) puts theforegoing in neurophysiological perspective:
There is good evidence that much of our normalmotor control is organized not merely as an ongoinginteraction between continuously operating automaticSherringtonian reflexes, but rather as centrallyreleased preformed packages of programed neuralinformation. One might well guess that adaptationto new requirements could be relatively.easily metby merely reprogramming relevant patterns of theoutgoing central neural discharge. However, thereis a growing body of research findings whichindicates that even cortically released patterns ofmotor'drive are not devoid of early interaction withcorresponding sensory mechanisms. For example wenow know that such a central discharge of motordrive is not only destined to activate musclesthrough relatively direct connections with spinalmotoneurones, but also, through collateral branchesof central fibers, to act directly upon SENSORYneural relay stations in spinal cord pathways. Thusthe corticospinal (Pyramidal) motor tract, not onlydescends to spinal cord networks generatingnotoneurone activity to drive skeletal muscles, butalso sends many collateral branches to synapsedirectly on second order afferent neurons in thesensory gracile and cuneate nuclei of the dorsalcolumns of the cord.
A clue to the functional implication of thisrather surprising fact is perhaps to be found insomewhat analogous mechanisms operating in theperiphery. For example it is nov well establishedthat in many circumstances both alpha and gammamotoneurones, innervating the main (extrafusil) andmuscle spindle (intrafusil) fibers of a skeletalmuscle, can be coactivated at the sa*e time. It hasbeen proposed that when the combined alpha-gamaprogram operates "according to plan," the musclespindles contract (or relax) in just such a way asto null out any change in their sensory dischargecaused by mechanical shortening of the main muscle.This rather neat arrangement would ensure that ifall went well (i.e., according to plau), then thecentral nervous system (CNS) would not be botheredwith unnecessary sensory information. By contrast,if the "intended" response was not achieved, then

27
needed sensory information would indeed reach theCNG which, in turn, would presumably modify the nextmotor cowmand. This capability to recode rearrangedmotion inputs raises several questions.
Thus, the experienced pilot is apt to be disturbe4'and perhaps made sick by the unexpected sensory feedbackin simulators thzt may differ consider:ioly from the feed-back engendered by the same control actions in theaircraft. This statement concerning the reason for thepilot's disturbance is based on what is called thesensory conflict theory of motion sickness.
In many situations that provoke motion sickness, nosingle component of the motion Stiuulus is either strongor nauseogenic, but in combination the sensory stimuLiinduce sickness. In other situations, highly nauseogenicstimuli can be rendered benign by the addition of othermotioA stiua'li, apparently becauso the added stizuliremove the conflict. These lines vf evidence offerstrong support for conflict theory. A brief descriptionof two experimenti will sorve to illustrate these points.
Tilting the head 30 deg laterally toward the leftshoulder during sustained constant speed clockwise whole--body rotation about an earth-vertical axis (velocity 1.0rad/sec) produces a cross-coupled ("coriolis") stimulusto the semicircular canals resulting in a sensation offorward tumble (about 90 deg out of the plane of thehead movement). This well-known stimulus is disturbingand nauseogenic to most people, especially when repeatedseveral times, yet no single component of the stimulusis strong or even disturbing. The vertical semicircularcanals have received an "angular impulse" equivalent toa velocity change of 0.5 rad/sec. The horizontal canalshave received even less stimulation. Thus the canalstimuli are not strong or disturbing. A 30 deg lateraltilt stimulus to the otolith system is also neitherdisturbing nor nauseogenic. However, in combinationthese stimuli are nauseogenic because in terms of theconflict theory, the semicircular canals have signaledrotation of the head about one axis while the otolithsystem (influenced primarily by the gravity vector) hassignaled change in head position about another axis.Thus there is an intralabyrinthina conflict, and inaddition there is conflict between the intended headmovement and the perceived motion of the head and body.The central nervous system has been presented withsensory input calling for compensatory reactions in two
.1

28
different directions at the same time; the sensation isconfusing and the situation is nauseogenic.
If the same head tilt is made during the camerotation velocity of the body but while the initialangular acceleration is in pcogress, then exactly thesame cross-coupled stimulus occurs, but it is not at alldisturbing, disorienting, or nauseogenic. The reason isthat the angular acceleration vector has been added, andits vectoral resolution with the cross-coupled vectoryields a resultant vactor that remains aligned withgravity (Guedry and Benson, 1978). In this case thesemicircular canals signal rotation about an earth-vertical axne that is in alignment with the direction ofgravity signaled by the otolith system, and thus thereis no conflict. Almost the same degree of ameliorationof effects of cross-coupled semicircular canal stimulican be produced by horizontal optokinetic aftereffects(Guedry, 1978) (Figure 2), which appear to modulateactivity in the vestibular nuclei as though thehorizontal semicircular canal had been stimulated (Hennet al., 1974). Observations like these lend credence tothe conflict theory and illustrate that the patterningof sensory cues can pliv a significant role in thenauseogenic characteristics of motion stimuli.
A conciptualization (Benson, 1978; Reason and Brand,1975) of the sensory conflict theory of motion sicknessii shown in Figure 3. Basically, the idea is that whensensory inputs from the eyes, semicircular canals,otolith organs, and other mechanoreceptors are inrepeated or conti-ual conflict %4th regard to the state
of motion of the body relative to the earth, thenadaptive changes of the central prtcessing of theseinputs must occur to yield efficient control of motionin the unusual motion environment. Meanwhile, themismatched inputs also set off the motion sicknesssyndrome, perhaps for reasons elaborated earlier.
•eason and Brand (1975) propose that most sickness-provoking conflicts are of three types, shown in Table2, and they cite examples for each type. It is possiblethat all conditions that induce motion sickness are notsubsumed by the sensory conflict theory, but most casesof simulator 3ickness are probably attributable tosensory conflict becsase simulators seldom introducestrong accelerative stimuli. One of the more compelling
atlcuents for the role of sensory conflict in simulatorsickness is that experienced pilots seen to be sore
susceptible to simulator sickness than are novices.
-.-. - s .ew.. s m

29
t~w, (CONSTAT)
f, VN-Veutibular nuclei
000fto
FIGURE 2 Cross-Coupled Semicircular Canal Stimuli
Source: Guedry (1978).
__ _ _ _ __ _ _ _ __ _ _ _
-- ~ I S -i

30
EllOLOGY OF MO•ON 8UXCMESS
ofe" Nownso
FIGURE 3 Etiology of Notion Sickness
Source: Benson (1978).
Adaptation Studies*
Much of the basis of the sensory conflict theory ofnotion sickness was formed from studies of adaptation toexperimentally contrived rearranged sensory inputs
involving motion cues. Two rather extreme experimentalsituations illustrate thO essential points of suchstudies.
In the first situation, individuals moving about inan enclosed rotating room are subjected to a number ofrearranged sensory inputs. Because the coon is rotating,any movement along a straight line relative to the floorof the room is a curved path relative to the earth(vision-proprioception conflict). Any tilting movement
*This section was adapted from the workshop presentation
of Frederick E. Guedry.
t ... ... .. .. .. .. .)

31
TABLE 2 Types of Sensory Conflict
Type I When A and B simultaneously sigtalcontradictory information
Type 2 When A signals in the absence ofan expected B signal
Type 3 When 5 signals in the absence ofan expected A signal
Note: A and B represent members of a pair ofnormally correlated receptor systems: visual-inertial and canal-otolith.
Adapted from Reason and Brand (1975).
of the head produces semicircular canal responsesroughly at right angles to change-in-position signalsfrom the otolith organs, and thus there is theintralabyrinthine conflict described above.
The second situation involves the use of right/leftreversal dove prisms. When an individual moves about inthe normal force environment, visual feedback is right/left reversed.
Initially both of these situations induce severeproblems with control of movement and motion sickess.Within several days, control of motion is improved andsickness subsides. In the course of this adaptation,changes in sensorimotor reflexes and in perceived motionoccur. Upon return to a normal environment the recodedsensorimotor system causes problems.
After adjustment to the rotating room, head tilts ina normal static environment induce perceptions of motionand a vestibulo-ocular reflex (VOR) at right angles tothe head movement plane end thus 90 deg displaced from anormal response. Control of body movement in the normalenvironment is severely degraded, and nausea andvomiting are common complaints.
As adjustment to reversing prisms occurs, locomotorperformance improves, the gain of VOR produced by passivewhole-body oscillation in the dark is reduced and, aftera few days, the phase of the eye movements shifts and
S... - l n

32
eventually achieves almost 180 deg of phase reversal.At night upon retiring, some subjects experiencefeelings of turning to and fro or unidirectionally.
After removal of the reversing lenses, locomotordisturbances are pronounced and the gain of the VOR toprssive o.cillatory stimuli in the dark requires severaldays for recovery, although the phase of the oculomotorresponse returns fairly quickly (2 hours) towardnormalcy. Voluntary head turning produces blurredvision and illusory movement of the world, an effectthat may persist for two or three days.
The time course of adaptation seems to vary, notonly according to the severity of the sensory conflictbut also according to diffarent aspects of re'.ponsesselected for measurement. For example, in theexperiments by Gonshor and Melvill Jones (1976) in whichsubjects adapted to the left/right reversing prisms, thefirst evidence of VOR adaptation was gain reduction(revealed by sinusoidal oscillation in darkness);subsequently the VOR returned somewhat, but with a largephase shift to bring the VOR into accord with thereversed vision. After removal of the lenses,oscillation in the dark still revealed a large phaseshift in the VOl but the phase shift dissipated in about2 hours, whereas the gain of the response requiredseveral days for readaptation to normal levels. Thus,different components of the response system can havedifferent courses of adaptation and recovery. In theslow rotation room studies at Pensacola (Guedry, 1965;Graybiet et al., 1965), recovery from prolonged rotationalso seemed to reveal divergence of response changes.Some subjects, tested 3 weeks after exposure to 12 days
.1 of rotation at 10 rpm, reported return of vertiginoussensations and exhibited recovery toward normalcy of VOlresponses to head movements during rotation, yet theydid not experience motion sickness within a 2-hourexposure. Thus, motion sickness, which is one aspect ofthe overall response to an unusual motion environment,may have an adaptation and recovery time course thatdoes not necessarily parallel other responses undergoingadaptive change.
These extreme examples of sensory rearrangement insensory conflict studies ore mentioned to maka the pointthat substantial changes in perception of motion,postural control, and sensorimotor reflexes occur whenindividuals attempt to control body motion in rearrangedsensory environments for protracted periods. The
i ....

33
beginnings of these effects can be ieen after shortexposures. Studies that form the basis of thesedescriptions suggest that the central nervous systemcommences rather quickly to recode itself for adjustmentof perceptual and motor response to rearranged sensoryinputs having to do with the voluntary control of motion.
They also raise several questions for furtherresearch. Simulators probably never introduce the
extreme sensory rearrangement involved in theseexperimental studies. But the recoding of responsesprobably occurs more rapidly with less extreme situations(Collewijn et at., 1981). Unlike the studies justdescribed, simulators do not require the individual tobe exposed to the rearrangement situation continuously
for extended periods. But how concentrated can simulatorexposure be before some recoding occurs such thatperceptual and sensorimotor reflexes are changed? Thestrong simulator aftereffects that have been occasionallyreported suggest some reason for concern. How specificare changed sets of responses to the simulated flightcontrol situation? The answer seems to be not veryspecific, si_... simulator aftereffects have occurredduring aormal locomotion, driving, and while lyingdown. These aftereffects suggest that something morethan intellectual learning of procedures has occurred.
Oculomotor Adaptive Systems*
Many conditions that produce adaptive changes inoculomotor systems also produce dysfunction in the formof motion sickness symptoms. Viewing flight simulatorvisual systems may involve some of the very conditionsthat produce oculomotor adaptation. The results oflaboratory studies of oculomotor plasticity maytherefore be relevant to simulator sickness.
Tnese laboratory studies have emphasized differentaspects of the same problem. Studies with prisms havebeen very popular with psychologists, probably becauseof the traditional interest in perceptual adaptation,while optometric and physiologically oriented scientistshave explored oculomotor adaptations. The two domainsare, of course, related, and, in most if not All cases,
*This section was adapted from the workshop presentationof Sheldon M. Fbenholtz.

34
changes in perception can be deduced directly frcm theknown changes in oculomotor function,
Vertical divergence, for example, can be inducedthrough the uie of prisms (ore eye elevated more thanthe other) vith concomitant shifts in apparent targetelevation, after removal of pris*m, that are specific toeach eye (Ebenholtz, 1978). Another common condition isinduced asymmetric convergence or shift in lateral gaze.Both of these conditions lead to adaptation in gatedirection during the experience (training) followed by aperiod of resdaptation in which the individual isreturned to the normal environment. Adaptation inlateral gaze also leads to a change in apparent &at*direction and a shift in the Lateral orientation ofobjects. Still another type of adaptation results fromleft and right suctained head orientation. For example,maintaining a 30 deg head rotation to one side for about8-10 minutes may cause the subject to make an error (inthe direction of the sustained position) when attemptingto orient the head straight ahead and in describing thespatial orientation of objects.
At a theoretical level, these types of adaptationsmay be thought of as representing a resetting of theset-point or steady-state level of certain reflexes.The "doll reflex," for example, refers to the tendencyof the eyes to roll downward And the eyelids to closewhen the head is rotated backwards (Ebenholtz andShehilske, 1975). Conscious attempts to counter thedol. reflex will, over time, lead to adaptation of theresponse (ShebiLske and Karmichl, 1978), resuLting in achange in both eye level and perceptual effects thatinclude a change tn the apparent elevation of h visualtarget. It is as though the gain of the system ismodified and a new resting Level established. This Isan example of an adaptation in an otolith-dependertsystem, and it is interesting that merely sustainedposture in the presence of a visual target is sufficientfc adaptation in this oculomotor control system.
In each of thes tosl it is nesgative feedbackloop that operates to null error signals and thusmaintain normal postural and oculomotor control in theface of perturbations of reflexive origin. On thisbasis we may be able to understand more clearly themeaning of the conflict theory of motion sickness, interms of the processing of error signals in feedbackloops in the nervous system. Ver example, one way ofthinking about conflict is to consider it a demand for
i'~

35
change, i.e., an error signal in a negative feedbackcontrol system acting as a command to an adaptivenervous system to change its parameters.
The study of oculomotor function provides odditionalexcellent examples of adaptive control systems. Thus,the resting level of vergence (phoria) shifts over time,and distance perception changes, as a result of main-taining fixation on a near target (Ebenholtz and Fisher,1982) or from wearing prisms that induce a change invergence (Schor, 1979). Pnother closely related adaptivesystem is that involved with the control of focus orblur. In this case, the resting level of accommodationis modulated by maintaining focus on a near or far
target (Ebenholtz, 1983). Presumably, the longer anindividual stays focused on the target, the more likelyis the tonus of the ciliary muscle to change, modifyingthe resting level or dark focus of accommodation(Leibowftz and Owens, 1978). This is a feedforvard typeof control that complements the more widely understoodnegative feedback blur-control loop. The veraence andaccommodation systems are represented in Figure 4, inwhich tonus control represents the adaptive feedforwardloops, to which we are now referring.
There is a reciprocal relationship between these twotypes of control loops, and in the case of convergenceand accommodation, they differ in their time constants,one (feedback) being on the order of 100-500 ms and theother (feedforward) capable of lasting for hours. Thisis a situation that could be described as functionalsymbiosis between a feedback and an adaptive feedforwardloop. To the extent that the feedforward loop (tonuscontrol) is successful, it takes the load off thenegative feedback (blur or disparity) control loop. Butthe feedforward system is not "intelligent"; it crn onlybe updated when an error exists in the negative feedbackloop--hence the symbiotic nature of the Telationshipbetween the two control loops.
This symbiotic relationship between feedforward andfeedback loops probably underlies adaptive plasticity.Updating the feedforward systems by changing theirset-points allows them to be more effective, which, inturn, allows :he error detecting feedback controlsystems to relax.
In unpublished studies of the resting state ofconvergence and accommodation, it was found that theaftereffects were functions of exposure duration and themagnitude of the change demanded of the feedforward
'i I- .III-. - I ll II~I I . II I I I IIl 1 i i •

36
FOR + C +.~
anoosl +
FIGURE 4 Vergence and Accommodation Control Systems
Note: C: controller; A/C: accomm3dative convergence;
C/A: convergence-induced accommodation.
Source: Ebenholtz and Fisher (1982).
loop. These variables may &lso be critical for the timecourse (retention) of the aftereffects that occur withvisual simulation systems.
Perhaps the single most significant adaptive controlsystem for the simulator sickness problem is thevestibulo-ocular reflex (VOR). This is a compensatoryocular response that maintains the direction of gaze,enabling one to fix on a visual target wh•le moving thehead. It has no feedback loop of its own respondingprimarily to radial accelerative forces, but it doesreceive the benefits of feedbock from other sources,such as the optokinetic, pursuit, and vergence systems(e.g., Post and Leibowitz, 1982). Dove prisms haveoften been used to reverse the VOR, making it appear,before adaptation, that the world turns with you, but attwice the head velocity. Motion sickness almostinvariably occurs with this procedure, both when theprisms are initially worn and again after adaptation,vhen the prisms are removed and normal viewing isrestored.
I

37
Adaptation of the direction en4 gain of the VOR hasbeen reported in several studies sing diffuprentprocedures (Callan and Ebenholtz, 1982; Giutnier andRobinson, 1975; Melvill Jones, 1977; Kiles and Fuller,1974). The symptoms of motion uickneen thst so commonlyoccur in studies of adaptation of the VOR that theremust be strong clues for understanding simulatorsickness. We may be looking at the same problem,stemming from plasticity in oculomotor control systcms,that can be induced experimentally e: in a simulator,
When the VOl is manipulated experimentally, a heacmovement produces a "slip" in the target image relativeto the tracking eye, rather than saintenance cf gare.This slip of the optokinetic stimulus represents theerror signal that the oculomotor contol system triee toeliminate, leading to a change in the feedforward signalthat controls the direction and velocity of the VOR.This error signal may also be the neurological basis forconflict leading to the symptoms of motion sickness.Figure 5 displays the course of gain changes anddirectional plasticity in the VOR in vector diagramsrepresenting the circumstances that initiate theadaptive response and those that resul• after adaptationhas occurred. The diagram also permits the predictionof the direction of movement illusions that typicallyaccompany VOR adaptations (Dubois, 1982).
Robinson (1976) has studied the physiological basisfor adaptive plasticity in the VOR on the premise thatan incoming velocity gradient, an optoiinetic stifulus,is an important source of information that updates theVOR. The vestibular cerebellum (the flocculus) may be aregion in which incoming visual information could performthe updating function. In support of this, ablationstudies with cats have shown that flocculectomyeliminates the ability to adapt the VCR.
Under stroboscopic illumination, exposure to right/left reversing prisms produced some plasticity in theVOa but the gain was greatly reduced over that obtainedwith steady illumination, according to a study by ?elvillJones and Mandl (1979). Note, however, that nausea,which normally accompanies this type of adaptation, wasabsent. This supports the view that the velocity of theslip signal is important to the magnitude of theadaptation, since intermittent stimulation lowers thenumber of discrepant signals per unit time that thesystem is forced to cope with. This concept leads tothe suggestion that we may be able to reduce the motion
-- xi iil

38
icIi *i I i
aIF
4wd
£IF
T 111 ia lt

39
0
C:0
16~
04 C
-. 4 E
V. 0
0 6d
r. S..w0 40
z~ 0

40
sickness properties of a visual display by reducing thevelocity of the input signals. The update rate would
only have to be sufficient to support the apparentmotion desired in the display.
These adaptations all seem to require an errorsignal. The plastic changes occur as a negative feed-back system responds to this error (slip) signal.Exercising the VOR feedforward loop by itse., hr-vever,
is not sufficient to permit either initial adal....ion orreadaptat'on back to "normal" levels.
The principle thL .*erges is that the very functionof adaptation is to eliminate or reduce the load on theclosed-loop feedback system by substituting a properlyupdated (adapted) feedforward signal. The evidence
suggests that recurrent, systematic directional errorsin negative feedback loops tend to generate adaptiveresponses in the associated feedforward loops. Theseadaptive shifts, in turn, serve to reduce the errors inthe associated negative feedback loops. In short,negative feedback loops serve as the updating system for
the feedforvard loops.Unresolved and systematic errors in negative feedback
loops are not well tolerated by organisms. Thesesignals, in addition to calling forth an adaptive
feedforward responsP, also cause eye strain, dizzintss,apparent motion, disorientation, and motion sickrtsfs.It follows fro, this hypothesis that the conflictsspecified by the sensory conflict theory may be
isomorphic with the conditions that produce sustainederrors in negative feedback loops governing posturalcontrol.
There is strong ncurophysiological evidence for theinteraction between visual and vestibular inputs at thevestibular nucleus (Waespe and Henn, 1977; Daunton andThomsen, 1979). It supports the notion that the visual
stimulus modulates the output of the vestibular nucleus.If this output is modulated beyond some level, thesymptoms of motion sickness are likely to occur.
Simulator sickness is visual stimulation producingnausea. According to the Treisman (1977) hypothesis and
the supporting studies by Money, visual stimulationactivates the vestibular mechanisms that normallyfacilitate the emetic response to poisons. There isprobably also an adaptive response leading to a changein the gain, phase, and direction of the VOa and othervestibular-spinal reflexes.
The vestibular system, including the vestibular

41
nuclei and the vestibular cerebellum, have, as oneessential function, the control of muscle tonus. Thiseixtends to the extraocular muscles and the controL ofeye movements, driving the -uscles that contribute tohead positioning, and those that contribute to theantigravity reflexes. This implies that it iscritically important to identify the relationshipbetween the stimuli (visual, vestibular, andproprioceptive) and the reflexes mediated by thevestibular system. If we can specify these stimuli(inputs) in the flight simulator, and the resultantmotor responses, we will also have gone a long waytoward defining and measuring conflict. If one canmeasure the linear and angular acceleration vectors thatare operating instantaneously, then one can attempt tocorrelate them with the direction and magnitude of theoptokinetic vector at that same time. The comparison ofthose two vectors could be a measure of conflict and ofthe !ikelihood either of ensuing adaptation or simulatorsickness. This is at least a testable hypothesis,which, if supported, cutld lead to the development ofeffective cl-untermeasures. This is of specialimportance, since one of the problems with the conflicttheory is that it is too general to be tested.
As a final observation, it should be noted that
substantial individual differences exist i"susceptibility to the various forms of ocv.onotoradaptations, includina VOR plasticity. The relationshipbetween these potential indices an4 -.- asures of symptomson exposure to flight simulators remains to bedetermined.
Comments on Theories of Motion Sickness
By whatever name it is known--neural mismatch, cueconflict, perceptual decorrelation, or sensoryincongruity--sensory conflict theory is the most commonexplanation for motion sickness. It postulates areferencing function in which motion information fromvision, the vestibular system, and proprioception may bein conflict with the expected values of these inputs,based on a neural store that reflects past experience(Kennedy and Frank, 1983; Reason, 1978). (For a summaryof sensory conflict theory applied to simulatorsickness, see Kennedy and Frank, 1983.)
Althoug:i sensory conflict theory often seeme

42
explanatory after the fact, it is not sufficientlydefined to enable us to make predictions about themagnitude of the conflict in various dynamic situations.Several types of conflict seem to apply: betweensensory modalities (i.e., visual-vestibular), vithin asensory system (i.e., otolith-canal or ambient-focal);or between expected and experienced patterns of notionstimulation. Furthermore, it has been suggested (Benson,1978) that phase and gain parameters of various sensorysystems may play a role in the magnitude of the corflict.This implies that the conflict cannot be precisely
defined based on the physical (distal) stimulusproperties, but must also incorporcte the characteristicsof the sensory transducers, vhich are subject tovariation.
Conflict theory does not explain why sickness failsto occur in certain situations with apparent conflict,and, conversely, it does not clearly predict sickness incertain situations such as vertical linear oscillationin which sickness has been observed (O'ilanlon andMcCauley, 1974).
Despite the deficiencies of sensory conflict theory,it is accepted by oset researchers as a good workinghypothesis for m'tion sickness, and it is in accord withmuch of the data. The questions it raises are valuablechallenges for imrovLng the state of the theory.

RECOK4XENDED COUNTERMEASURES FOR EXISTING SIMULATORS
As we can see from the current stote of knowledge, agreat deal still remains to be learned about the effectsof simulator sickness. At the same time, simulators arean effective training device and the simulators currentlyin use will be operational for some time. Thus animportant immediate goal is to find ways for users tocope with the adverse effects of simulator sickness.
The workshop participants felt that simplyrecommending directions for basic research on thefundamental mechanisms was not adequate. They discusseda number of hypotheses for ameliorating simulator sick-ness in current simulators and generated a preliminarylist of suggested countermeasures (see Table 3, whichaugments a list suggested earlier by Frank et a.1.1983). Although these countermeasures remain to bevalidated, this tentative list can be the source of adhoc solutions to the practical problems..
Freeze. Although freeze can be a valuableinstructional feature in a simulator, it can also bevery diset.tucerting if used indiscriminately. freeze inan off-horizon situation, i.e., 30 degrees win& down, isnot good procedure. Aaecdotal evidence suggests thatwhen a fixed-base simulator is frozen end the pilot isasked to exit, some pilots will refuse to get out.Others crawl out very carefully, feeling that they mayfall, even when they know it is a fixed-bast system. Iffreeze is used judiciously it should eliminate somefeelings of diacomfort without reducing the trainingvalue of the freeze feature.
43

two
44
TABLE 3 Recommended Countermeasure* for CurrentSimulators
Judicious use of freeze and resetAvoid prolonged and intensive exposureRemove scene content before entering or exitingTune/calibrate visual and inertial lagsAvoid motion at a frequency of 0.2 H&briefing pilots on likelihood of symptomsPreadaptation and incremental exposure"Post-simulator visual-motor SamesSyllabus/scenario solutions (reduce maneuvers):
Turns-while-taxiingHish-accaleration maneuversInversion or steep turns
Reduce scenario turbulence
Check personal and medical statusAvoid large head movementsAutogenic feedback therapy (biofeedback)Notion-sickness medication
Reset. The reset function usually is used inconjunction with freeze. After the freeze or at the endof some scenario, the instructor say decide to initiatea new scenario by pressing the reset button. The pilotmay see many miles of video stream by, perhaps backward,within a second or two. This can be very disconcertingand sometimes disorienting to the pilot. The screenshould be blanked or the pilot should close his eyesvhen the reset function is used.
Exposure Duration. The data generally indicate thatexposure duration contributes to sickness. LUmitingexposure duration can provide temporary relief frombuilding symptoms. The recommendation to limit exposureduration and intensity is related to the "incrementalexposure" suggestion.
Maneuver tuteonaty. On the basis of experiences inthe SAAC and anecdotal information, the number andintensity of flight maneuvers in a sioulatov sessionappears to be related to simulator sickness. The high

45
incidence of symptoms in the SAAC occurred when thepilots were flying 35 air combat maneuvering engagements
in daily two-hour sessions.
Viiual Scene Termination. At the end of a sgnarioor a simulation session, the visual scene should beremoved before the pilot is asked to leave the simulator.
Tho visual scene should also be off when the pilotenters the simulator.
Viiual and Inertial Lags. Periodic checks ot theviý;iial and inertial lags are recommended. Even if they
net specifications during icceptance testing, they
shoL-d be checked and calibrated regularly.
Motion Spectrum. Research has indicated that whole-
body motion at a frequency of about 0.2 Hz is the mostnauseogenic. For motion-based simulators, sickness may
be less likely if the simulator motion at that frequencycan te reduced.
Briefing. Providing a briefing for pilots who are
unfamiliar with the simulator can be helpful byindicating that the experience of symptoms is not anabnormal reaction. Giving them knowledge about thesyndrome reduces the anxiety that sometimes accompaniesthe development of unexpected symptoms.
Preadaptation and Incremental Exposure. Researchhas shown that tolerance to head movements duringrotation can be developed by a series of exposures at an
acceleration level low enough to avoid symptoms. Thisto'chnique of incremental oxposure also may be effective
for simulator sickness.
Visual-Motor Games. There is some evidence thatactive body movement facilitates readaptation to anormal inertial environment. Playing a name like ping
pong that involves hand-eye coordination and bodymovement could help speed recovery from simulator
aftereffects.
Syllabus Planning. The dose effect in simulatorsickness is probably related to the frequency andintensity of flight maneuvers and the duration of thesirmulated mission. Planning the training syllabus toreduce the dose (especially in the f&rat few days)
should reduce the incidence of symptoms.

46
Scenario Turbulence. In some simulators, turbulenceis an instructional variable. Avoiding high turbulencelevels is recommended when problems of simulator sick-ness are anticipated (i.e., with on experienced pilotwho has a mild case of flu and has not flown in thesimulator for an extended period of time).
Personal Health Status. Hangover, flu shots, etc.can contribute to an individual's susceptibility tosimulator sickness, and should be avoided prior to"flying" a simulator. (Chewing tobacco also is notrecommended.)
Reduce Head Movement. Large, rapid head movementsduring angular motion can cause vestibular corioliseffects, and head movements during visually represented
angular motion can cause pseudocoriolis effects. Both ofthe effects are excellent stimuli for motion sickness.Excessive head movement is not recommended in an environ-ment in which there is either actual motion or visuallyimplied motion effects. A motion-base simulator hasboth.
Autogenic Feedback Therapy. Research at NASA-Amesand the Air Force School of Aviation Medicine has foundautogenic feedback therapy (biofeedback) to be effectivein the redIuction of motion sickness symptoms in pro-vocative laboratory tests.
Medication. Many medications have been applied formotion sickness; some quite successfully. Flightsurgeons can recommend medication to reduce symptomswithout interfering significantly with performance.
No firm data exist on the effects of simulatorsickness or its aftereffects on the probability ofdisorientation during flight. A pilot suffering fromsimulator sickness, however, is a likely candidate fordisorientation in flight and should exercise caution ----until the effects have subsided. For most people thisis likely to take I or 2 hours, but for others theeffects are intermittent and have been reported as much
Inas 10 hours after an intense AC&4 simulator session(Kellogg et al., 1980).
The operational commands should become aware of theproblem of simulator sickness. In one case, for twoNavy simulators, a rule was established that pilot*

47
could not fly an aircraft for 12 hours after their firstexposure to the simulator; that rule has been relaxedover the last year or so, but the problem of simulatorsickness remains. A "12 hour no fly" rule way not bewarranted in the absence of supporting data, if such arule plays havoc with scheduling of the simulator or th~eaircraft. Some countermeasures will clearly be morepractical than others in the context of operations andflight training.

RECc12•EvDATIONS FC1 RESEARCH
Numerous topics for research surfaced in the three daysof the workshop. At this stage there are more questionsthan answers about simulator sickness. In this sectionwe attempt to surzmarize the -any research suggestionsthat were generated by the participants. Although thelimitations of the workshop precluded our givingpriorities to the many research suggestions, they arecategorized here by objective:
1. Problem Definition2. Theory/Model Development3. 1!ethodology
4. Determination of Causes and Processes5. Validation of Candidate Countermeasures
Problem Definition
1.1 How extensive is the simulator sicknessproblem? The magnitude and consequences of simulatorsickness must be determined in order to make reasonablerecommendations about solutions. Field studies of theincidence of the problem are needed. (The NavelTraining Equipment Center plans to undertake such astudy in 1934.)
1.2 A coordinated survey of all military flightsimulators should be conducted usin3 a standardizedquestionnaire. Co:mprehensive results should becompiled, listing the precipitating causes and resultantsymptoms. To ensurt coniidentiality, the results ofsuch a questionnaire should be compiled by an agency,
48
//

ago
49
such as NASA, that does not represent a threat to thepilots and air crew who respond.
Theory/Model Development
2.1 The sensory conflict theory presents a goodstarting point for the study and understanding ofsimulator sickness. Simulator designers need the typeof information that can be communicated in a good model.However, in order to be really helpful, the terms willhave to be reduced to mathematical statements of thenature and extent of the conflicts that cause theproblem. Such i mathematical representation (e.g., Oman,1980) will help make the theory testable and will guidethe necessary research.
2.2 Sensory conflict theory in its present formdoes not satisfactorily address the coherence orpredictability of the sensory mismatch. It is likelythat adaptation occurs only in response to predictablesensory mismatches. We need to know more about bothsickness and adaptation as a function of thepredictability of the sensory conflict.
2.3 We shvuld beLable to quantify the conflict ifwe have accurate measures of the acceleration impartedto the head and compare thar vector with the vectorrequired by the motion pattern implied by the simulatorvisual system. The difference between these two vectorswould represent a good first approximation to thequantification of theisensory conflict. Using reflexiveresponses such as the vestibulo-ocular reflex (VOR),would sake predictions possible about the outcome ofvisual and vestibularivectors, and the discrepancybetween the actual and predicted VOR could be consideredan index of the mismatch.
Some workshop participants suggested that the VOR
approach may be impractical in a simulator environment,in which the visual display is very complex, pilot headmovement is complex, and there are many more variablesthan in the laboratory.
Other researchers caution that phase relationshipsof various sensory processes can lead to peculiareffects. Even if the amplitudes of visual and vestibularinputs ore eqjal, sensory mismatch can result from phasedifferencis in the to sensory systems. This makes itdifficult to quantify the conflict on the basis of theexternal dynamics alone.
a:' .- ____-_____ I_____I ___________________E____

50
Quantification of sensory conflict i. a majorresearch goal for the study of simulator sickness.
Methodology
3.1 Because the simulator sickness problem involvesso many variables (see the appendix for a sumary list),consideration should be given to using efficient researchmethods such as economical multifactur designs (Simon,1979). We should determine the variables with theireatest poe.eitial payoff and investigate them first.
j.2 The reliability nf the dependent measures ofsimulator sickness need to be investigated. With whatconsistency do the symptoms of simulator sickness occurin individuals? If there is considerable fluctuation inan individual's motion sickness response system, thereliability of the criterion measures may be, say, r -
0.5. We need to develop reliable criteria for effectiveanalysis of the problem.
3.3 Physiological indices of motion sickness shouldbe investigated. It vas well established, however, thatpeople tend to have idiosyncratic patterns of symptomdevelopment. The possibility of developing individualprofiles of symptom development should be investigated.
3.4 Individual differences are important and shouldbe accounted for in any comprehensive model of simulatorsickness. There are larte individual differences in rollvection, for example, and also apparently in simulatorsickness, yet we have no data on their correlations. Weshould seek to predict susceptibility to simulator sick-ness in individuals on the basis of knovledge of othersensory processes.
3.5 The gain of the VOR may be a good measure ofsimulator aftereffects and adaptation. The use of theVOR would require the development of techniques tomeasure pilots' head and eye movements accurately in asimulator; some researchers suggest that it may beimpractical to obtain such measures. The feeiibility ofobtaining accurate measures of the visual scene and thepilots' head and eye movement in a simulationenvironment should be determined.
3.6 Measurement of the motion in the visual sceneis not straightforvard, particularly translationalmovement. What is the proper measure of the visualstimulus? There is the physical motion on the screenand there is the implied (porceived) motion of the pilot.

Ma
for exam.ple, a lateral-quick-atop maneuver at twodifferent altitudes may involve the same perceived bodymotion by the pilot but different notion metrics on thescreen. Perceived distance may be an important variablethat relates displayed motion and perceived body-motion.
Determination of Causes and Processes
4.1 A task analysis is needed to index the tasksbeing performed in the simulator relative to theincidence of simulator sickness. The visual componentsof the task may be important as vell as pilot workloadand flight maneuvers.
4.2 Head movement analysis is needed. An exampleof a complete record of head and eye movements during asimulator session is needed to determine head/eyecoordination and its relationship to the visual displaysystem. Also, patterns of head and eye movements ofexperienced and inexperienced pilots should be analyzedboth in the simulator and in the aircraft for variousmaneuvers. Experienced pilots may have establishedpatterns of head movements in the aircraft that areinappropriate for particular simulator dynamics.
4.3 The most direct approach to investigatingsimulator sickness would be to manipulate the visualdisplay variablhs and the motion-base variables in asimulator. A rejearch simulator that enabled thesevariables to be changed easily would be needed. Visualsystem FOY and scene detail, for example, could bestudied in combination with verious lags and distortionsof the motion base, all with a variety of simulatedairctift maneuvers. Such a research simulator couldalso support study of the efficacy of candidatecountermeasures.
4.4 The contribution of other sources of motioninformation, such as G-seats and helmet-loaders, needsto be studied. How is this information integrated intothe pilot's perception of spatial orientation and bodydynamics? Do these devices contribute to simulatorsickness? Could they contribute to prevention?
4.5 Is there an optimal FOV, large enough to enablepositive transfer of training from the simulator to theaircraft, but small enough to reduce the incidence ofsimulator sickness?
4.6 Nor* information is needed about the phase andgain relationship of the various sensory processes
/

52
involved. for example, if the otolith response is phaseadvanced at a frequency of C.2 Hz but vision is not,this could be the basis for conflict, at least in somecases.
4.7 More basic research is needed on vection. Theeffects on vection of leads and lags in the visual andinertial systems should be investigated. For example,is visual motion most provocative in the same frequencydomain (less than 0.5 HO) as real motion?
4.8 Certain oculomotor variables should beinvestigated for their contribution to simulator sick-ness, such as distance to the display, convergence, andaccommodation. Simulator displays should not inadver-tently encourage convergence and accommodation to driftapart.
4.9 To understand the simulator sickness phenomenon,we need to know the underlying neurological mechanisms,frow, the retina to the vomiting center. The vestibularnuclei and the cerebellum may be of particular impor-tance, particularly their role in motion perception andsensory conflicts.
4.10 We need to know more about ''v visusl O..Itoninfluences the vestibular system. Dia work of Waespeand Henn (1977) should be extended.
4.11 Would labyrinthine defectives (LDs) be immuneto simulator sickness •--tn confronted by a strong movingvisual environment? This information would underscorethe essential role of the vestibular system in simulatorsickness and support the notion that simulator sicknessis s subset of motion sickness.
4.12 The study of as4ptation is essential forunderstanding simulator sickness. Some aftereffectsseem to be transitory and intermittent, while othersseem to be continuous and dissipating. The time courseof adaptation and readaptation with periodic exposuresis an important unknown. Similarly, the transfer ofadaptation between the simulator and the aircraft isunknown. These phenomena must be understood to supportrecomendations that could affect flight safety, such asthe minimum times between exposure and flight. Much ofour understanding of these processes has come from basicresearct. Perhaps more applied research would befruitful in the area of adaptation to real and visuallyimplied motion.
, i

53
Evaluation of Candidate Countermeasuros
5.1 Incremental exposure regimens (Graybiel et a&.,
1969) could be developed if we could establish a range
of severity of the conditions that contribute to
simulator sickness. Susceptible individuals could be"preadapted" before being exposed to the most severe
conditions, such as intensive ACH engagements.
5.2 Active controllers and passive observers maydiffer in their probability of experiencing sickness(McGuinness et at., lq81) and in their rate ofadaptation (Reason and Benson, 1978; Guedry and Benson,1983). Research on these differences in active andpassive roles could contribute to our knowledge of theetiology of simulator sickness and tu strategies for
reducing it.
5.3 Field of view is sugg.-ated as a primary factor
in sinklator sickness. More information is needed on
the relationship betveen FOV and sickness. If the
incidence of sickness robe steeply beyond some value of
1'OV, there would be support for guidelines f3;o FOV in
simulation. A related concept is to increase FOV over
repeated exposures as adaptation is developed. Thesepossibilities should be explored in research.
5.4 Simulator exposure probably involves a
recalibration of the sensorimotor processes, followed byanother period of recalibration upon removal from thesimulation. Certain hand-eye coordiration games, likeping pong, might facilitate this recalibration process.They also would be useful from a motivational standpoint.
5.5 Medications ured for motion sickness might beeffective in the prevention of simulator sicknewa.
5.6 The velocity of the optokinetic stimulus on the
simulator display is a very useful variable because itrepresents the mAgnitude of the stimulus to adapt.Stroboscopic illumination of such a "slip signal"eliminates the motion sickness symptoms that accompanyoptokinetically induced nausea (Mtlvill Jones and Kandl,1979). This seems to offer reasonable hope thatdegrading the update rate of moving stimuli in\ thesimulator display might be sufficient to supporttraining while eliminating simulator sickness.\Advocating degraded update rates, however, appears to becounter to engineering advancements. Further work ineeded to define simulator specifications in terms of"the destree perceptual effects rather than engiseeringadvances for physical realism.
I\

APPENDIXPOTENTIAL CONTRIPUTORS TO SIMULATOR SICKNESS
Characteristics of simulators and users that must beconsidered as potential contributors to simulatorsickness:
INDEPENDENT VARIABLES
Motion and vibrationAxesFrequencyAccelerationExposure durationLagsPhase/gain
VisionField of viewFraming offectRetinal eccentricityOff-axis displayScene features
NumberAppearance
Display typeModel boardComputer-generated imageryPoint source
Pilot head movement
55
/

56
Visual motionLagsPh me /ga inOptometric propertiesSpatial frequencyRaster scanPhosphoresi aRefresh rateVelocityTemporal frequencyLi ear/angular acceleration vectorsSpectral densityDistortion (temporal and spatial)Coillimat ionMagnificationAl ianing
Simulator featuresMotion base/fixed base
Visual system
m~otion systemOther motion cueing systems
Doeversus vindowDnmcmodeling of aircraft
Gsahelmet-loader, anti-G-suit
FrequencyAmplitudeDuration
Turns-whi ic-taxiing
Simulator usefreezeReset
Dissolve scenesWarning signals
Cont roller/passengerTask loadingindoctrinationlBrief ing/demonstrationBuffet

57
Ii iviYlual differencesExperience/@kill level
AircraftSimulator
Field dependence/independenceAttitude (set)Medical statusMotion sickness susceptibility
DEPENDENT VARIABLES
Motion sickness symptomatologyObjective (signs)Subjective (symptoms)
Performance
Flashbacks
Postural disequilibrium (ataxia and other balancemeasures)
Eye movement (and vestibulo-ocular reflex)
OTHER ISSUES
AdaptationTime courseSpecificityTransfer of adaptation
Dual (multiple) adaptationPositive/negative transfer
Active/passive
Transfer of trainingPositive/negativeFlight safety
Sensory conflict identificationVisual-vestibularOtolith-canalIntravisual (fo:al-ambient)Somatosensory-other (G-seat)Multiple sources of conflictSpatial/temporal conflictConflict with neural storeMeasurement (magnitude) of conflictSignlfic.nce of conflict
~ .. ,.~- . . . - -- -. . -

REFERENCES
Barrett, G.V., and Thornton, C.L.1968 Relationship betveen perceptual style and
simulator sickness. Journal of AppliedPsychology 52(4)304-308.
Benson, A.J.1978 Motion sickness. In G. Dhenin and J
Ernstinx. ads., Aviation Medicine. Physiologyand H Factors, Volume 1. London: Tri-MedBooks Ltd.
Callan, J.W., and Ebenholts, S.M.1982 Directional changes in the vestibular ocular
response as a result of adaptation to opticaltilt. Vision Research 22:37-42.
Casali, J.G., and Wierville, W.W.1980 The effects of various design alternatives on
moving-base criving simulator discomfort.Human Factors 22(6)741-756.
Collevijn, H., Martins, A.J., and Steinman, R.N.1981 Natural retinal image motion: origin and
change in vestibular and oculomotorphysiology. In B. Cohen, ad., Annals of NeyYork Academy of Sciences 374. New York: NevYork Academy of Sciences.
Crampton, G.H., and Young, F.A.1953 The differential effect of a rotary visual
field on susceptibles and non-susceptibles tomotior sickness. Journal of Comparative andPhysiological Psychology 46(6):451-453.
59
P" i niiM,,11•a ,nw4 -IM
-Poll.::..

60
Crane, D.F.1983 Compensation for time delay in flight
simulator visual-display syptems.AIAA-83-1080. AIAA Flight SimulationCouference, Niagra falls, N.Y*
Crosby, T.N., and Kennedy, R.S.1982 Postural Disequilibrium and Simulator Sickness
Folloving flights in a P3-C Operational FlightTrainer. Paper presented at the 53rd AnnualScientific Meeting of the Aerospace MedicalAssociation, Bal Harbor, Fla., May.
Dichgans, J., and Brandt, T.1973 Optokinetic motion sickness as pseudo-coriolis
effect induced by moving visual stimuli. Act&Oto-Laryngologica 76:-339-348.
Daunton, N., and Thomsen, D.1979 Visual modulation of otolith-dependent units
in cat vestibular nuclei. Experimental BrainResearch 37:173-176.
Dubois, P.H.1982 Effect of Vestibulo-Ocular Retraining on
Object Position Constancy: Prediction byVector Analysis. M.S. thesis, Department ofPsychology, University of Wisconsin.
Ebenholtz, S.M.1978 Aftereffects of sustained vertical
divergence: induced vertical phoria andillusory target height. Perception 7:305-314.
1983 Accomeodative hysteresis: a precursor forinduced myopia? Investigative Ophthalmologyand Visual Science 24:513-515.
Ebenholtz, S.M., and Fisher, S.K.1982 Distance adaptation depends upon plasticity in
the oculomotor control system. Perception andPsychophy3ics 31: 551-560.
Ebenholtz, S.M., and Shebilske, W.L.1975 The doll reflex: ocular counterrolling vith
head-body tilt in the median plane. "isionResearch 15:713-717.
Frank, L.H.1981 Simulator Sickness. Invited address, NASA
Ames Research Center, Moffett Field, Calif.,August.

61
I
Frank, L.H., and Crosby, T.N.1982 Psychophysiological Disturbances in the
2FI17A, CH-46A WST (Memorandum N-712:LHF).Human Factors Laboratory, Naval TrainingEquipment Center, Orlando, Fla.
Frank, L.H., Kennedy, R.S., McCauley, M.E., and Kellogg,R.S.
1983 Simulator sickness: reaction to a transformedperceptual world. I. Scope of the Problem.NAVTRAEQUIPCEN TN-65. Naval TrainingEquipment Center, Orlando, Fla.
Fregly, A.R.1974 Vestibular ataxia and its measurement in man.
Pp. 321-26G in H.H. Kornhuber, ed., Handbookof Sensory Physiology, Vol. 6/2. Berlin:Springer-Verlag.
Gauthier, G.M., and Robinson, D.A.1975 Adaptation of the human vestibulo-ocular
reflex to magnifying lenses. Brain Research92:331-335.
Gonshor, A., and Melvill Jones, G.1976 Extreme vestibular-oculomotor adaptation
induced by prolonged optical reversal ofvision. Journal of Physiology 256:381-414.
Graybiel, A., Deane, F.R., and Colehour, J.K.1969 Prevention of overt motion sickness by
incremental exposure to otherwise highlystressful Coriolis accelerations. AerospaceMedicine 40:142-148.
G-aybitel, A., Kennedy, R.S., Knoblock, E.C., Guedry,F.!., Jr., Merts, W., Mc.eod, M.E., Colehour, J.K.,Miller, R.I., II, Fregly, A.R.
1965 Effects of *xposure to a rotating environment(10 rpm) on four aviators fcr a period of
twelve days. Aerospace Medicine 36(8):733-754.Guedr7 .. Jr.65 F.Orentation of the rotation-axis relative to
gravity: its influence on nystagnus and thesensation of rotation. Act& Oto-Laryngologica60:30-48.
1978 Visual counteraction of nauseogenic anddisorienting effects of some whole-bodymotions--a proposed mechanism. Aviation
Space and Environmental Medicine 49(1):36-41.
2I
r•r
tdk
/

62
Guedry, F.E., Jr., and Benson, A.J.1978 Coriolis cross-coupling effects: disorienting
and nauseogenic or not? Aviation,_Space andEnvironmental Medicine 49 (l)29-35.
1983 Modification of pre- and post-rotationalresponses by voluntary motor activity of thelimbs. Experimental Brain Rsa-arch 52:190-198.
Hartman, B.O.1976 Report on field study--SAAC Simulator at Luke
APB, Arizona.. Staff study report. USAFSchool of Aerospace Medicine, Brooks AFB, Tex.
Havron, M.D., and Butler, L.F.1957 Evaluation of Training Effectiveness of the
2FH2 Helicopter Flight Trainer Research Tool.Technical Report NAVTRADEVCEN 1915-00-I.Naval !raining Device Center, Port Washir.;ta,N.Y.
Henn, V., Young, L.R., and Finley, C.1974 Vestibular nucleus units in alert monkeys are
41lso influenced by moving visual fields.
Experimental Brain Research 71:144-149.Homick, J.L., ed.
1982 Space Motion Sickness. JSC 18681. Workshopproceedings, NASA Johnson Space Center,Houston, Tax., June 21-22.
James, W.1882 The sense of dizziness in deaf-mutes.
American Journal of Otology 4(4)239-254.Kellogg, L.S., Castors, C.H., and Coward, R.E.
1980 Psychophysiological Effects of Training in aFull Vision Simulator. Paper presented atannual meeting of the Aerospace MedicalAssociation, Anaheim, Calif., May 12-15.
Kennedy, 1.5., and Frank, L.R.1983 A Review of Motion Sickness With Special
Reference to Simulator Sickness. Paperprepared for distribution at the NAS/NRCCommittee on Human Factor* Workshop onSimulator Sickness, Monterey, Calif.,September 26-28.
Kennedy, R.S., Frank, L.H., and McCauley, M.E.1983 Simulator Sickness: Reaction to a Transformed
Perceptual World. IL. Sourcebook andSuggestions for Research. Orlando, Fla.:Naval Training Equipment Center.
___ __/_ .

63
Kennedy, R.S., Graybiel, A., McDonough, R.C., and
Beckvith, F.D.1968 Symptomatology under storm conditions in the
North Atlantic in control subjects and inpersons with bilateral labyrinthine defects.Act& Oto-Laryngologica 66:533-540.
Leibowitz, H.W., and Owens, D.A.1978 New evidence for the intermediate position of
relaxed accommodation. DocumentsOphthalmologica 46:123-147.
Leibovitz, H.W., and Post, R.B.1982 Two modes of processing concept and some
implications. Pp. 343-363 in J. Beck, ed.,Organization and Repres-ntation inPerception. Hillsdale, N.J.: LawrenceErlbaum.
Leibowitz, L.W., Post, R.B., Brandt, T.H., and Dichdans,J.
1982 Implications of recent developments in dynamicspatial orientations and visual resolutionsfot vehicle guidance. Pp. 231-260 in A.
Werthein, W. Wagenaar, and H.W. Leibovitz,feds., Tutorials in Motion Perception. NewYork: Plenum Press.
McCauley, M.E., and Kennedy, 1.S.1976 Recommended Human Exposure Limits for Very Lov
Frequency Vibration (TP-76-36). PacificMissile Test Center, Pt. Mugu, Calif.
McGuiness, J., Bouwman, J.H., and Forbes, J.H.1981 Simulator Sickness Occurrences in the 2E6 Air
Combat Maneuvering Simulator (ACMS).Technical Report NAVTRAEQUIPCEN80-C-0135-4500-1. Naval Training EquipmentCenter, Orlando, Fla.
Melvill Jones, G.1974 Adaptive neurobiology in space flight. In The
Proceedings of the Skylab Life SciencesSymposium, Volume 2, JSC 09275 NASATMKX-58154. Houston: Johnson Space FlightCenter, National Aeronautics and SpaceAdministration.
1977 Plasticity in the adult vestibulo-ocularreflex arc. Philosophical Transactions of theRoyal Society of London B.278:319-334.
Melvill Jones, G., and Mandl, G.1979 Effects of strobe light on adaptation of
vestibulo-ocular reflex (VOR) to visionreversai. brain ,ui~arch ,64:300-303:
I ~ I ?'r|I

64
Miles, V.A., and Fuller, J.H.1974 Adaptive plasticity in the vestidulo-ocular
responses of the rhesus monkey. BrainResearch 80:512-516.
Miller, J.W., and Goodson, J.E.1958 A note concerning "motion sickness" in the
2-F2-H Hover Trainer. Research Project NM1701 11: Subtask 3; Report 1. Naval Schoolof Aviation Medicine, Pensacola, Fla.
1960 Motion sickness in a helicopter simulator.Aerospace Medicine 31:204-212.
Money, K.E.1970 Motion sickness. Physiological Reviews
50(l):1-39.1980 Flight simulator motion sickness in the Aurora
CP 140 FOS. Technical Communication No.80-C-44. Defence and Civil Inatitute ofEnvironmental Medicine, Dovnsview, Ont.
Money, K.E., and Cheung, B.S.1983 Another function of the inner ear:
facilitation of the emetic response topoisons. Aviation, Space and EnvironmentalMedicine (March):208-211.
Nicogousian, A.E.$ and Parker, J.F., eds.1982 Space Physiology and Medicine. NASA SP-447.
Washington, D.C.: National Aeronautics andSpace Administration.
O'Hanlon, J.F., and McCauley, M.E.
1974 Motion sickness incidence as a function of thefrequency and acceleration of a verticalsinusoidal motion. Aerospace Medicine45(4)366-369.
Oman, C.M.1980 A heuristic mathematical model for the
dynamics of sensory conflict and motionsickness. Report No. MVT-80-1. Man-VehicleLaboratnry, Center for Space Research,Massachusetts Institute of Technology.
Post, 1.B., and Leibowitz,-,.W.
1982 The effect of convergence on the vestibularocular reflex and implications for perceivedm~ovement.! Vision Research 22:461-465.
Puig, J.A.1970 Motion in ilight Training: A Human Factors
View. NAVTRADEVCEN 1H-177. Naval TrainingDevice Center, Orlando, Fla.
w

65
1971 The sensory interaction of visual and motioncues. In Commemorative Technical JournalLNTDC 25th Anniversary. Naval Training DeviceCenter, Orlando, ?la.
Reason, J.T.1978 Motion sickness adaptation: a neural mismatch
model. Journal of the Royal Society ofMedicine 71:819-829.
Reason, J.T., and Benson, A.J.1978 Voluntary movement control and adaptation to
cross-coupled stimulation. Aviation, Spaceand Environmental Medicine 49:1275-1280.
Reason, J.T., and Brand, J.J.1975 Motion Sickness. New York: Academic Press.
Reason, J.T., and Dist, E.1971 Simulator sickness in passive observers
(FPRC/1310). London: Flying PersonnelResearch Committee, Winistry of Defense.
Ricard, G.L., Norman, D.A., and Collyer, S.C.1976 Compensating for flight simulator CGI system
delays. Presented at the 9th NTEC/IndustryConference, Orlando, Fla.
Ricard, G.L., and Puig, J.A.1977 Delay of visual feedback in aircraft
simulators. Applied Psychology 59:2250-2258.Robinson, D.A.
1976 Adaptive gain control of the vestibulo-ocularreflex by the cerebellum. Journal ofNeurophysiology 39:954-969.
Schor, C.M.1979 The influence of rapid prism adaptation upon
fixation disparity. Vision Research19:757-765.
Seevers, J.A., and Makinney, R.L.
1979 Simulator for air-to-air combat motion systemS~investigation. AFHRL-TR-79-18. Air ForceHuman Resources Laboratory, Brooks AFB, Tex.
Semple, C.A., Hennessy, R.T., Sanders, X.S., Cross,S.K., Beith, B.H., and McCauley, M.E.
1980 Aircrew training devicea: fidelity features.AFHRL-TR-80-36. Air Force Human ResourcesLaboratory, Brooks AFB, Tex.
Shebilske, W.L., and Karmichl, C.M.1978 Illusory visual direction during and after
backward head tilts. Perception and?sychophysics 24-:'543-545.
1~7

66
Simon, C.W.1979 Applications of Advanced Experimental
Methodologies to AWAVS Training Research.Technical Report. Naval Training EquipmentCenter, Orlando, Fla.
Sinacori, J.G.1967 V/STOL ground-based simulation techniques.
USAAVLABS Technical Report No. 67-55. ArmyAviation Material Laboratories, Fort
Treisman, M. E
1977 Motion sickness: an evolutionaryhypothesis. Science 197:493-495.
U.S. Department of Defense1981 Human Engineering Design Criteria for
Military Systems, Equipment, andFacilities. KILSTD 1472C. Washington, D.C.
Waespe, W., and Henn, V.1977 Neuronal activities in the vestibular
nuclei of the alert monkey duringvestibular and optokinetic stimulation.Experimental Brain Research 27:523-538.
1978 Conflicting visual-vestibular stimulationand vestibular nucleus activity in alertmonkeys. Experimental Brain Research33:203-211.

REPORT DOCUMENTATION PAaE 51V053 COMPL9TING F0011
* 9
L1 A~~~~~~b- Aqg 3 14 ?9e @9ae.?Y'3@ O~
Research Isasues In Simulator Sickness: Technical Reportcon
Proceedings of a Workshop a '5e9Qv*fo"44 ofpo.riveoj~g
Michael E. McCauley. editor N0O0i4-81-C-0017
C071031its.e on Human Facttris 4 eO u..SiNational Research Council Work Unit No. 11R196-167Weiohinaon.9C D.. C.a 20418a ses oCC" Twn.11ln Psychoog -4o1n Octbe 1980911
Of~ic* of Naval Researcho Is *geeo"* of 1`e:
a IV.~Ia5*4W C ~..0.2a wet- ft c-lt OF*- is nfl "'CL" W a.11
Brooks All, Texas, the Army Rsssae,ý.n Institute field Wnt. Fort Rucker.Alabama. and the U. S. Naval Tr. .. ing Equipment Center, Orlando, Floridas.
;m1 ltuitrc -1 ' mn Ja ct.frsvz sercfthSimuatio / Human Engineering Research
--!*btion Sickneses / C¶jisibular,So ensory bn f I Ict) rT ) 2loSimulatsor Sickness CowALirtoee" MAMAe Factora
A. Iss Iace I -n. - ,bi. . It --... .. g 1~fr 1. 6 ..
JýSimulator sicknes41. ai t h symptoms similar to mtion sickness, occursfrequently in military and civilian flight trainers. ilmiuaetor sicknessappears to be independent of whether a fixed bass or moving base simulator
*ia used. ?4stho.In foi amelioration are described as swell an recommnsdations
for futut. 7seaoaich t de lop coaunts ronenures. re.
DO ,'~,,14 I OCno.a a:. Old wax 1a Unclassifiled
111 100le I I.~I S~fiyC~amamse a 54 i. m

A i 7i
a~L4,,
R, A








![Afa Advisor Presentation[1]](https://img.pdfslide.us/doc/110x75/55891a03d8b42af47c8b4598/afa-advisor-presentation1.jpg)