Embed Size (px)
Citation preview

AETIOLOGY AND CLASSIFICATION
OF MALOCCLUSION
Rav GovenderBChD; MFDS RCS Edin.; MSc. Lond.; MORTH RCS Eng.

Learning objectives
• CLASSIFICATION
• AETIOLOGY Skeletal Factors Soft Tissue Factors, often not recognised Dental factors Habits Iatrogenic Factors / local
Case Discussions

Complex interactions among multiple factors that influence growth and development.
AETIOLOGYComplex multifactorial
Genetically determined, both local and skeletal factors eg. class III, a skeletal factor and hypodontia a local factor are both genetically determined.Specific genetic syndromes, Pierre Robin or acromegaly
Environmental factors / Trauma, Local

CLASSIFICATION
• British standards institute OR BSI• Angle’s classification• Andrews classification
The British standards institute is based on the incisor relationship.
Angle’s and Andrews classification is based on the molars relationship.
• Dental
• Skeletal
Dental

BSI
The overjet should be 2-4mm with a vertical overlap of one third of the crown of the lower incisors.


Classification by molar relationship
Andrew
Angle
A. The distal surface of the upper first molar occludes with the mesiobuccal cusp of the lower second permanent molar ANDREW
B. The mesiobuccal cusp of the upper first permanent molar occludes with t he buccal groove of the lower first permanent molar. ANGLE
C. Half class IID. Full unit class II

Canine classification
Class II
CLASS I

CLASSIFICATION
SKELETAL: Antero-posterior
vertical
Transverse
Mild moderate and severeIn 3 planes
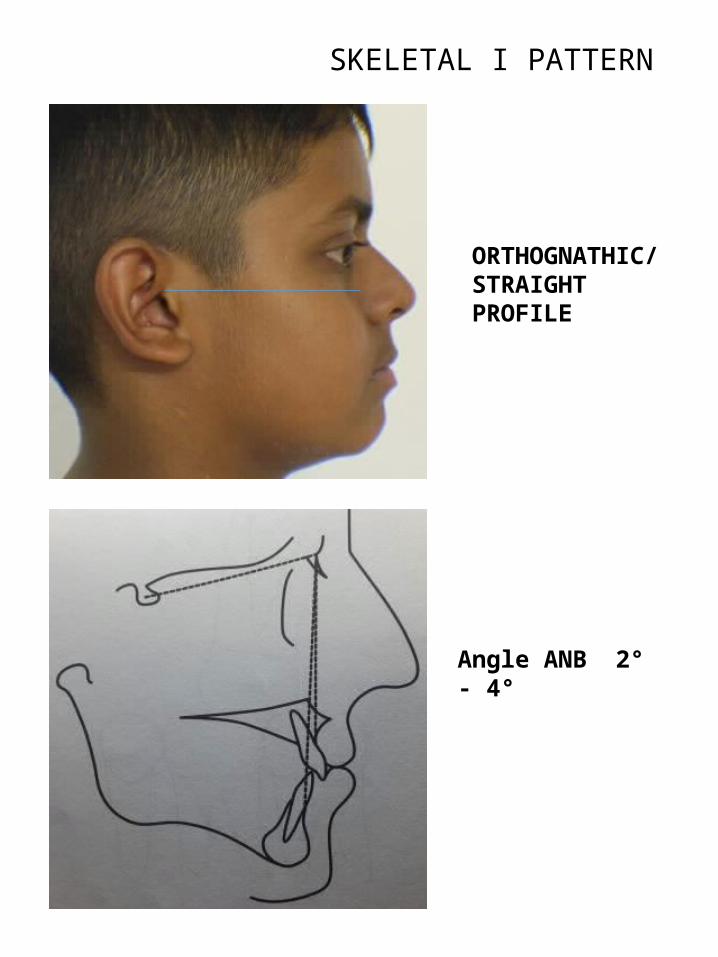
SKELETAL I PATTERN
ORTHOGNATHIC/STRAIGHT PROFILE
Angle ANB 2° - 4°

SKELETAL II PATTERN
CONCAVE PROFILE
ANB EXCEEDS 4°

SKELETAL II
Usually due to mandibular retrognathia.Ceph. Study By Mc Namara et. al.
Class II is not a single entity, But mandibular skeletal retrusion most common.
Small % is maxillary protrusion
Almost half the sample had excessive vertical dimension.

CLASS II INCISOR RELATIONSHIP
These diagrams show how partial reduction of the overjet does not allow the lip to cover the upper incisors.
The upper incisors will return to their pre-treatment position.

SKELETAL III PATTERN
CONVEX PROFILE
ANB LESS THAN 2°

SKELETAL III
Caused by maxillary deficiency and /or mandibular prognathism.
Definitive familial and racial tendency for mandibular prognathism.
Maxillary deficiency not clear, but environmental factors unlikely.
Hapsburg jaws. Royal Family in Spain that ruled around 1660
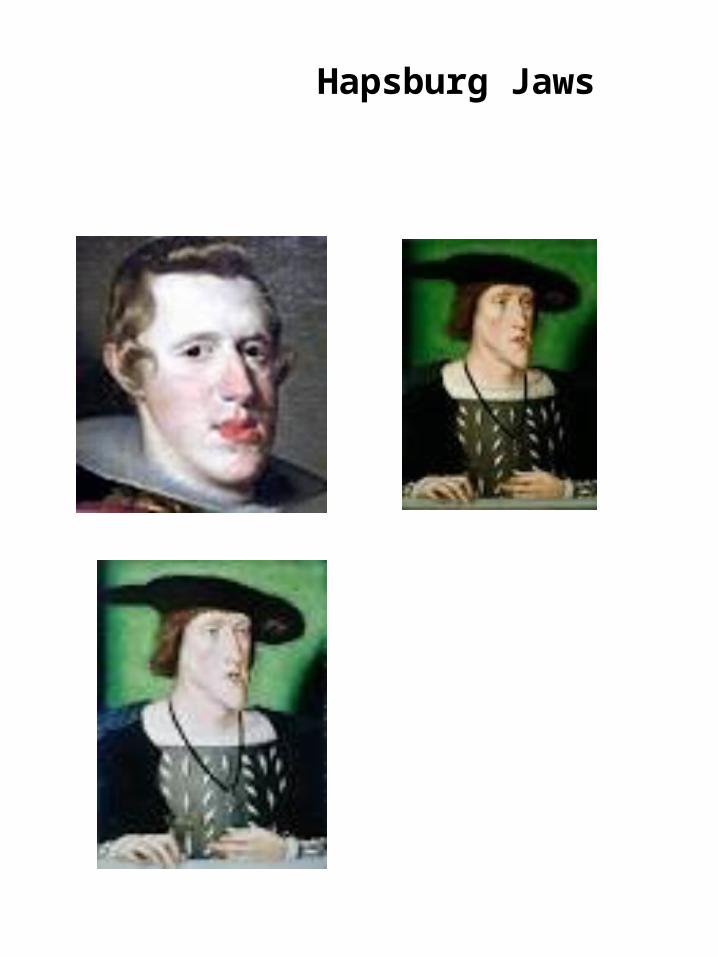
Hapsburg Jaws

• Class I the mandible is 2 -3 mm posterior to the maxilla
• Class II the mandible is retrusive relative to the maxilla
• Class III the mandible is protrusive relative to the maxilla

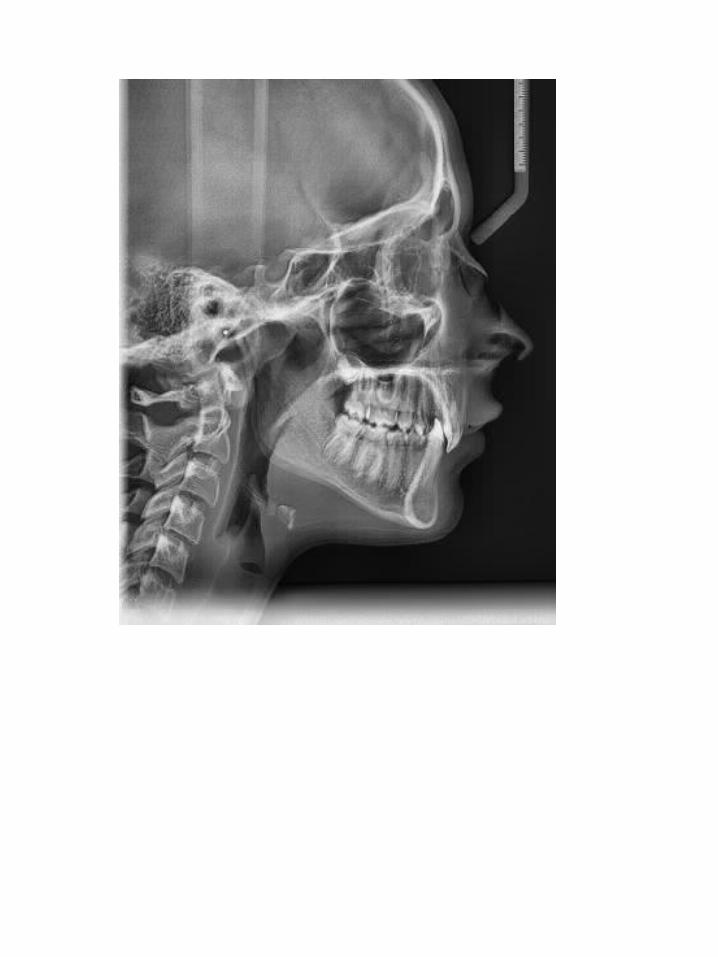
CLASSIFICATION
Vertical assessment, Inherited
Assessment of lower facial height. The distance x from a point between the eyebrows to the base of the nose is equivalent to the distance y from the base of the nose to the chin.
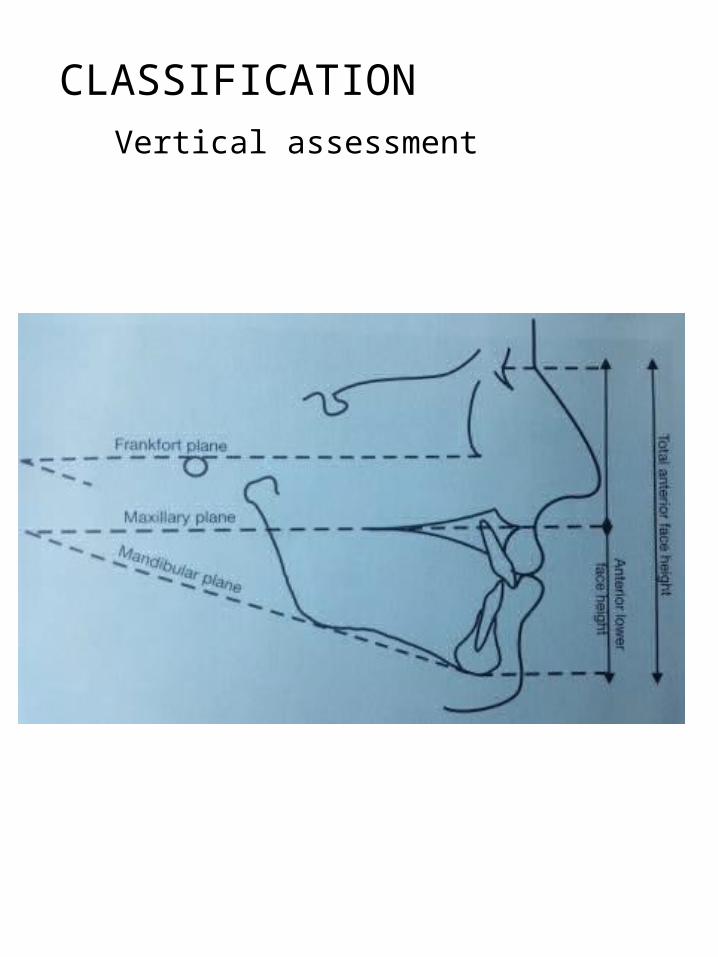
CLASSIFICATION
Vertical assessment

CLASSIFICATION
Frontal view, assess the vertical and transverse discrepancy.
Vertical skeletal assessment

Vertical assessment Factors that influence and increase the vertical dimension.
Increased vertical dimension: AOBThumb sucking habit
Partial nasal obstruction. Harvold study, Lopatiene et.al Lithuanian study. ( 7- 15 Yr s).
The main characteristics of the respiratory obstruction syndrome
hypertrophied tonsils or adenoids,
mouth breathing,
open-bite, cross-bite,
excessive anterior face height,
incompetent lip posture,
increased upper incisor show
narrow external nares,
"V" shaped maxillary arch

Vertical assessment Long face syndrome
Vertical growth pattern
Increased LAFH
Downward rotation of the mandible (clockwise rotation)
Excessive eruption of molars leading to AOB
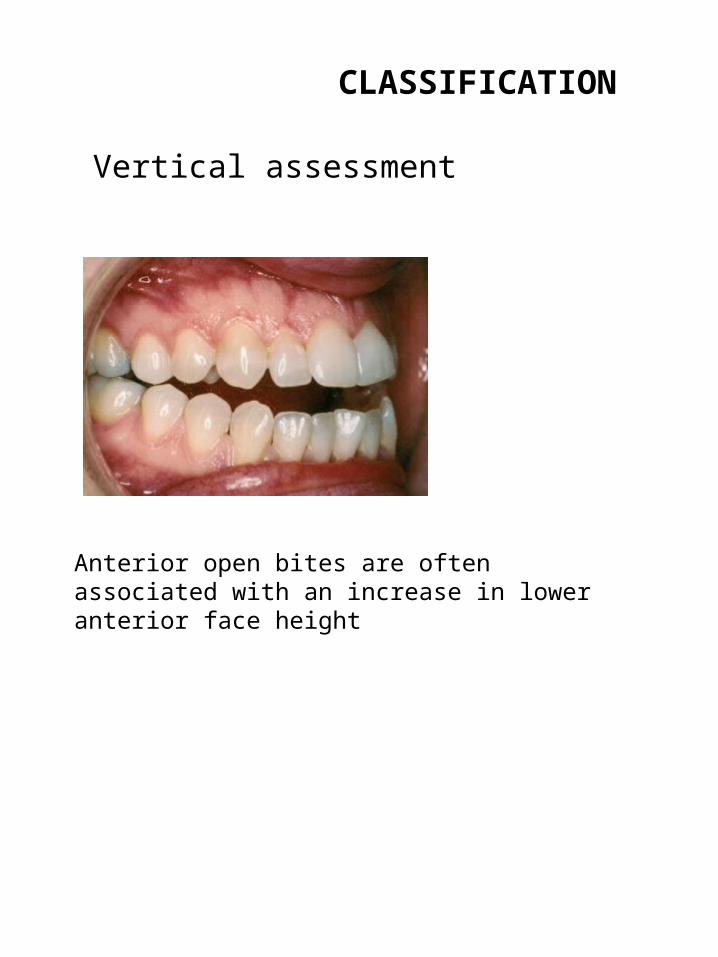
CLASSIFICATION
Vertical assessment
Anterior open bites are often associated with an increase in lower anterior face height

CLASSIFICATIONVertical assessment
Profile of a patient with a much reduced lower anterior facial height.
Compare with long face syndrome

Low angle patient /short face syndrome
Horizontal growth patternIncreased overbiteDecreased LAFHUpward and forward rotation of the mandible, i.e. anticlockwise rotation of the mandible. Increased eruption of the mandibular teeth, i.e. incisors
Both forward and backward growth rotations results in LLS crowding, right until the late thirties. (Bolton Brush Study by Holly Broadbent, 1966)

CLASSIFICATION
Vertical Assessment
The reduced lower anterior face height is often associated with a deep bite as shown

The face is divided into fifths.Middle fifthMedial two fifthsOuter two fifths
Assess from above and behind the patient.(assess facial centre, i.e. mid eye-brow, tip of nose, philtrum of upper lip and chin point should line up
TRANSVERSE ASSESSMENT

Transverse discrepancy
True facial asymmetry Apparent facial asymmetry, associated with crossbite and mandibular displacement.
Intra-orally check for -crossbite and mandibular deviation-scissor bite and “ “Compare mand-maxillary arches for shape and size.
Clinically Dental centre-lines
Check for a cant in the maxillary occlusal plane. ( the patient bites on a tongue spatula and relate to inter-pupillary line).

Asymmetric condylar growth. Deviation of the lower dental midline to the left.Asymmetries are more common in class II and class III malocclusions.
Transverse discrepancy

Intra orally


THE ROLE OF THE SOFT TISSUES,IN THE AETIOLGY OF MALOCCLUSION
LipsTongueFraenumLabio-mental foldNasiolabial angle
LIPSLip competency
Lip lengthLip tonicity (muscular, or flaccid and everted)Degree of protrusion or retrusion,All these factors are related.

THE ROLE OF THE SOFT TISSUES,IN THE AETIOLGY OF MALOCCLUSION
LIPSLip competency,Competent lips can be considered normal and desirable, because
• Aesthetics: incompetent lips in conjunction with a short upper lip can lead to the appearance of the patient showing too much upper incisor tooth and gingival tissue on smiling. (Gummy smile)
• Function: It provides the patient wit lip-to-lip anterior oral seal during swallowing.
• Health: helps prevent gingival drying which can be associated with gingival hyperplasia and gingivitis.

THE ROLE OF THE SOFT TISSUES,IN THE AETIOLGY OF MALOCCLUSION
LIPS
Class II Division IProclined upper incisorsLip trapSTABILITY the upper incisors should be under the control of the lower lip.

THE ROLE OF THE SOFT TISSUES,IN THE AETIOLGY OF MALOCCLUSION
LIPS
Lip incompetence, lips separated at rest by more than 3 – 4 mm.Increased incisal show at restProtrusion of the upper incisorsLip trap, the lower lip rests behind the upper incisors.

THE ROLE OF THE SOFT TISSUES,IN THE AETIOLGY OF MALOCCLUSION
Lips
Incompetent Flaccid and evertedStability
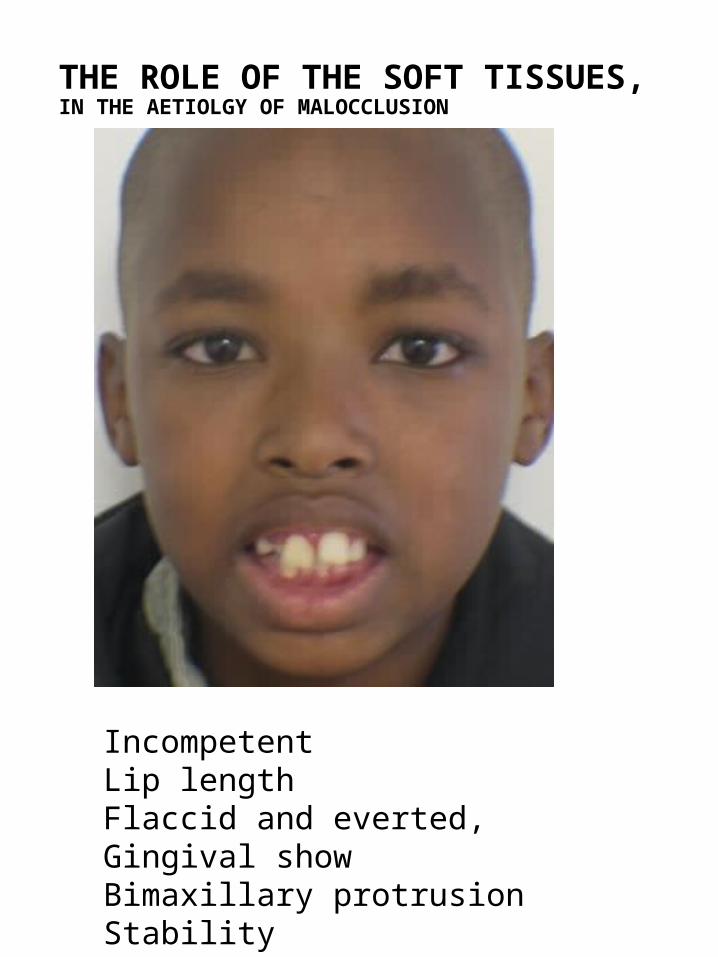
THE ROLE OF THE SOFT TISSUES,IN THE AETIOLGY OF MALOCCLUSION
Incompetent Lip lengthFlaccid and everted,Gingival showBimaxillary protrusionStability

THE ROLE OF THE SOFT TISSUES,IN THE AETIOLGY OF MALOCCLUSION
LIPSThin Strappy lipsClass II Division II

THE ROLE OF THE SOFT TISSUES,IN THE AETIOLOGY OF MALOCCLUSION
Tongue thrust: usually adaptive. The tongue is placed between the teeth to achieve an anterior oral seal.
Endogenous tongue thrust:Rare,On swallowing the tongue is pushed between the upper and lower incisors. Associated with sigmatism (lisping). May also be associated with bimaxillary proclination.
An adaptive tongue thrust will cease when a lip to lip contact can be achieved after treatment.
Tongue Size: Macroglossia

Large Tongue
Tongue interposed between the upper and lower incisors. AOB OF 7MM

Large tongue

LABIOMENTAL FOLD
Indicative of Deep biteReduced lower face height Low mandibular angle



THE INFLUENCE OF THE NASIO-LABIAL FOLD
Retraction of the upper lip is contra-indicatedIn adults consider orthognathic inetervention.

LOCAL FACTORS IN MALOCCLUSION
DEFN: local factors affect one or more adjacent /opposing teeth to produce local disturbances in in dental development.The longer they act more severe the disturbance.
• Variations in tooth number• Abnormalities in tooth position• Labial fraenum• Trauma• Crossbites• Dento-alveolar disproportion.

Variation in tooth Number
Hypodontia, most common upper lateral incisors, lower incisors and lower second premolars.
Supernumery teeth Supplemental , dichotomy of tooth germ. Incisor, premolar (extract the most displaced tooth)
Early conical forming: offshoot of the dental lamina. Develop between upper centrals. Single but more common multiple. Erupts unless inverted. Causes median diastema. Remove if orthodontics is planned.
Late tuberculate forming: thought to represent a third dentition. Develops palatal to 1 / 1, single or multiplePrevents eruption of the incisors

Midline Supernumary
Odontome
Complex: Mix of enamel dentine and cementumMaxillary incisor region Prevents eruption of the incisorsSurgical removal and bond an eruption appliance to align the unerupted incisors.
Compound odontome:Radiopaque mass of tissue, occurs in the mandible or posterior maxilla.

The role of premature loss of primary teeth
The factors that determine the outcome:The tooth lostAge of patientDentoalveolar disproportion, crowding vs spacing.Degree of intercuspationHigh angle v low angle

Management of early loss
•Compensatory extractions- to maintain inter-arch relations.
•Balancing extractions- to maintain centre-line.
•Space maintainers, Advantages and disadvantages.

Prolonged retention of primary teeth /ankylosis
•Tooth fails to maintain its position in the developing occlusion.
More common in the mandible > Ds and Es.Due to,Absence of a successorGenetic,Trauma
Pathogenesis: Ankylosis occurs during the reparative phase of tooth resorption, the tooth fails to erupt and the alveolus continues to grow in some cases enveloping the tooth.

Effects of prolonged retention primary teeth / ankylosis
•Progressive infraocclusion of the primary molar, difficult extraction and lack of alveolar height development.
•The permanent successor if present results in delayed eruption, impaction disturbed root formation/ cystic change
•Tipping and over-eruption of adjacent and opposing teeth and crowding.

Management of infraocclusionFactors to consider before treatment,
•Presence or absence of permanent successor•Degree of infraocclusion•Is there a co-existing malocclusion •Long term prognosis of the primary molar
Treatment options•Decision based on the above factors Interceptive extraction (absent 5) –spontaneous space closureIf there is a malocclusion then orthodontic space closure.Surgical subluxation, break the ankylosisRestorative approach re-establish occlusion

18 15 14 24 25 28 48 45 35 38
Infra-occluding Es are difficult to extract , with minimal damage to alveolus.

Abnormalities in tooth form
•Fusion, the tooth retains separate pulp chambers.
•Gemination, common pulp chamber,
•Dilaceration, angulation between the crown and root.
Requires a joint orthodontic restorative and surgical approach.

Dilaceration

Dilaceration

Abnormalities in tooth position
Most common Maxillary cuspidGeneticLocal and environmental factors
Important clinical signs, POSITION AND FORM OF 2 / 2Guidance theory, (peck and peck)
Interchange in position of two permanent teeth, one of which is almost always a canine.Mx: canine and premolarMd: canine and lateral incisorIncomplete, crown overlap onlyComplete, both crown and apex overley
Genetic and environmentalMigration during normal eruptionLocal pathology. Treatment options:Orthodontic alignment of incomplete transposition.Orthodontic alignment in the transposed position
Transposition

Transposition

Labial fraenum and the midline diastema
70% cases with a midline diastema associated with a large fleshy fraenum attached to the incisive papilla.
Diagnosis: blanching of the incisive papilla on gentle lip retraction. Orthodontic space closure in the absence of fraenectomy has a 84% relapse.
Collagenous fibres of a large fraenum disrupt the normal transeptal fibre system between the 1 /1
Radiographically a V shaped crestal notch between the 1 / 1 is seen.

Treatment
Aim of fraenectomy is to promote the transeptal fibres across the defect.
Timing: Must be after the eruption of the 3 / 3.
Done just prior to orthodontic space closure. The post op. scar contraction across the defect aides stability.
If done after orthodontic space closure, access is limited, and risk of root damage.

Crossbites Discrepancy in arch relation, lateral or sagittal mandibular movement as a result of cuspal interference from CR to CO.
Aetiology:Skeletal V dentalSoft tissueDentoalveolarHabits, digit sucking Why treatAestheticsDental, pain and wearPeriodontal loss of attachmentTMJ riskRisk of developing of a true asymmetry if left untreated during the developmental stage.
Treatment options
Address the problem in the primary dentition
Removable and fixed appliancesSlow expansion v rapid expansion. (RME v quad).Cross arch elastics.Selective grinding of Cs

Role of dental trauma in malocclusion
Damage to permanent tooth germ from an injury to primary tooth.
Type of injury , intrusive v avulsion determines the damage to the successor.
Prior to crown formation < 4yrs disturbance in enamel formation resulting in coronal defect. Later injuries will displace the crown relative to the root resulting in dilaceration and impaction of the permanent successor. Treatment will require SE and bonding an eruption appliance.
Drift of permanent teeth ffg. early loss of primary teeth.
Direct injury of permanent incisor =AvulsionIntrusive injury = Ankylosis

Discussion
Problems,Mobile 41, Gingival recession of 41Deep bite If not corrected 41 will have a poor long term prognosis.

Appliance design
To correct anterior crossbite
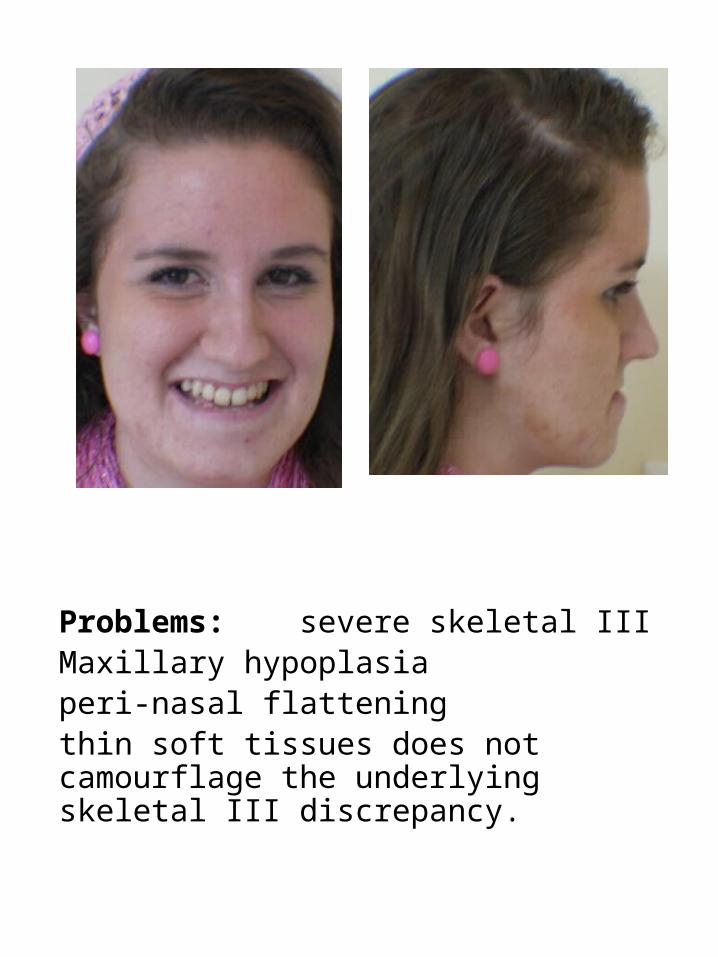
Problems: severe skeletal IIIMaxillary hypoplasiaperi-nasal flatteningthin soft tissues does not camourflage the underlying skeletal III discrepancy.
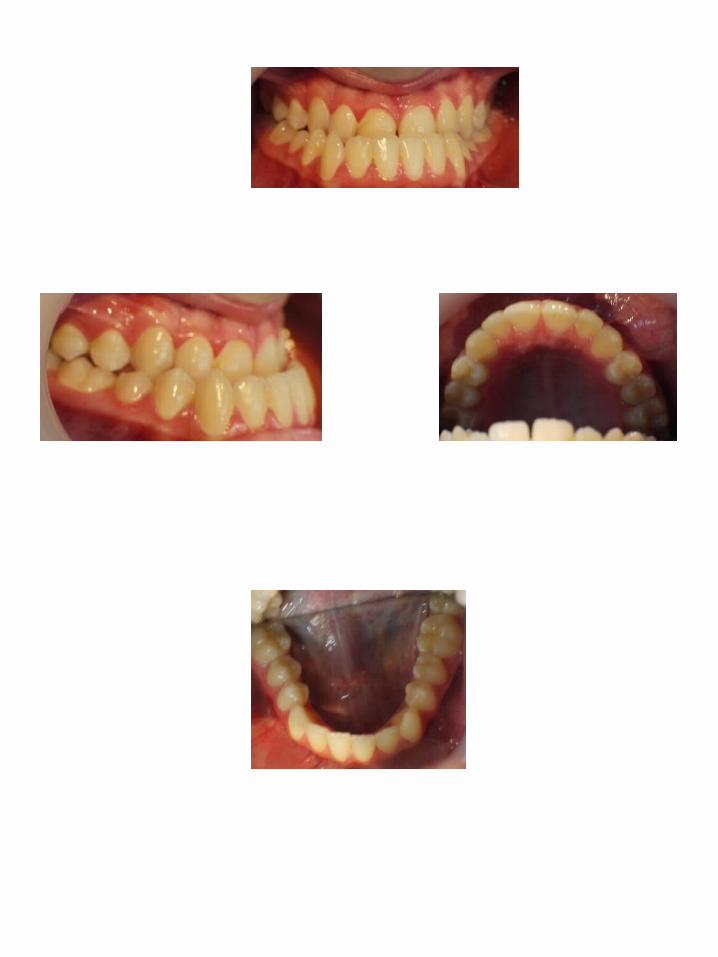






Problems: increased vertical dimension 7mm AOB cuspid to cuspid ms crowded arches bimaxillary proclination 24 crossbite poor rct on 46, guarded prognosis


Steep mandibular plane angleProclinationLip incompetenceIncreased vertical proportionsAOB.Adverse swallowing pattern46 rct

Aims of treatment
Address the crowdingCorrect the crossbiteEstablish an overbite Level and align the arches.
Extraction: 4 4 6 5
Palatal tads to intrude upper buccal segments.


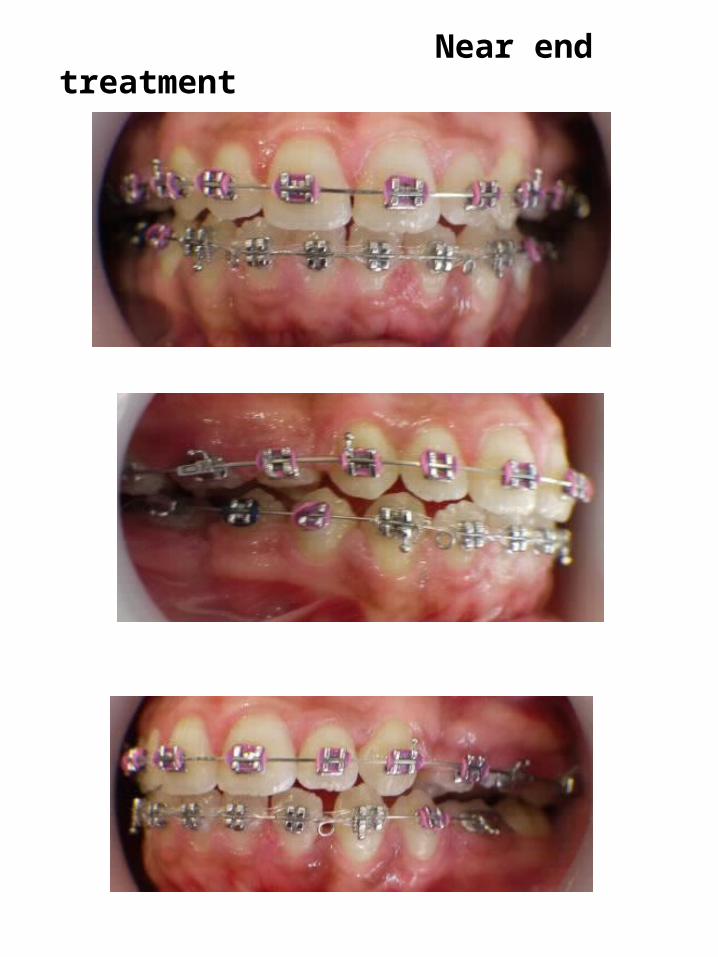
Near end treatment


Questions
1. Ankylosis of a primary tooth can result in (a) in its infra-occlusion. T / F (b) delayed root formation in the permanent successor. T / F (c) cystic change in the permanent successor. (d) None of the above. T /F
2. A dilacerated tooth, (a) has genetic aetiology, T / F (b) environmental aetiology T /F (C) None of the above T / F (b) both of the above T / F
3. A large tongue interposed between the upper and lower incisors. (a) causes an anterior openbite. T / F (b) associated with short face syndrome. T / F (c ) proclination of the incisors. T / F (d) none of the above. T / F

Questions
Deep overbite can be associated with,(a) reduced lower anterior face height. T / F(b) palatal trauma. T / F(c) Stripping of the lower labial gingivae. T / F(d) All of the above. T /F
A severe skeletal III discrepancy,(a) has reverse overjet. T / F(b) Dental compensation for the underlying skeletal III base. T / F(c) Best addressed with joint orthodontic / orthognathic intervention. T / F (d) All of the above. T / F






























