Embed Size (px)
Citation preview

AED Treatment and the Adverse AED Treatment and the Adverse Effects of AEDs in the I/DD PatientEffects of AEDs in the I/DD Patient
Michael C. Smith M.D. Michael C. Smith M.D.
Rush Epilepsy CenterRush Epilepsy Center

EPILEPSYEPILEPSY ININ THETHE MULTIPLYMULTIPLY- - HANDICAPPEDHANDICAPPED
Uneasy reminders of our human fragility
One measure of the humanity of a civilization is its compassion for its most
disadvantaged citizens.

Treatment with AEDsTreatment with AEDs
• Goals of therapyGoals of therapy
- No seizuresNo seizures
- No side effectsNo side effects
- Allow patient to maximize their potentialAllow patient to maximize their potential

Treatment OptionsTreatment Options
• Medications are the primary treatment.Medications are the primary treatment.
- Consider potential side effectsConsider potential side effects
- Consider patients health statusConsider patients health status
- Consider self-management skillsConsider self-management skills
- Consider CostConsider Cost
• Resective surgery may be an optionResective surgery may be an option
• Vagal nerve stimulation is effective in the Vagal nerve stimulation is effective in the MR/DD populationMR/DD population

Principles for Treatment ofPrinciples for Treatment ofEpilepsy in Special PopulationsEpilepsy in Special Populations
• EfficacyEfficacy
- Attempt monotherapy whenever possibleAttempt monotherapy whenever possible
- Agent appropriate for the seizure type(s)Agent appropriate for the seizure type(s)
- Broad spectrum agent when seizure types are mixed or unknownBroad spectrum agent when seizure types are mixed or unknown
- Select an agent that will not exacerbate seizuresSelect an agent that will not exacerbate seizures
- Minimize trough levelsMinimize trough levels
• SafetySafety
- Minimize drug-drug interactionsMinimize drug-drug interactions
- Minimize side effectsMinimize side effects
- Select an agent with known and manageable risksSelect an agent with known and manageable risks
- Select an agent that will not exacerbate other conditionsSelect an agent that will not exacerbate other conditions
• SimplificationSimplification
- Minimize number of agents usedMinimize number of agents used
- Minimize number of daily dosesMinimize number of daily doses
- Simplify medication administration processes and costsSimplify medication administration processes and costs
- Improve quality of lifeImprove quality of life

THE ART OF AED MANAGEMENTTHE ART OF AED MANAGEMENT
• Drug selectionDrug selection
• Introduction & titrationIntroduction & titration
• Clinical monitoringClinical monitoring
• Managing AEsManaging AEs
• Rotating AEDsRotating AEDs
• Transitioning therapiesTransitioning therapies
• Drug reductionDrug reduction
• MonotherapyMonotherapy
Individualizationof therapy

ESTABLISH NEED FOR AED ESTABLISH NEED FOR AED THERAPYTHERAPY
• bonafide seizure episodes bonafide seizure episodes (vs. other causes of LOC)(vs. other causes of LOC)
• verify sz recurrenceverify sz recurrence
• verify sz are non-symptomatic, i.e., not verify sz are non-symptomatic, i.e., not due to a transient causedue to a transient cause
• beware of mimickersbeware of mimickers

Decision on TreatmentDecision on Treatment
• To treat or not to treatTo treat or not to treat
• Goals of therapy – seizure free, no side effectsGoals of therapy – seizure free, no side effects
• MonotherapyMonotherapy
• Rational polypharmacyRational polypharmacy
• When to initiate – discontinue therapyWhen to initiate – discontinue therapy
• AED monitoring AED monitoring
• Patient – re-evaluation – patient not responding as Patient – re-evaluation – patient not responding as expectedexpected

AED SELECTIONAED SELECTION
• overall efficacyoverall efficacy
• efficacy for specific sz types or efficacy for specific sz types or epilepsy syndromesepilepsy syndromes
• efficacy against comorbid conditionsefficacy against comorbid conditions
• interactions with other drugsinteractions with other drugs
• ease of introduction, follow-upease of introduction, follow-up
• drug safetydrug safety
• costcost

AnticonvulsantsAnticonvulsants
• Standard AEDsStandard AEDs
- PhenobarbitolPhenobarbitol
- PhenytoinPhenytoin
- CarbamazepineCarbamazepine
- Divalproex SodiumDivalproex Sodium
• New AEDsNew AEDs
- GabapentinGabapentin
- LamotrigineLamotrigine
- LevetiracetamLevetiracetam
- OxcarbazepineOxcarbazepine
- TiagabineTiagabine
- TopiramateTopiramate
- ZonisamideZonisamide
- FelbamateFelbamate
- PregabalinPregabalin

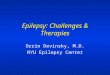
AED Options
TonicTonic Tonic-Tonic-clonicclonic MyoclonicMyoclonic AtonicAtonic Infantile Infantile
SpasmsSpasms AbsenceAbsence
Phenytoin, Carbamazepine, Phenobarbital,
Gabapentin, Tiagabine,
Oxcarbazepine Pregabalin
ACTHTopiramate?Tiagabine?Vigabatrin?
Ethosuximide
Valproate, Lamotrigine, Topiramate, FelbamateZonisamide, Levetiracetam
GeneralizedPartial
SimpleComplex
Secondarily generalized

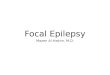
Possible Aggravation ofPossible Aggravation ofSeizures or Epilepsy SyndromesSeizures or Epilepsy Syndromes
CBZCBZ PHTPHT LTGLTG GBPGBP VGBVGB TGBTGB BDZBDZ VPAVPA
AbsenceAbsence ++ ++ ++ ++ ++ ++
MyoclonicMyoclonic ++ ++ ++ ++ ++
Juvenile myoclonic epilepsyJuvenile myoclonic epilepsy ++ ++ ++
Lennox-Gastaut syndromeLennox-Gastaut syndrome ++ ++ ++ ++ ++ ++
Benign epilepsy of childhood Benign epilepsy of childhood with centro-temporal spikeswith centro-temporal spikes
++
Severe myoclonic epilepsy in Severe myoclonic epilepsy in infancyinfancy
++ ++ ++ ++
Landau-Kleffner syndrome/ Landau-Kleffner syndrome/ electrical status epilepticus electrical status epilepticus during slow sleepduring slow sleep
++ ++
CBZ=carbamazepine; PHT=phenytoin; LTG=lamotrigine; GBP=gabapentin; VGB=vigabatrin; TGB=tiagabine; BDZ=benzodiazepine.
Bourgeois BF. Epilepsia. 2003;44(suppl 2):27-32.

NICE:NICE:Drug Options by Epilepsy SyndromeDrug Options by Epilepsy Syndrome
Drug ofDrug of
First ChoiceFirst ChoiceSecondSecond
Choice DrugChoice DrugOtherOther
DrugsDrugsDrugsDrugs
to Avoidto Avoid
Lennox-Lennox-Gastaut Gastaut syndromesyndrome
LamotrigineLamotrigine11
ValproateValproate
TopiramateTopiramate1,21,2
ClobazamClobazam
ClonazepamClonazepam
EthosuximideEthosuximide
LevetiracetamLevetiracetam
FelbamateFelbamate44 CarbamazepineCarbamazepine22
OxcarbazepineOxcarbazepine22
Landau-Landau-Kleffner Kleffner syndromesyndrome
LamotrigineLamotrigine11
ValproateValproate
SteroidsSteroids33
LevetiracetamLevetiracetam
TopiramateTopiramate22
SulthiameSulthiame44 CarbamazepineCarbamazepine22
OxcarbazepineOxcarbazepine22
Myoclonic Myoclonic astatic astatic epilepsyepilepsy
ClobazamClobazam
ClonazepamClonazepam
ValproateValproate
TopiramateTopiramate1,21,2
LamotrigineLamotrigine
LevetiracetamLevetiracetam---- CarbamazepineCarbamazepine22
OxcarbazepineOxcarbazepine22
National Institute of Clinical Excellence. Clinical Guideline 20. October 2004.National Institute of Clinical Excellence. Clinical Guideline 20. October 2004.Available at: http://www.nice.org.uk/CG020.Available at: http://www.nice.org.uk/CG020.
11Should be used as a first choice under circumstances as outlined in the NICE technology of newer AEDs.Should be used as a first choice under circumstances as outlined in the NICE technology of newer AEDs.22Hepatic enzyme-inducing AED.Hepatic enzyme-inducing AED.33Steroids: prednisolone or ACTH.Steroids: prednisolone or ACTH.44Not licensed in the UK, but available by importation.Not licensed in the UK, but available by importation.

LENNOX- GASTAUT SYNDROMELENNOX- GASTAUT SYNDROME
• Childhood onset (age 1-8)Childhood onset (age 1-8)
• High seizure frequencyHigh seizure frequency
• Tonic, atonic, absence, myoclonic, GTC and partial szsTonic, atonic, absence, myoclonic, GTC and partial szs
• EEG: AEEG: Abnormal background, slow s/w (<3cps), often multifocal, bnormal background, slow s/w (<3cps), often multifocal, bursts of 10 hz fast during sleepbursts of 10 hz fast during sleep
• MRMR
• Many patients in LTC facilities and Group Homes are Adult Lennox-Many patients in LTC facilities and Group Homes are Adult Lennox-Gastaut SyndromeGastaut Syndrome

AEDs Useful for Lennox-Gastaut Syndrome and AEDs Useful for Lennox-Gastaut Syndrome and others Seizure Types in I/DD Populationothers Seizure Types in I/DD Population
• ValproateValproate
• FelbamateFelbamate
• LamotrigineLamotrigine
• LevetiracetamLevetiracetam
• ZonisamideZonisamide
• TopiramateTopiramate
• VNSVNS

MONITORING AED THERAPY - MONITORING AED THERAPY - EFFICACYEFFICACY
• use patient calendars to calculate seizure use patient calendars to calculate seizure frequencyfrequency
• calculate seizure index (sz/day)calculate seizure index (sz/day)
• levels are a surrogate for efficacy:levels are a surrogate for efficacy:use for monitoring compliance, changes in use for monitoring compliance, changes in pharmacokineticspharmacokinetics

THERAPEUTIC ENDPOINTSTHERAPEUTIC ENDPOINTS
• introduce slowly if possibleintroduce slowly if possible
• increase dose until seizures controlled or increase dose until seizures controlled or side effects obtainedside effects obtained
• individual response varies greatlyindividual response varies greatly
• individual side effects vary greatlyindividual side effects vary greatly

MANAGING EMERGENT ADVERSE MANAGING EMERGENT ADVERSE EFFECTSEFFECTS
Dose related toxicities (drowsiness, dizziness, Dose related toxicities (drowsiness, dizziness, cognitive impairment, etc)cognitive impairment, etc)
• slow titration rateslow titration rate
• reduce new medicationreduce new medication
• reduce concomitant therapies (reduce total reduce concomitant therapies (reduce total drug load)drug load)

MONITORING AED THERAPY - MONITORING AED THERAPY - TOXICITIESTOXICITIES
• routinely inquire about common side routinely inquire about common side effectseffects
• use open-ended interviewinguse open-ended interviewing
• instruct to call immediately if lethargy, instruct to call immediately if lethargy, nausea, vomiting, ataxia or nausea, vomiting, ataxia or sz sz
• educate caretakers, esp when patient educate caretakers, esp when patient feedback is limitedfeedback is limited
• be sure to examine gait, coordination, be sure to examine gait, coordination, speechspeech

ComplianceCompliance
• Non-compliance – major issue in epilepsyNon-compliance – major issue in epilepsy
• Patients dislike medication and believe they Patients dislike medication and believe they are responsible for cognitive dysfunctionare responsible for cognitive dysfunction
• VA cooperative study – computer chip in VA cooperative study – computer chip in bottle cap gives date/time bottle openedbottle cap gives date/time bottle opened
- Majority missed AEDs; some regularlyMajority missed AEDs; some regularly

WHEN SHOULD AED REGIMENS BE WHEN SHOULD AED REGIMENS BE CHANGED?CHANGED?
• lack of efficacylack of efficacy
• poor tolerationpoor toleration
• pharmacokinetic considerationspharmacokinetic considerations
- dosing issuesdosing issues
- peak dose effectspeak dose effects
- tolerabilitytolerability
- drug interactionsdrug interactions

AED SELECTION AFTER 1AED SELECTION AFTER 1STST FAILURE FAILURE
• Use same criteria as initial selectionUse same criteria as initial selection
• Failure due to lack of efficacy may Failure due to lack of efficacy may reflect refractory epilepsyreflect refractory epilepsy
• ““Rational” polytherapy, i.e., selection Rational” polytherapy, i.e., selection on basis of AED mechanism has never on basis of AED mechanism has never been provenbeen proven

MONOTHERAPY:MONOTHERAPY:DRUG REDUCTION WORKS!DRUG REDUCTION WORKS!
• 44 institutionalized patients with 44 institutionalized patients with intractable CPS, SGTCS or “mixed” szintractable CPS, SGTCS or “mixed” sz
• 4 or 5 AEDs at baseline4 or 5 AEDs at baseline
• reduced to mono- or duo-therapyreduced to mono- or duo-therapy
- CBZ (9%)CBZ (9%)
- PHT (18%)PHT (18%)
- VPA (36%)VPA (36%)
- combination of above (36%)combination of above (36%)
Mirza WU et al. Drug Invest. 5:320-326, 1993

PINECREST STUDYPINECREST STUDYRESULTSRESULTS
• ALL patients had successful reductionsALL patients had successful reductions
• ALL patients had improvements in sz controlALL patients had improvements in sz control
• Transient rise in sz for 1/3 pts on barbituratesTransient rise in sz for 1/3 pts on barbiturates
• Behavior improvedBehavior improved
sz freesz free >50% reduct>50% reduct
monotherapy (n=28)monotherapy (n=28) 13 (46%)13 (46%) 15 (54%)15 (54%)
duotherapyduotherapy (n=16)(n=16)1 (6%)1 (6%)15 (94%)15 (94%)
Mirza WU et al. Drug Invest. 5:320-326, 1993

AED REDUCTION STUDIESAED REDUCTION STUDIES
• Schmidt D.Schmidt D. Reduction of two-drug therapy in intractable epilepsy. Reduction of two-drug therapy in intractable epilepsy. EpilepsiaEpilepsia. 1983;24:368-76.. 1983;24:368-76.
• Clancy RRClancy RR. New anticonvulsants in pediatrics: Carbamazepine and . New anticonvulsants in pediatrics: Carbamazepine and valproate. valproate. Curr Probl PediatrCurr Probl Pediatr. 1987;17:133-209.. 1987;17:133-209.
• Mirza WU, Credeur LJ, Penry JKMirza WU, Credeur LJ, Penry JK. . Results of antiepileptic drug reduction in patients with multiple handicaps and epilepsy. Drug Invest 1993;5:320-6.
• Pellock JM, Hunt PAPellock JM, Hunt PA. A decade of modern epilepsy therapy in . A decade of modern epilepsy therapy in institutionalized mentally retarded patients. institutionalized mentally retarded patients. Epilepsy ResearchEpilepsy Research. .
• Poindexter AR, Berglund JA, Kolstoe PD. Changes in antiepileptic drug prescribing patterns in large institutions: preliminary results of a five-year experience. Am J Ment Retard 1993;98:34-40.

Clinical Use of AEDs in MRDD PatientsClinical Use of AEDs in MRDD Patients
• Serum levels important to compliance, AED Serum levels important to compliance, AED toxicity especially when on multiple AEDstoxicity especially when on multiple AEDs
• Routine blood work not usually helpful in Routine blood work not usually helpful in surveillance of AEs but many centers surveillance of AEs but many centers mandate routine testing in MRDD patientsmandate routine testing in MRDD patients
• Medical remission is goal; disease remission Medical remission is goal; disease remission (seizure free off AEDs is unlikely in patients (seizure free off AEDs is unlikely in patients with significant CNS pathology) while not with significant CNS pathology) while not probable is possibleprobable is possible

Special Considerations in MRDD PatientsSpecial Considerations in MRDD Patients
• Patient may not be able to express complaints Patient may not be able to express complaints about AEDsabout AEDs
• Don’t complain of itching, pain, dizziness and Don’t complain of itching, pain, dizziness and other important subjective symptomsother important subjective symptoms
• Caregiver must be vigilant about change in Caregiver must be vigilant about change in patient wellbeingpatient wellbeing
• Cosmetic side effects can effect the health Cosmetic side effects can effect the health and QOL of patient (gingival hyperplasiaand QOL of patient (gingival hyperplasia

Special Considerations In MRDD PatientsSpecial Considerations In MRDD Patients
• Many MRDD patients are on AEDs for lifeMany MRDD patients are on AEDs for life
• Cosmetic side effects occur only after years Cosmetic side effects occur only after years of AED exposureof AED exposure
• Many MRDD patients are on multiple AEDs Many MRDD patients are on multiple AEDs that lead to toxicity due to drug loadthat lead to toxicity due to drug load
• Some metabolic changes induced by AEDs Some metabolic changes induced by AEDs can lead to serious morbiditycan lead to serious morbidity
-osteoporosis; atherosclerosis-osteoporosis; atherosclerosis

Adverse EffectsAdverse Effects
• Types of Adverse EffectsTypes of Adverse Effects
- Exaggerated pharmacological effect (OD)Exaggerated pharmacological effect (OD)
- AE unrelated to pharmacological effect (other AEs)AE unrelated to pharmacological effect (other AEs)
- Undersirable SE that accompanies primary Undersirable SE that accompanies primary pharmacological effect (CNS AEs of AEDs)pharmacological effect (CNS AEs of AEDs)
- Allergic Reactions ( rash,immune organ dys)Allergic Reactions ( rash,immune organ dys)
- Idiosyncratic Reactions (hepatic ,hematologic)Idiosyncratic Reactions (hepatic ,hematologic)
- Physical DependencePhysical Dependence

CNS AdverseEffectsCNS AdverseEffects
• CNS AEs are dose and drug load dependentCNS AEs are dose and drug load dependent
• High doses-sedation/lethargy,encephalopathyHigh doses-sedation/lethargy,encephalopathy
• Mood change/hyperactivity/psychosisMood change/hyperactivity/psychosis
• Paradoxical sz (Pb,Bz,DPH,CBZ ,new AEDs)Paradoxical sz (Pb,Bz,DPH,CBZ ,new AEDs)
• Classic Cerebellar syndrome w/ DPH,PbClassic Cerebellar syndrome w/ DPH,Pb
• Peripheral neuropathy 10-15% (DPH et al)Peripheral neuropathy 10-15% (DPH et al)
• Diplopia (CBZ,LTG,Pb,Bz)Diplopia (CBZ,LTG,Pb,Bz)

CNS AEs: Established vs New AEDsCNS AEs: Established vs New AEDs
AtaxiaAtaxiaBlurredBlurredVisionVision
CognitiveCognitiveEffectsEffects DizzinessDizziness DrowsinessDrowsiness FatigueFatigue HeadacheHeadache
EstablishedEstablished
CarbamazepineCarbamazepine ++ ++ ++ ++ ++
EthosuximideEthosuximide ++ ++ ++ ++ ++
PhenobarbitalPhenobarbital ++ ++ ++ ++ ++ ++
PhenytoinPhenytoin ++ ++ ++ ++ ++ ++
PrimidonePrimidone ++ ++ ++ ++ ++ ++
ValproateValproate ++ ++ ++ ++
NewNew
FelbamateFelbamate ++ ++ ++ ++
GabapentinGabapentin ++ ++ ++ ++ ++
LamotrigineLamotrigine ++ ++ ++ ++ ++
LevetiracetamLevetiracetam ++ ++ ++
OxcarbazepineOxcarbazepine ++ ++ ++ ++ ++ ++
TiagabineTiagabine ++ ++ ++ ++
TopiramateTopiramate ++ ++ ++
VigabatrinVigabatrin ++ ++ ++ ++ ++
ZonisamideZonisamide ++ ++ ++ ++ ++Chapman DP, et al. South Med J. 1997;90:L171-L180.

Other AEs: Established vs New AEDsOther AEs: Established vs New AEDs
AlopeciaAlopecia HirsutismHirsutism HyponatremiHyponatremiaa
HypersensitivityHypersensitivityKidneyKidneyStonesStones
InducesInducesCyt450Cyt450
EstablishedEstablished
CarbamazepineCarbamazepine ++ ++ ++ ++
EthosuximideEthosuximide ++
PhenobarbitalPhenobarbital ++ ++
PhenytoinPhenytoin ++ ++ ++
PrimidonePrimidone ++ ++
ValproateValproate ++
NewNew
FelbamateFelbamate ++
GabapentinGabapentin
LamotrigineLamotrigine ++
LevetiracetamLevetiracetam
OxcarbazepineOxcarbazepine ++ ++
TiagabineTiagabine
TopiramateTopiramate ++ ++
VigabatrinVigabatrin
ZonisamideZonisamide ++ ++Chapman DP, et al. South Med J. 1997;90:L171-L180.

Dermatologic ReactionsDermatologic Reactions
• Rash: range from mild erythema to life Rash: range from mild erythema to life threatening exfoliative reaction and bullae threatening exfoliative reaction and bullae formation (skin and mucous membranes)formation (skin and mucous membranes)
• Dose-related exanthem most common and Dose-related exanthem most common and responds to dose reduction (CBZ)responds to dose reduction (CBZ)
• Serious drug rash-systemic signs Serious drug rash-systemic signs (fever,myalgia,eosinophilia,lymph nodes)(fever,myalgia,eosinophilia,lymph nodes)
• Exfoliative rxn,erythema multiforme.Lyell Exfoliative rxn,erythema multiforme.Lyell synd,S-J synd: 1-4 wks after drug startssynd,S-J synd: 1-4 wks after drug starts
• Hypertrichosis-DPH,CBZ:Alopecia-VPAHypertrichosis-DPH,CBZ:Alopecia-VPA

Exanthematous Rxn-CBZExanthematous Rxn-CBZ

Steven-Johnson SyndromeSteven-Johnson Syndrome

Mucosal Lesions S-J SyndromeMucosal Lesions S-J Syndrome

GI and Hematologic AEs: GI and Hematologic AEs: Established vs New AEDsEstablished vs New AEDs
GIGIIrritationIrritation AnorexiaAnorexia HepatotoxicityHepatotoxicity
WeightWeightGainGain HematologicHematologic
EstablishedEstablished
CarbamazepineCarbamazepine ++ ++
EthosuximideEthosuximide ++ ++
PhenobarbitalPhenobarbital ++
PhenytoinPhenytoin ++
PrimidonePrimidone
ValproateValproate ++ ++ ++
NewNew
FelbamateFelbamate ++ ++ ++ ++
GabapentinGabapentin ++
LamotrigineLamotrigine ++
LevetiracetamLevetiracetam
OxcarbazepineOxcarbazepine
TiagabineTiagabine ++
TopiramateTopiramate ++
VigabatrinVigabatrin ++
ZonisamideZonisamide ++Chapman DP, et al. South Med J. 1997;90:L171-L180.

HepatotoxicityHepatotoxicity
• Must separate true hepatoxicity from a benign Must separate true hepatoxicity from a benign minor elevation of liver enzymes(5-10%)minor elevation of liver enzymes(5-10%)
• Evaluate synthetic liver function (coagulation Evaluate synthetic liver function (coagulation factors by PT/PTT and albumin level)factors by PT/PTT and albumin level)
• Hepatotoxicity often a component of a Hepatotoxicity often a component of a systemic or allergic reaction (other organs)systemic or allergic reaction (other organs)
• Toxic hepatotoxicity (arene oxide metabolite Toxic hepatotoxicity (arene oxide metabolite in VPA) Felbamate ?in VPA) Felbamate ?
• Hepatotoxicity-n/v,icterus,coagulpoathy Hepatotoxicity-n/v,icterus,coagulpoathy encephalopathyencephalopathy

Hematologic EffectsHematologic Effects
• AEs range from mild hemolytic anemia to life-AEs range from mild hemolytic anemia to life-threatening aplastic anemiathreatening aplastic anemia
• Toxic effects on bone marrow-rareToxic effects on bone marrow-rare
• TE due to hypersensitivity,2’ to lupus-like TE due to hypersensitivity,2’ to lupus-like effect, toxic inhibition of marroweffect, toxic inhibition of marrow
• Aplastic anemia-effects all cell lines Aplastic anemia-effects all cell lines (agranulocytosis then thrombocytopenia)(agranulocytosis then thrombocytopenia)

Common Hematologic EffectsCommon Hematologic Effects
• Carbamazepine : dose-dependent leukopenia-Carbamazepine : dose-dependent leukopenia-granulocytes<1000 (concurrent viral infection)granulocytes<1000 (concurrent viral infection)
• Mild anemia ( many AEDs)Mild anemia ( many AEDs)
• Valproate: dose-dependent thrombocytopenia Valproate: dose-dependent thrombocytopenia platelet ct<50,000.Decrease platelet adhesion platelet ct<50,000.Decrease platelet adhesion even at normal numbers (bleeding time)even at normal numbers (bleeding time)
• Drop in all cell lines require bone marrow Drop in all cell lines require bone marrow exam.(? Repeat CBC)exam.(? Repeat CBC)

Cosmetic and Other AEsCosmetic and Other AEs
• Requires chronic exposure over yearsRequires chronic exposure over years
• Coarsening of facial features-DPHCoarsening of facial features-DPH
• Facial hair in females-DPHFacial hair in females-DPH
• Dupuytren’s contractures-PB/PrimodoneDupuytren’s contractures-PB/Primodone
• Gingival Hyperplasia-DPHGingival Hyperplasia-DPH
• Frozen shoulder-PB/PrimodoneFrozen shoulder-PB/Primodone

Coarsening of Facial FeaturesCoarsening of Facial Features

Dupuytren’s ContractureDupuytren’s Contracture

Plantar Fibroma -phenobarbPlantar Fibroma -phenobarb

Gingival HyperplasiaGingival Hyperplasia

Gingival HyperplasiaGingival Hyperplasia
• Associated with chronic phenytoin use but Associated with chronic phenytoin use but not with other hydantoins (ethotoin)not with other hydantoins (ethotoin)
• Responsible for serious gum disease and Responsible for serious gum disease and tooth decaytooth decay
• Can be improved with vigorous brushing and Can be improved with vigorous brushing and teeth flossingteeth flossing
• May be associated with other disordersMay be associated with other disorders
- myocardial infarction in young associated - myocardial infarction in young associated with chronic gum/tooth infectionwith chronic gum/tooth infection

Bone DiseaseBone Disease
• Osteopenia-P450 inducer (DPH,Pb,CBZ)Osteopenia-P450 inducer (DPH,Pb,CBZ)
• Osteomalacia ?VPAOsteomalacia ?VPA
• Osteopenia 2’ to decreased active Vit DOsteopenia 2’ to decreased active Vit D

Bone Health in Women With Bone Health in Women With EpilepsyEpilepsy
• Greater prevalence of hip osteopenia versus Greater prevalence of hip osteopenia versus normal controls based on agenormal controls based on age
• Significant reductions in vitamin D and IGFBP-3 in Significant reductions in vitamin D and IGFBP-3 in women receiving enzyme-inducing AEDs women receiving enzyme-inducing AEDs
• Enzyme-inducing agents (CBZ and PHT) Enzyme-inducing agents (CBZ and PHT) associated with significant deficits in total hip associated with significant deficits in total hip bone mass density and bone resorption marker, bone mass density and bone resorption marker, respectivelyrespectively
• Lamictal or VPA not associated with deficits in Lamictal or VPA not associated with deficits in bone mass or bone turnover markersbone mass or bone turnover markers
Seale et al, poster presented at AES, Dec 2000

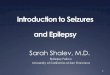
Bone Health Study Results:Bone Health Study Results:Baseline Total Hip Bone Mass Density Baseline Total Hip Bone Mass Density
by AED by AED
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
CBZ LTG PHT VPA
Z S
core
CBZ vs normative controls p<0.0002
Seale et al, poster presented at AES, Dec 2000

Bone Health Study Results:Bone Health Study Results:Baseline Lumbar Spine and Total Hip Baseline Lumbar Spine and Total Hip
Bone Mass DensityBone Mass Density
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
CBZ LTG PHT VPA
Z S
co
re
Seale et al, poster presented at AES, Dec 2000

Treatment of AED-Associated Treatment of AED-Associated Bone DiseaseBone Disease
• Multiple therapies available for bone diseaseMultiple therapies available for bone disease
- Calcium Calcium
- Vitamin D supplementationVitamin D supplementation
- BisphosphonatesBisphosphonates
- Hormone replacementHormone replacement
- CalcitoninCalcitonin
• Few studies evaluating the effect of therapies Few studies evaluating the effect of therapies in AED-associated bone diseasein AED-associated bone disease

Idiosyncratic Drug Reactions: Idiosyncratic Drug Reactions: Conventional WisdomConventional Wisdom
• Possibly life-threateningPossibly life-threatening
• Unpredictable from knowledge of drug’sUnpredictable from knowledge of drug’sbasic pharmacologybasic pharmacology
• Dose-independentDose-independent
• Can involve a wide variety of organsCan involve a wide variety of organs
• Usually appear in first 3 to 6 monthsUsually appear in first 3 to 6 months
• May recurMay recur
• Not reproducible in animal modelsNot reproducible in animal modelsAdapted with permission from Glauser TA. Adapted with permission from Glauser TA. Epilepsia.Epilepsia. 2000;41(suppl 8):S16-S29. 2000;41(suppl 8):S16-S29.

Idiosyncratic Reactions Associated With Idiosyncratic Reactions Associated With Traditional AEDsTraditional AEDs
CBZ=carbamazepine; ESM=ethosuximide; PB=phenobarbital; PHT=phenytoin; VPA=valproic acid.CBZ=carbamazepine; ESM=ethosuximide; PB=phenobarbital; PHT=phenytoin; VPA=valproic acid.
Adapted with permission from Glauser TA. Adapted with permission from Glauser TA. Epilepsia.Epilepsia. 2001;41:S16-S29. 2001;41:S16-S29.
CBZCBZ ESMESM PBPB PHTPHT VPAVPA
AgranulocytosisAgranulocytosis XX XX XX XX XX
Stevens-Johnson syndStevens-Johnson synd XX XX XX XX XX
Aplastic anemiaAplastic anemia XX XX XX XX XX
Hepatic failureHepatic failure XX XX XX XX
Allergic dermatitis/rashAllergic dermatitis/rash XX XX XX XX XX
Serum sickness reactionSerum sickness reaction XX XX XX XX XX
PancreatitisPancreatitis XX XX XX

Idiosyncratic Reactions:New AEDsIdiosyncratic Reactions:New AEDs
Newer AEDs are associated with fewer IDRs than the traditional AEDsNewer AEDs are associated with fewer IDRs than the traditional AEDs
FBM=felbamate; GBP=gabapentin; LTG=lamotrigine; TPM=topiramate; TGB=tiagabine; FBM=felbamate; GBP=gabapentin; LTG=lamotrigine; TPM=topiramate; TGB=tiagabine; OXZ=oxcarbazepine; ZNS=zonisamide.OXZ=oxcarbazepine; ZNS=zonisamide.
Adapted with permission from Glauser TA. Adapted with permission from Glauser TA. Epilepsia.Epilepsia. 2000;41:S16-S29. 2000;41:S16-S29.
FBMFBM GBPGBP LTGLTG TPMTPM TGBTGB OXZOXZ ZNSZNS
AgranulocytosisAgranulocytosis X X
Stevens-Johnson syndromeStevens-Johnson syndrome X X X X
Aplastic anemiaAplastic anemia X X
Hepatic failureHepatic failure X X
Allergic dermatitis/rashAllergic dermatitis/rash X X X X X X X X X X X X
Acute myopia/secondaryAcute myopia/secondaryangle-closure glaucomaangle-closure glaucoma X X

Clinical Profile for Patients at High Risk for Idiosyncratic Reactions Clinical Profile for Patients at High Risk for Idiosyncratic Reactions to Valproic Acid, Felbamate, and Lamotrigineto Valproic Acid, Felbamate, and Lamotrigine
Adapted with permission from Glauser TA. Adapted with permission from Glauser TA. Epilepsia.Epilepsia. 2000;41(suppl 8):S16-S29. 2000;41(suppl 8):S16-S29.
Valproic AcidValproic Acid(Hepatotoxicity)(Hepatotoxicity)
Children under the age ofChildren under the age of2 years2 years
Multiple concomitant AEDs Multiple concomitant AEDs
Underlying metabolic diseaseUnderlying metabolic disease
Developmental delayDevelopmental delay
FelbamateFelbamate(Aplastic anemia)(Aplastic anemia)
CaucasianCaucasian
Adults more than childrenAdults more than children
Females more than malesFemales more than males
Previous cytopeniaPrevious cytopenia
History of an AED allergyHistory of an AED allergyor toxicity or toxicity
History of an autoimmune disorder History of an autoimmune disorder
On felbamate less than 1 yearOn felbamate less than 1 year
Lamotrigine Lamotrigine (Stevens-Johnson syndrome(Stevens-Johnson syndromeor toxic epidermal necrolysis)or toxic epidermal necrolysis)
Children more than adultsChildren more than adults
Concurrent valproic acid useConcurrent valproic acid use
High starting doseHigh starting dose
Rapid titrationRapid titration
On lamotrigine less thanOn lamotrigine less than1 year1 year

CNS AEs: Established vs New AEDsCNS AEs: Established vs New AEDs
AtaxiaAtaxiaBlurredBlurredVisionVision
CognitiveCognitiveEffectsEffects DizzinessDizziness DrowsinessDrowsiness FatigueFatigue HeadacheHeadache
EstablishedEstablished
CarbamazepineCarbamazepine ++ ++ ++ ++ ++
EthosuximideEthosuximide ++ ++ ++ ++ ++
PhenobarbitalPhenobarbital ++ ++ ++ ++ ++ ++
PhenytoinPhenytoin ++ ++ ++ ++ ++ ++
PrimidonePrimidone ++ ++ ++ ++ ++ ++
ValproateValproate ++ ++ ++ ++
NewNew
FelbamateFelbamate ++ ++ ++ ++
GabapentinGabapentin ++ ++ ++ ++ ++
LamotrigineLamotrigine ++ ++ ++ ++ ++
LevetiracetamLevetiracetam ++ ++ ++
OxcarbazepineOxcarbazepine ++ ++ ++ ++ ++ ++
TiagabineTiagabine ++ ++ ++ ++
TopiramateTopiramate ++ ++ ++
VigabatrinVigabatrin ++ ++ ++ ++ ++
ZonisamideZonisamide ++ ++ ++ ++ ++Chapman DP, et al. South Med J. 1997;90:L171-L180.

GI and Hematologic AEs: GI and Hematologic AEs: Established vs New AEDsEstablished vs New AEDs
GIGIIrritationIrritation AnorexiaAnorexia HepatotoxicityHepatotoxicity
WeightWeightGainGain HematologicHematologic
EstablishedEstablished
CarbamazepineCarbamazepine ++ ++
EthosuximideEthosuximide ++ ++
PhenobarbitalPhenobarbital ++
PhenytoinPhenytoin ++
PrimidonePrimidone
ValproateValproate ++ ++ ++
NewNew
FelbamateFelbamate ++ ++ ++ ++
GabapentinGabapentin ++
LamotrigineLamotrigine ++
LevetiracetamLevetiracetam
OxcarbazepineOxcarbazepine
TiagabineTiagabine ++
TopiramateTopiramate ++
VigabatrinVigabatrin ++
ZonisamideZonisamide ++Chapman DP, et al. South Med J. 1997;90:L171-L180.

Other AEs: Established vs New AEDsOther AEs: Established vs New AEDs
AlopeciaAlopecia HirsutismHirsutism HyponatremiHyponatremiaa
HypersensitivityHypersensitivityKidneyKidneyStonesStones
InducesInducesCyt450Cyt450
EstablishedEstablished
CarbamazepineCarbamazepine ++ ++ ++
EthosuximideEthosuximide ++
PhenobarbitalPhenobarbital ++ ++
PhenytoinPhenytoin ++ ++ ++
PrimidonePrimidone ++ ++
ValproateValproate ++
NewNew
FelbamateFelbamate ++
GabapentinGabapentin
LamotrigineLamotrigine
LevetiracetamLevetiracetam
OxcarbazepineOxcarbazepine ++ ++
TiagabineTiagabine
TopiramateTopiramate ++ ++
VigabatrinVigabatrin
ZonisamideZonisamide ++ ++Chapman DP, et al. South Med J. 1997;90:L171-L180.

ConclusionsConclusions
• Goal is seizure freedom without side effectsGoal is seizure freedom without side effects
• AED choice depends on seizure type or typesAED choice depends on seizure type or types
• Monotherapy or rational polypharmacyMonotherapy or rational polypharmacy
• Co-morbidities (mood disorder, headache, Co-morbidities (mood disorder, headache, behavioral disturbance, weight, endocrine behavioral disturbance, weight, endocrine dysfunction) should be considered in dysfunction) should be considered in selectionselection

ConclusionsConclusions
• Adverse effects of AEDs must be recognized Adverse effects of AEDs must be recognized and promptly managedand promptly managed
• MRDD patients have special considerations in MRDD patients have special considerations in the recognition and management of AEsthe recognition and management of AEs
• Caregivers must be vigilant and act as Caregivers must be vigilant and act as patients advocate in preventing AEspatients advocate in preventing AEs
• The longterm treatment of MRDD patients with The longterm treatment of MRDD patients with multiple AEDs puts them at high risk for AEsmultiple AEDs puts them at high risk for AEs
• CNS AEs due to ‘drug load’ of multiple AEDs CNS AEs due to ‘drug load’ of multiple AEDs is commonis common