Embed Size (px)
Citation preview

(Gihaoabaldbmsua
Clinical Review: Focused
Adverse Effects of Corticosteroids on BoneMetabolism: A Review
Raj Mitra, MDAbstract: Glucocorticoid (GC) exposure is the most common etiology of drug-inducedsecondary) osteoporosis. Twenty percent of all cases of osteoporosis have been attributed toC exposure. Significant risk factors for the development of fractures after GC exposure
nclude age older than 65 years, prolonged GC exposure (�3 months), positive familyistory of osteoporosis, and low calcium intake. GCs are known to inhibit bone remodelingnd to increase fracture risk. GC exposure alters the fragile balance between osteoclast andsteoblast activity in bone metabolism. GC stimulates osteoclast-mediated bone resorptionnd reduces osteoblast-mediated bone formation, which results in increased overall netone resorption. Specifically, the 2 main effects of GCs on bone metabolism are (1) inducingpoptosis in osteoblasts and osteocytes, thereby decreasing bone formation, and (2) pro-onging the lifespan of osteoclasts and increasing bone resorption. The risk of fractureecreases 3 months after cessation of GC therapy; thus, a 3-month period may be idealetween GC exposures in patients at high risk for the development of osteoporosis. Patientsanaged with GCs who are at high risk for the development of secondary osteoporosis
hould have appropriate diagnostic testing; pre-GC exposure medication management (ie,se of bisphosphonates, human parathyroid hormone); and a limitation of GC therapy, withwait period of 3 months between GC exposures if possible.
PM R 2011;3:466-471
INTRODUCTION
Steroids were first described in 1901 in the management of sciatica and cancer pain [1,2]. In1932, Cushing [3] described the effects of glucocorticoid (GC) exposure on bone metabo-lism, and, in 1953, GCs subsequently were used neuroaxially for spinal pathology [4]. Sincethat time, GCs have become common in the palliative management of the spine (especiallyin cases of neurogenic claudication and radiculopathy attributed to a herniated disk),inflammatory arthropathies, and musculoskeletal pain disorders [5,6].
The mechanism by which GCs provide patients long-term relief for pain syndromes isnot totally clear. It has been postulated that, in addition to their anti-inflammatory effects,GC may induce neuronal reorganization [7]. GCs may also exert their analgesic effects bybinding cytosolic GC receptor located on primary and secondary immune cells [8].
Although GC-induced osteoporosis is the leading cause of secondary osteoporosis, manypatients do not undergo appropriate preprocedure risk assessment before GC exposure [9].Unlike primary osteoporosis, which is characterized by low bone mass in the absence of adisease process or exposure, secondary osteoporosis may result from a variety of chronicconditions and exposures, including exposure to GCs [10]. Other adverse effects associatedwith GC exposure include mania, hyperglycemia, hypertension, weight gain, insomnia, anddisorders of bone metabolism that lead to osteoporosis (Table 1) [11].
Roughly one-fifth of all osteoporosis cases have been attributed to GC exposure; despitethe high prevalence, however, no formal guidelines exist for steroid exposure in high-riskpopulations that undergo repeated GC therapy [12]. Although many physicians will limitthe number of GC therapies in a calendar year, there is no clear consensus on the number ofGC exposures and dosage. The intention of this article is, first, to summarize the literature
concerning the effects of GC on bone metabolism and, second, to formulate evidence-basedPM&R © 2011 by the American Academy of P1934-1482/11/$36.00
Printed in U.S.A.466
R.M. Stanford University School of Medicine,450 Broadway St, Mailcode 6342, RedwoodCity, CA 94063. Address correspondence to:R.M.; e-mail: [email protected]: nothing to disclose
Peer reviewers and all others who controlcontent have no relevant financial relation-ships to disclose.
Disclosure Key can be found on the Table ofContents and at www.pmrjournal.org
Submitted for publication March 24, 2010;accepted February 7, 2011.
hysical Medicine and RehabilitationVol. 3, 466-471, May 2011
DOI: 10.1016/j.pmrj.2011.02.017

w
h
467PM&R Vol. 3, Iss. 5, 2011
recommendations for the use of GCs in patients at high riskfor the development of secondary osteoporosis and fractures.
METHODS
Search Strategy and Selection Criteria
A computer-aided search of several databases was performed:MEDLINE (US National Library of Medicine, Bethesda, MD),1966 to October 2010; EMBASE (Elsevier BV, Amsterdam,the Netherlands), 1982 to present; CINAHL (CumulativeIndex to Nursing and Allied Health Literature; EBSCO Indus-tries, Glendale, CA), 1982 to October 2010; and all EBM(Evidence-Based Medicine, US National Library of Medicine,Bethesda, MD) reviews, including Cochrane DSR (Databaseof Systematic Reviews, ACP Journal Club (American Collegeof Physicians, Philadelphia, PA); DARE (Database of Ab-stracts of Reviews of Effects; National Health Service Centerfor Reviews & Dissemination (NHS CRD), University ofYork, York, UK), and CCTR (Cochrane Controlled TrialsRegister, now known as Cochrane Database of SystematicReviews, The Cochrane Collaboration). The search termswere steroid, corticosteroid, bone, and metabolism. Caseseries and studies with low statistical power were omitted forthis focused review.
Epidemiology
Osteoporosis attributed to GC exposure is the most commonetiology of drug-induced (secondary) osteoporosis, with one-fifth of all cases of osteoporosis having been attributed to GCexposure [13]. Corticosteroid used in musculoskeletal andspinal pain syndromes accounts for almost half of all GCtreatments. GC therapy has become quite common, espe-cially in the elderly population. It has been reported that upto 2.5% of the general population in the United Kingdommay be receiving steroid therapy at any given time, whereasroughly 10% of Americans require long-term GC therapy forthe management of chronic illness [14,15]. Almost 50% ofpatients receiving chronic GC therapy will develop osteope-nia and fractures; 17% of these patients will develop fractureswithin the first year of GC therapy [16]. Significant riskfactors for the development of fractures after steroid exposure
Table 1. Major adverse sequelae of glucocorticoid exposure
HyperglycemiaWeight gainOsteoporosisDiabetes mellitusHypertensionMania or hypomaniaImmune suppressionCushing syndromeHypothalamic pituitary adrenal axis suppression
include age older than 65 years, prolonged steroid exposure
(�3 months), positive family history of osteoporosis, andlow calcium intake [17] (Table 2). Patients receiving long-term steroid medication have been found to have an elevatedrisk of developing new fractures after vertebroplasty [18].Furthermore, the incidence of vertebral fractures is higher inpatients with GC-induced osteoporosis when compared withprimary osteoporosis [19].
Pathophysiology
Oral GC has been shown to increase bone resorption in adose-response relationship [20]. Steroids are produced inthe adrenal cortex and modulated by the hypothalamic–pituitary–adrenal axis. Corticotropin-releasing hormone(CRH) produced by the hypothalamus stimulates the pi-tuitary gland to produce adrenocorticotropic hormone(ACTH); ACTH, in turn, stimulates the adrenal cortex toproduce glucocorticoids [21]. Sex steroids are importantin bone metabolism. Patients with lower free androgenand estradiol levels are more likely to have symptomaticvertebral body fractures [22].
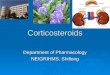
GC exposure alters the fragile balance between osteoclastand osteoblast activity in bone metabolism (Figure 1) [23].GC receptors have been found in human osteoblasts andosteoclasts [24]. GC stimulates osteoclast-mediated boneresorption and reduces osteoblast-mediated bone formation,which results in increased overall net bone resorption. Spe-cifically, the 2 main effects of GCs on bone metabolism are(1) inducing apoptosis in osteoblasts and osteocytes, therebydecreasing bone formation; and (2) prolonging the lifespan ofosteoclasts and increasing bone resorption [25,26]. In con-trast, in postmenopausal osteoporosis, increased bone re-sorption seems to be the key factor [27].
Effects on Osteoblasts
The majority of normal osteoblasts will undergo apoptosis.The remainder will differentiate into an osteocyte, which iscapable of proliferation and secretion of osteoid matrix inte-gral for bone formation. In addition, osteoblasts secrete nu-clear factor–�B ligand (RANKL, an osteoclast activator) as
ell as osteoprotegrin (a RANKL inhibitor).GC affects osteoblasts throughout their lifespan and in-
ibits stem cell differentiation into osteoblasts [28]. These
Table 2. Patients at risk for the development of glucocortico-id-induced osteoporosis
Advanced age (�65 y)Prolonged exposureKnown history of osteoporosisFamily history of osteoporosisLow calcium intakeHistory of fractureFamily history of hip fracture
Rheumatoid arthritis
pc
rutfrbpsb
idchapsmphmc
s
468 Mitra ADVERSE EFFECTS OF CORTICOSTEROIDS ON BONE METABOLISM
stem cells instead proliferate into adipocytes and decrease theosteoblast pool [29]. GC also causes osteoblasts to decrease
roduction of insulin-like growth factor (IGF-I), which de-reases proliferation and anabolic activity [30]. The overall
effect of GC on osteoblasts, therefore, results in significantlydecreased anabolic activity, apoptosis, and decrease in stemcell differentiation into osteocytes; this, in turn, decreases thesecretion of osteoid matrix and new bone formation.
Effects on Osteoclasts
Osteoclasts are essentially members of the macrophage fam-ily and eventually differentiate into multinucleated giant cells[31]. Osteoclasts attach to the bone surface and digest bonematrix by creation of an acidic environment; these cellsnormally work in harmony with osteoblasts and eventuallyundergo apoptosis.
As mentioned above, the increase in osteoblast RANKligand production (induced by GC) leads to increased oste-oclastic activity. In addition, receptor activation of RANKligand secondary to GC exposure prolongs the lifespan ofosteoclasts [14]. Parathyroid hormone also leads to stimula-tion of the osteoclasts.
Systemic Effects of GC Exposure
GC exposure has been demonstrated to affect the hypotha-lamic–pituitary–adrenal axis; production of adrenal and go-nadal hormones are reduced (including estrogen and testos-terone) [32]. Osteoprotegrin and estrogen both inhibitosteoclast activity. Experiments have demonstrated that acti-
Figure 1. Glucocorticoid stimulates osteoclast-mediatedbone resorption and reduces osteoblast-mediated bone for-mation, which results in increased overall net bone resorption.Specifically, the 2 main effects of glucocorticoids on bonemetabolism are (A) inducing apoptosis in osteoblasts andosteocytes, thereby decreasing bone formation; and (B) pro-longing the lifespan of osteoclasts and increasing bone resorp-tion [13]. Reprinted with permission.
vation of the estrogen receptor � and androgen receptor
esult in a stimulatory effect on both the cortical and trabec-lar bone mass in males [33]. Reduction in estrogen recep-or activation secondary to GC exposure, therefore, mayurther increase bone resorption (by decreasing estrogen-elated osteoclast inhibition). Recently, much interest haseen placed on GC receptor antagonists; the steroid mife-ristone (RU-486) is primarily antiestrogenic, and re-earch on its efficacy in decreasing the incidence of bonereakdown is limited [34].
GCs are known to affect calcium metabolism by decreas-ng renal uptake and intestinal absorption in a dose-depen-ent manner [25]. GC exposure, which decreases renal cal-ium uptake, in turn, stimulates an increase in parathyroidormone (PTH), further increasing the number of osteoclastsnd stimulating bone resorption [35]. Interestingly, not allatients managed with GC develop low bone mineral den-ity. The current literature suggests that the phenomenonay be caused by multiple genes as opposed to polymor-hism in a single gene [36]. Vitamin D polymorphisms,owever, have not been consistently linked to low boneineral density in patients managed with GC, and the asso-
iation is still unclear [37,38].GC therapy also has been associated with the develop-
ment of avascular necrosis. It has been postulated that GCpotentiates fat accumulation in bone marrow, which subse-quently leads to intraosseous hypertension, decreased bloodflow, and eventually necrosis of bone [39]. The proximalfemur is most commonly involved, followed by distal femur-proximal tibial plateau, and shoulder [40].
GC Exposure and Fracture Risk
Fractures continue to be a common risk of prolonged steroidexposure and remain the most clinically relevant endpoint.The magnitude of the risk and relationship to duration ofexposure are not clear. Steroids are known to increase frac-ture risk by their inhibition of bone remodeling [41]. Patientsmanaged with long-term steroids have a significantly higherrisk of developing vertebral compression fractures [42]. Atudy by Cooper et al [43] reported a doubling of the risk of
hip fractures in patients with rheumatoid arthritis who hadbeen managed with long-term steroids, when compared withage- and gender-matched community controls.
There are numerous studies that have analyzed the rela-tionship between dosage of GC and fracture risk. Bone losssecondary to GC treatment has been shown to be dosedependent, with an increase in fracture risk being correlatedwith GC dosage [44]. Eighty percent of patients with asthmamanaged with high-dose GC therapy had a decrease in bonemineral density compared with 33% of patients managedwith a low dose of GCs [45]. Fractures may occur within3 months of GC therapy at dosages as low as 2.5 mg of pred-nisone daily [46]. De Vries et al [47] analyzed 191,752
patients who were receiving intermittent GCs over a 10-year
469PM&R Vol. 3, Iss. 5, 2011
period; those patients who received less than 7.5 mg ofprednisone daily had a roughly 60% increase in vertebralbody fracture. In the same study, a dose-dependent relation-ship was described with patients who received 30 mg of oralprednisone daily having substantially more risk of spinalfracture than those who received 7.5 mg of prednisone daily.
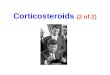
GC therapy has been shown to affect trabecular bone slightlymore than cortical bone, which affects the spine more than thehip [48]. Although the risk of fracture increases within the firstfew months of GC exposure, the likelihood of fracture rapidlydecreases after cessation of steroid therapy [49]. The highest rateof bone loss occurs in the first 6 months of treatment [50]. Therelationship between cessation of GC exposure and a decrease infracture risk has been well characterized by Van Staa et al [48],with the greatest decrease in relative risk occurring within thefirst 3 months of cessation (Figure 2).
Management
Appropriate management may help prevent or reduce boneloss and fracture development in patients chronically ex-posed to GC [51]. Bisphosphonates are the first-line agentsfor the prevention of GC-induced osteoporosis. Teriparatide,calcium supplements, active vitamin D, and hormonal re-placement are alternative agents [21]. Patients have beenshown to achieve optimal results when they have been pre-scribed calcium supplements and vitamin D before and dur-ing bisphosphonate use [52] (Table 3).
Alendronate has been shown to be beneficial in increasingbone mineral density and deceasing vertebral spinal frac-tures. At 1-year follow-up, patients exposed to GC who weretreated with alendronate were found to have 3% increase inlumbar spine bone mineral density and an overall 40%relative risk reduction [53]. Risedronate has been shown to
Figure 2. Adjusted relative rate of nonvertebral fractures aftercessation of oral glucocorticoids. Reprinted with permissionfrom reference [48].
reduce the relative vertebral body fracture risk by 70%; in
contrast to alendronate, risedronate has been approved toprevent and treat GC-induced osteoporosis [54].
Benucci et al [55] analyzed 69 patients with rheumatismwho were receiving low-dose GC therapy; 23 patients hadcontraindications to bisphosphonate therapy and were man-aged with oral calcium and vitamin D. The remaining 46patients received bisphosphonate therapy (intramuscularneridronate) in addition to oral calcium and vitamin D. At12-month follow-up, the group managed with bisphospho-nate had significantly increased lumbar and femoral bonemineral density. Results of studies have demonstrated thatintravenous bisphosphonate infusion presents an effectivealternative for patients who cannot tolerate oral medications[56]. Reid et al [57] compared intravenous single infusion ofzoledronate with daily risedronate in patents managed withGC in a double-blind, randomized, controlled trial; it wasfound that the single intravenous infusion was more effectiveat increasing lumbar spine bone mineral density at 12 months.
Teriparatide is a recombinant human parathyroid hor-mone. The medication induces preosteoblasts into osteo-blasts, thereby stimulating formation of new bone [58]. Inaddition, teriparatide decreases osteoblast apoptosis [59].
Devogelaer et al [60] conducted a double-blind random-ized control study on the efficacy of teriparatide 20 mg/d oralendronate 10 mg/d in 387 patients with GC-induced osteo-porosis on bone mineral density of the lumbar spine, femoralneck, and total hip. It was found that bone mineral densitywas increased in both groups, with teriparatide being signif-icantly more efficacious then alendronate. In a similar trial,Saag et al [61] compared the efficacy of teriparatide withalendronate in 428 patients with GC-induced osteoporosis.The patients were followed up for 36 months; it was foundthat the patients in the teriparatide group had significantlygreater increases in bone mineral density, higher serum cal-cium concentration, and fewer vertebral fractures than sub-jects in the alendronate group [61].
The American College of Rheumatology recommends thatpatients who are chronically managed with GC (eg, �5 mgprednisone daily for 3 months) start calcium daily, vitamin D,and bisphosphonates [62]. Bisphosphonate therapy also wasrecommended to be started in patients with T scores of �1on bone mineral density testing [63]. Calcitonin has beenshown to prevent GC-induced bone loss, but to ourknowledge no studies have documented decreased frac-ture risk [64].
Table 3. Recommendations for patients with osteoporosiswho are undergoing glucocorticoid injections
Increase daily calcium intake to �1000 mgBisphosphonate useBaseline bone mineral densitometryParathyroid hormone treatmentMinimize steroid dosage, especially in patient older than 65 y
Three-month waiting time between steroid injections
470 Mitra ADVERSE EFFECTS OF CORTICOSTEROIDS ON BONE METABOLISM
Dual-energy x-ray absorptiometry scans have been shownto be valuable in the monitoring of bone density in patientsexposed to GC [65]. Early detection of decreased bone den-sity may allow the physician to initiate medication treatments(ie, bisphosphonates) as well as to discontinue further expo-sure to GC (if this is an option); thus, early detection maysignificantly decrease skeletal morbidity [66].
CONCLUSION
Based on the current literature, essential facts have been estab-lished. GC exposure alters the fragile balance between osteoclastand osteoblast activity in bone metabolism, which favors overallbone loss. Osteoblasts exposed to GC have significantly de-creased anabolic activity, induction of early apoptosis, and adecrease in stem cell differentiation into osteocytes; this, in turn,decreases the secretion of osteoid matrix and new bone forma-tion. GC exposure also induces receptor activation of RANKligand secretion exposure, which, in turn, increases activity andprolongs the lifespan of osteoclasts.
The metabolic effects of GC increases the relative risk offracture development in a dose-dependent manner. Further-more, the cessation of GC decreases the relative risk offractures over the first year; this decrease is most profoundwithin the first 3 months of cessation of GC therapy. Becausethe risk for fracture decreases after cessation of GC exposureafter 3 months, a 3-month period may be ideal between GCexposures in patients at high risk for the development ofosteoporosis [24,59].
Patients managed with GCs who are at high risk for thedevelopment of secondary osteoporosis should have appropri-ate diagnostic testing, pre-GC exposure medication manage-ment (ie, use of bisphosphonates, human parathyroid hor-mone), and a limitation of GC therapy, with a wait period of 3months between GC exposures if possible.[67].
REFERENCES1. Sicard MA. Les injections medicamenteuseextraduraqles per voie sara-
coccygiene. C R Seances Soc Biol Fil 1901;53:396-398.2. Cathelin F. Mode d’action de a cocaine injete dausl’escapte epidural par
le procede du canal sacre. C R Seances Soc Biol Fil 1901;53:452-453.3. Cushing HW. The basophil adenomas of the pituitary body and their
clinical manifestations (pituitary basophilism). Bull Johns HopkinsHosp 1932;50:137-195.
4. Lievre JA, Bloch-Michel H, Pean G, et al. L’hydrocortisone en injectionlocale. Rev Rhum 1953;20:310-311.
5. Roberts ST, Willick SE, Rho ME, Rittenberg JD. Efficacy of lumbosacraltransforaminal epidural steroid injections: a systematic review. PM R2009;1:657-668.
6. Botwin K, Brown LA, Fishman M, Rao S. Fluoroscopically guidedcaudal epidural steroid injections in degenerative lumbar spine steno-sis. Pain Physician 2007;10:547-558.
7. Fowler RJ, Blackwell GJ. Anti-inflammatory steroid induced biosynthe-sis of a phospholipase A2 inhibitor which prevents prostaglandingeneration. Nature 1979;278:456-459.
8. Spies CM, Burmester GR, Buttgereit F. Analyses of similarities and
differences in glucocorticoid therapy between rheumatoid arthritis andankylosing spondylitis: a systematic comparison. Clin Exp Rheumatol2009:27(Suppl 55):S152-S158.
9. Willenberg HS, Lehnert H. 2008. Basics and management of glucocor-ticoid-induced osteoporosis. Internist 2008;49:1186-1194.
10. Consensus Development Conference V, 1993. Diagnosis, prophylaxis,and treatment of osteoporosis. Am J Med 1994;90:646-650.
11. Brown ES. Effects of glucocorticoids on mood, memory, and thehippocampus. Treatment and preventive therapy. Ann N Y Acad Sci2009;1179:41-55.
12. Adinoff AD, Hollister JR. Steroid-induced fractures and bone loss inpatients with asthma. N Engl J Med 1983;309:265-268.
13. Soen S, Tanaka Y. Glucocorticoid-induced osteoporosis: skeletal man-ifestations of GC use and 2004 Japanese Society for Bone and MineralResearch-proposed guidelines for its management. Mod Rheumatol2005;15:163-118.
14. Kerachian MA, Seguin C, Harvey EJ. Glucocorticoids in osteonecrosisof the femoral head: a new understanding of the mechanisms of action.J Steroid Biochem Mol Biol 2009;114:121-128.
15. Van Staa TP, Leufkens HG, Abenhaim L, et al. Use of oral corticoste-roids in the United Kingdom. Q J Med 2000;93:105-111.
16. Weinstein RS, Manolagas SC. Apoptosis in GC-induced bone disease.Curr Opin Endocrinol Diabetes 2008;12:219-223.
17. Lambrinoudaki I, Kung AW. Management of steroid-induced osteopo-rosis. Chin Med J (Engl) 2000;113:681-685.
18. Hiwatashi A, Westesson PL. Patients with osteoporosis on steroidmedication tend to sustain subsequent fractures. AJNR Am J Neurora-diol 2007;28:1055-1057.
19. Van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C. Oralcorticosteroids and fracture risk: relationship to daily and cumulativedoses. Rheumatology 2000;15:1383-1389.
20. Langhammer A, Forsmo S, Syversen U. Long-term therapy in COPD:any evidence of adverse effect on bone? Int J Chron Obstruct PulmonDis 2009;4:365-380.
21. Coursin DB, Wood KE. Corticosteroid supplementation for adrenalinsufficiency. JAMA 2002;287:236-240.
22. Tuck SP, Scane AC, Fraser WD, Diver MJ, Eastell R, Francis RM. Sexsteroids and bone turnover markers in men with symptomatic vertebralfractures. Bone 2008;43:999-1005.
23. Olney RC. Mechanisms of impaired growth: effect of steroids on boneand cartilage. Horm Res 2009;72(Suppl 1):30-35.
24. Yoshioka T, Sato B, Matsumoto K. Ono K. Steroid receptors in osteo-blasts. Clin Orthop Relat Res 1980;148:297-303.
25. Migliaccio S, Brama M, Malavolta N. Management of glucocorticoids-induced osteoporosis: role of teriparatide. Ther Clin Risk Manag 2009;5:305-310.
26. Calder JD, Buttery L, Revel PA, Pearse M, Polak JM. Apoptosis: asignificant cause of bone cell death in osteonecrosis of the femoral head.J Bone Joint Surg Br 2004;86:1209-1213.
27. Dalle Carbonare L, Arlot ME, Chavassieux PM, et al. Comparison oftrabecular bone microarchitecture and remodeling in GC-induced andpostmenopausal osteoporosis. J Bone Miner Res 2001;16:97-103.
28. De Nijs RN. Glucocorticoid-induced osteoporosis: a review on patho-physiology and treatment options. Minerva Med 2008;99:23-43.
29. Baron R, Rawadi G. Targeting the Wnt/beta-catenin pathway to regu-late bone formation in the adult skeleton. Endocrinology 2007;148:2635-2643.
30. Delany AM, Durant D, Canalis E. Glucocorticoid suppression of IGF Itranscription in osteoblasts. Mol Endocrinol 2001;15:1781-1789.
31. Ross FP. Osteoclast biology and bone resorption. In: Favus MJ, Lian JB,Goldring SR, eds. Primer on the Metabolic Diseases and Disorders ofMineral Metabolism. Washington, DC: American Society for Bone andMineral Research; 2006:30-35.
32. Lane NE, Lukert B. The science and therapy of glucocorticoid induced
bone loss. Endocrinol Metab Clin North Am 1998;27:465-483.
471PM&R Vol. 3, Iss. 5, 2011
33. Ohlsson C, Vandenput L The role of estrogens for male bone health.Eur J Endocrinol 2009;160:883-889.
34. Mohler ML, He Y, Wu Z, Hong SS, Miller DD. Non-steroidal GCreceptor antagonists: the race to replace RU-486 for anti-GC therapy.Expert Opin Ther Pat 2007;17:59-81.
35. Kuroki Y, Kaji H, Kawano S, et al. Short-term effects of GC therapy onbiochemical markers of bone metabolism in Japanese patients: a pro-spective study. J Bone Miner Metab 2008;26:271-278.
36. Xu XH, Dong SS, Guo Y, et al. Molecular genetic studies of gene identificationfor osteoporosis: the 2009 update. Endocr Rev 2010;31:447-505.
37. Hustmyer FG, Peacock M, Hui S. Bone mineral density in relation topolymorphism at the vitamin D receptor gene locus. J Clin Invest1994;94:2130-2134.
38. Sainz J, Van Tornout JM, Loro ML. Vitamin D receptor gene polymor-phisms and bone density in prepubertal American girls of Mexicandescent. N Engl J Med 1997;337:77-82.
39. Clinkscales A, Cleary JD. Steroid-induced avascular necrosis. AnnPharmacother 2002;36:1105.
40. Habib GS, Saliba W, Nashashibi M. Local effects of intra-articularcorticosteroids. Clin Rheumatol 2010;29:347-356.
41. Hein GE. Particular features of steroid-induced osteoporosis. Ortho-pade 2007;36:708, 710-713.
42. Arai K, Hanyu T, Sugitani H, et al. Risk factors for vertebral fracture inmenopausal or postmenopausal Japanese women with rheumatoidarthritis: a cross-sectional and longitudinal study. J Bone MinerMetabol 2006;24:118-124.
43. Cooper C, Coupland C, Mitchell M. Rheumatoid arthritis, corticoste-roid therapy and hip fracture. Ann Rheum Dis 1995;54:49-52.
44. Compston J. Management of GC-induced osteoporosis. Nat Rev Rheu-matol 2010;6:82-88.
45. Goldstein MF, Fallon JJ, Harning R. Chronic glucocorticoid therapyinduced osteoporosis in patients with obstructive lung disease. Chest1999;16:1733-1749.
46. Civitelli R, Ziambaras K. Epidemiology of GC-induced osteoporosis. JEndocrinol Invest 2008;31(Suppl):2-6.
47. De Vries F, Bracke M, Leufkens HGM, et al. Fracture risk with inter-mittent high dose oral glucocorticoid therapy. Arthritis Rheum 2007;56:208-214.
48. Van Staa TP, Leufkens HG, Abenhaim L, et al. Use of oral corticoste-roids and risk of fractures. J Bone Miner Res 2000;15:993-1000.
49. Van Staa TP, Leufkens HG, Cooper C: The epidemiology of corticosteroid-induced osteoporosis: a meta-analysis. Osteoporos Int 2002;13:777-787.
50. Manchikanti, L. Role of neuraxial steroids in interventional pain man-agement. Pain Physician 2002;5:182-199.
51. Kennedy CC, Papaioannou A, Adachi JD. Glucocorticoid-induced os-teoporosis. Womens Health (Lond Engl) 2006;2:65-74.
52. Kennel KA, Drake MT. Adverse effects of bisphosphonates: implica-tions for osteoporosis management. Mayo Clin Proc 2009;84:632-637.
53. Saag KG, Emkey R, Schnitzer TJ, et al. Alendronate for the preventionand treatment of glucocorticoids-induced osteoporosis. Glucocortico-ids-Induced Osteoporosis Intervention Study Group. N Engl J Med1998;339:292-299.
CME QuestionThe effects of glucocorticoid administration on bone metabolism inc
a. induction of apoptosis in osteoblastsb. promotion of stem cell differentiation in osteocytesc. prolonging the life span of osteoclastsd. stimulation of osteoclast mediated bone resorption
Answer online at me.aapmr.org
54. Cohen S, Levy RM, Keller M, et al. Risedronate therapy preventscorticosteroid-induced bone loss: a twelve-month, multicenter, ran-domized, double-blind, placebo-controlled, parallel-group study. Ar-thritis Rheum 1999;42:2309-2318.
55. Benucci M, Saviola G, Baiardi P, et al. Effects of monthly intramuscularneridronate in rheumatic patients in chronic treatment with low-doseglucocorticoids. Clin Exp Rheumatol 2009;27:567-573.
56. Reid DM, Devogelaer JP, Saag K, et al. Zoledronic acid and risedronate in theprevention and treatment of GC-induced osteoporosis (HORIZON): a multi-centre, double-blind, double-dummy, randomised controlled trial. HORI-ZON investigators. Lancet 2009;373:1253-1263.
57. Reid DM, Devogelaer J, Saag K, et al. Effect of a single infusion ofzoledronic acid 5mg versus oral risedronate 5 mg on bone mineraldensity at lumbar spine, hip, femoral neck and trochanter in patientswith GC induced osteoporosis. J Bone Miner Res 2008;23:s122.
58. Canalis E, Giustina A, Bilezikian JP. Mechanisms of anabolic therapiesfor osteoporosis. N Engl J Med 2007;357:905-916.
59. Jilka RL, Weinstein RS, Bellido T, Roberson P, Parfitt AM, ManolagasSC. Increased bone formation by prevention of osteoblast apoptosiswith parathyroid hormone. J Clin Invest 1999;104:439-446.
60. Devogelaer JP, Adler RA, Recknor C, et al. Baseline GC dose and bone mineraldensity response with teriparatide or alendronate therapy in patients withGC-induced osteoporosis. J Rheumatol 2010;37:141-148.
61. Saag KG, Zanchetta JR, Devogelaer JP, et al. Effects of teriparatideversus alendronate for treating GC-induced osteoporosis: thirty-six-month results of a randomized, double-blind, controlled trial. ArthritisRheum 2009;60:3346-3355.
62. Recommendations for the prevention and treatment of glucocorticoids-induced osteoporosis: 2001 update. American College of Rheumatol-ogy Ad Hoc Committee on Glucocorticoids-Induced Osteoporosis.Arthritis Rheum 2001;44:1496-1503.
63. Adler RA, Hochberg MC. Suggested guidelines for evaluation andtreatment of glucocorticoid-induced osteoporosis for the Departmentof Veterans Affairs. Arch Intern Med 2003;163:2619-2624.
64. Luengo M, Pons F, Martinez de Osaba MJ, Picado C. Prevention offurther bone mass loss by nasal calcitonin in patients on long termglucocorticoids therapy for asthma: a two year follow up study. Thorax1994;49:1099-1102.
65. Werth VP. Glucocorticoid-induced osteoporosis evaluation, preven-tion, and treatment. J Clin Rheumatol 1997;3(2 Suppl):69-73.
66. Reid IR. Glucocorticoid-induced osteoporosis: assessment and treat-ment. J Clin Densitom 1998;1:65-73.
67. Mori S. Prevalence of steroid osteoporosis. Clin Calcium 2006;16:1782-1787.
This CME activity is designated for 1.0 AMA PRA Category 1 Credit™ andcan be completed online at me.aapmr.org. Log on to www.me.aapmr.org,go to Lifelong Learning (CME) and select Journal-based CME from thedrop down menu. This activity is FREE to AAPM&R members and $25 fornon-members.
ll of the following except:
lude a