Embed Size (px)
Citation preview

National Institute on Drug AbuseBringing the full power of science to bear on drug abuse and addictionNora D. Volkow, M.D.DirectorNational Institute on Drug Abuse
Advancing Addiction Science to Address the Opioid Crisis
Advancing Addiction Science
Wilson M. Compton, M.D., M.P.E.Deputy Director
National Institute on Drug Abuse
Science = Solutions

16,849
47,055
52,404
63,632
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
199920002001200220032004200520062007200820092010201120122013201420152016
Overdose Deaths Increased Markedly in 2016

Virtually All of the U.S. Have Increased Drug Overdoses: Estimated Age-adjusted Death Rates for Drug Poisoning by County
20151999
https://www.cdc.gov/nchs/data-visualization/drug-poisoning-mortality/

Other Synthetic Opioids(e.g. fentanyl)
Commonly Prescribed Opioids(natural and semi-synthetic opioids and methadone)
Heroin
Methadone
Overdose Deaths Primarily from Opioids: Prescription Drugs, Heroin and Synthetics (i.e. Fentanyl and similar)

ENVIRONMENTAL AVAILABILITY: Current Opioid Crisis Originated with Prescribing Increases
Opioid prescriptions Tripled to MORE THAN 200 MILLION prescriptions in recent years
0
50
100
150
200
250
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
Opio
id P
resc
riptio
ns in
MILL
IONS

People Misusing Analgesics Obtain them Directly & Indirectly by Prescription
Source where pain relievers obtained for most recent misuse
10%
36%87%
10%
3%
54%
Friend/Relative
Prescription
Other
Their Prescription
Their Friend/RelativeOther
Source: Han, Compton, et al. Annals of Internal Medicine 2017;167(5):293-301
Source where pain relievers obtained for most recent misuse
10%
36%87%
10%
3%
54%
Friend/Relative
Prescription
Other
Their Prescription
Their Friend/RelativeOther
Source: Han, Compton, et al. Annals of Internal Medicine 2017;167(5):293-301
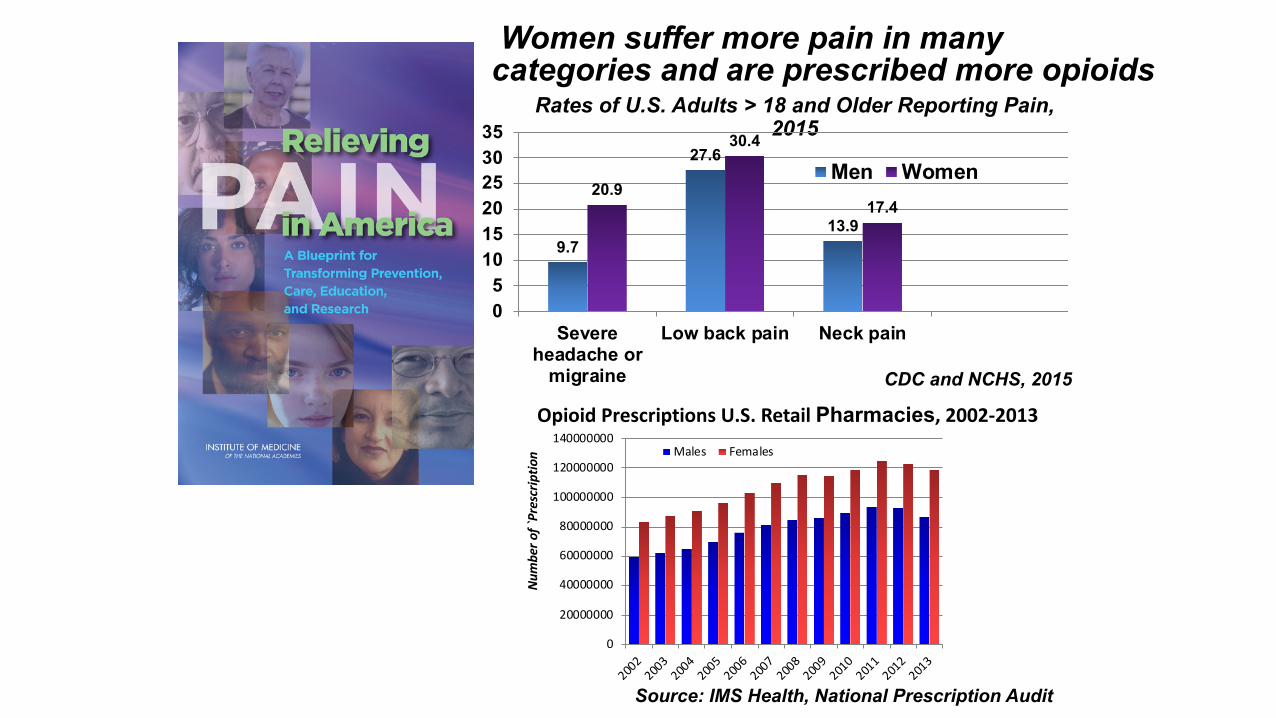
Rates of U.S. Adults > 18 and Older Reporting Pain, 2015
CDC and NCHS, 2015
9.7
27.6
13.9
20.9
30.4
17.4
05
101520253035
Severeheadache or
migraine
Low back pain Neck pain
Men Women
Women suffer more pain in many categories and are prescribed more opioids
0
20000000
40000000
60000000
80000000
100000000
120000000
140000000
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Males Females
Opioid Prescriptions U.S. Retail Pharmacies, 2002-2013
Source: IMS Health, National Prescription Audit
Num
ber o
f `Pr
escr
iptio
n

Analgesic Mechanisms of Mu Opiate Drugs (Heroin, Vicodin, Morphine)
Thalamus(pain)
ACC(pain)
PAG(pain)
Accumbens(reward)

Rx Opioid Misuse has been a Risk Factor for Heroin Use
% Heroin Treatment Admissions that Used Heroin or Rx Opioid First
Source: Cicero et al. JAMA Psychiatry. 2014;71(7):821-826.
Most current heroin users started opioid use with prescription opioids.
Decade of First Opioid Use (No. of Abusers)

Most Heroin Users Report Previous Non-Medical Use of Prescription Opioids,
National General Population: •Within 5 years, 3.6% of non-medical users of opioids progressed to
heroin within 5 years (i.e. less than 1% per year) (Muhuri, Gfroerer, Davies. 2013)
Local Longitudinal Study of Non-medical users: •Within 3 years, 7.5% progressed to heroin (i.e. 2.8% per year) (Carlson,
Nahhas, martins, Daniulaityte. 2015)
BUT Only a Small Proportion of Non-Medical Users Progress to Heroin

Heroin Users: First Opioid Now Likely to be Heroin
Source: Cicero T et al. Addictive Behaviors 2017;74:63-66

ECONOMICS: Heroin Increases Due to Lower Price and Greater Availability
$-
$500
$1,000
$1,500
$2,000
$2,500
$3,000
$3,50019
8119
8219
8319
8419
8519
8619
8719
8819
8919
9019
9119
9219
9319
9419
9519
9619
9719
9819
9920
0020
0120
0220
0320
0420
0520
0620
0720
0820
0920
1020
1120
12
"Retail" Price Per Pure Gram
National Drug Control Strategy--Data Supplement 2014. https://www.whitehouse.gov/sites/default/files/ondcp/policy-and-research/ndcs_data_supplement_2014.pdf

Fentanyl and Counterfeit Products Broaden Risk Population
Source: Jones CM, et al. AJPH 2017, Mar;107(3):430-432.

Graphs from NY Times Article based on CDC MMWR Report2017
2016 Fentanyl-Related Deaths Surpassed Heroin or Rx

ECONOMICS: CHEAP
Fentanyl Precursor Chemicals

Increasing Prenatal Exposure
Admissions for Newborn Withdrawal Syndromes
(Number per 1000 Admissions)
Source: Tolia VN, Patrick SW, et al. NEJM 2015;372:2118-2126 Science = Solutions

Counties Deemed Highly Vulnerable to Rapid Dissemination of HCV or HIV
Source: Van Handel et al, JAIDS 2016
Rising rates of HCV
Suryaprasad et al. Clin Infect Dis. 2014
HIV (and Hepatitis C) Outbreak Linked to Oxymorphone Injection
Use in Indiana, 2015Peters et al.
The New England Journal of Medicine2016;375:229-239

Science = Solutions: Using Research to Improve HIV and Hepatitis C in Rural Areas
NIH is partnering with the CDC, SAMHSA and the Appalachian Regional Commission (ARC) to conduct research to address increased opioid injection drug use and resulting overdose, HIV and Hepatitis C infection.
• Improve understanding problem’s scope; contributing health trends• Identify resources, obstacles •Develop intervention approaches
to address these health threats

0
10
20
30
40
50
60
70
80
90
Opioid Analgesic Deaths Involving Benzodiazepines Benzodiazepine Deaths Involving Opioid Analgesics
2004 2005 2006 2007 2008 2009 2010 2011Pe
rcen
t
Opioid Analgesics BenzodiazepinesSource: CM Jones, JK McAninch. American Journal of Preventive Medicine 2015;49:493-501.
AAPC = 8.4% (95% CI 7.1%-9.7%)
AAPC = 1.5% (95% CI 0.8%-2.2%)
Overlap of Benzodiazepines and OpioidsOpioid Analgesic ED Visits and OD Deaths Involving Benzodiazepines &
Benzodiazepine ED Visits and OD Deaths Involving Opioids
Science = Solutions
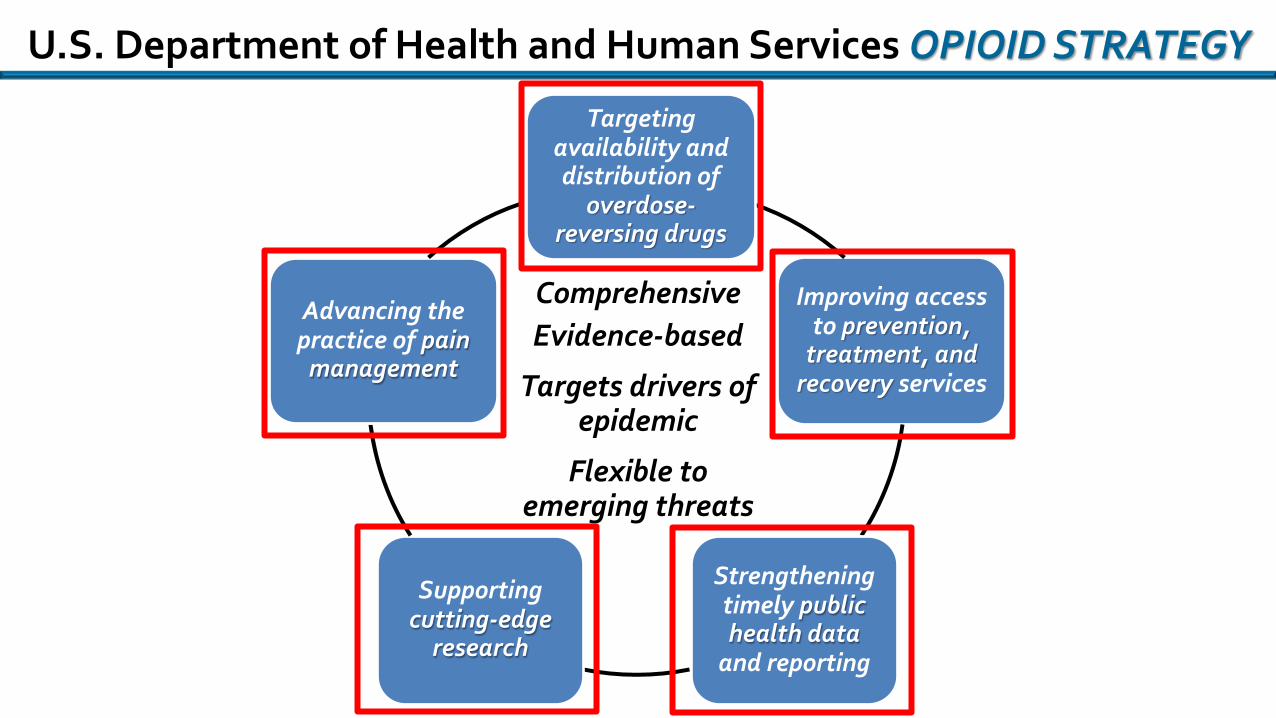
U.S. Department of Health and Human Services OPIOID STRATEGY
Improving access to prevention,
treatment, and recovery services
Targeting availability and distribution of
overdose-reversing drugs
Strengthening timely public health data
and reporting
Supporting cutting-edge
research
Advancing the practice of pain
management
ComprehensiveEvidence-based
Targets drivers of epidemic
Flexible to emerging threats

Inadequate Pain Treatment as a Driver?
1.9 million adults had prescription opioid use disorders(0.8% of the U.S. adult population)
91.8 million adults used prescription opioids (37.8% of the U.S. adult population)
11.5 million adults misused prescription opioids (4.7% of the U.S. adult population)
48.7
8.9
16.2
7.0
12.0
7.2
66.3
11.2
2.210.8
4.62.4 0.9 0.6 1.0 relieve physical pain
relax or relieve tensionexperimentget high or feel goodhelp with sleephelp with emotions or feelingsincrease/decrease effects of other drugshooked or have to misuseother reason
Source: Han, Compton, et al. Annals of Internal Medicine 2017 (epub Aug 1, 2017)

Limited Medical Education on Pain (and Addiction)
Mezei L, et al. Pain education in North American medical schools J Pain. 2011
Number of med schools teaching 0 to 5 hours, 5 to 10 hours, etc.. U.S. medical schools dark gray bars, Canadian schools light gray.
Pain Education in USA:
9 Mean Hours(range 1-31)

Doctors Continue to Prescribe Opioids for Ninety-one Percent of Overdose Patients
Source: Larochelle et al. Ann Intern Med. 2016;164(1):1-9.
high dose moderate doselow dose none
14%
13%
63% of high-dose opioid pts still on high dose 31-90 days after OD
17%of high- dose
patients overdosed
again within two years
In a 2-year follow-up of 2848 commercially insured patients who had a nonfatal opioid overdose during long-term opioid therapy :
Ø33-39% of those with active opioid prescriptions during follow-up also were prescribed benzodiazepines.

Opioid Prescribing Guidelines
Ø Intended for primary care providersØ Applies to patients >18 years old in chronic pain
outside of end-of-life careØ Builds on joint CDC, NIDA, ONC, SAMHSA summary
on “Common Elements in Guidelines for Prescribing Opioids for Chronic Pain” and the NIH Pathways to Prevention for Opioids in Treating Chronic Pain
Ø PUBLISHED MARCH 15, 2016
Ø Recent Landscape for Guidelines:§ Small Number§ Outdated§ Not Conflict Free
ØSolution….

Resources for Medical Students, Resident Physicians & Faculty
Web training on pain assessment and treatment
Archived NIDA CME Courses:
Safe Prescribing for PainManaging Pain Patients
Who Abuse Rx Drugs
Opioid Education
Upcoming NIDA CME Course:
Adolescent Substance Use (Prescription Opioid Module)
Bringing NIDA research to
clinical practice
Medical schools have developed innovative curriculum resources about how to identify and treat patients with substance use disorders

0
10
20
30
40
50
60
70
1Q20
102Q
2010
3Q20
104Q
2010
1Q20
112Q
2011
3Q20
114Q
2011
1Q20
122Q
2012
3Q20
124Q
2012
1Q20
132Q
2013
3Q20
134Q
2013
1Q20
142Q
2014
3Q20
144Q
2014
1Q20
152Q
2015
3Q20
154Q
2015
1Q20
162Q
2016
Opio
id M
ME
in B
ILLIO
NS
Opioid Morphine Milligram Equivalents Prescribed Declined 23.1% from
3rd quarter 2010 to 2nd quarter 2016
Recent Declines in Opioid Prescriptions

RESEARCH TARGET:
Safe, Effective Strategies for Pain Management

Soergel DG, et al., Pain 2014. Manglik A, et al., Nature 2016. DeWire SM, et al., JPET 2013. Bohn LM, et al., Science 1999
A Promising New Generation Of Pain Therapeutics
Science = Solutions
Biased Mu-Opioid Receptor Ligands

Research on the Neurobiology of Pain
• Males had higher K opioid receptor availability than females presumably from increased dynorphin. • Could this help explain gender differences in pain
catastrophizing??
Vijay et al., Am J Nucl Med Mol Imaging. 2016 6(4):205-214.
Males
Females
Gender Differences in Kappa Opioid Receptor Availability

Direct Overdose InterventionNaloxone Distribution for opioid overdose victims.
The potential for direct intervention to save lives.
Ø “Evzio” naloxone auto-injector APPROVED BY FDA, April 3, 2014
Science = Solutions
Ø “Narcan Nasal Spray” naloxone APPROVED BY FDA, November 18, 2015

Receptor occupancy by INTRANASAL equivalent to INTRAVENOUS Naloxone
Baseline
Phillip et al. J Pharmacol ExpTher 2016
Intranasal Intravenous
NALOXONE REQUIRES FAST AND EFFICIENT DELIVERY as achieved with iv injection but few know how to inject
0 2 4 6 8 1 0 1 20
2
4
6
8
1 0
H o u rs P o s td o s e
Na
lox
on
e P
lasm
a C
on
ce
ntr
ati
on
(n
g/m
L)
1 x 2 0 m g /m L IN
2 x 2 0 m g /m L IN
1 x 4 0 m g /m L IN
2 x 4 0 m g /m L IN
0 .4 m g IM
Intranasal Narcan
Injectable
Blo
od C
once
ntra
tion
Positive pharmacology of nasal naloxone: Rapid onset and high peak blood level

Retail Pharmacy Prescriptions for Naloxone Increase Markedly
• Retail prescriptions show an increase of 9520% from the 4th quarter of 2013 to 2nd quarter 2016.
• Outpatient prescribing of naloxone may complement community-based distribution and first responder access.
Sources: Jones CM, Lurie PG, Compton WM. Am J Public Health. 2016;106(4):689-690; IMS Health, published https://www.performance.gov/content/reduce-opioid-related-morbidity-and-mortality Science = Solutions
0
5000
10000
15000
20000
25000
30000
35000
1Q2010
3Q2010
1Q2011
3Q2011
1Q2012
3Q2012
1Q2013
3Q2013
1Q2014
3Q2014
1Q2015
3Q2015
1Q2016
20142015
2016

Medications are Effective for Opioid Use Disorder
Medication Assisted Treatment (MAT) can DECREASE:• Opioid use• Opioid-related overdose deaths• Criminal activity• Infectious disease transmission
And INCREASE• Social functioning• Retention in treatment
Kakko J et al., The Lancet 2003.

Effective Medications for Opioid AddictionFull Agonist: Methadone (daily dosing)
Partial Agonist: Buprenorphine (3-4X week, or implant)
Antagonists: Naltrexone (monthly extended release)
effect
no effect
agonist antagonist
Binds to the receptor and activates it;
Full agonists have maximal effect.
Partial agonist have intermediate effect.
Prevent Heroin from binding.
Binds to receptor but has no effect.
Prevents heroin from binding.
Op
ioid
Eff
ec
t
Full Agonist(Methadone)
Partial Agonist(Buprenorphine)
Antagonist(Naltrexone)
Log Dose
Science = Solutions

Medications are Underused
25%
75%
MAT No MAT
In 2014, only 25% of opioid admissions had treatment plans that included receiving medications.
Treatment Episode Data Set (TEDS): 2004-2014.
Jones C et al., Am J Public Health 2015.
In 48 states and D.C., Opioid Abuse and Dependence Rates Exceed Buprenorphine Treatment Capacity

• Probuphine: buprenorphine implant; releases sustained dose for up to 6
months (FDA Approval May 26, 2016)
• Initiating buprenorphine treatment in the emergency department improves
treatment engagement and reduces illicit opioid use
• Extended release naltrexone initiated in criminal justice settings lowers
relapse rates and overdoses
• Abstinence from opioids over 12 Weeks with interim buprenorphine
Science Driven Solutions: Improving Addiction Treatment
Lee JD, et al., Addiction 2015;100:1005-1014
and New Eng J Med 2016;374:1232-1242
Abstinence with Interim Buprenorphine
Sigmon SC et al. N Engl J Med 2016.

Antibodies and Vaccines to Treat OUD and Prevent Overdose
•Heroin vaccine validated in primate model in 2017
•First vaccine for fentanyl and fentanyl analogs reported in a mouse model in 2016
•Reduces drug reaching the brain
•Protect high-risk individuals against overdose Bremer et al, 2017;
Bremer et al, 2016; Janda and Treweek, 2012.

Non-Pharmacological Treatments for Addiction
Salling and Martinez, 2016.
Transcranial Direct Current Simulation (tDCS)
Deep Brain Stimulation (DBS)Implanted electrodes emit electrical stimulation to targeted brain region
Transcranial Magnetic Stimulation (TMS)

Using Research to End the Opioid CrisisNIH Opioid Research Initiative
PAIN MANAGEMENTSafe, effective, non-addictive strategies
OPIOID ADDICTION
TREATMENTNew, innovative medications and
technologies
OVERDOSE REVERSAL
Interventions to reduce mortality
and link to treatment
Non-Opioid Analgesics
Biomarkers For Pain
Opioid Vaccines
Nonpharmacological Treatments (e.g. TMS)
Respiratory Stimulation Devices

• Complex biological, developmental and social aspects of substance use and addiction suggest multipronged responses.• The severity of the opioid crisis demands
urgent action.
Summary:
Advancing Addiction Science
www.drugabuse.gov
Science = Solutions

























![Non-opioid & Opioid IV Anesthetics Copy [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/55cf8c8a5503462b138d78d4/non-opioid-opioid-iv-anesthetics-copy-compatibility-mode.jpg)



