Embed Size (px)
Citation preview

AADS
Aitanctcs
F
D
A
2
dvances in the Treatment ofttention-Deficit/Hyperactivityisorder: A Guide for Pediatric Neurologists
haron B. Wigal, PhD, Stephanie Chae, Avni Patel, and Robin Steinberg-Epstein, MD
The purpose of this article is to assist pediatric neurologists in practice and in training to betterunderstand and distinguish between several of the most commonly prescribed treatments forattention-deficit/hyperactivity disorder (ADHD) in school-aged children. Among the variouspharmacotherapies available for ADHD, 4 specific medications will be reviewed: oral releaseosmotic system methylphenidate hydrochloride (CON; Concerta, McNeil Pharmaceuticals),lisdexamfetamine dimesylate (LDX; Vyvanse, Shire Pharmaceuticals), atomoxetine (ATX; Strat-tera, Eli Lilly), and guanfacine extended-release (GXR; Intuniv, Shire Pharmaceuticals). Thisarticle contains information including medication-release pattern, administration includingavailable dosing, adverse reactions, and case studies to serve as a guide to help determinewhen a particular treatment might be more appropriate than another. Although ADHD isapparent across the lifespan, this article will focus on children with ADHD from ages 6 to 12years old. Importantly, although a number of stimulant and nonstimulant treatment options areavailable for school-aged children diagnosed with ADHD, choosing the best treatment optionsis highly dependent on obtaining thorough family and medical histories.Semin Pediatr Neurol 17:230-236 © 2010 Elsevier Inc. All rights reserved.
6c
Muybdwlnnpdte
ToAeagA
ttention-deficit/hyperactivity disorder (ADHD) is themost common child psychiatric disorder of hyperactiv-
ty, impulsivity and/or inattention. It is a chronic conditionhat affects people of all ages from young children throughdulthood. Symptoms of ADHD are noticeable and diag-osed at various stages of life although more commonly inhildren before age 7 years. In children with ADHD, symp-oms may be apparent socially, emotionally, and academi-ally. ADHD may lead to low self-esteem, poor peer relation-hips, delinquencies, and substance abuse. Approximately
rom the Department of Pediatrics, Child Development Center, Universityof California, Irvine, CA.
r Sharon B. Wigal is a consultant for Abbott, McNeil, NuTec, Shire, Taisho,and the NIMH; has received grant/research support from Addrenex, EliLilly, McNeil, Next Wave Pharmaceuticals, Otsuka, Psychogenics, Quin-tiles, Shionogi Pharm, Shionogi Pharm, Shire, and the NIMH; and is onthe speaker or advisory boards for McNeil, the NIMH, Shire, and UCB.Dr Robin Steinberg-Epstein is a consultant for McNeil and Shire; hasreceived grant/research support from Addrenex, Eli Lilly, McNeil, NextWave Pharmaceuticals, Otsuka, Psychogenics, Quintiles, ShionogiPharm, Shire, and the NIMH; and is on the speaker or advisory boardsfor Eli Lilly, McNeil, and Shire.
ddress reprint requests to Sharon B. Wigal, PhD, Department of Pediatrics,Child Development Center, University of California, Irvine, CA 92612.
AE-mail: [email protected]
30 1071-9091/10/$-see front matter © 2010 Elsevier Inc. All rights reserved.doi:10.1016/j.spen.2010.10.005
5% of children identified with ADHD since childhood willontinue to exhibit symptoms as adults.1
To diagnose ADHD, the Diagnostic and Statistical Manual ofental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) issed.1 Approximately 3% to 7% of children from ages 8 to 15ears old meet criteria for ADHD. The diagnosis of ADHD cane divided into 3 categories: predominantly inattentive, pre-ominantly hyperactive-impulsive, and combined type,hich is both inattentive and hyperactive. The DSM-IV-TR
ists 9 different symptoms for both categories of inattentive-ess and hyperactivity-impulsivity (Table 1). To be diag-osed with one of the categories of ADHD, a child mustresent with 6 of the 9 symptoms of impairment in at least 2ifferent settings, such as classroom and home. These symp-oms must be present for at least 6 months and must not bexplained by other psychiatric diagnoses.
Based on current research, including the Multimodalityreatment Study of Children with ADHD (MTA), there isverwhelming consensus that the primary treatment ofDHD is medication and that accessory symptoms are ben-fited by multimodal treatment (a combination of medicationnd alternative treatments).2 This is further supported by theuidelines set forth by 3 major academies (the Americancademy of Neurology, the American Academy of Child &
dolescent Psychiatry, and the American Academy of Pedi-
aase
TTs
vtAeAatsfilpoap
SSmsAlafsd
CTtFaidcm
tami
SptCOoa
lodip
TD
I
H
D
ADHD treatment update 231
trics) as well as by international consensus.3 Although somelternative treatments (eg, nutrition and exercise) have beenhown to improve psychiatric comorbidities, there is limitedvidence to suggest their direct benefit for ADHD.4
reatment Algorithmhe Texas Children’s Medication Algorithm Project5 was de-
able 1 DSM-IV-TR Criteria of Symptomatology in Attention-eficit Disorder
nattention: must include at least 6 of the followingsymptoms of inattention that must have persisted forat least 6 months to a degree that is maladaptive andinconsistent with developmental level:
Often fails to give close attention to details or makescareless mistakes in schoolwork, work, or otheractivities
Often has difficulty sustaining attention in tasks or playactivities
Often does not seem to listen to what is being saidOften does not follow through on instructions and fails
to finish schoolwork, chores, or duties in theworkplace (not due to oppositional behavior or failureto understand instructions)
Often has difficulties organizing tasks and activitiesOften avoids or strongly dislikes tasks (such as
schoolwork or homework) that require sustainedmental effort
Often loses things necessary for tasks or activities(school assignments, pencils, books, tools, or toys)
Often is easily distracted by extraneous stimuliOften forgetful in daily activitiesyperactivity/impulsivity: must include at least 6 of the
following symptoms of hyperactivity-impulsivity thatmust have persisted for at least 6 months to a degreethat is maladaptive and inconsistent withdevelopmental level:
Hyperactivity evidenced by fidgeting with hands or feet,squirming in seat
Hyperactivity evidenced by leaving seat in classroom orin other situations in which remaining seated isexpected
Hyperactivity evidenced by running about or climbingexcessively in situations where this behavior isinappropriate (in adolescents or adults, this may belimited to subjective feelings of restlessness)
Hyperactivity evidenced by difficulty playing or engagingin leisure activities quietly
Hyperactivity evidenced by often on the go or acting asif driven by a motor
Hyperactivity evidenced by talking excessivelyImpulsivity evidenced by blurting out answers to
questions before the questions have been completedImpulsivity evidenced by showing difficulty waiting in
lines or awaiting turn in games or group situationsImpulsivity evidenced by interrupting or intruding on
others
ata from DSM-IV-TR. Copyright 2000 American Psychiatric Asso-ciation.
igned to be used in community mental health centers, pro- m
iding suggestions for drug choice as it applies to ADHDreatment. As a guide that serves as the basis for the Americancademy of Child & Adolescent Psychiatry practice param-ter on the treatment of children and adolescents withDHD,6 it offers opportunities to determine pharmacother-py with maximal benefits while taking into considerationhe unique attributes of any given case. Overall, this consen-us-driven algorithm establishes the use of a stimulant for therst stage of treatment followed by a second stage of stimu-
ant, progressing to nonstimulant use. Although some as-ects of this algorithm are no longer relevant, such as the usef pemoline (mostly because of concerns regarding fatal hep-totoxicity), the general rationale still can be used and ap-lied to presently available agents.
timulantstimulants have been used to treat symptoms of ADHD forore than 50 years. As mentioned earlier, the Texas Consen-
us Conference Panel on Pharmacotherapy of ChildhoodDHD developed the use of stimulant medications as first-
ine options for the medical management of children anddolescents with classic ADHD without other complicatingeatures.5,6 The expectation is that 70% of patients will re-pond to the first stimulant that is tried with the recommen-ation that a second be tried to yield up to an 80% benefit.7
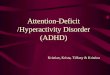
ase Study 1his child has been diagnosed with ADHD, inattentive sub-
ype and comorbid oppositional defiant disorder (ODD; seeigure 1 below for Case Study 1). Following the treatmentlgorithm,5 this would suggest starting with a stimulant med-cation. One must first consider whether there are contrain-ications to a stimulant. We know that there is no knownardiac history in this patient to suggest a need for a pretreat-ent echocardiogram. No laboratory studies are necessary.Given that her weight is greater than the 95th percentile,
here is no concern that weight loss will be a problem for her,nd, in fact, stimulants may at first be helpful. Although thereay be some initial weight loss, we would not expect ongo-
ng weight loss.In general, over two thirds of the Multimodality Treatment
tudy of Children with ADHD sample exhibited concurrentsychiatric disorders.2 As for ODD, the literature supportshe use of stimulants in patients with ODD and ADHD.8
ontrolling ADHD with a stimulant may offer benefits forDD symptoms. There is certainly evidence that in the facef ODD, stimulants still work to improve ADHD symptomsnd do not worsen the ODD.3
How does one know which stimulant to choose? Stimu-ants generally belong to either the methylphenidate familyr the amphetamine family. The first consideration is one ofuration. Given that this is a 9 year old with homework that
s taking an inordinate amount of time to complete and herroblems exist throughout the school day, a long-acting
edication would be the most appropriate. Table 2 provides
km
cSMftposLdatssesam
NAhaolpdipllstttbik
eated w
232 S.B. Wigal et al
ey details of a few research studies regarding the develop-ent of 2 of these products.For the purpose of our discussion, we have chosen to
ompare 2 long-acting medications: lisdexamfetamine (LDX;hire Pharmaceutical, Wayne, PA) and Concerta (CON;cNeil Pharmaceuticals, Fort Washington, PA) (See Table 3
or summary information about these 2 stimulants). Al-hough they have similar duration of action and side effectrofiles, there are subtle differences that may lead to a choicef one over the other. For example, studies suggest that theeverity of appetite suppression may be more significant forDX and other amphetamines than for other methylpheni-ate products with the same average duration of action. Suchn “adverse effect” might actually be of benefit for this par-icular patient. By contrast, if this child could not be taught towallow a pill, LDX can be combined with a liquid to make aolution. Overall, either of these medications serves as anxcellent option for her. However, should she respond withignificant sleep-onset problems, one might choose a shorter-cting (ie, not a sustained- or extended-release) stimulant
Identification and Presenting Complainfor diagnosis and treatment of possible Athe last 3 years teachers had mentioned problems staying on task during schoolwsprinkling of “B’s” and “D’s”. She has diffiend to see what happens. Mom often findbottom of her backpack. Her mom also mto and is quite a daydreamer. She misplaher; always forgetting things at school. Shhomework assignment.
In addition, her mother reports that the tetime making friends. She also has a lot ofights and demands things her way. She git comes to her relationship with her broth
Physical Exam: She is moderately obesotherwise has a normal general and neur
Family History: There is a maternal histand grandmother having ADHD diagnosebehavior or mental health problems. No fdeath or structural cardiac defects.
Supporting Data: ADHD rating scales ssignificant elevations in inattentive and op
Diagnosis: ADHD, predominantly inatte
Treatment considerations and diagnos- Child’s weight is > 95th percentile- Oppositional Defiant Disorder (O- No other psychiatric condition ide
disorders)
Key questions for differential treatmen- Is the child’s weight within the no- Is ODD or some other comorbid d- Are there any contraindications to
Case
Figure 1 A case study of a child tr
edication. l
onstimulantslthough stimulant drug treatments have proved to beighly effective and safe in treating symptoms of ADHD,pproximately 20% of children with ADHD fail to respondr have significant side effects to one of the first 2 stimu-ants that are tried. Following the treatment algorithm,5
ractitioners are encouraged to consider nonstimulantrugs as second-line treatments, with the exception of
ndividuals with ADHD having an active substance abuseroblem, comorbid anxiety, or tics, for which nonstimu-
ants would be the first-line treatment.9 Thus, nonstimu-ants are used when ADHD patients fail to respond totimulants or have increased side effects. Furthermore,here are subgroups of children whose comorbid condi-ions (eg, anxiety, tics) may be exacerbated by stimulantreatment. Thus, alternate pharmacotherapy may yieldeneficial effects on accessory symptoms while also treat-
ng primary ADHD symptoms. Table 4 summarizes severaley studies regarding development of 2 specific nonstimu-
-year-old girl was brought into the clinic er mother was concerned because for daughter was seated up front due to r grades are mostly “C’s” with a ishing books and likes to skip to the ompleted, ungraded homework at the that she does not listen when spoken
loses things that are not important to takes hours to complete a simple
also mentioned that she has a hard getting along with her mom; she picks ng with her dad and is a tomboy when initiates fights with her brother.
ht 47 kg (>95th percentile)) but xam.
DHD, including the patient’s mother girl’s father does not have any history of istory exists for sudden, unexpected
d by both parent and teacher showed nal symptoms.
btype with a comorbid problem of ODD
ulation:
gnosed. (i.e., anxiety or autism spectrum
nge, high or low? r present with ADHD symptoms? ent?
#1
ith stimulant pharmacotherapy.
ts: A 9DHD. Hthat herork. Heculty fins her centionsces or e can
achers f troubleets aloer. She
e (weigologic e
ory of As. The amily h
ubmittepositio
ntive su
tic form DD) diantified
t: rmal raisorde treatm
Study
ant medications.

T
S
S
W
B
P
W
O
T
DADIODA
C
T
F
W
M
G
B
C
S
ADHD treatment update 233
able 2 Representative Studies of 2 Stimulant Treatments for ADHD
OROS Methylphenidate Hydrochloride
Citation Emphasis Conclusion
wanson et al, 200211 Laboratory school study comparing objective activitylevels during structured classroom activities andoutside recess activities
CON treatment improved attention and behavior duringclassroom seatwork but generally showed nodifference from placebo in the playground
wanson et al, 200412 Comparative trial of 2 long-acting MPH products inthe laboratory school setting
The specific time-course profiles are demonstrated,which show differences in onset and duration
olraich et al, 200113 Randomized study comparing placebo, immediaterelease MPH tid and CON
Demonstrated significance of both MPH treatmentsover placebo with equivalent efficacy to each other
Lisdexamfetamine
Citation Emphasis Conclusion
iederman, et al,200714
Laboratory school study of LDX demonstrating itslong acting effects
Significant improvements were noted from the firsttime point measured until 12 h. However, nopredose baseline was measured
ennick, 2010 15 Absorption and metabolic conversion of LDX tod-amphetamine
Blood vs liver tissue as responsible for the conversionof the inactive prodrug to active amphetaminetreatment
igal, et al, 200916 Laboratory school study evaluating the onset andoffset effects of LDX
Placebo controlled study of LDX with efficacy extendedin both directions from Biederman et al, 200714
ROS, Oral release osmotic system; CON, Concerta (OROS methylphenidate hydrochloride); MPH, Methylphenidate; tid, 3 times per day.
able 3 Summary Information for 2 Commonly Prescribed Stimulants to Treat ADHD
Stimulants
Product OROS Methylphenidate Hydrochloride (Concerta) LDX Dimesylate (Vyvanse)
elivery System Methylphenidate Oral Release Osmotic System d-amphetamine prodrugpproval by FDA August 2000 February 2007oses 18, 27, 36, 54, and 72 mg; (2 � 36 mg) Twenty, 30, 40, 50, 60, and 70 mg
nitial dose 18 mg 30 mgnset of activity 1 h 1.5 huration of activity Up to 12 h postdose, extended Up to 13 h postdose, extendeddministration Once daily in the morning with or without food; Swallow
whole; do not crush or chewDaily in the morning with or without food;
May dissolve it in water.ommon side effects Decreased appetite, dry mouth, trouble sleeping, dizziness,
stomach ache, increased sweating, headache, nausea,Upper abdominal pain, decreased appetite,
dry mouth, dizziness, irritability,
anxiety, weight loss, irritability insomnia, weight lossable 4 Representative Studies of 2 Nonstimulant Treatments for ADHD
Atomoxetine
Citation Study Description Conclusion
araone et al, 200717 Statistical extension of Wigal, et al, laboratoryschool study (see below)
Forecasting to 8-wk treatment period showed continuedgreater efficacy for mixed amphetamine salts,extended-release MAS-XR compared with ATX
igal et al, 200518 Laboratory school study measuring time courseeffects of ATX and MAS-XR
Short-term study replicating significant ATX within 1-wkof initial dosing and time course effects incomparison with amphetamine treatment
ichelson et al, 200219 Clinic study of ATX with quality of lifemeasurements
Demonstrated treatment effects within 1 wk of usage
reenhill et al, 200720 Comparison of two different methods for initiatingATX to reduce incidence of adverse events
Lower risk of adverse events if over the first few weeksof treatment, patients receive doses divided into 2 perday and titrated to full dose (1.2 mg/kg/d) moreslowly
Guanfacine Extended Release
Citation Study Description Conclusion
iederman et al, 200821 Forced dose escalation study of GXR vs placebo for8 wks
Improvements with GXR similar to other nonstimulants
onnor & Rubin,201022
Review paper on GXR Mild slowing of heart rate and some lowering of systolicblood pressure and diastolic blood pressure occursand requires vital sign monitoring during treatment
pencer et al, 200923 Coadministration of GXR and stimulant medication Increased ADHD symptom improvement with no new
adverse events
CT(tncbaa
ssickinstcass
mltfmcikrr
sstAthm
wrt
ted wit
234 S.B. Wigal et al
ase Study 2his child was diagnosed with ADHD, combined subtypesee Figure 2). However, there are some distinct concernshat may alter the choice of medication. Although it wouldot be incorrect to choose a stimulant as the treatment ofhoice, one must consider how this child presents (eg, highlood pressure, a family history of a tic disorder, low weight,nd a potential comorbid anxiety issue). Each of these issuesre explored more closely later.
Although studies of stimulant medication typically show atatistically significant increase in blood pressure, they do nothow a clinically relevant increase. However, one of the med-cation options, guanfacine extended-release (GXR) (a re-ently available extended-release form of guanfacine), is anown antihypertensive agent and thus can cause decreases
n blood pressure. Therefore, one might opt to consider thisonstimulant as a strong possibility because, in this case,uch blood pressure effects are an advantage. It is importanto become familiar with the side effect profile of each medi-ation because they can sometimes be used to the patient’sdvantage (Table 5). In addition, instructions to familieshould be clear about discontinuation practices. For in-
Identification and Presenting Complaiconcerns regarding inconsistent grades areports that he will get “A’s” on tests but w“C’s” as final grades. At a parent-teacherdisrupts other students when they are sptalkative. He has trouble listening and folclass. He feels as if his teacher “hates” h
He says he does not understand why othhis older brother, with whom he is continuis video games. His mother also notices tmessy and disorganized. Mom is also conthat he sleeps with the light on. He will nextremely afraid of dogs, even the neigh
Physical Exam: The patient weighs 26.4has normal general and neurologic exam130/85.
Family History: There is no maternal or however the father had an alcohol probleolder brother is diagnosed and in treatmeexists for sudden, unexpected death or s
Diagnosis: ADHD, combined subtype
Treatment considerations: - Sibling with chronic tic disorder - Blood pressure - Co-morbid symptoms of anxiety
Case
Key questions for differential treatmen- Is there a family history of tics or - Is the child’s blood pressure with
Figure 2 A case study of a child trea
tance, GXR should be tapered off with decreases in incre- h
ents of 1 mg every 3 to 7 days as directed on the productabel. This would even be important for a child with hyper-ension because it would be very important for this child’samily to be aware of potential rebound hypertension if theedication were to be suddenly withdrawn. Of course, any
hild with elevated blood pressure also requires further med-cal investigation to determine the etiology. In a child withnown hypertension being managed by a cardiologist, neph-ologist, or pediatrician, that physician should be consultedegarding possible medication choices.
As for the history of a tic disorder, there is evidence thattimulant treatment, at least temporarily, may increase tics inome individuals.10 Longer-term studies show, however, thathere is no overall increase in tics in most individuals.10 As forTX, there is no evidence of an effect on tics in either direc-
ion. GXR, in contrast, may decrease tics because guanfacineas commonly been prescribed as a primary treatment forotor tics in the non–extended-release form.Stimulants and ATX may lead to decreased appetite and
eight loss, but GXR does not appear to have an effect in thategard. Finally, anxiety seems to be a presenting problem forhis child. The stimulants may worsen anxiety. GXR generally
is 10 ½-year-old boy presents with eral behavioral complaints. His mother turn in projects and will end up with nce, his teacher mentioned that he
blurts out answers, and is very irections, and often daydreams in
favors other students in the class.
’t see things the way he does including uing. The only thing he will sit still for backpack and his room are extremely because he is still so afraid of the dark d the night at a friend's house and is ppy.
t below 5th percentile) and otherwise the exception of blood pressure being
l history of mental health disorders; to marriage. In addition, the patient’s chronic tic disorder. No family history l cardiac defects.
y #2
e’s Disorder? al limits, high or low?
h nonstimulant pharmacotherapy.
nts: Thnd sevill not
confereeaking,lowing dim and
ers donally arghat his cernedot spenbor's pu
kg (juss, with
paternam priornt for atructura
Stud
t: Tourettin norm
as no effect on anxiety, whereas ATX has mild anxiolytic

bocsf
rfirAGf
ATs
CEtiwfigteh
R
1
1
1
1
1
1
1
1
1
1
TN
FD
IO
D
A
C
ADHD treatment update 235
enefits. Therefore, if one had the sense that anxiety were anverriding issue, ATX might be the medication of choice. Ofourse, one might alternatively consider medical therapiespecifically focused on anxiety, but these options will not beurther considered in this review.
As mentioned earlier, stimulants produce an overall moreobust response, with over 70% of subjects responding to therst stimulant tried and up to 80% to the second one. Theesponse to the nonstimulant medications (both GXR andTX) is closer to 50%. Prolonged sedation may be seen withXR in the first several weeks of use and with ATX in the first
ew days of use.For this patient, it seems likely that starting either GXR or
TX may provide some unique benefits or protections. Seeable 5 for summary information for each of these 2 non-timulant medications.
onclusionsach of the reviewed stimulant and nonstimulant medica-
ions has its own set of benefits and drawbacks. Thus, it ismperative for individual practitioners to gain familiarityith the nuances of treatment options. By reviewing researchndings and medication properties of each, following the sug-ested practical algorithm, and carefully choosing the best op-ion for a particular patient profile, neurologists can gain clinicalxperience in the optimal treatment of ADHD in children while
able 5 Summary Information for 2 Commonly Prescribedonstimulants to Treat ADHD
Nonstimulants
Product
GuanfacineExtended-Release
(Intuniv)Atomoxetine(Strattera)
DA approval September 2009 November 2002oses 1, 2, 3, and 4 mg 10,18,25,40, 60,
80, and 100 mgnitial dose 1 mg 0.5 mg/kgnset ofactivity
Some effects in 1 wk Some effects in1 wk
uration ofactivity
6-8 h extended 7-9 h and up to 24 h
dministration Once daily in themorning. Swallowwhole; do not crushor chew
Once or twice dailyby mouth with orwithout food
ommon Sideeffects
Sleepiness, dry mouthdrowsiness,dizziness low bloodpressure, irritability,headache,constipation, nausea,not hungry(decreased appetite),stomach pain
Abdominal pain,decreasedappetite, nauseaor vomiting,dizziness, moodswings,somnolence
elping them reach their true potential.
eferences1. American Psychiatric Association, DSM: IV TR: Diagnostic and Statis-
tical Manual of Mental Disorders (ed 4). Washington, DC, AmericanPsychiatric Publishing, Inc, 2000, pp 78-85
2. MTA Cooperative Group: A 14-month Randomized Clinical Trial ofTreatment strategies for attention deficit hyperactivity disorder. ArchGen Psychiatry 56:1073-1086, 1999
3. Kutcher S, Aman M, Brooks SJ, et al: International consensus statementon attention-deficit/hyperactivity disorder (ADHD) and disruptive be-havior disorders (DBDs): clinical implications and treatment practicesuggestions. Eur Neuropsychopharmacol 14:11-28, 2004
4. Larzelere MM, Campbell JS, Robertson M: Complementary and alter-native medicine usage for behavioral health indications. Prim Care37:213-236, 2010
5. Pliszka SR, Crismon ML, Hughes CW, et al: Texas Consensus ConferencePanel on pharmacotherapy of childhood attention deficit hyperactivitydisorder. Revision of the algorithm for pharmacotherapy of attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 45:642-657, 2006
6. Pliszka S: Practice parameter for the assessment and treatment of chil-dren and adolescents with attention-deficit/hyperactivity disorder.J Am Acad Child Adolesc Psychiatry 7:894-921, 2007
7. Elia J, Ambrosini PJ, Rapoport JL: Treatment of attention-deficit-hyper-activity disorder. N Engl J Med 340:780-788, 1999
8. Connor DF, Doerflor LA: Attention-deficit/hyperactivity disorder andcomorbid oppositional defiant disorder or conduct disorder. Curr At-tention Dis Rep 1:5-11, 2009
9. American Academy of Child and Adolescent Psychiatry (AACAP): Of-ficial action: Practice parameter for the assessment and treatment ofchildren and adolescents with attention-deficit/hyperactivity disorder.J Am Acad Child Adolesc Psychiatry 46:894-921, 2007
0. Poncin Y, Sukhodolsky DG, McGuire J, et al: Drug and non-drug treat-ments of children with ADHD and tic disorders. Eur Child AdolescPsychiatry 7 16:78-88, 2007 (suppl 1)
1. Swanson J, Gupta S, Williams L, et al: Efficacy of a new pattern ofdelivery of methylphenidate for the treatment of ADHD: Effects onactivity level in the classroom and on the playground. J Am Acad ChildAdolesc Psychiatry 41:1306-1314, 2002
2. Swanson JM, Wigal SB, Wigal T, et al: A comparison of once-dailyextended release methylphenidate formulations in children with atten-tion-deficit/hyperactivity disorder in the laboratory school (The Co-macs Study). Pediatrics 113:206-216, 2004
3. Wolraich ML, Greenhill LL, Pelham W, et al: Randomized, controlledtrial of OROS methylphenidate once a day in children with attention-deficit/hyperactivity disorder. Pediatrics 108:883-892, 2000
4. Biederman J, Boellner SW, Childress AC, et al: Lisdexamfetamine dime-sylate and mixed amphetamine salts extended-release in children withADHD: A double-blind, placebo-controlled, crossover analog class-room study. Biol Psychiatry 62:970-976, 2007
5. Pennick M: Absorption of lisdexamfetamine dimesylate and its enzy-matic conversion to d-amphetamine. Neuropsychiatr Dis Treat 6:317-327, 2010
6. Wigal SB, Kollins SH, Childress AC, et al: A 13-hour laboratory schoolstudy of lisdexamfetamine dimesylate in school-aged children withattention-deficit/hyperactivity disorder. Child Adolesc Psychiatry MentHealth 3:17, 2009
7. Faraone SV, Wigal SB, Hodgkins P: Forecasting three-month outcomesin a laboratory school comparison of mixed amphetamine salts ex-tended release (Adderall XR) and atomoxetine (Strattera) in school-aged children with ADHD. J Atten Disord 11:74-82, 2007
8. Wigal SB, McGough JJ, McCracken JT, et al: A laboratory school com-parison of mixed amphetamine salts extended release (Adderall XR)and atomoxetine (Strattera) in school-aged children with attention def-icit/hyperactivity disorder. J Atten Disord 9:275-289, 2005
9. Michelson D, Allen AJ, Busner J, et al: Once-daily atomoxetine treat-ment for children and adolescents with attention deficit hyperactivitydisorder: A randomized, placebo-controlled study. Am J Psychiatry
159:1896-1901, 2002
2
2
2
2
236 S.B. Wigal et al
0. Greenhill LL, Newcorn JH, Gao H, et al: Effect of two different methodsof initiating atomoxetine on the adverse event profile of atomoxetine.J Am Acad Child Adolesc Psychiatry 46:566-572, 2007
1. Biederman J, Melmed RD, Patel A, et al: A randomized, double-blind,placebo-controlled study of guanfacine extended release in children andadolescents with attention-deficit/hyperactivity disorder. Pediatrics 121:
e73-e84, 20082. Connor DF, Rubin J: Guanfacine extended release in the treatment ofattention deficit hyperactivity disorder in children and adolescents.Drugs Today 46:299-314, 2010
3. Spencer TJ, Greenbaum M, Ginsberg LD, et al: Safety and effectivenessof coadministration of guanfacine extended release and psychostimu-lants in children and adolescents with attention-deficit/hyperactivity
disorder. J Child Adolesc Psychopharmacol 19:501-510, 2009