Embed Size (px)
Citation preview
Advances in Personalised Medicine and Potential Impact on the the MDT
Dr Alastair Greystoke
Senior Lecturer and Honorary Consultant Medical Oncologist,
Northern Centre for
Cancer Care, Freeman Hospital, Newcastle
0 1 2 3 4 5 6 7 8 >8
0
5
10
15
20
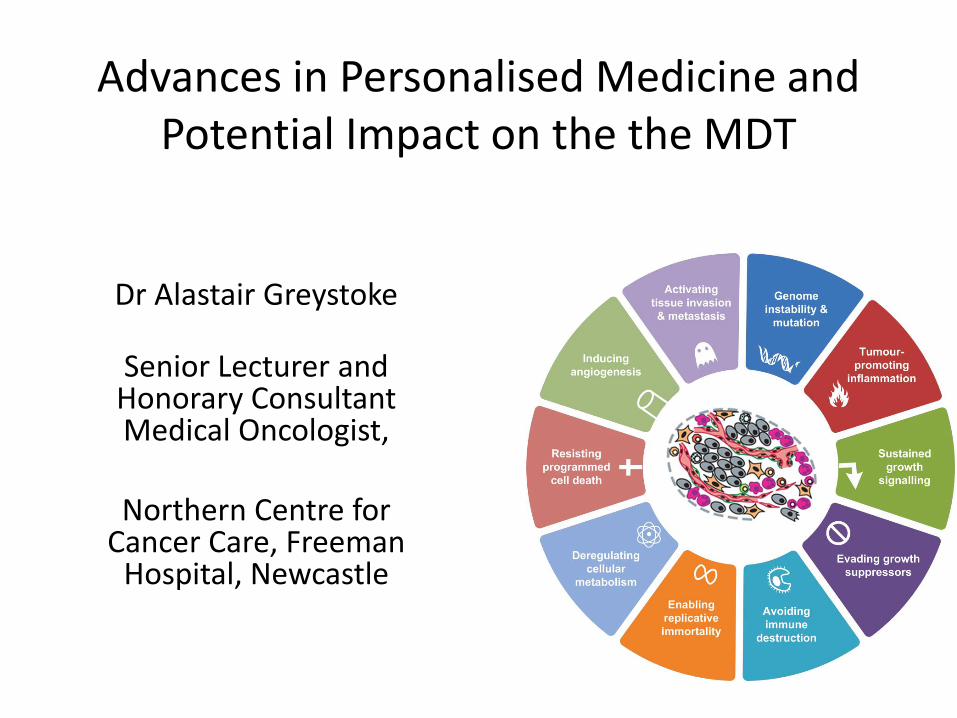
ACE-27 SCore
% P
atie
nts
0 1 2 3 4
0
10
20
30
40
50
Perfomance Status
% P
atie
nts
Newcastle upon Tyne Hospitals NHS Foundation Trust audit data 2013
For better, for worse? A review of the care of patients who died within 30 days of receiving systemic anti-cancer therapy. NCEPOD 2008
Concerns over tolerability in a patient population with multiple co-morbidities impacts on therapy rates
Potential ways to improve treatment outcome in NSCLC
• Optomise chemotherapy
– (bevaciazumab)/nintedanib
• Targeted therapy
– (EGFR/ALK (ROS-1, C-Met……))
• Immunotherapy
• ?Treat more patients with safer drugs?
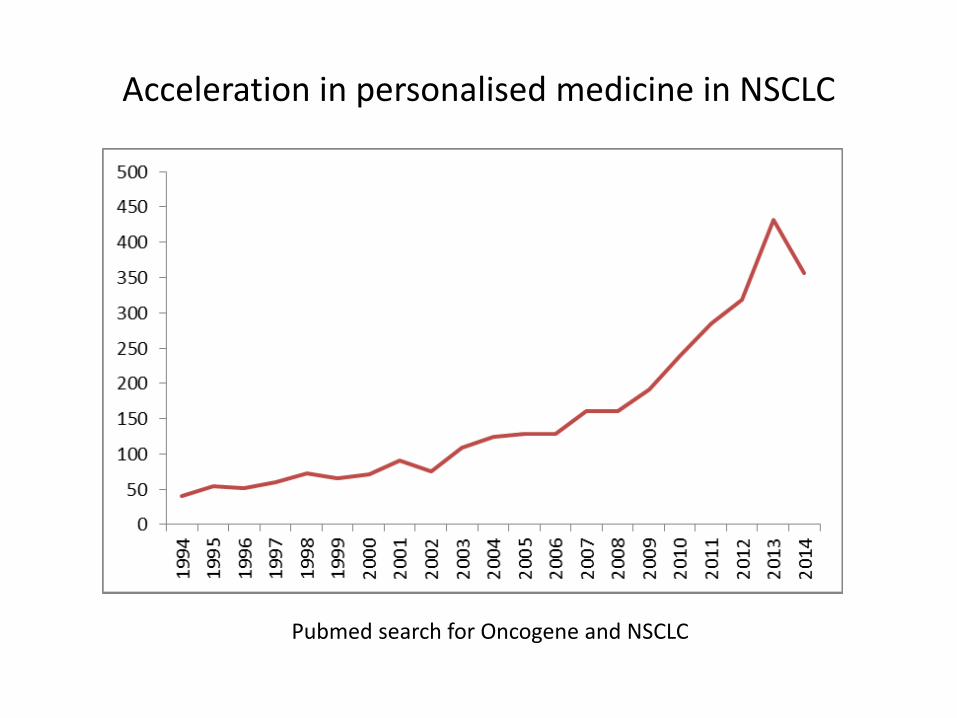
Acceleration in personalised medicine in NSCLC
Pubmed search for Oncogene and NSCLC
Importance of EGFR-ALK • Different disease
– Demographics
– Pattern of spread
– Prognosis
• Different treatments
– EGFR inhibitors (1st -3rd generation)
– ALK inhibitors (1-2nd generation)
• Paradigm shift in the way we look at NSCLC
– SMP2/Matrix
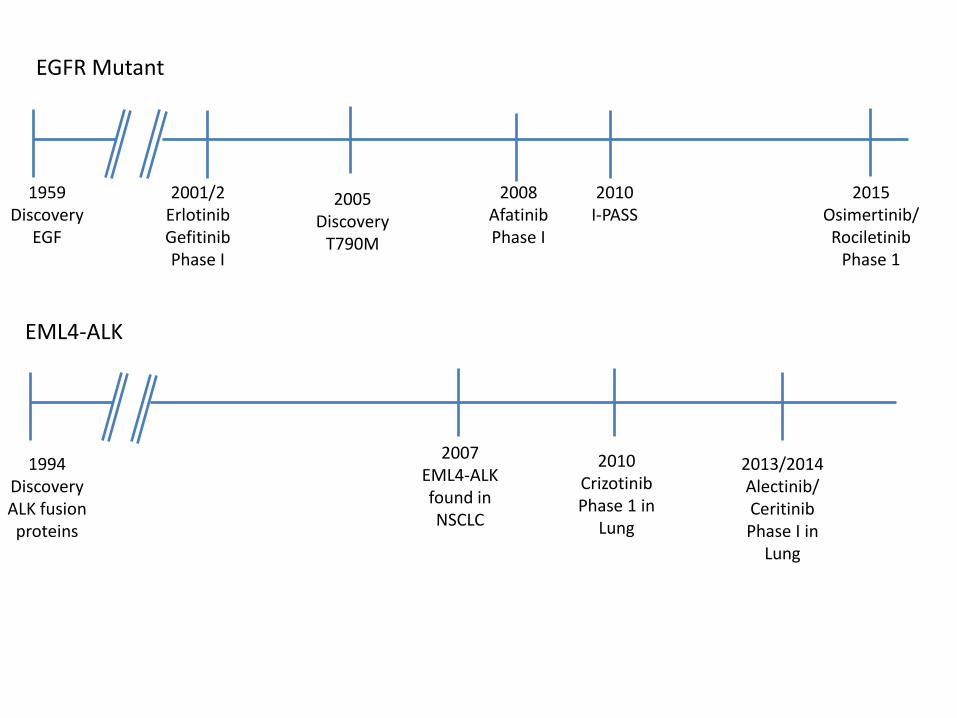
1959 Discovery
EGF
2001/2 Erlotinib Gefitinib Phase I
2010 I-PASS
2005 Discovery
T790M
2015 Osimertinib/Rociletinib
Phase 1
2008 Afatinib Phase I
2007 EML4-ALK found in NSCLC
1994 Discovery ALK fusion proteins
2010 Crizotinib Phase 1 in
Lung
2013/2014 Alectinib/ Ceritinib Phase I in
Lung
EGFR Mutant
EML4-ALK
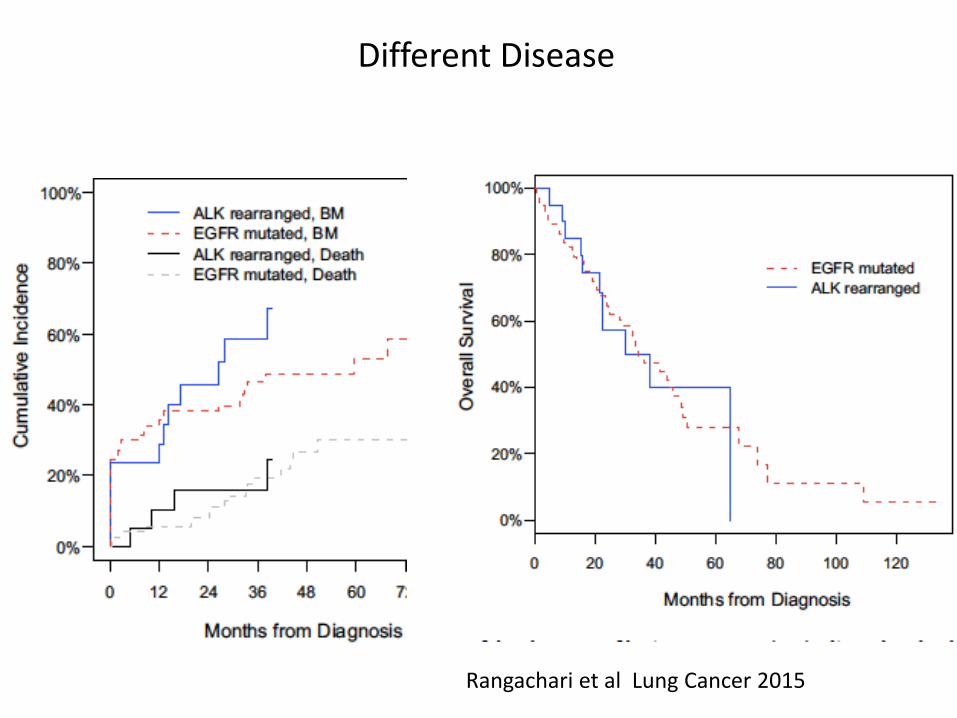
Rangachari et al Lung Cancer 2015
Different Disease
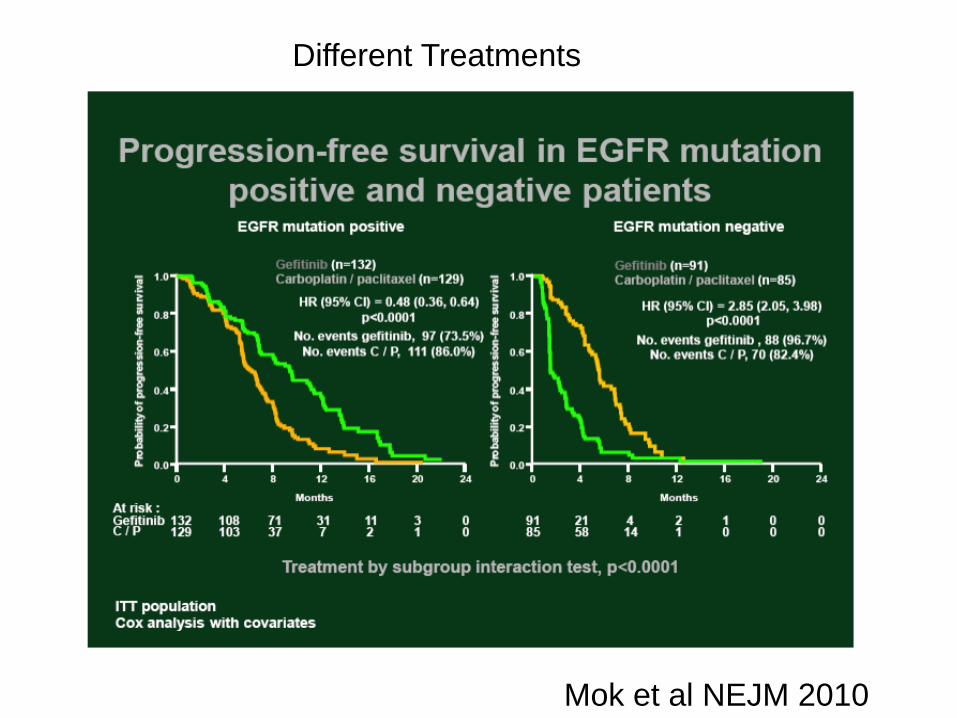
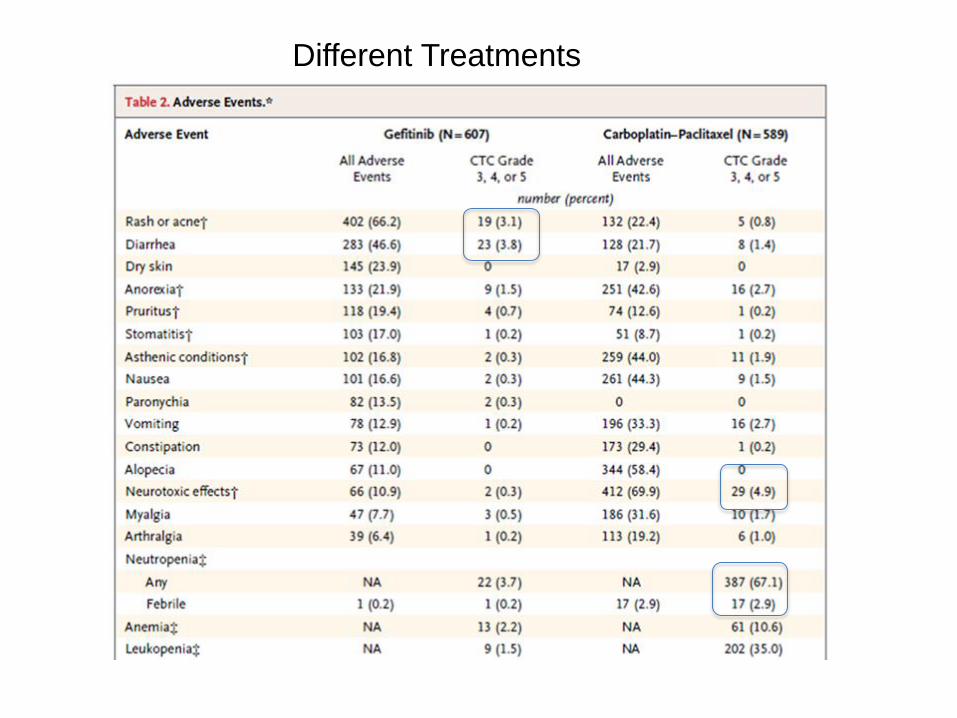
Different Treatments
Mok et al NEJM 2010
Different Treatments
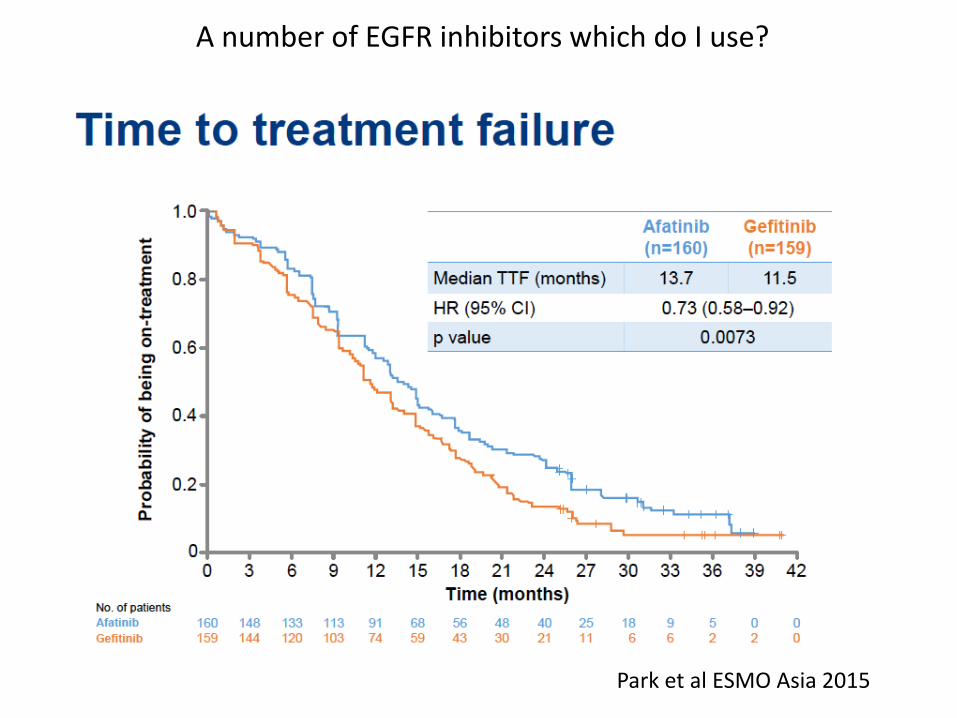
A number of EGFR inhibitors which do I use?
Park et al ESMO Asia 2015
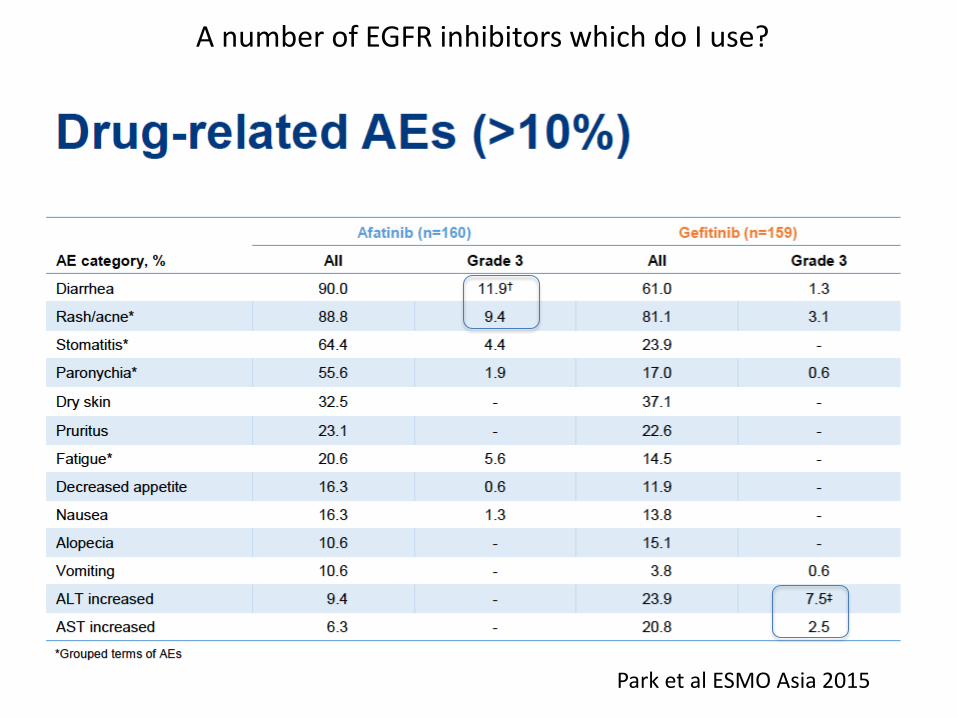
A number of EGFR inhibitors which do I use?
Park et al ESMO Asia 2015
ALK inhibitors
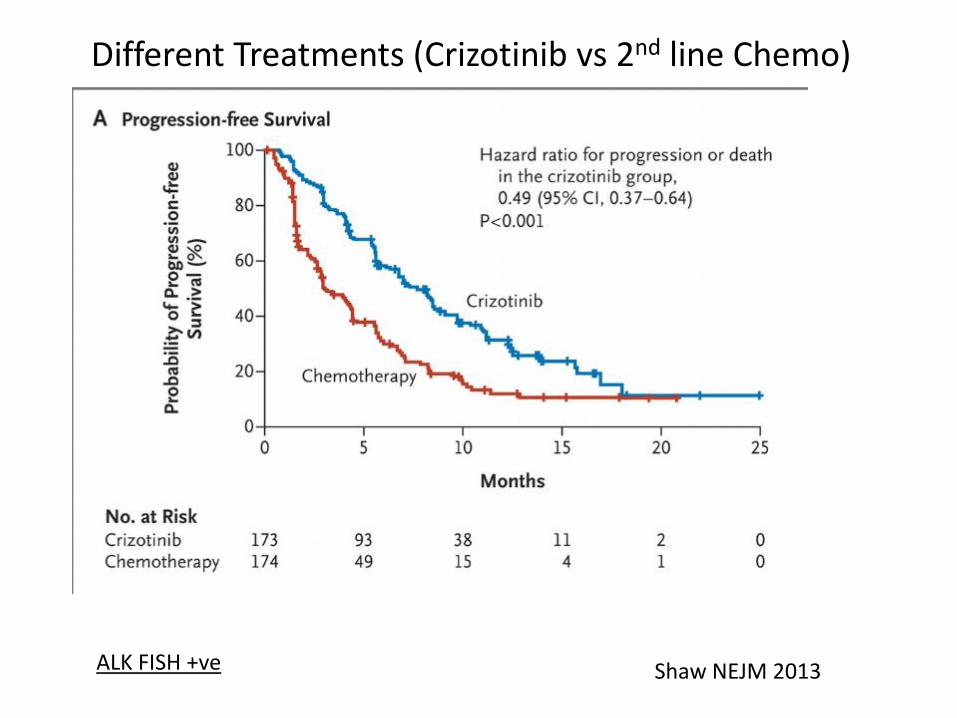
Different Treatments (Crizotinib vs 2nd line Chemo)
Shaw NEJM 2013 ALK FISH +ve
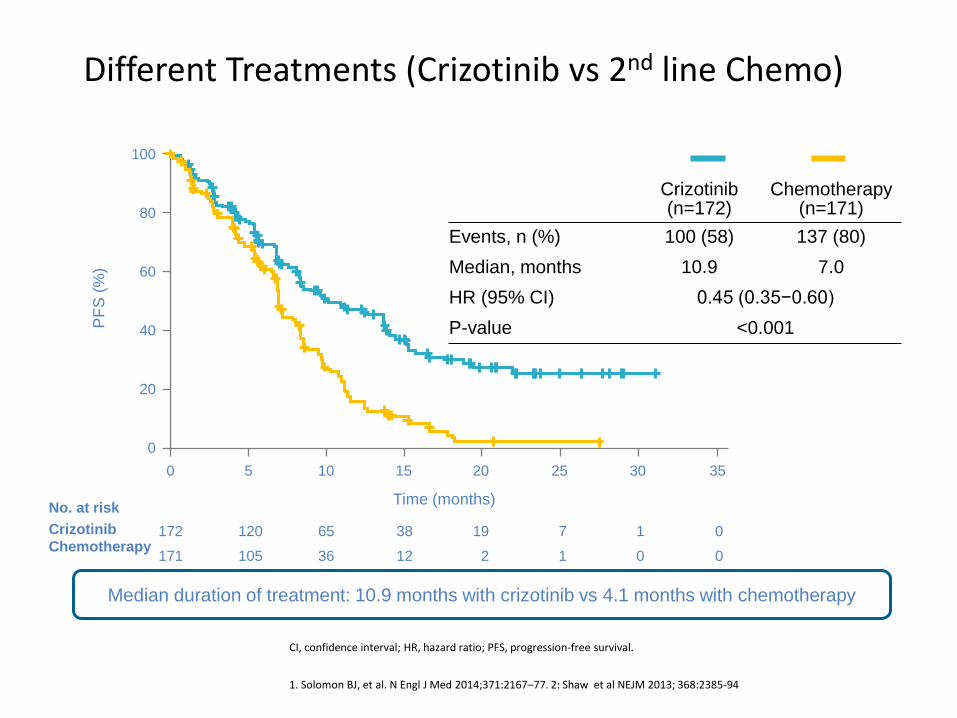
CI, confidence interval; HR, hazard ratio; PFS, progression-free survival.
1. Solomon BJ, et al. N Engl J Med 2014;371:2167–77. 2: Shaw et al NEJM 2013; 368:2385-94
PF
S (
%)
100
80
60
40
20
0
Time (months)
172 120 65 38 19 7 1 0
171 105 36 12 2 1 0 0
0 5 10 15 20 25 30 35
Crizotinib (n=172)
Chemotherapy (n=171)
Events, n (%) 100 (58) 137 (80)
Median, months 10.9 7.0
HR (95% CI) 0.45 (0.35−0.60)
P-value <0.001
Median duration of treatment: 10.9 months with crizotinib vs 4.1 months with chemotherapy
Crizotinib
Chemotherapy
No. at risk
Different Treatments (Crizotinib vs 2nd line Chemo)
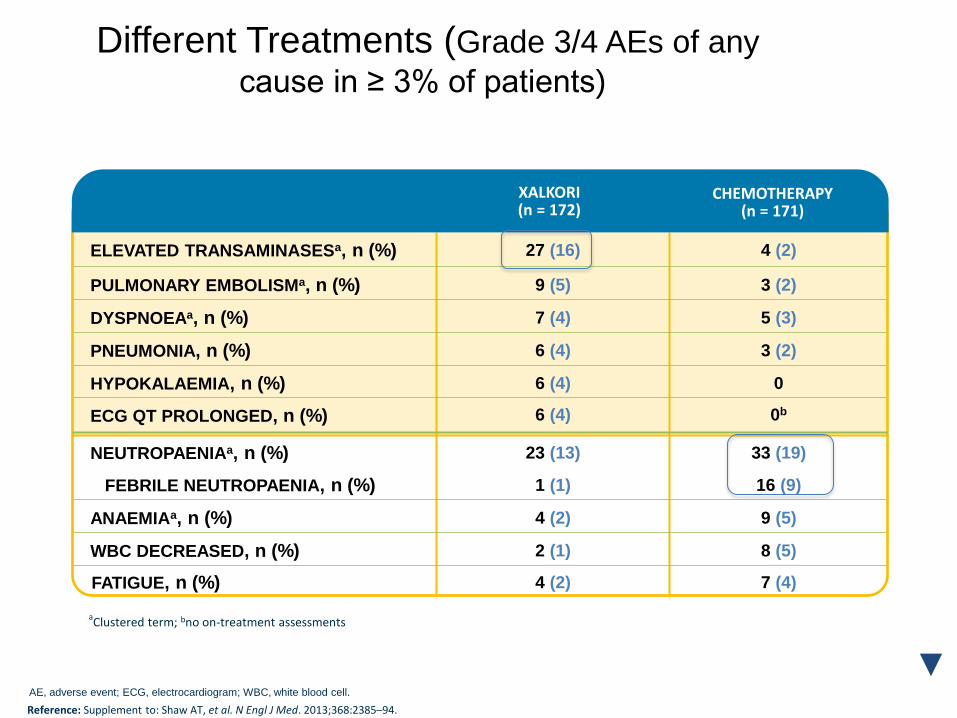
Different Treatments (Grade 3/4 AEs of any
cause in ≥ 3% of patients)
ELEVATED TRANSAMINASESa, n (%) 27 (16) 4 (2)
PULMONARY EMBOLISMa, n (%) 9 (5) 3 (2)
DYSPNOEAa, n (%) 7 (4) 5 (3)
PNEUMONIA, n (%) 6 (4) 3 (2)
HYPOKALAEMIA, n (%) 6 (4) 0
ECG QT PROLONGED, n (%) 6 (4) 0b
NEUTROPAENIAa, n (%) 23 (13) 33 (19)
FEBRILE NEUTROPAENIA, n (%) 1 (1) 16 (9)
ANAEMIAa, n (%) 4 (2) 9 (5)
WBC DECREASED, n (%) 2 (1) 8 (5)
FATIGUE, n (%) 4 (2) 7 (4)
XALKORI (n = 172)
CHEMOTHERAPY (n = 171)
aClustered term; bno on-treatment assessments
AE, adverse event; ECG, electrocardiogram; WBC, white blood cell.
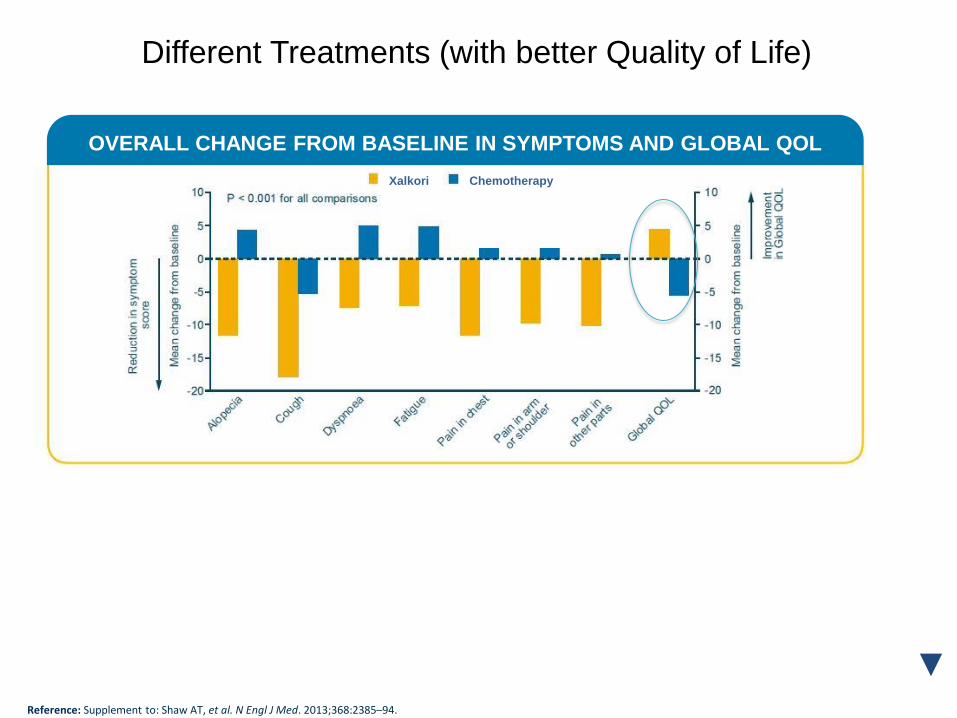
Reference: Supplement to: Shaw AT, et al. N Engl J Med. 2013;368:2385–94.
Reference: Supplement to: Shaw AT, et al. N Engl J Med. 2013;368:2385–94.
OVERALL CHANGE FROM BASELINE IN SYMPTOMS AND GLOBAL QOL
Chemotherapy Xalkori
Different Treatments (with better Quality of Life)
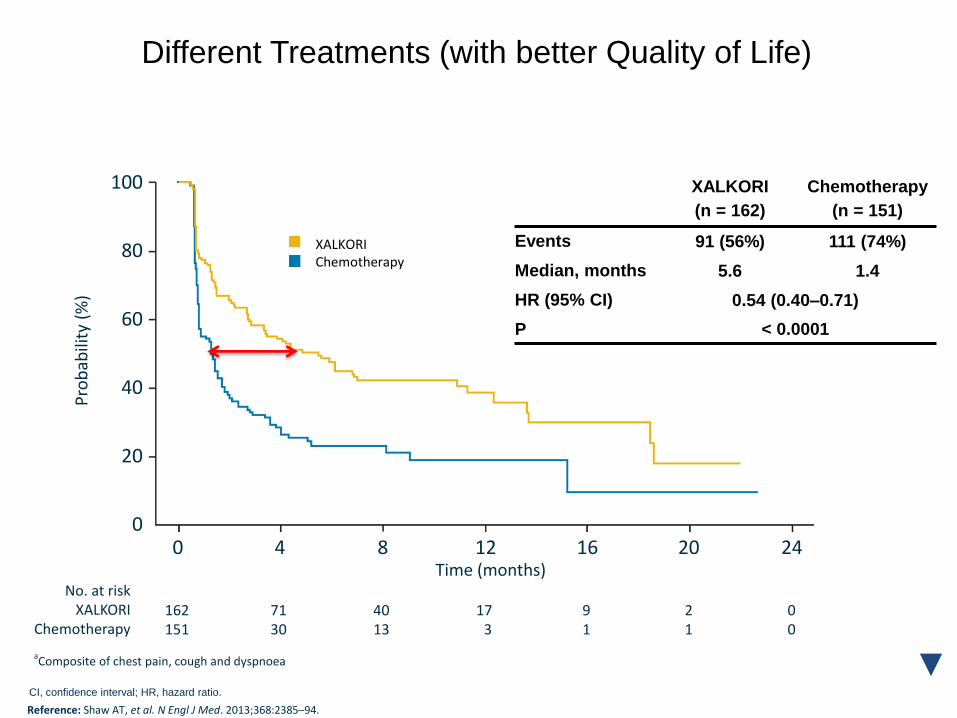
100
80
60
40
20
0 0 4 8 12 16 20 24
Time (months)
162 71 40 17 9 2 0 151 30 13 3 1 1 0
No. at risk XALKORI
Chemotherapy
Pro
bab
ility
(%
)
XALKORI
(n = 162)
Chemotherapy
(n = 151)
Events 91 (56%) 111 (74%)
Median, months 5.6 1.4
HR (95% CI) 0.54 (0.40–0.71)
P < 0.0001
aComposite of chest pain, cough and dyspnoea
CI, confidence interval; HR, hazard ratio.
XALKORI
Chemotherapy
Reference: Shaw AT, et al. N Engl J Med. 2013;368:2385–94.
Different Treatments (with better Quality of Life)
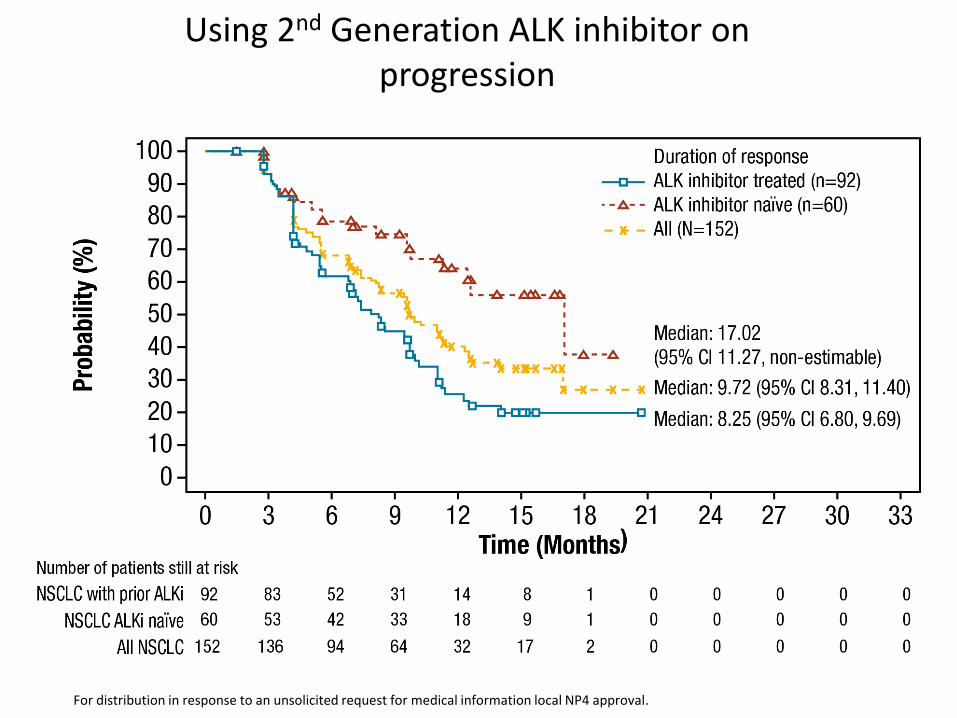
Using 2nd Generation ALK inhibitor on progression
18
For distribution in response to an unsolicited request for medical information local NP4 approval.
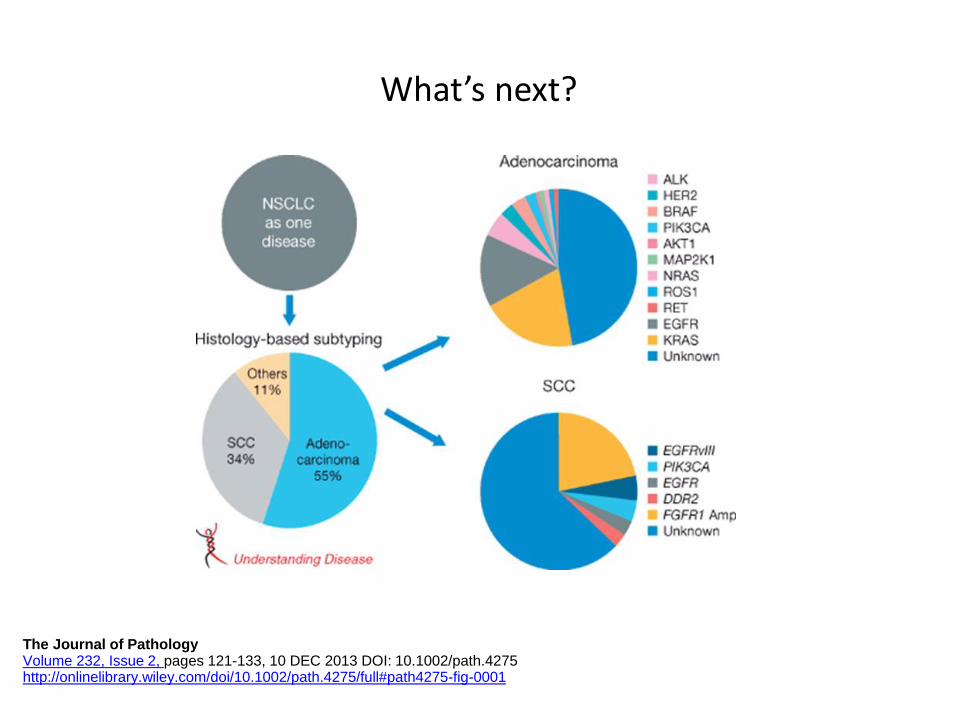
What’s next?
The Journal of Pathology Volume 232, Issue 2, pages 121-133, 10 DEC 2013 DOI: 10.1002/path.4275 http://onlinelibrary.wiley.com/doi/10.1002/path.4275/full#path4275-fig-0001
Emerging data on new populations to treat with targeted therapy
• Ros-1
• Ret
• B-Raf
• C-Met
• (?K-Ras)
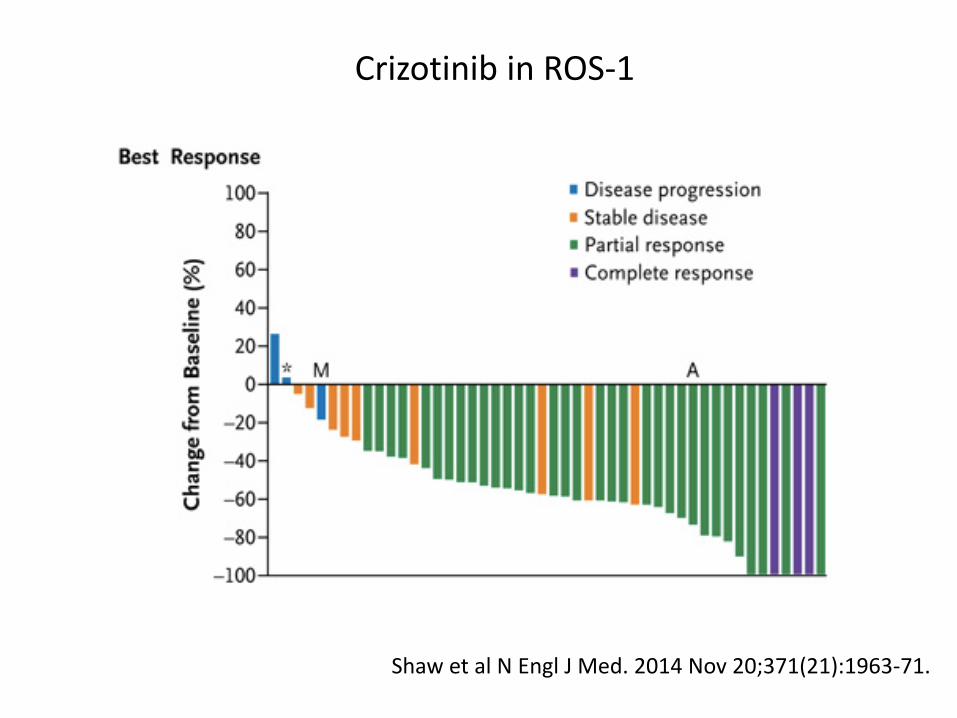
Shaw et al N Engl J Med. 2014 Nov 20;371(21):1963-71.
Crizotinib in ROS-1
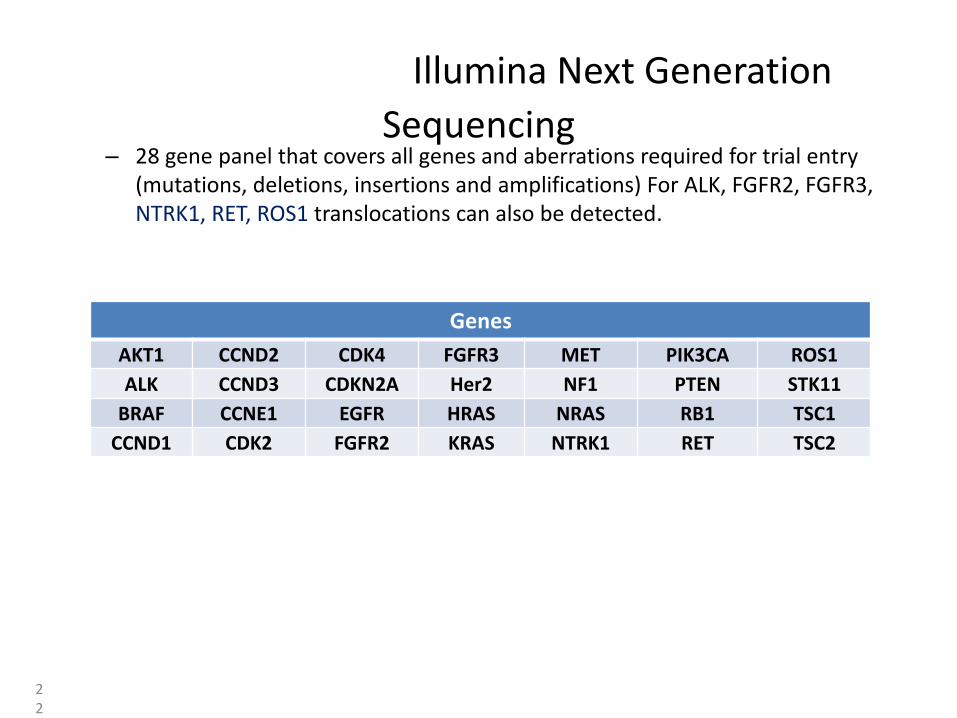
Illumina Next Generation
Sequencing – 28 gene panel that covers all genes and aberrations required for trial entry
(mutations, deletions, insertions and amplifications) For ALK, FGFR2, FGFR3, NTRK1, RET, ROS1 translocations can also be detected.
22
Genes
AKT1 CCND2 CDK4 FGFR3 MET PIK3CA ROS1
ALK CCND3 CDKN2A Her2 NF1 PTEN STK11
BRAF CCNE1 EGFR HRAS NRAS RB1 TSC1
CCND1 CDK2 FGFR2 KRAS NTRK1 RET TSC2
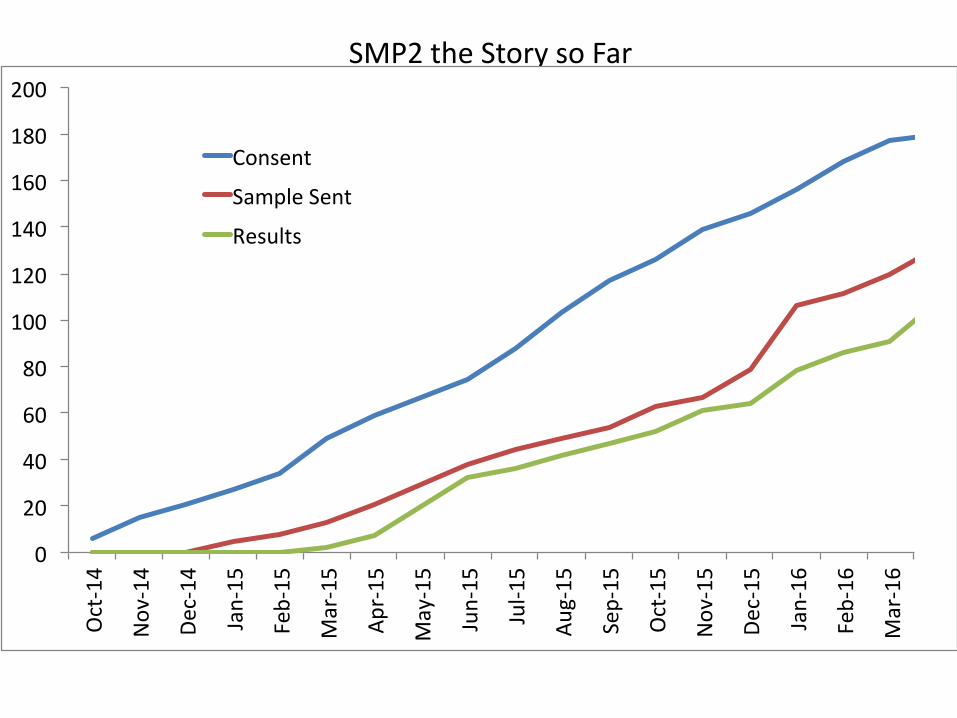
SMP2 the Story so Far
0
20
40
60
80
100
120
140
160
180
200Oct-14
Nov-14
Dec-14
Jan-15
Feb-15
Mar-15
Apr-15
May-15
Jun-15
Jul-15
Aug-15
Sep-15
Oct-15
Nov-15
Dec-15
Jan-16
Feb-16
Mar-16
Consent
SampleSent
Results
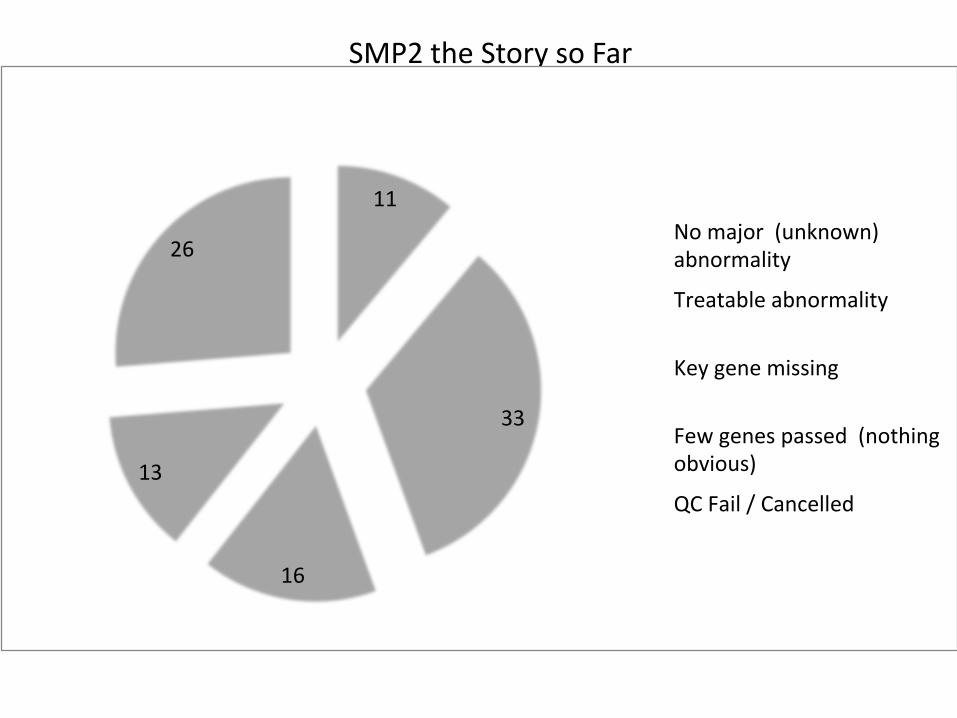
SMP2 the Story so Far
11
33
16
13
26Nomajor(unknown)abnormality
Treatableabnormality
Keygenemissing
Fewgenespassed(nothingobvious)
QCFail/Cancelled
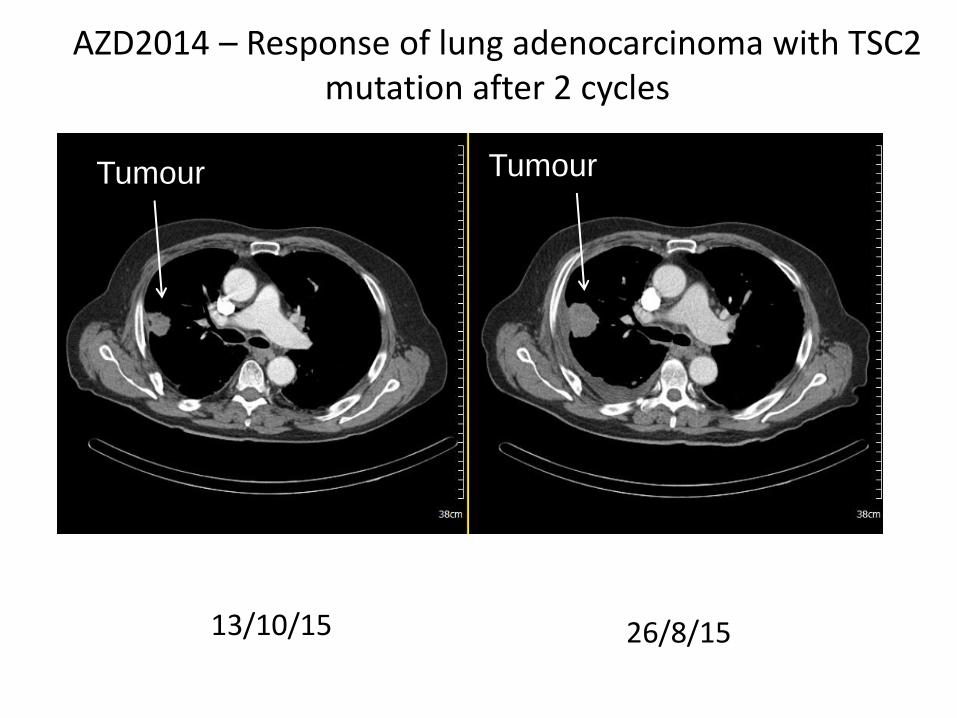
AZD2014 – Response of lung adenocarcinoma with TSC2 mutation after 2 cycles
13/10/15 26/8/15
Tumour Tumour
Summary
• Concept of “lung cancer” outdated
• Molecular targeted therapy can be efficacious and well tolerated when we identify the targets
• Trials of stratified medicine ongoing
• However new treatments for patients with lung cancer urgently needed
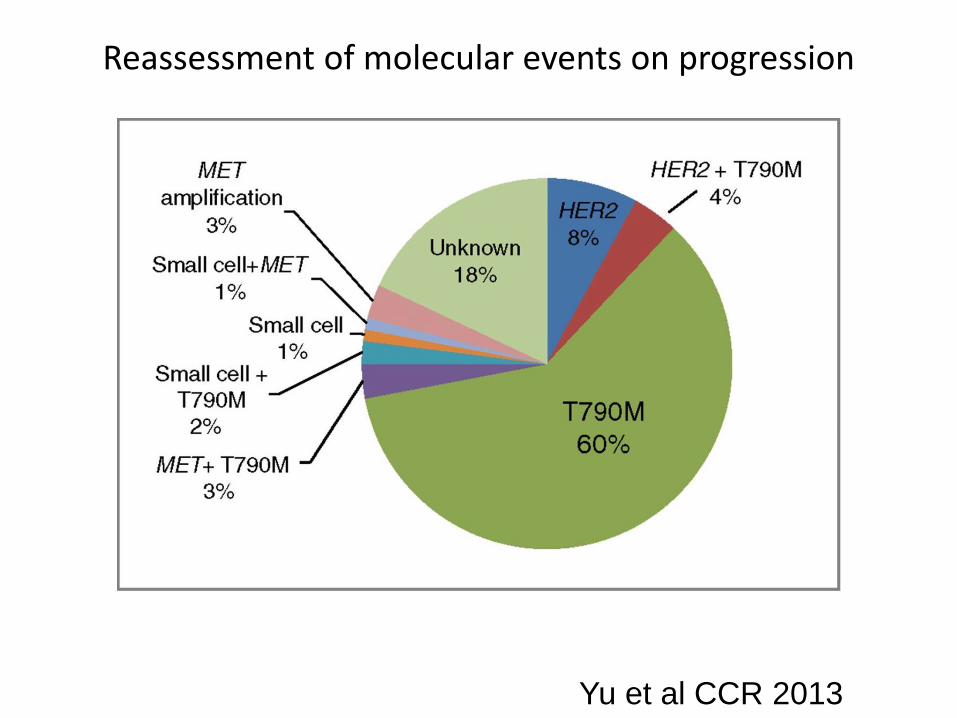
Reassessment of molecular events on progression
Yu et al CCR 2013
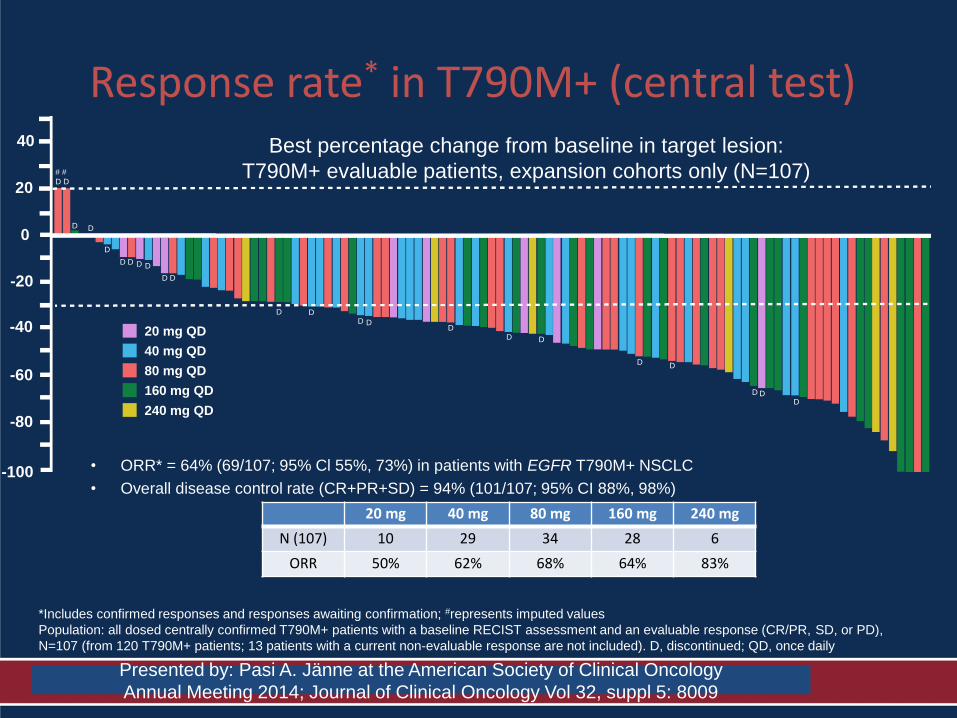
Response rate* in T790M+ (central test)
• ORR* = 64% (69/107; 95% Cl 55%, 73%) in patients with EGFR T790M+ NSCLC
• Overall disease control rate (CR+PR+SD) = 94% (101/107; 95% CI 88%, 98%)
20 mg 40 mg 80 mg 160 mg 240 mg
N (107) 10 29 34 28 6
ORR 50% 62% 68% 64% 83%
Best percentage change from baseline in target lesion: all evaluable T790M+ patients, Part B
*Includes confirmed responses and responses awaiting confirmation; #represents imputed values
Population: all dosed centrally confirmed T790M+ patients with a baseline RECIST assessment and an evaluable response (CR/PR, SD, or PD),
N=107 (from 120 T790M+ patients; 13 patients with a current non-evaluable response are not included). D, discontinued; QD, once daily
Best percentage change from baseline in target lesion:
T790M+ evaluable patients, expansion cohorts only (N=107)
40 mg QD
80 mg QD
160 mg QD
240 mg QD
20 mg QD
40
20
-20
-40
-60
-80
-100 0
# #
D D
D D
D
D D D D
D D
D D D D
D D D
D D
D D D
Presented by: Pasi A. Jänne at the American Society of Clinical Oncology
Annual Meeting 2014; Journal of Clinical Oncology Vol 32, suppl 5: 8009
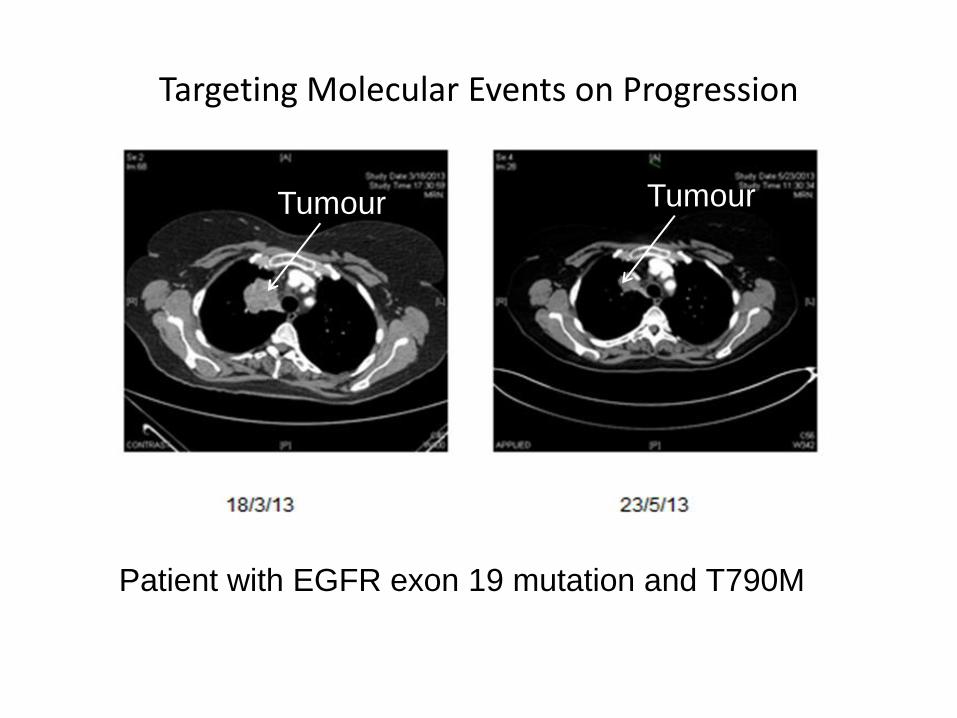
Targeting Molecular Events on Progression
Patient with EGFR exon 19 mutation and T790M
Tumour Tumour
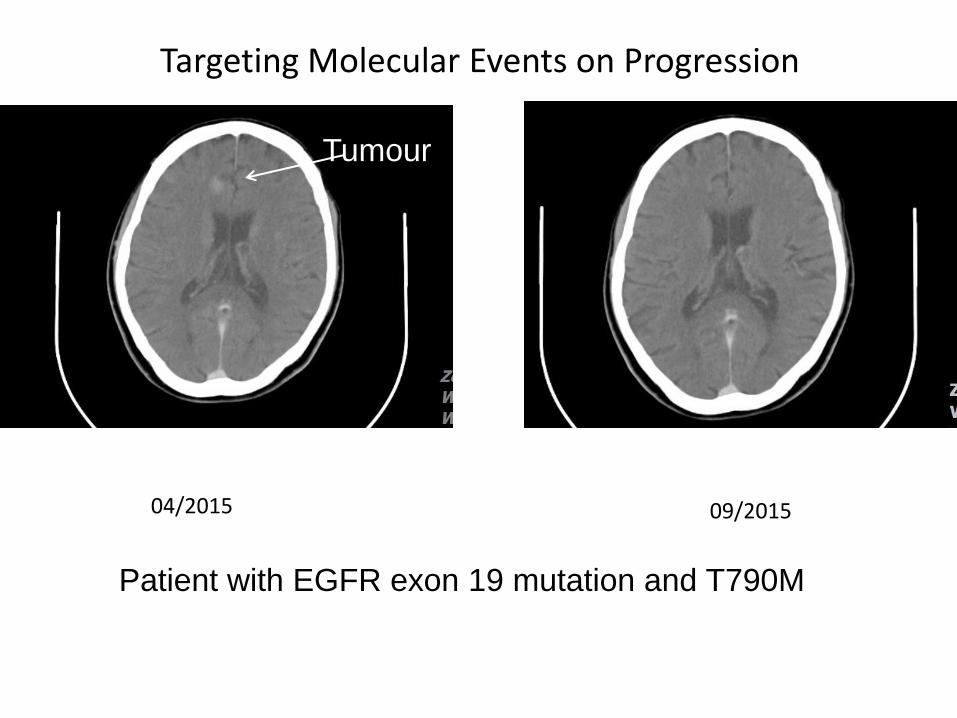
04/2015 09/2015
Tumour
Targeting Molecular Events on Progression
Patient with EGFR exon 19 mutation and T790M
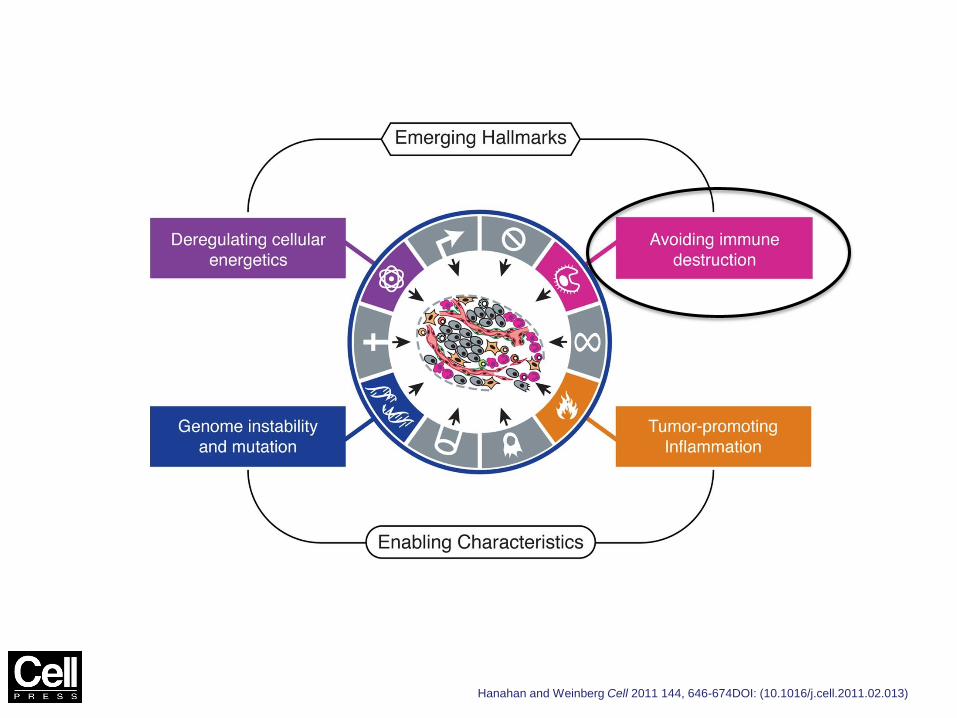
Figure 3
Hanahan and Weinberg Cell 2011 144, 646-674DOI: (10.1016/j.cell.2011.02.013)
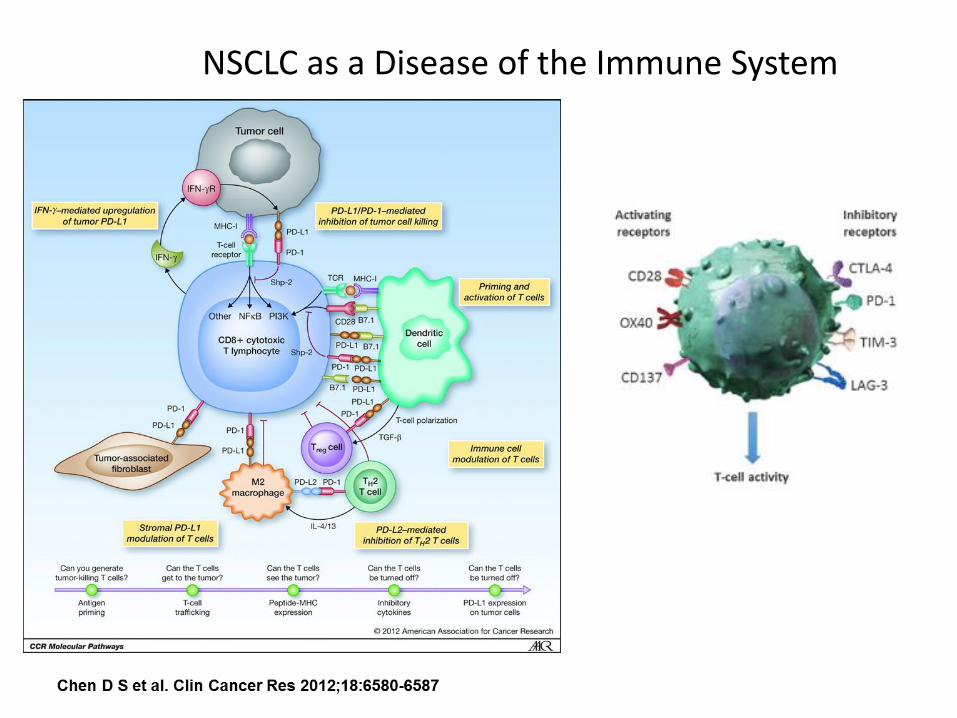
NSCLC as a Disease of the Immune System
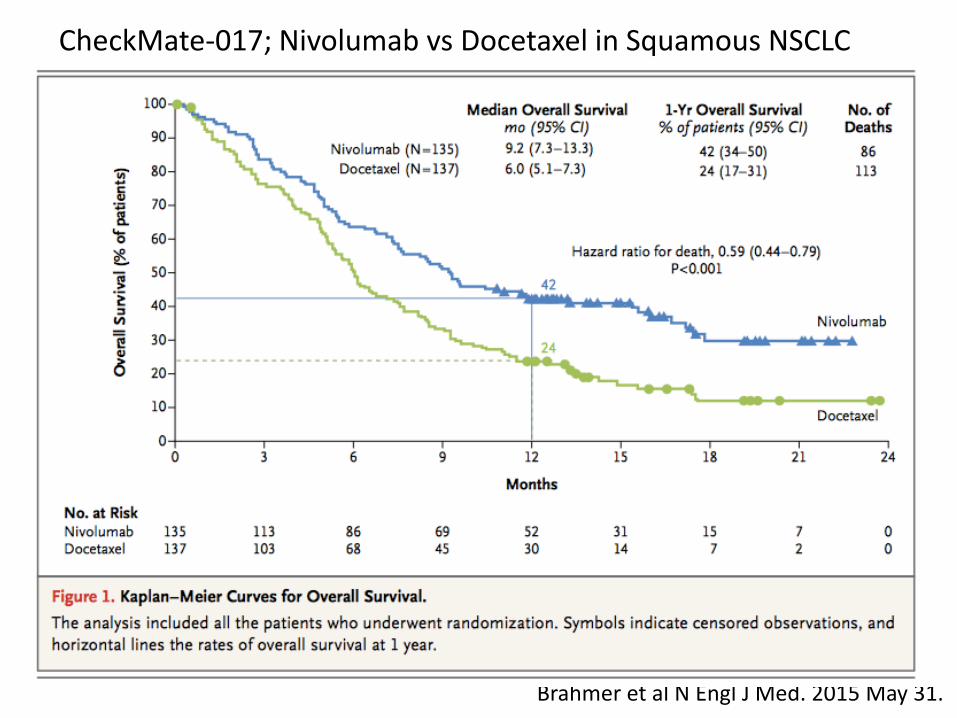
Brahmer et al N Engl J Med. 2015 May 31.
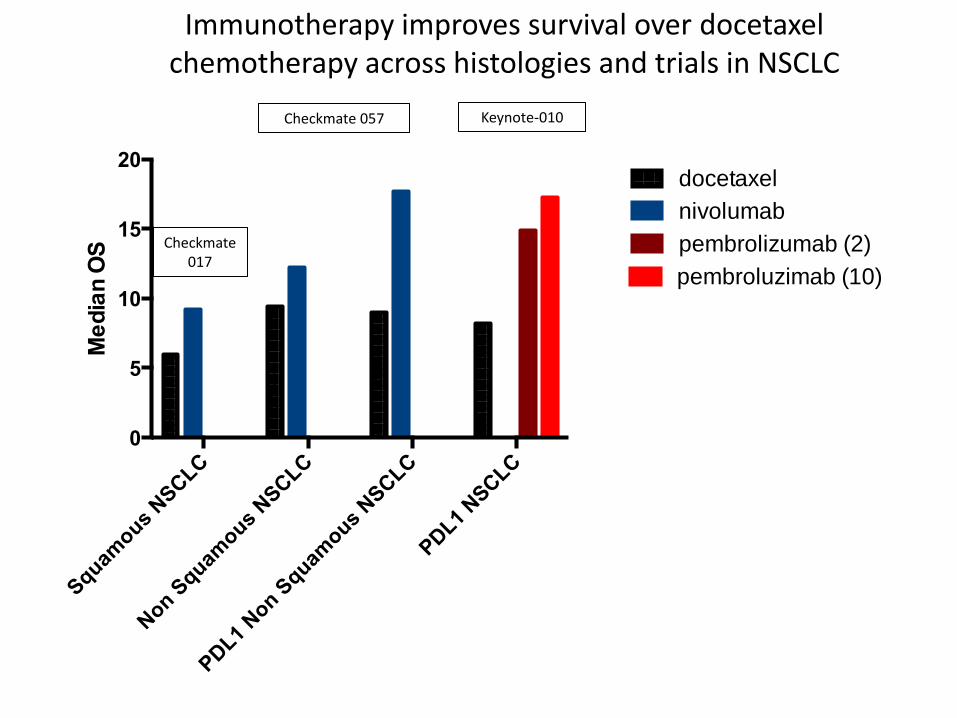
CheckMate-017; Nivolumab vs Docetaxel in Squamous NSCLC
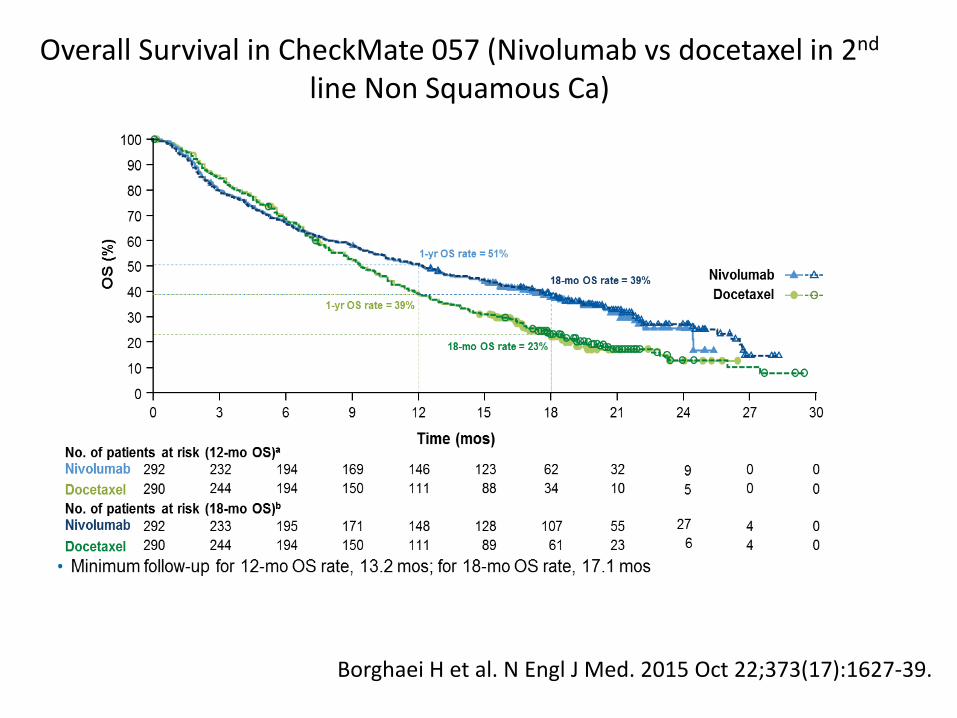
Overall Survival in CheckMate 057 (Nivolumab vs docetaxel in 2nd line Non Squamous Ca)
Borghaei H et al. N Engl J Med. 2015 Oct 22;373(17):1627-39.
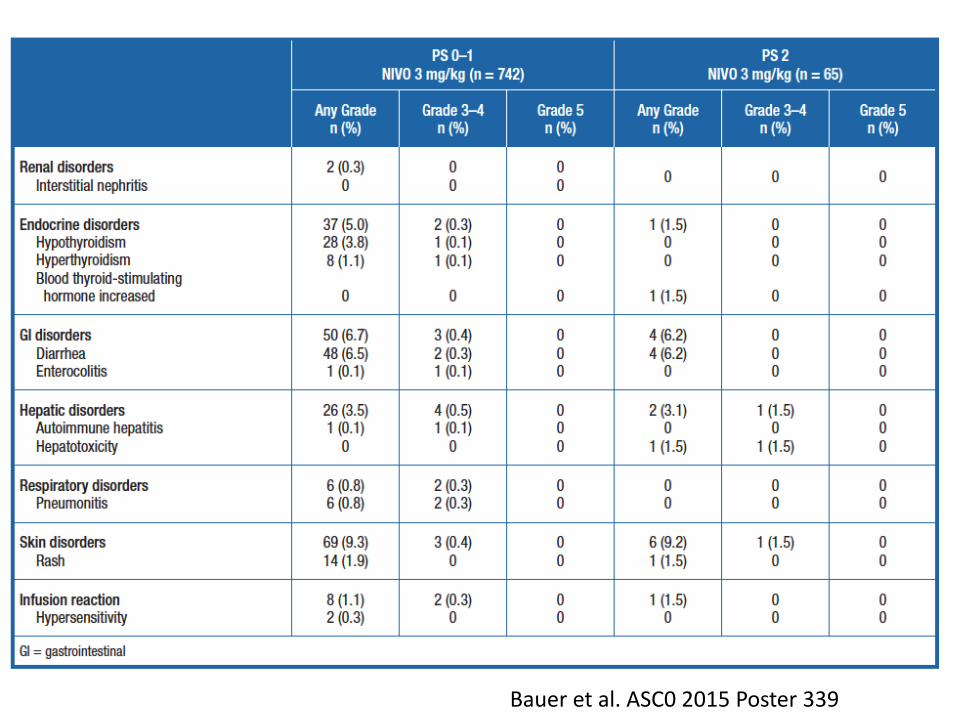
Bauer et al. ASC0 2015 Poster 339
Squam
ous NSCLC
Non S
quamous
NSCLC
PDL1
Non S
quamous
NSCLC
PDL1
NSCLC
0
5
10
15
20
Me
dia
n O
S
docetaxel
nivolumab
pembrolizumab (2)
pembroluzimab (10)
Checkmate 017
Checkmate 057 Keynote-010
Immunotherapy improves survival over docetaxel chemotherapy across histologies and trials in NSCLC
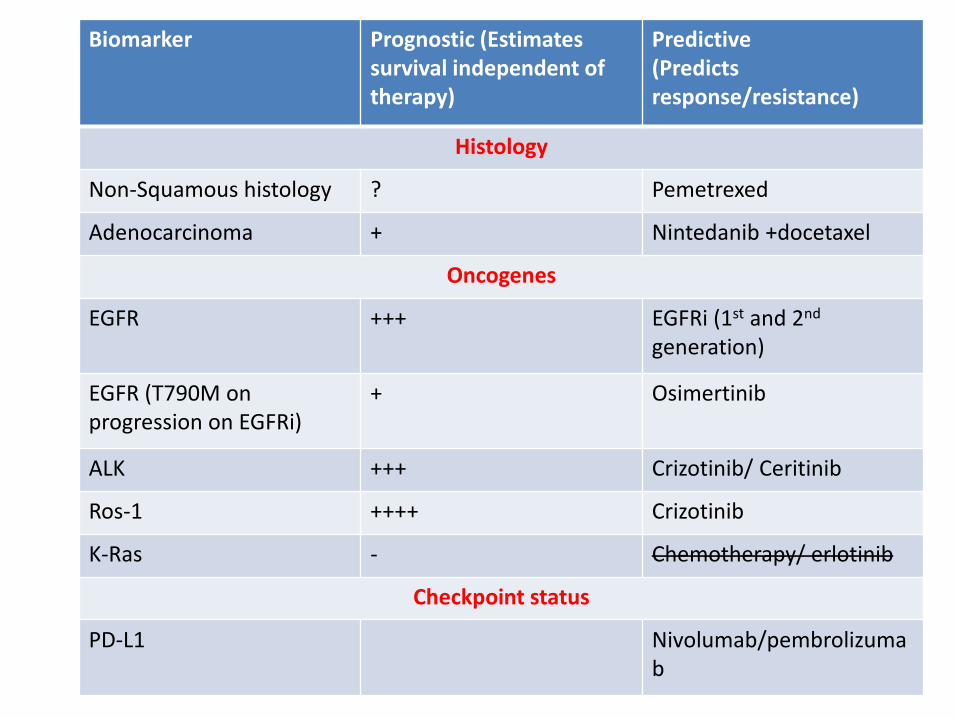
Biomarker Prognostic (Estimates survival independent of therapy)
Predictive (Predicts response/resistance)
Histology
Non-Squamous histology ? Pemetrexed
Adenocarcinoma + Nintedanib +docetaxel
Oncogenes
EGFR +++ EGFRi (1st and 2nd generation)
EGFR (T790M on progression on EGFRi)
+ Osimertinib
ALK +++ Crizotinib/ Ceritinib
Ros-1 ++++ Crizotinib
K-Ras - Chemotherapy/ erlotinib
Checkpoint status
PD-L1 Nivolumab/pembrolizumab
Summary • As an oncologist requiring increasing information
about the tumour to guide care • Implications for
– Biopsy size/ site – Biopsy handling/ analysis – Prioritization of tissue for tests that may impact on
patients care – (rebiopsy)
• Communication is key • Things coming in the near future
– cfDNA – Better biomarkers for immune agents
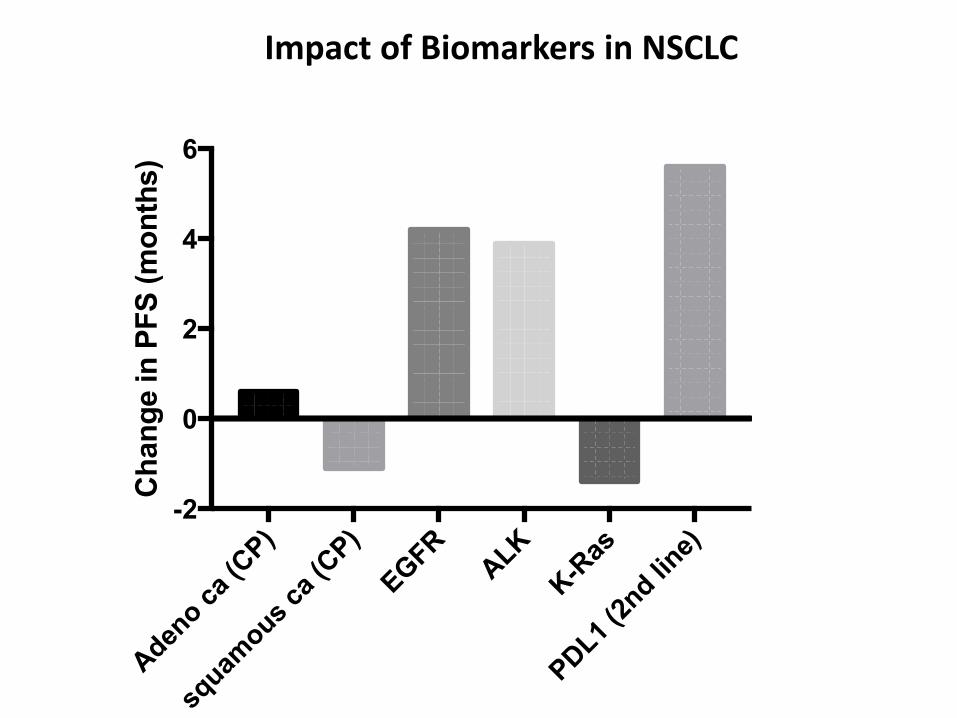
Aden
o ca
(CP)
squam
ous ca
(CP)
EGFR
ALK
K-R
as
PDL1
(2nd li
ne)-2
0
2
4
6C
han
ge in
PF
S (
mo
nth
s)
Impact of Biomarkers in NSCLC