Embed Size (px)
Citation preview

Advances in Dermatology 23 (2007) 289–306
ADVANCES IN DERMATOLOGY
Hidradenitis Suppurativa: An Update
Robert A. Lee, MD, PhDa,*, Andrew Yoon, BSb,Joseph Kist, MDa
aHospital of the University of Pennsylvania, Department of Dermatology, 3600 Spruce St.,2 Maloney, Philadelphia, PA 19104, USAbJefferson Medical College, 1020 Locust Street, Jefferson Alumni Hall, Philadelphia,PA 19107, USA
EDITORIAL COMMENTWhen hidradenitis suppurativa is severe, it may produce disabling pain, repulsiveodor, and scarring that ruins the quality of life. Therapy has, for decades, dependedupon antibiotics and intralesional steroids for mild disease and surgery for severe in-volvement. The advent of immunomodulatory medications and the use of antiandro-gens are expanding our options. Drs. Kist and Lee staff a clinic that is dedicated tothe care of patients who have hidradenitis suppurativa (HS). They share their thera-peutic experience along with the published evidence supporting their recommenda-tions. The algorithm summarizing management is invaluable.
William D. James, MD
Hidradenitis suppurativa (HS), was first described in 1833 by Frenchphysician Alfred Verneuil for its characteristic intertriginous distribu-tion [1,2]. It is a common inflammatory dermatosis characterized by
painful, recurrent abscesses and nodules primarily in intertriginous areas, suchas the axilla, groin, gluteal cleft, and inframammary folds. Chronic inflamma-tion can lead to sinus tract formation, scarring, and malodorous discharge,leading to pain, discomfort, and a decreased quality of life. Current treatmentsare often unsatisfactory. Medical interventions generally provide only tempo-rary, if any, relief of symptoms and are not curative. The success of surgicalapproaches varies greatly, depending on the location and severity of the af-fected areas. Patients presenting with advanced disease in functionally sensitiveareas often develop either recurrent disease with insufficiently wide excisions orsuffer extensive scarring from surgery. This review will summarize the currentliterature for the treatment of HS with emphasis on recent therapeutic advancesin medical therapies.
*Corresponding author. E-mail address: [email protected] (R.A. Lee).
0882-0880/07/$ – see front matterª 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.yadr.2007.07.001
290 LEE, YOON, & KIST
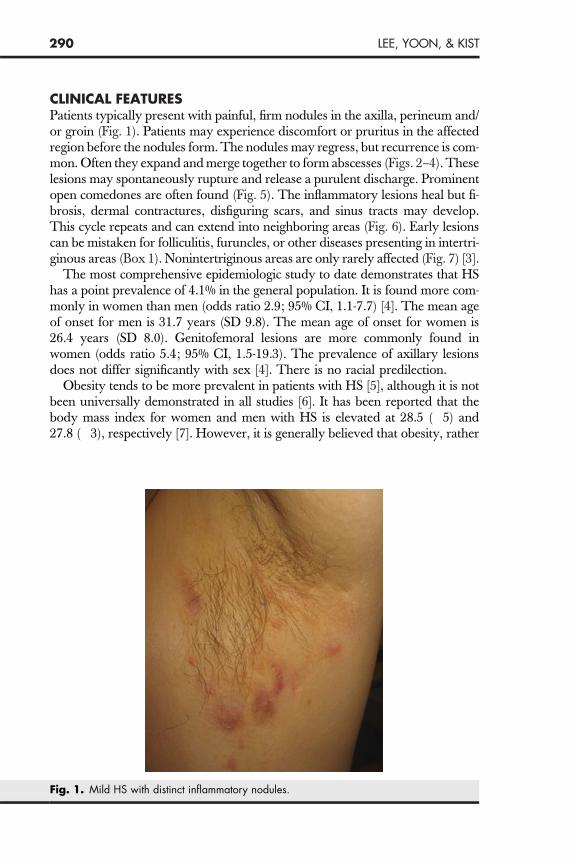
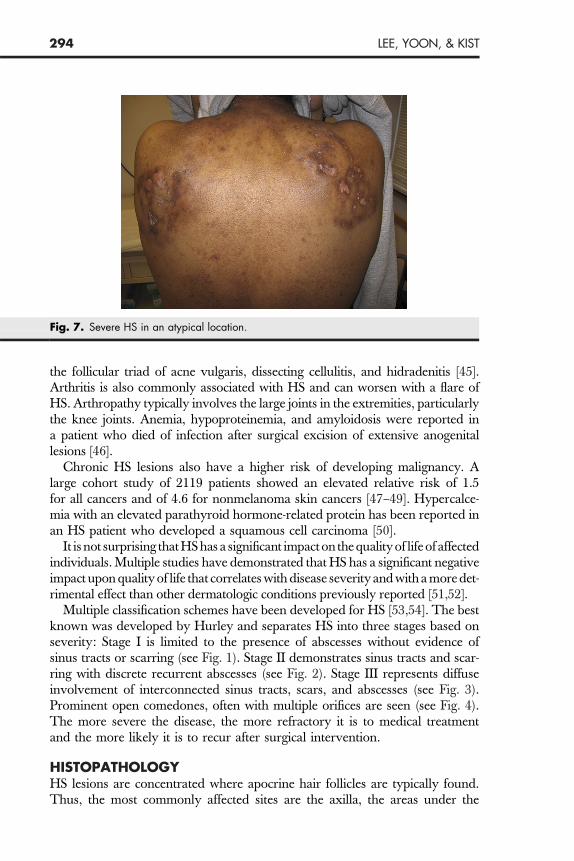
CLINICAL FEATURESPatients typically present with painful, firm nodules in the axilla, perineum and/or groin (Fig. 1). Patients may experience discomfort or pruritus in the affectedregion before the nodules form. The nodules may regress, but recurrence is com-mon. Often they expand and merge together to form abscesses (Figs. 2–4). Theselesions may spontaneously rupture and release a purulent discharge. Prominentopen comedones are often found (Fig. 5). The inflammatory lesions heal but fi-brosis, dermal contractures, disfiguring scars, and sinus tracts may develop.This cycle repeats and can extend into neighboring areas (Fig. 6). Early lesionscan be mistaken for folliculitis, furuncles, or other diseases presenting in intertri-ginous areas (Box 1). Nonintertriginous areas are only rarely affected (Fig. 7) [3].
The most comprehensive epidemiologic study to date demonstrates that HShas a point prevalence of 4.1% in the general population. It is found more com-monly in women than men (odds ratio 2.9; 95% CI, 1.1-7.7) [4]. The mean ageof onset for men is 31.7 years (SD 9.8). The mean age of onset for women is26.4 years (SD 8.0). Genitofemoral lesions are more commonly found inwomen (odds ratio 5.4; 95% CI, 1.5-19.3). The prevalence of axillary lesionsdoes not differ significantly with sex [4]. There is no racial predilection.
Obesity tends to be more prevalent in patients with HS [5], although it is notbeen universally demonstrated in all studies [6]. It has been reported that thebody mass index for women and men with HS is elevated at 28.5 (�5) and27.8 (�3), respectively [7]. However, it is generally believed that obesity, rather
Fig. 1. Mild HS with distinct inflammatory nodules.
291HIDRADENITIS SUPPURATIVA
than being a primary cause, acts as a secondary factor, aggravating diseasethrough mechanical trauma at skin folds.
A high incidence of smoking occurs amongst hidradenitis patients. Of HS pa-tients, 89% are active smokers compared with 46% of controls [8,9]. While HSis not typically thought to be related to medications, it has been reported to beexacerbated by lithium [10,11] and sirolimus [12].
In women, HS occurs almost exclusively after menarche. Premenstrual flaresare common in about 50% of all cases. HS tends to improve with pregnancyand rebounds after parturition. Signs of virilization can been seen in HS but
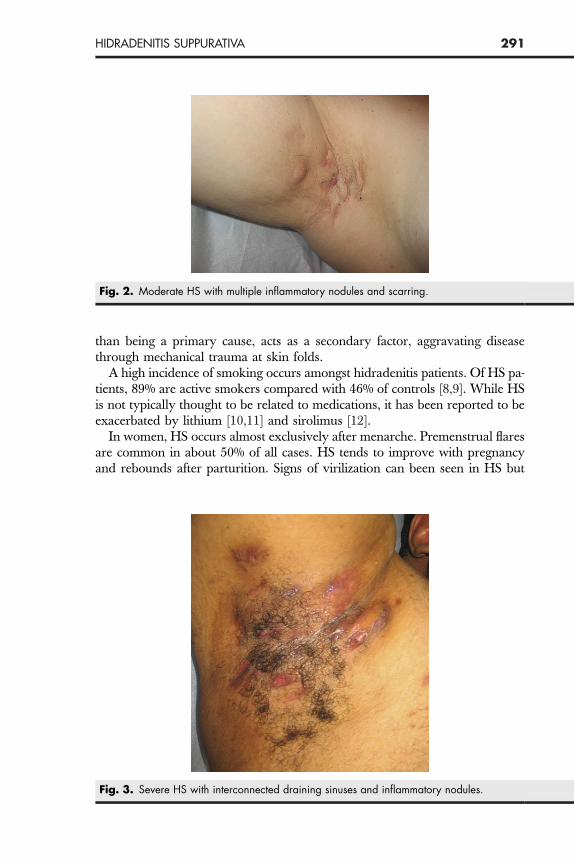
Fig. 2. Moderate HS with multiple inflammatory nodules and scarring.
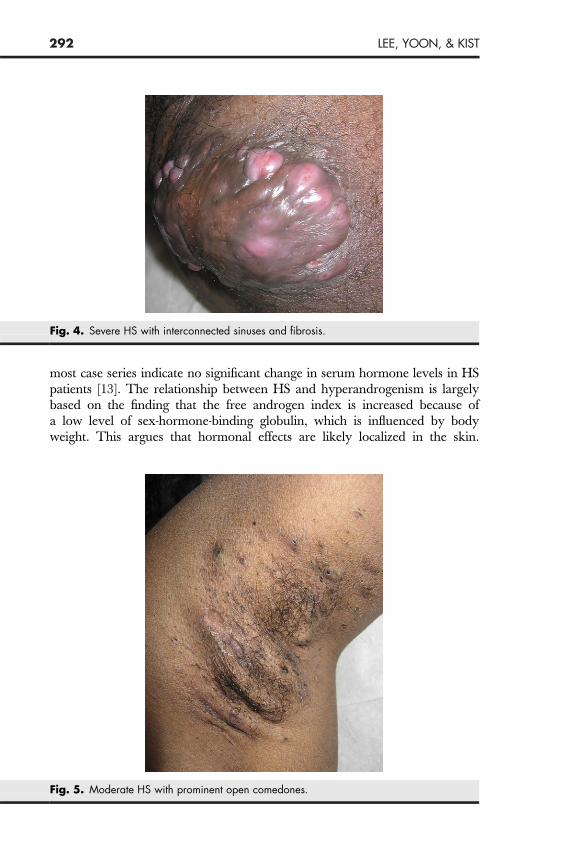
Fig. 3. Severe HS with interconnected draining sinuses and inflammatory nodules.
292 LEE, YOON, & KIST
most case series indicate no significant change in serum hormone levels in HSpatients [13]. The relationship between HS and hyperandrogenism is largelybased on the finding that the free androgen index is increased because ofa low level of sex-hormone-binding globulin, which is influenced by bodyweight. This argues that hormonal effects are likely localized in the skin.
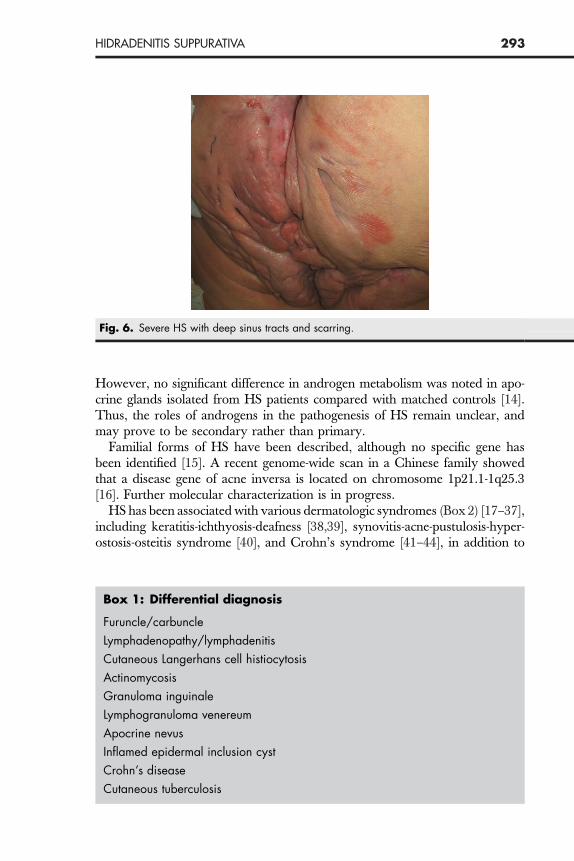
Fig. 4. Severe HS with interconnected sinuses and fibrosis.
Fig. 5. Moderate HS with prominent open comedones.
293HIDRADENITIS SUPPURATIVA
However, no significant difference in androgen metabolism was noted in apo-crine glands isolated from HS patients compared with matched controls [14].Thus, the roles of androgens in the pathogenesis of HS remain unclear, andmay prove to be secondary rather than primary.
Familial forms of HS have been described, although no specific gene hasbeen identified [15]. A recent genome-wide scan in a Chinese family showedthat a disease gene of acne inversa is located on chromosome 1p21.1-1q25.3[16]. Further molecular characterization is in progress.
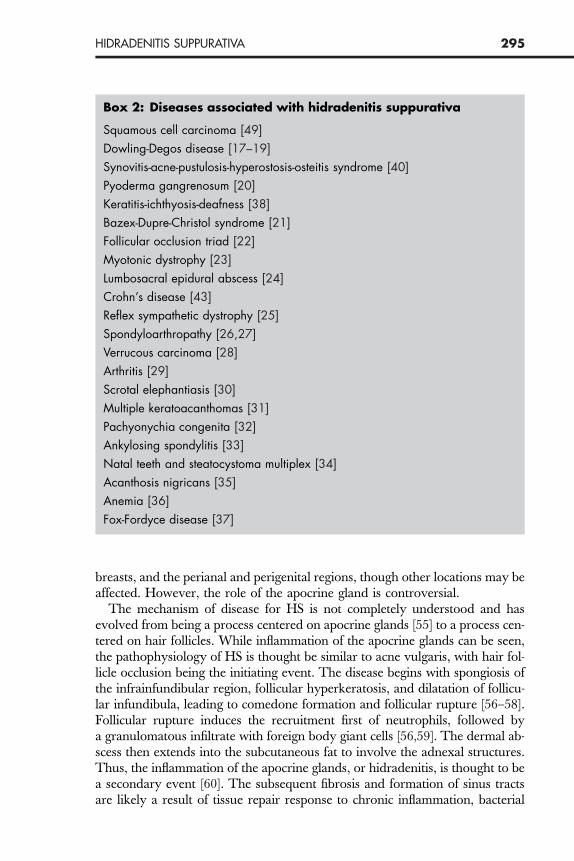
HS has been associated with various dermatologic syndromes (Box 2) [17–37],including keratitis-ichthyosis-deafness [38,39], synovitis-acne-pustulosis-hyper-ostosis-osteitis syndrome [40], and Crohn’s syndrome [41–44], in addition to
Fig. 6. Severe HS with deep sinus tracts and scarring.
Box 1: Differential diagnosis
Furuncle/carbuncle
Lymphadenopathy/lymphadenitis
Cutaneous Langerhans cell histiocytosis
Actinomycosis
Granuloma inguinale
Lymphogranuloma venereum
Apocrine nevus
Inflamed epidermal inclusion cyst
Crohn’s disease
Cutaneous tuberculosis
294 LEE, YOON, & KIST
the follicular triad of acne vulgaris, dissecting cellulitis, and hidradenitis [45].Arthritis is also commonly associated with HS and can worsen with a flare ofHS. Arthropathy typically involves the large joints in the extremities, particularlythe knee joints. Anemia, hypoproteinemia, and amyloidosis were reported ina patient who died of infection after surgical excision of extensive anogenitallesions [46].
Chronic HS lesions also have a higher risk of developing malignancy. Alarge cohort study of 2119 patients showed an elevated relative risk of 1.5for all cancers and of 4.6 for nonmelanoma skin cancers [47–49]. Hypercalce-mia with an elevated parathyroid hormone-related protein has been reported inan HS patient who developed a squamous cell carcinoma [50].
It is not surprising that HS has a significant impact on the quality of life of affectedindividuals. Multiple studies have demonstrated that HS has a significant negativeimpact upon quality of life that correlates with disease severity and with a more det-rimental effect than other dermatologic conditions previously reported [51,52].
Multiple classification schemes have been developed for HS [53,54]. The bestknown was developed by Hurley and separates HS into three stages based onseverity: Stage I is limited to the presence of abscesses without evidence ofsinus tracts or scarring (see Fig. 1). Stage II demonstrates sinus tracts and scar-ring with discrete recurrent abscesses (see Fig. 2). Stage III represents diffuseinvolvement of interconnected sinus tracts, scars, and abscesses (see Fig. 3).Prominent open comedones, often with multiple orifices are seen (see Fig. 4).The more severe the disease, the more refractory it is to medical treatmentand the more likely it is to recur after surgical intervention.
HISTOPATHOLOGYHS lesions are concentrated where apocrine hair follicles are typically found.Thus, the most commonly affected sites are the axilla, the areas under the
Fig. 7. Severe HS in an atypical location.
295HIDRADENITIS SUPPURATIVA
breasts, and the perianal and perigenital regions, though other locations may beaffected. However, the role of the apocrine gland is controversial.
The mechanism of disease for HS is not completely understood and hasevolved from being a process centered on apocrine glands [55] to a process cen-tered on hair follicles. While inflammation of the apocrine glands can be seen,the pathophysiology of HS is thought be similar to acne vulgaris, with hair fol-licle occlusion being the initiating event. The disease begins with spongiosis ofthe infrainfundibular region, follicular hyperkeratosis, and dilatation of follicu-lar infundibula, leading to comedone formation and follicular rupture [56–58].Follicular rupture induces the recruitment first of neutrophils, followed bya granulomatous infiltrate with foreign body giant cells [56,59]. The dermal ab-scess then extends into the subcutaneous fat to involve the adnexal structures.Thus, the inflammation of the apocrine glands, or hidradenitis, is thought to bea secondary event [60]. The subsequent fibrosis and formation of sinus tractsare likely a result of tissue repair response to chronic inflammation, bacterial
Box 2: Diseases associated with hidradenitis suppurativa
Squamous cell carcinoma [49]
Dowling-Degos disease [17–19]
Synovitis-acne-pustulosis-hyperostosis-osteitis syndrome [40]
Pyoderma gangrenosum [20]
Keratitis-ichthyosis-deafness [38]
Bazex-Dupre-Christol syndrome [21]
Follicular occlusion triad [22]
Myotonic dystrophy [23]
Lumbosacral epidural abscess [24]
Crohn’s disease [43]
Reflex sympathetic dystrophy [25]
Spondyloarthropathy [26,27]
Verrucous carcinoma [28]
Arthritis [29]
Scrotal elephantiasis [30]
Multiple keratoacanthomas [31]
Pachyonychia congenita [32]
Ankylosing spondylitis [33]
Natal teeth and steatocystoma multiplex [34]
Acanthosis nigricans [35]
Anemia [36]
Fox-Fordyce disease [37]

296 LEE, YOON, & KIST
superinfection, and necrotic debris [61]. Unlike acne, excessive sebum produc-tion is not observed in HS [62].
MICROBIOLOGYWith multiple species of bacteria isolated from HS lesions, the role of infectionis not clearly understood. While organisms can be isolated from HS lesions,many cultures are routinely negative. Thus, bacterial infection is likely second-ary to chronic sinus tracts and moisture rather than of primary etiologic impor-tance. When present, bacterial cultures are often polymicrobial. Staphylococcusaureus, S epidermidis, Streptococcus milleri, and S hominis have all been describedfrom aspiration of deep lesions about 49% of the time [63]. Cultures takenfrom carbon dioxide laser ablation studies show coagulase-negative staphylo-cocci are the most common aerobic organisms isolated from HS lesions (21of 25 patients). S aureus was second (14 of 25 patients). Peptostreptococcus was themost common anaerobic organism (9/25). Enterococcus, Enterobactericiae, diph-theroids, Bacillus cereus, Proprionibacterium acnes, Lactobacillus, and Bacteroides havealso been described [64].
THERAPYTreatment of HS is challenging and response depends on the clinical severity ofthe disease. While its pathophysiology remains unclear, HS shares many sim-ilar features with acne vulgaris and is approached therapeutically in a similarmanner. Medical treatments can reduce inflammation and associated tender-ness and drainage, but usually do not halt disease progression. Antibioticscan be helpful, particularly if specific organisms can be demonstrated. How-ever, antibiotics require fairly long courses of therapy.
Medical therapy can be divided into topical and systemic. Clindamycin is theonly topical medication that has been extensively studied. A randomized con-trol trial with 27 patients showing improvement of abscesses and pustules, butnot of inflammatory nodules, at 12 weeks with clindamycin 1% solution twicedaily [65].
Systemic medications can be further divided into antibiotics, retinoids, hor-monal modulators, and immunosuppressants. Systemic antibiotics are oftenprescribed for HS. In a randomized control comparing topical clindamycin1% twice a day to tetracycline 500 mg twice daily, patients using tetracyclineshowed significant improvement over baseline for at least 3 months. However,there was no statistical difference in improvement between the two treatmentarms [66]. All patients were on at least 3 months of treatment. Pustules and ab-scesses appeared to improve within the first 3 months but inflammatory nod-ules were more refractory to treatment, requiring longer treatment durationto see any effect. A recent case series of 14 patients receiving oral clindamycin300 mg twice a day and rifampicin 300 mg twice a day for 10 weeks achievedremission in 8 of the 14 patients. Remission was induced in 2 additional pa-tients when minocycline was substituted for clindamycin, and 4 patientswere unable to tolerate the treatment because of diarrhea [67].

297HIDRADENITIS SUPPURATIVA
Results from systemic retinoids, particularly isotretinoin, have proven to bedisappointing in the treatment of HS, unlike the results in treating acne vulga-ris. Despite some promising case reports, a prospective trial with long-term fol-low-up showed that only 23% of HS patients benefit from isotretinoin 0.5 to1 mg/kg. Only 16% of patients showed any durable remission after treatmentwithdrawal [68]. These clinical results may reflect the minor role sebum pro-duction appears to play in HS.
Antiandrogen therapy is also used in acne vulgaris and has been studied inHS. A randomized controlled trial comparing cyproterone acetate and norges-trel using a reverse sequential regimen with a crossover at 6 months. Patientswere followed for 12 months. Seven patients cleared, five improved, four re-mained unchanged, and two worsened. There was no significant difference be-tween the two treatment groups [69]. A case series of four patients treated withcyproterone acetate 100 mg per day showed improvement by 2 months, butsymptoms tended to flare once the dose was lowered to 50 mg per day [70].Finasteride, a 5-alpha reductase inhibitor, has also been reported to improveHS symptoms. A case series of six patients on finasteride 5 mg once a dayshowed improvement by 8 weeks and remissions from 8 to 18 months.Main side effects were generalized pruritus and breast tenderness [71]. Spirono-lactone has been used successfully in the treatment of acne [72,73]. While itsuse in acne is not universally accepted [74], its antiandrogen properties meritfurther investigation for its effectiveness in treating HS.
Immunosuppressive therapy has been used to address the acute inflamma-tory stages of the disease with varying degrees of success. An interesting caseof a renal transplant patient with severe HS and chronic granulomatous diseaseshowed remission of his HS lesions with his posttransplantation immunosup-pression regimen of prednisone 5 mg per day, mycophenolate mofetil1000 mg twice a day, and tacrolimus 1 mg twice a day [75]. Cyclosporine A(3-4 mg/kg) has been reported in multiple case reports to work in about 8 weeks[76]. Relapse of milder disease has been noted when the drug is withdrawn[77]. A single case report of a combination of azathioprine, methlyprednisolone,and isotretinoin was effective in a patient with both Crohn’s disease and HS[78]. In a small case series of three patients, methotrexate was not shown tobe effective in HS [79]. Patients administered dapsone (50-150 mg per day)demonstrated significant improvement of their disease by 4 to 12 weeks butwould relapse when the medicine was stopped. Short courses of systemicand intralesional steroids have been reported but have not been studied system-atically [80].
Tumor necrosis factor a (TNF-a) is a proinflammatory cytokine that can beproduced by multiple cells of the body, including activated T cells, keratino-cytes, and Langerhans cells. TNF-a has numerous effects at the cellular level,and these effects may be relevant to the pathophysiology of HS. Initially, pa-tients with Crohn’s disease with concomitant HS showed improvement of theirHS lesions when treated with the anti-TNF-a agent infliximab [81]. Furtherreports of other agents followed.
298 LEE, YOON, & KIST
Infliximab is a human-mouse monoclonal chimeric antibody against theTNF-a molecules. Multiple case series with a follow-up period of up to6 months showed significant improvement [81–86]. More recently, a patientwas reported to have a sustained, excellent response (including an 80% im-provement in his quality-of-life score) to infliximab 5 mg/kg every 8 weeks incombination with methotrexate 7.5 mg/wk for 104 weeks [87]. Less impressiveefficacy was observed in seven patients with severe HS who were treated withmultiple infusions of infliximab 5 mg/kg. While five of the seven patients dem-onstrated improvement at week 6, only two patients were substantially im-proved by week 10. Moreover, significant adverse events were noted,including the development of colon cancer, a multifocal motor neuropathy,and a severe allergic reaction [88]. Thus, enthusiasm generated through successin observational reports and small studies must be tempered with a cautiousrespect for the recalcitrance of HS and for the potential of medication-associ-ated adverse events.
Etanercept is a recombinant soluble fusion protein consisting of two identicalchains of the TNF-a receptor fused with the Fc portion of human IgG1. Etaner-cept functions as a competitive inhibitor for binding of TNF-a at its receptor. Ina case series, six female patients treated with etanercept with 17 to 40 weeks offollow up showed significant improvement. Most patients did have at least oneflare [89]. Adalimumab is a humanized monoclonal antibody against the TNF-amolecules. Both etanercept and adalimumab bind to soluble and membrane-bound TNF leading to cell lysis. Two case reports on adalimumab for thetreatment of hidradenitis showed it was effective in one patient who became re-fractory to infliximab [90,91]. While no long-term safety data is available forTNF-a inhibitors, a meta-analysis of rheumatoid arthritis patients using inflix-imab and adalimumab suggests an increase in serious infections and malignan-cies [92].
Nonsurgical local modalities have been reported, none of which have provedsatisfactory. Cryotherapy has been tried but involves significant comorbidity.A case series of 10 patients reports improvement in 8 patients. However, therewas a significant rate of complications, with 6 patients developing infectionsand 5 developing ulcers [93].
Carbon dioxide laser [94] appeared to be promising alternative to surgery. Acase series of 34 patients who were treated with a scanner-assisted carbon diox-ide laser and who had an average follow-up of 34 months showed a low recur-rence rate at treated sites (4 of 34 patients). However, this treatment did notprevent further disease flares [95].
Photodynamic therapy with topical aminolevulinic acid has been attempted.One case series reported no effect of photodynamic therapy using 20% topicalaminolevulinic acid and either a 633-nm diode laser or a broad-spectrum redlight source. Four patients enrolled with only two patients completing thestudy. One demonstrated modest improvement but the other patient worsened[96]. Another case series reports four patients with a response to topical amino-levulinic acid using a blue light source [94].

299HIDRADENITIS SUPPURATIVA
There is a single patient with concomitant hyperhidrosis who benefited frominjection of botulinum toxin for axillary HS [97].
Radiotherapy with x-rays has been reported to be useful in control of the dis-ease [98]. Destruction of the hair follicles is thought to play a role in sustainedremissions. No randomized controlled studies have been performed with thistechnique.
Surgical excision is the treatment of choice for early disease. Surgical tech-niques for excision and repair vary, depending on extent of disease, locationof lesions, existing comorbidities, and chronicity of disease [99]. Hair follicleand apocrine gland areas should be excised to fascia to ensure adequateremoval of appendageal structures [100]. While a detailed discussion of surgicaltechniques employed is beyond the scope of this review, there are certain recur-ring themes impacting recurrence rates [2]: location of lesions, extent of exci-sion, method of closure, and age of patient. The extent of excision isprobably the most important modifiable factor. Exteriorization of lesions isthought to be important for proper reepitheilization and closure. Incisionaltechniques uniformly lead to disease recurrence (Fig. 8) and should be avoided.Thus, wide local excision correlates with decreased recurrence [101]. Healingby secondary intention is thought to offer the lowest rate of recurrence, butis associated with a prolonged postoperative recovery [102]. Closures with flapsand grafts have a significantly lower recurrence rate than do primary closures[103]. Later age of onset appears to have a favorable prognosis in recurrencerates [104]. Other factors to consider include operative risk, likelihood of infec-tion, postoperative recovery time, scarring and associated wound contracture,skin irritation, and cutaneous sensory changes.
Fig. 8. Moderate HS with linear scars after multiple incision and drainage procedures.
300 LEE, YOON, & KIST
SUMMARYHS is a chronic, debilitating inflammatory dermatosis that is often refractory totreatment. Many medical therapies have been tried and some show efficacy.The introduction of new immunosuppressive medications has revolutionizedthe treatment of psoriasis in dermatology. These therapies have the potentialto powerfully abort the molecular signals driving inflammation in HS and per-haps even induce a remission. This may offer patients an alternative to radicalexcisional surgery. However, more studies are needed to evaluate the long-term effects of these medications, particularly in light of their associationwith an increased risk of malignancy and infection.
Evaluation of treatment efficacy has been hindered by a lack of uniform stan-dards to track treatment response. The classic clinical classification system has
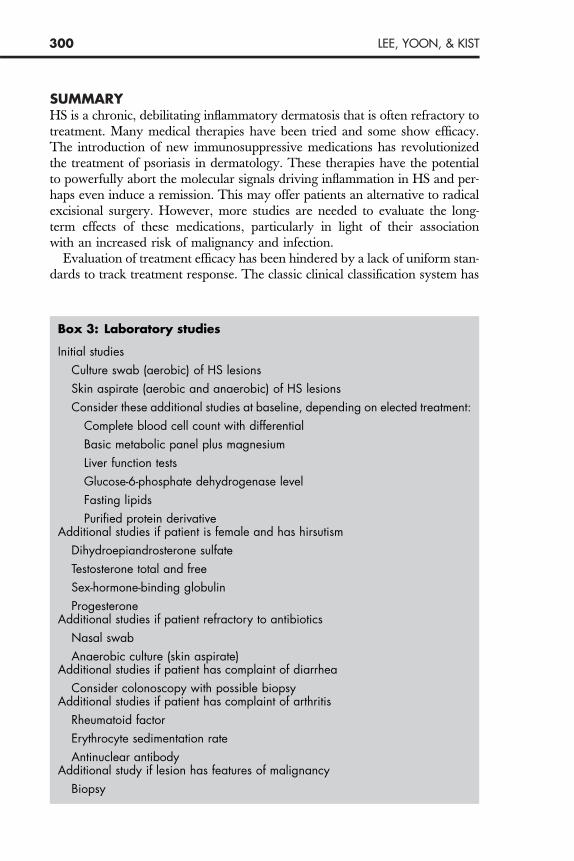
Box 3: Laboratory studies
Initial studies
Culture swab (aerobic) of HS lesions
Skin aspirate (aerobic and anaerobic) of HS lesions
Consider these additional studies at baseline, depending on elected treatment:
Complete blood cell count with differential
Basic metabolic panel plus magnesium
Liver function tests
Glucose-6-phosphate dehydrogenase level
Fasting lipids
Purified protein derivativeAdditional studies if patient is female and has hirsutism
Dihydroepiandrosterone sulfate
Testosterone total and free
Sex-hormone-binding globulin
ProgesteroneAdditional studies if patient refractory to antibiotics
Nasal swab
Anaerobic culture (skin aspirate)Additional studies if patient has complaint of diarrhea
Consider colonoscopy with possible biopsyAdditional studies if patient has complaint of arthritis
Rheumatoid factor
Erythrocyte sedimentation rate
Antinuclear antibodyAdditional study if lesion has features of malignancy
Biopsy
301HIDRADENITIS SUPPURATIVA
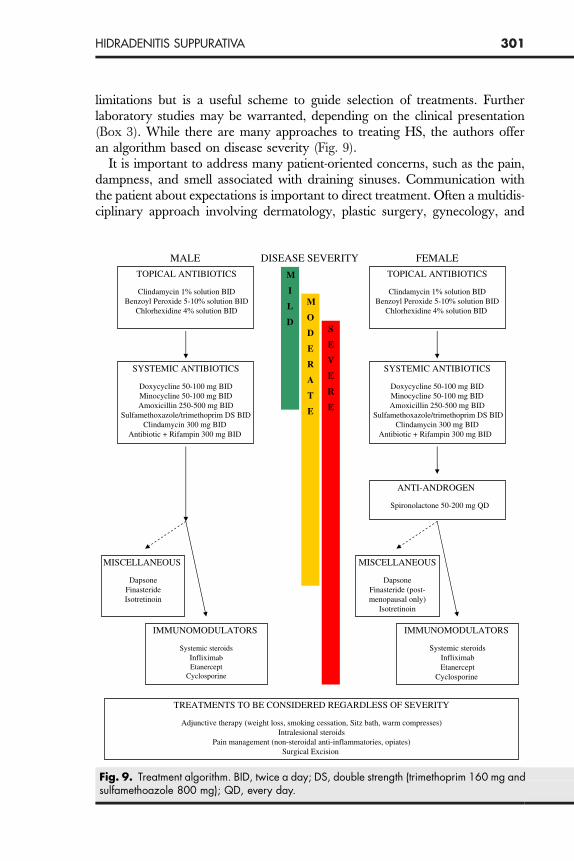
limitations but is a useful scheme to guide selection of treatments. Furtherlaboratory studies may be warranted, depending on the clinical presentation(Box 3). While there are many approaches to treating HS, the authors offeran algorithm based on disease severity (Fig. 9).
It is important to address many patient-oriented concerns, such as the pain,dampness, and smell associated with draining sinuses. Communication withthe patient about expectations is important to direct treatment. Often a multidis-ciplinary approach involving dermatology, plastic surgery, gynecology, and
MALE DISEASE SEVERITY FEMALE
TOPICAL ANTIBIOTICS M
I
L
D
M
O
D
E
R
A
T
E
SYSTEMIC ANTIBIOTICS
Doxycycline 50-100 mg BIDMinocycline 50-100 mg BIDAmoxicillin 250-500 mg BID
Sulfamethoxazole/trimethoprim DS BIDClindamycin 300 mg BID
Antibiotic + Rifampin 300 mg BID
IMMUNOMODULATORS
Systemic steroidsInfliximabEtanercept
Cyclosporine
MISCELLANEOUS
DapsoneFinasterideIsotretinoin
S
E
V
E
R
E
TOPICAL ANTIBIOTICS
SYSTEMIC ANTIBIOTICS
Doxycycline 50-100 mg BIDMinocycline 50-100 mg BIDAmoxicillin 250-500 mg BID
Sulfamethoxazole/trimethoprim DS BIDClindamycin 300 mg BID
Antibiotic + Rifampin 300 mg BID
IMMUNOMODULATORS
Systemic steroidsInfliximabEtanercept
Cyclosporine
MISCELLANEOUS
DapsoneFinasteride (post-menopausal only)
Isotretinoin
ANTI-ANDROGEN
Spironolactone 50-200 mg QD
TREATMENTS TO BE CONSIDERED REGARDLESS OF SEVERITY
Adjunctive therapy (weight loss, smoking cessation, Sitz bath, warm compresses)Intralesional steroids
Pain management (non-steroidal anti-inflammatories, opiates)Surgical Excision
Fig. 9. Treatment algorithm. BID, twice a day; DS, double strength (trimethoprim 160 mg andsulfamethoazole 800 mg); QD, every day.
302 LEE, YOON, & KIST
urology may be necessary to diagnose and treat the disease. Both medical andsurgical options should be explored before embarking on therapy.
AcknowledgmentsThe authors would like to thank the Hidradenitis Suppurativa Foundation,Inc., for the use of its public research database to facilitate the writing of thisarticle.
References[1] Verneuil A. NonEnl’Hidrosadenite Phlegmoneuse Et Des Abces Sudoripares. Arch Gen
Med. 1864;24:537–57.[2] Jemec GB. Hidradenitis suppurativa. J Cutan Med Surg 2003;7:47–56.[3] Greer KE. Letter: facial involvement with hidradenitis suppurativa. Arch Dermatol
1974;109:408.[4] Jemec GB, Heidenheim M, Nielsen NH. The prevalence of hidradenitis suppurativa and its
potential precursor lesions. J Am Acad Dermatol 1996;35:191–4.[5] Edlich RF, Silloway KA, Rodeheaver GT, et al. Epidemiology, pathology, and treatment of
axillary hidradenitis suppurativa. J Emerg Med 1986;4:369–78.[6] Jemec GB, Heidenheim M, Nielsen NH. Hidradenitis suppurativa—characteristics and
consequences. Clin Exp Dermatol 1996;21:419–23.[7] Harrison BJ, Read GF, Hughes LE. Endocrine basis for the clinical presentation of hidrade-
nitis suppurativa. Br J Surg 1988;75:972–5.[8] Konig A, Lehmann C, Rompel R, et al. Cigarette smoking as a triggering factor of hidrade-
nitis suppurativa. Dermatology 1999;198:261–4.[9] Freiman A, Bird G, Metelitsa AI, et al. Cutaneous effects of smoking. J Cutan Med Surg
2004;8:415–23.[10] Marinella MA. Lithium therapy associated with hidradenitis suppurativa. Acta Derm Vene-
reol 1997;77:483.[11] Gupta AK, Knowles SR, Gupta MA, et al. Lithium therapy associated with hidradenitis sup-
purativa: case report and a review of the dermatologic side effects of lithium. J Am AcadDermatol 1995;32:382–6.
[12] Mahe E, Morelson E, Lechaton S, et al. Cutaneous adverse events in renal transplant recip-ients receiving sirolimus-based therapy. Transplantation 2005;79:476–82.
[13] Harrison BJ, Kumar S, Read GF, et al. Hidradenitis suppurativa: evidence for an endocrineabnormality. Br J Surg 1985;72:1002–4.
[14] Barth JH, Kealey T. Androgen metabolism by isolated human axillary apocrine glands inhidradenitis suppurativa. Br J Dermatol 1991;125:304–8.
[15] Von Der Werth JM, Williams HC, Raeburn JA. The clinical genetics of hidradenitis suppu-rativa revisited. Br J Dermatol 2000;142:947–53.
[16] Gao M, Wang PG, Cui Y, et al. Inversa acne (hidradenitis suppurativa): a case report andidentification of the locus at chromosome 1p21.1-1q25.3. J Invest Dermatol 2006;126:1302–6.
[17] Dixit R, George R, Jacob M, et al. Dowling-Degos disease, hidradenitis suppurativa andarthritis in mother and daughter. Clin Exp Dermatol 2006;31:454–6.
[18] Bedlow AJ, Mortimer PS. Dowling-Degos disease associated with hidradenitis suppurativa.Clin Exp Dermatol 1996;21:305–6.
[19] Loo WJ, Rytina E, Todd PM. Hidradenitis suppurativa, Dowling-Degos and multiple epider-mal cysts: a new follicular occlusion triad. Clin Exp Dermatol 2004;29:622–4.
[20] Ah-Weng A, Langtry JA, Velangi S, et al. Pyoderma gangrenosum associated with hidra-denitis suppurativa. Clin Exp Dermatol 2005;30:669–71.
[21] Yung A, Newton-Bishop JA. A case of Bazex-Dupre-Christol syndrome associated with mul-tiple genital trichoepitheliomas. Br J Dermatol 2005;153:682–4.
303HIDRADENITIS SUPPURATIVA
[22] Chicarilli ZN. Follicular occlusion triad: hidradenitis suppurativa, acne conglobata, anddissecting cellulitis of the scalp. Ann Plast Surg 1987;18:230–7.
[23] Cooper SM, Dawber RP, Hilton-Jones D. Three cases of androgen-dependent disease asso-ciated with myotonic dystrophy. J Eur Acad Dermatol Venereol 2003;17:56–8.
[24] Russ E, Castillo M. Lumbosacral epidural abscess due to hidradenitis suppurativa. AJR AmJ Roentgenol 2002;178:770–1.
[25] Moroz A, Lee MH, Clark J. Reflex sympathetic dystrophy with hidradenitis suppurativa ex-acerbation: a case report. Arch Phys Med Rehabil 2001;82:412–4.
[26] Leybishkis B, Fasseas P, Ryan KF, et al. Hidradenitis suppurativa and acne conglobata as-sociated with spondyloarthropathy. Am J Med Sci 2001;321:195–7.
[27] Hellmann DB. Spondyloarthropathy with hidradenitis suppurativa. JAMA 1992;267:2363–5.
[28] Cosman BC, O’Grady TC, Pekarske S. Verrucous carcinoma arising in hidradenitis suppu-rativa. Int J Colorectal Dis 2000;15:342–6.
[29] Hamoir XL, Francois RJ, Van den Haute V, et al. Arthritis and hidradenitis suppurativa diag-nosed in a 48-year-old man. Skeletal Radiol 1999;28:453–6.
[30] Konety BR, Cooper T, Flood HD, et al. Scrotal elephantiasis associated with hidradenitissuppurativa. Plast Reconstr Surg 1996;97:1243–5.
[31] Fenske NA, Groover CE, Lober CW, et al. Dowling-Degos disease, hidradenitis suppura-tiva, and multiple keratoacanthomas. A disorder that may be caused by a single underlyingdefect in pilosebaceous epithelial proliferation. J Am Acad Dermatol 1991;24:888–92.
[32] Todd P, Garioch J, Rademaker M, et al. Pachyonychia congenita complicated by hidrade-nitis suppurativa: a family study. Br J Dermatol 1990;123:663–6.
[33] Grassi W, Offidani AM, Blasetti P, et al. HLA-B27 negative ankylosing spondylitis and hi-dradenitis suppurativa: report of a case. Clin Rheumatol 1988;7:278–83.
[34] McDonald RM, Reed WB. Natal teeth and steatocystoma multiplex complicated by hidra-denitis suppurativa. A new syndrome. Arch Dermatol 1976;112:1132–4.
[35] Stone OJ. Hidradenitis suppurativa following acanthosis nigricans. Report of two cases.Arch Dermatol 1976;112:1142.
[36] Tennant F Jr, Bergeron JR, Stone OJ, et al. Anemia associated with hidradenitis suppurativa.Arch Dermatol 1968;98:138–40.
[37] Spiller RF, Knox JM. Fox-Fordyce disease with hidradenitis suppurativa. J Invest Dermatol1958;31:127–35.
[38] Maintz L, Betz RC, Allam JP, et al. Keratitis-ichthyosis-deafness syndrome in associationwith follicular occlusion triad. Eur J Dermatol 2005;15:347–52.
[39] Montgomery JR, White TW, Martin BL, et al. A novel connexin 26 gene mutation associ-ated with features of the keratitis-ichthyosis-deafness syndrome and the follicular occlusiontriad. J Am Acad Dermatol 2004;51:377–82.
[40] Ozyemisci-Taskiran O, Bolukbasi N, Gogus F. A hidradenitis suppurativa related SAPHOcase associated with features resembling spondylarthropathy and proteinuria. Clin Rheu-matol 2006;5(5):789–91.
[41] Attanoos RL, Appleton MA, Hughes LE, et al. Granulomatous hidradenitis suppurativa andcutaneous Crohn’s disease. Histopathology 1993;23:111–5.
[42] Gower-Rousseau C, Maunoury V, Colombel JF, et al. Hidradenitis suppurativa and Crohn’sdisease in two families: a significant association? Am J Gastroenterol 1992;87:928.
[43] Burrows NP, Jones RR. Crohn’s disease in association with hidradenitis suppurativa. Br JDermatol 1992;126:523.
[44] Ostlere LS, Langtry JA, Mortimer PS, et al. Hidradenitis suppurativa in Crohn’s disease. Br JDermatol 1991;125:384–6.
[45] Wortsman XC, Holm EA, Wulf HC, et al. Real-time spatial compound ultrasound imagingof skin. Skin Res Technol 2004;10:23–31.
[46] Moschella SL. Hidradenitis suppurativa. Complications resulting in death. JAMA1966;198:201–3.
304 LEE, YOON, & KIST
[47] Lapins J, Ye W, Nyren O, et al. Incidence of cancer among patients with hidradenitis sup-purativa. Arch Dermatol 2001;137:730–4.
[48] Gordon SW. Squamous cell carcinoma arising in hidradenitis suppurativa: case report.Plast Reconstr Surg 1977;60:800–2.
[49] Donsky HJ, Mendelson CG. Squamous cell carcinoma as a complication of hidradenitissuppurativa. Arch Dermatol 1964;90:488–91.
[50] Welsh DA, Powers JS. Elevated parathyroid hormone-related protein and hypercalcemiainapatientwith cutaneous squamous cell carcinomacomplicatinghidradenitis suppurativa.South Med J 1993;86:1403–4.
[51] von der Werth JM, Jemec GB. Morbidity in patients with hidradenitis suppurativa. Br JDermatol 2001;144:809–13.
[52] Wolkenstein P, Loundou A, Barrau K, et al. Quality of life impairment in hidradenitis suppu-rativa: A study of 61 cases. J Am Acad Dermatol 2006;56(4):621–3.
[53] Sartorius K, Lapins J, Emtestam L, et al. Suggestions for uniform outcome variables whenreporting treatment effects in hidradenitis suppurativa. Br J Dermatol 2003;149:211–3.
[54] Hurley H. Axillary hyperhidrosis, apocrine bromhidrosis, hidradenitis suppurativa, andfamilial benign pemphigus. In: Roegnick RH, Roegnick HH, editors. Dermatologic surgery.New York: Marcel Dekker; 1989. p. 717–43.
[55] Shelley WB, Cahn MM. The pathogenesis of hidradenitis suppurativa in man; experimen-tal and histologic observations. AMA Arch Derm 1955;72:562–5.
[56] Boer J, Weltevreden EF. Hidradenitis suppurativa or acne inversa. A clinicopathologicalstudy of early lesions. Br J Dermatol 1996;135:721–5.
[57] Jemec GB, Hansen U. Histology of hidradenitis suppurativa. J Am Acad Dermatol1996;34:994–9.
[58] Yu CC, Cook MG. Hidradenitis suppurativa: a disease of follicular epithelium, rather thanapocrine glands. Br J Dermatol 1990;122:763–9.
[59] Sellheyer K, Krahl D. "Hidradenitis suppurativa" is acne inversa! An appeal to (finally)abandon a misnomer. Int J Dermatol 2005;44:535–40.
[60] Jemec GB, Thomsen BM, Hansen U. The homogeneity of hidradenitis suppurativa lesions.A histological study of intra-individual variation. Apmis 1997;105:378–83.
[61] Attanoos RL, Appleton MA, Douglas-Jones AG. The pathogenesis of hidradenitis suppura-tiva: a closer look at apocrine and apoeccrine glands. Br J Dermatol 1995;133:254–8.
[62] Jemec GB, Gniadecka M. Sebum excretion in hidradenitis suppurativa. Dermatology1997;194:325–8.
[63] Jemec GB, Faber M, Gutschik E, et al. The bacteriology of hidradenitis suppurativa. Der-matology 1996;193:203–6.
[64] Lapins J, Jarstrand C, Emtestam L. Coagulase-negative staphylococci are the most commonbacteria found in cultures from the deep portions of hidradenitis suppurativa lesions, as ob-tained by carbon dioxide laser surgery. Br J Dermatol 1999;140:90–5.
[65] Clemmensen OJ. Topical treatment of hidradenitis suppurativa with clindamycin. Int JDermatol 1983;22:325–8.
[66] Jemec GB, Wendelboe P. Topical clindamycin versus systemic tetracycline in the treatmentof hidradenitis suppurativa. J Am Acad Dermatol 1998;39:971–4.
[67] Mendonca CO, Griffiths CE. Clindamycin and rifampicin combination therapy for hidra-denitis suppurativa. Br J Dermatol 2006;154:977–8.
[68] Boer J, van Gemert MJ. Long-term results of isotretinoin in the treatment of 68 patients withhidradenitis suppurativa. J Am Acad Dermatol 1999;40:73–6.
[69] Mortimer PS, Dawber RP, Gales MA, et al. A double-blind controlled cross-over trial of cy-proterone acetate in females with hidradenitis suppurativa. Br J Dermatol 1986;115:263–8.
[70] Sawers RS, Randall VA, Ebling FJ. Control of hidradenitis suppurativa in women using com-bined antiandrogen (cyproterone acetate) and oestrogen therapy. Br J Dermatol1986;115:269–74.
305HIDRADENITIS SUPPURATIVA
[71] Joseph MA, Jayaseelan E, Ganapathi B, et al. Hidradenitis suppurativa treated with finas-teride. J Dermatolog Treat 2005;16:75–8.
[72] Shaw JC. Low-dose adjunctive spironolactone in the treatment of acne in women: a retro-spective analysis of 85 consecutively treated patients. J Am Acad Dermatol 2000;43:498–502.
[73] Sato K, Matsumoto D, Iizuka F, et al. Anti-androgenic therapy using oral spironolactone foracne vulgaris in Asians. Aesthetic Plast Surg 2006;30:689–94.
[74] Farquhar C, Lee O, Toomath R, et al. Spironolactone versus placebo or in combinationwith steroids for hirsutism and/or acne. Cochrane Database Syst Rev 2003:CD000194.
[75] Bolanowski A, Mannon RB, Holland SM, et al. Successful renal transplantation in patientswith chronic granulomatous disease. Am J Transplant 2006;6:636–9.
[76] Buckley DA, Rogers S. Cyclosporin-responsive hidradenitis suppurativa. J R Soc Med1995;88:289P–90P.
[77] Rose RF, Goodfield MJ, Clark SM. Treatment of recalcitrant hidradenitis suppurativa withoral ciclosporin. Clin Exp Dermatol 2006;31:154–5.
[78] Tsianos EV, Dalekos GN, Tzermias C, et al. Hidradenitis suppurativa in Crohn’s disease.A further support to this association. J Clin Gastroenterol 1995;20:151–3.
[79] Jemec GB. Methotrexate is of limited value in the treatment of hidradenitis suppurativa. ClinExp Dermatol 2002;27:528–9.
[80] Slade DE, Powell BW, Mortimer PS. Hidradenitis suppurativa: pathogenesis and manage-ment. Br J Plast Surg 2003;56:451–61.
[81] Lebwohl B, Sapadin AN. Infliximab for the treatment of hidradenitis suppurativa. J AmAcad Dermatol 2003;49:S275–6.
[82] Sullivan TP, Welsh E, Kerdel FA, et al. Infliximab for hidradenitis suppurativa. Br J Dermatol2003;149:1046–9.
[83] Adams DR, Gordon KB, Devenyi AG, et al. Severe hidradenitis suppurativa treated withinfliximab infusion. Arch Dermatol 2003;139:1540–2.
[84] Martinez F, Nos P, Benlloch S, et al. Hidradenitis suppurativa and Crohn’s disease: re-sponse to treatment with infliximab. Inflamm Bowel Dis 2001;7:323–6.
[85] Roussomoustakaki M, Dimoulious P, Chatzicostas C, et al. Hidradenitis suppurativa asso-ciated with Crohn’s disease and spondyloarthropathy: response to anti-TNF therapy.J Gastroenterol 2003;38:1000–4.
[86] Rosi YL, Lowe L, Kang S. Treatment of hidradenitis suppurativa with infliximab in a patientwith Crohn’s disease. J Dermatolog Treat 2005;16:58–61.
[87] Thielen AM, Barde C, Saurat JH. Long-term infliximab for severe hidradenitis suppurativa.Br J Dermatol 2006;155:1105–7.
[88] Fardet L, Dupuy A, Kerob A, et al. Infliximab for severe hidradenitis suppurativa: Transientclinical efficacy in 7 consecutive patients. J Am Acad Dermatol 2007;56(4):624–8.
[89] Cusack C, Buckley C. Etanercept: effective in the management of hidradenitis suppurativa.Br J Dermatol 2006;154:726–9.
[90] Moul DK, Korman NJ. The cutting edge. Severe hidradenitis suppurativa treated with ada-limumab. Arch Dermatol 2006;142:1110–2.
[91] Scheinfeld N. Treatment of coincident seronegative arthritis and hidradentis supprativawith adalimumab. J Am Acad Dermatol 2006;55:163–4.
[92] Bongartz T, Sutton AJ, Sweeting MJ, et al. Anti-TNF antibody therapy in rheumatoid ar-thritis and the risk of serious infections and malignancies: systematic review and meta-analysis of rare harmful effects in randomized controlled trials. JAMA 2006;295:2275–85.
[93] Bong JL, Shalders K, Saihan E. Treatment of persistent painful nodules of hidradenitis sup-purativa with cryotherapy. Clin Exp Dermatol 2003;28:241–4.
[94] Gold M, Bridges TM, Bradshaw VL, et al. ALA-PDT and blue light therapy for hidradenitissuppurativa. J Drugs Dermatol 2004;3:S32–5.
306 LEE, YOON, & KIST
[95] Lapins J, Sartorius K, Emtestam L. Scanner-assisted carbon dioxide laser surgery: a retro-spective follow-up study of patients with hidradenitis suppurativa. J Am Acad Dermatol2002;47:280–5.
[96] Strauss RM, Pollock B, Stables GI, et al. Photodynamic therapy using aminolaevulinic aciddoes not lead to clinical improvement in hidradenitis suppurativa. Br J Dermatol2005;152:803–4.
[97] O’Reilly DJ, Pleat JM, Richards AM. Treatment of hidradenitis suppurativa with botulinumtoxin A. Plast Reconstr Surg 2005;116:1575–6.
[98] Zeligman I. Temporary x-ray epilation therapy of chronic axillary hidradenitis suppurativa.Arch Dermatol 1965;92:690–4.
[99] Kagan RJ, Yakuboff KP, Warner P, et al. Surgical treatment of hidradenitis suppurativa:a 10-year experience. Surgery 2005;138:734–40 [discussion: 740–1].
[100] Parks RW, Parks TG. Pathogenesis, clinical features and management of hidradenitis sup-purativa. Ann R Coll Surg Engl 1997;79:83–9.
[101] Ritz JP, Runkel N, Haier J, et al. Extent of surgery and recurrence rate of hidradenitis sup-purativa. Int J Colorectal Dis 1998;13:164–8.
[102] Morgan WP, Harding KG, Hughes LE. A comparison of skin grafting and healing by gran-ulation, following axillary excision for hidradenitis suppurativa. Ann R Coll Surg Engl1983;65:235–6.
[103] Mandal A, Watson J. Experience with different treatment modules in hidradenitis suppur-itiva: a study of 106 cases. Surgeon 2005;3:23–6.
[104] Jemec GB. Effect of localized surgical excisions in hidradenitis suppurativa. J Am AcadDermatol 1988;18:1103–7.





























