Embed Size (px)
Citation preview
LWW/AENJ AENJ-08-00029R2.rev January 21, 2009 19:44 Char Count= 0
Advanced Emergency Nursing JournalVol. 31, No. 1, pp. 27–33
Copyright c© 2009 Wolters Kluwer Health | Lippincott Williams & Wilkins
CasesO F N O T EColumn Editor: Elda G. Ramirez, PhD, RN, FNP-BC, FAANP
Patient With a Globe RuptureCarmen T. Paniagua, EdD, RN, CPC, ANP, ACNP-BC;Connie M. Gunter, BSN, MS;Jonathan D. Casciano, MD;Randy P. Maddox, MD
AbstractEye injuries are a leading cause of monocular blindness within the United States. The managementof patients who have sustained eye injuries can be challenging for advanced practice nurses (APNs)who work in emergency care settings. APNs are required to have a thorough understanding ofeye injuries in order to promptly and accurately assess and manage eye emergencies. This articlepresents a case of a patient with an open eye globe rupture and discusses the assessment, diagno-sis, and management for this patient. Key words: emergency eye trauma, eye globe rupture eyeinjury, globe rupture, traumatic globe rupture
IN the United States, nearly 2.4 millioneye injuries occur each year (Centersfor Disease Control and Prevention, Na-
tional Center for Health Statistics, 2008).Approximately 95% of all eye injuries arereported to be minor, with the remain-ing 5% considered to have the potential ofresulting in permanent vision loss and/orpermanent anatomic change (Kuhn, Morris,
From the College of Nursing & College of Medicine andEmergency Department ACNP (Dr Paniagua), Emer-gency Department Nurse III (Ms Gunter), Ophthalmol-ogy Resident PGY-3, Jones Eye Institute (Dr Casciano),and Emergency Medicine (Dr Maddox), University ofArkansas for Medical Sciences, Little Rock.
The authors thank Carolyn Bloom, RN, for her contri-bution.
Corresponding author: Carmen T. Paniagua, EdD, RN,CPC, ANP, ACNP-BC, College of Nursing & College ofMedicine, Emergency Department ACNP, University ofArkansas for Medical Sciences, Little Rock, AR 72205(e-mail: [email protected])
Witherspoon, & Mann, 2006). Emergency de-partments (EDs) treat 0.3% of these injuries(McGwin and Owsley, 2005). Open eye globeinjury is part of this small percentage of trau-matic injury.
CASE REPORT
An 18-year-old Hispanic male presented theED triage area. According to the patient, onthe previous night he had consumed a largeamount of alcohol. During this intoxicatedstate, he injured his right eye after runninginto a glass window. The patient then fellasleep and did not seek medical attention forapproximately 18 hr.
An acute care nurse practitioner (ACNP)working in the nonurgent side of the ED cameto assist with the interpretation in Spanish.The ACNP also performed the history andphysical examination.
27

LWW/AENJ AENJ-08-00029R2.rev January 21, 2009 19:44 Char Count= 0
28 Advanced Emergency Nursing Journal
Table 1. History of present illness for patientwith a right eye injurya
O = Onset: 18 hr ago
L = Location: Right eye
D = Duration: Progressive pain; now
constant
C = Characteristics: Swollen, red, irritated,
right eye
A = Aggravating factors: Photophobia and
bending forward
R = Relieving factors: Unable to obtain
relief with closing the eye
T = Treatment: Patient placed sunglasses
over eyes
aOLDCART mnemonic for history of present illness.
Chief Complaint
The patient stated, “I have an irritation in myright eye.”
History of present illness. The patientstated that the onset of the injury was 18 hrprior. The patient complained of progressivepain and then stated, “It’s constant now.”Thepatient also described a swollen, red, irritatedright eye. He stated that his pain was aggra-vated by photophobia and bending forward;nothing relieved the pain. The patient put apair of sunglasses over his eyes and came tothe ED (Table 1).
Medical history. Noncontributory. Patientdenied any past ocular conditions and deniedever wearing glasses or contact lens. Currentmedications: None. Allergies: No known al-lergies. Immunization status: Tetanus immu-nization was up-to-date.
Surgical history/hospitalizations. None.Family history. Noncontributory.Social history. The patient worked as a
landscaper and he denied tobacco use. Posi-tive for “occasional” alcohol consumption re-ported as 2–3 or 3–4 (as previously statedabove) beers on weekends. He denied anyrecreational drug use, including intravenousdrugs.
Review of systems—Constitutional. Thepatient denied any fever or chills or malaise.
Skin: No rash or itching reported. Head/Eyes/Ears/Nares/Throat (HEENT): No previ-ous blurred vision, pain, or eye trauma. Car-diovascular: No chest pain or palpitations.Pulmonary: No cough or shortness of breath.Gastrointestinal: No vomiting or diarrhea.Genitourinary: No frequency with urinationor discharge. Musculoskeletal: No pain in ex-tremities or joints. Neurologic: No localizingweakness or trouble speaking. Hematopoi-etic: No easy bruising or prolonged bleed-ing. Immunologic: No frequent or recur-rent infections. Psychiatric: No depression oranxiety.
Physical examination—General. The pa-tient is a well-developed, well-nourished, con-scious, and coherent individual in moderatedistress. Vital signs: Oral temperature 98.2◦F(36.7◦C), pulse 72 beats per minute, respi-ratory rate 14 per minute, blood pressure132/74 mmHg, and pulse oximetry was 98%on room air. Skin: Warm and dry. Normaltexture and turgor. HEENT: Head: Normo-cephalic, without evidence of trauma. Eyes:Gross external examination revealed a 1-cmlaceration of the right upper eyelid and a0.5-cm laceration of the right upper eyelidskin crease. In addition, conjunctival hemor-rhage (2+) and scleral buckling with extru-sion of ocular contents was noted (Fig 1). Vi-sual acuity 20/200 right eye and 20/20 lefteye without correction. Visual fields showed
Figure 1. Patient with right eye globe rupture
showing scleral buckling and extrusion of ocular
contents.

LWW/AENJ AENJ-08-00029R2.rev January 21, 2009 19:44 Char Count= 0
January–March 2009 � Vol. 31, No. 1 Patient With a Globe Rupture 29
the six cardinal direction of gaze intact forboth eyes. Extraocular movements were in-tact for both eyes. A teardrop-shaped pupil(i.e., pupil distortion suggestive of globerupture with iris prolapsed) was noted inthe right eye. The right eye was reactiveto light; accommodation was compromisedbecause of the teardrop-shaped pupil. Theleft eye was equal, round, and reactive tolight and accommodation. Intraocular pres-sure reading was deferred because of visibleprolapsed iris of the right eye. Relative af-ferent pupillary response was performed asa reliable way to rule out optic nerve dis-ease. This response was normal for both eyes.Ears: Both ear canals were patent. Tympanicmembranes were clear. Nares: Without rhi-norrhea. Mouth/throat: Mucous membraneswere moist, without erythema or exudate.
Neck: Supple, without adenopathy ormeningismus. Carotids equal. Trachea:Midline. No bruits or jugular venous disten-tion. Chest: Normal AP diameter. Adequateexpansion without retractions. No chestwall tenderness. Lungs are clear bilaterallywith good tidal volume. Abdomen: Soft andnontender without masses, guarding or re-bound tenderness. Bowel sounds active. Nohepatosplenomegaly. Back: Without spinal orcostovertebral angle tenderness. Extremities:Upper extremities—full range of motion.Good strength bilaterally. No cyanosis, club-bing, or edema. Peripheral pulses intact.Sensation intact. Lower extremities—fullrange of motion. Good strength bilaterally.No cyanosis, clubbing, or edema. Peripheralpulses intact. Sensation intact. Neurologic:Alert and oriented to person, place, time, andevent. Cranial nerves II–XII grossly intact.Motor and sensory examination nonfocal.Reflexes symmetric.
IMAGING STUDIES
Computerized tomography (CT) without con-trast was performed to visualize the anatomyof the globe and orbit and to note any in-traocular foreign body (i.e., glass). The CT re-sults were reported as negative. Computer-
Table 2. Differential diagnoses for a patientwith a globe rupture
Conjunctival laceration
Corneal laceration
Retinal detachment
Subconjunctival hemorrhage
Vitreous hemorrhage
ized tomography scanning is the most sensi-tive, readily available imaging study to detectoccult rupture, associated optic nerve injury,and small foreign bodies. CT can also visualizethe anatomy of the globe and orbit (Pokhrel &Loftus, 2007).
DIAGNOSTIC TESTS
Coagulation and complete blood cell countwere ordered. The results were within normallimits.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis for this patientincluded corneal laceration, retinal detach-ment, and vitreous hemorrhage (Table 2). Inaddition, other problems such as subconjunc-tival hemorrhage and conjunctival lacerationneeded to be considered when considering allof the differential diagnoses.
ASSESSMENT/DIAGNOSIS/ICD-9 CODE
Right eye globe rupture/rupture eye with pro-lapse of intraocular tissue 871.1.
ED COURSE
A protective rigid shield was applied to coverthe patient’s right eye, while an emergentconsult was placed to the ophthalmologist.The ACNP conferred with the ED collabo-rative physician, who agreed with the ex-amination and management of this patient.The ophthalmologist noted corneal edemaand opacification with fluorescein under aportable slit lamp (Table 3). The left eye wasalso dilated, which demonstrated a normal

LWW/AENJ AENJ-08-00029R2.rev January 21, 2009 19:44 Char Count= 0
30 Advanced Emergency Nursing Journal
Table 3. Examination findings: Slit lamp
Lids/Lashes: 1-cm laceration of the right
upper eyelid and 0.5-cm laceration of the
right upper-eyelid skin crease
Conjunctiva/Sclera: Conjunctival
hemorrhage (2+) and scleral buckling
with extrusion of ocular contents
Cornea: Approximately (5 mm) corneal
laceration originating at the temporal
limbus and extending centrally; mild
corneal edema and central epithelial
defect
Anterior chamber: Shallow with visible iris
prolapse through the wound
Iris (I): Teardrop-shaped pupil with the apex
of the teardrop pointing to the area where
the iris was prolapsed
Lens: Clear
optic nerve and fundus. The use of di-lute topical 0.5% proparacaine (Opthane) iscontraindicated in patients with globe rup-ture (Roberson, 2007). A prophylactic intra-venous antibiotic was administrated to pre-vent endophthalmitis, an inflammation ofthe intraocular cavities, which can poten-tially have devastating complications includ-ing blindness (Roberson, 2007).
OPERATIVE INTERVENTION
The patient was transported to the operatingroom to repair the globe rupture within anhour of arrival to the ED. The eye wound wasclosed with one 9-0 nylon suture at the limbusand five 10-0 interrupted nylon sutures werealso placed. The patient’s eyelid lacerationswere closed using 6-0 vicryl sutures tied in amare’s tail. A bandage contact lens was placedon his right eye to reduce discomfort fromcorneal epithelial defects, to promote healingof corneal wounds and wound dehiscence af-ter surgery.
POSTOPERATIVE CARE
The patient was discharged postoperativelyto be following up the next day at theophthalmology outpatient clinic. Discharge
instructions included bed rest, wear sun-glasses to prevent ocular injury, moxifloxacin(Vigamox) 0.05% ophthalmic solution, onedrop every hour, to prevent bacterial conjunc-tivitis, prednisolone every 2 hr to decreaseinflammation, brimonidine tartrate/timolol(Combigan) 0.2% ophthalmic solution, 1 droptwice a day, to decrease intraocular pressure,and atropine 1% ointment, 1% solution to beinstilled in the conjunctival sac four times aday. The atropine ophthalmic is a combina-tion of a cycloplegic agent, which paralyzesthe ciliary muscle of the eye resulting in lossof accommodation, and a mydriatic agent thatis used to dilate the pupil to better visualizethe retina (Titcomb, 1999).
The following day at his postoperative ex-amination, the patient’s right eye vision was20/400 and his intraocular pressure was el-evated to 42 mmHg. Eyelid sutures were in-tact without evidence of infection. There was3+ injection of the sclera. Corneal edema waspresent with multiple Descemet’s folds andresidual iris incarceration of the main wound.Descemet’s folds are present in any conditionthat causes inflammation of the cornea or theanterior chamber (Schuler, 2007).
Two days postoperatively, the examina-tion revealed that the patient’s corneal lac-eration was resolving and there was nolonger “leakage.” The patient’s vision was20/80 (both eyes of the vitreous, the gel-like substance that helps the eye maintain itsround shape) with an intraocular pressure of13 mmHg (normal 10–20 mmHg).
The patient was also seen 6 days postoper-atively. Fundus examination of the right eyewas reported as 20/25 and intraocular pres-sure was 11 mmHg. The patient noted thathis vision was much better and denied blurredor double vision or any other symptoms orcomplaints.
DISCUSSION
Healthcare outcomes depend on timely man-agement. Prompt recognition and appropri-ate treatment of ocular trauma is essen-tial. Careful eye examination and certain

LWW/AENJ AENJ-08-00029R2.rev January 21, 2009 19:44 Char Count= 0
January–March 2009 � Vol. 31, No. 1 Patient With a Globe Rupture 31
Figure 2. A. Horizontal section through the eyeball and the optic nerve. B. Ligaments and suspensory
ligament of the eyeball.
ophthalmologic tests can assist nurse practi-tioners with a diagnosis to make decisionsabout appropriate treatment and referral forpatients with ophthalmologic injuries.
When an eye injury/illness presents, thegeneral eye examination should include agross examination (Fig 2), slit-lamp exami-
nation, and fundoscopic examination. If eyepain is reported, topical anesthetic drops canbe used unless they are contraindicated. Theuse of topical anesthetic drops is contraindi-cation in a patient with a globe rupture.
The general eye examination includes vi-sual acuity, visual fields, pupils, EOMs, APDR,
LWW/AENJ AENJ-08-00029R2.rev January 21, 2009 19:44 Char Count= 0
32 Advanced Emergency Nursing Journal
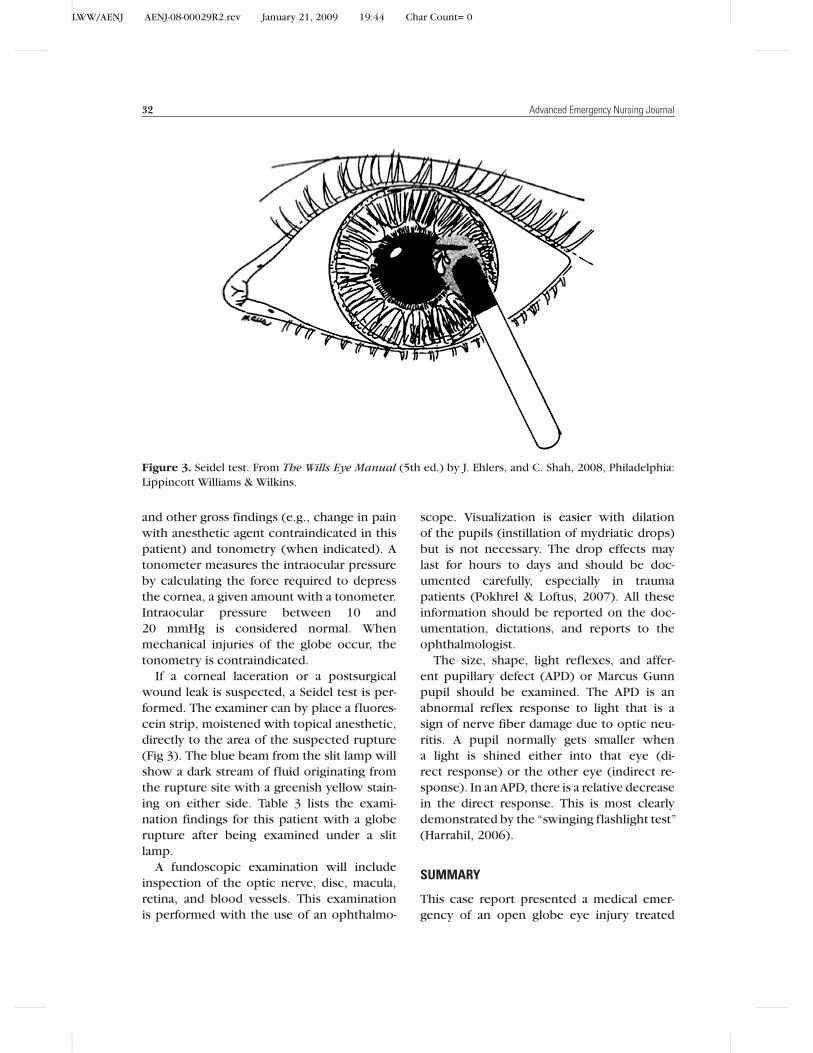
Figure 3. Seidel test. From The Wills Eye Manual (5th ed.) by J. Ehlers, and C. Shah, 2008, Philadelphia:
Lippincott Williams & Wilkins.
and other gross findings (e.g., change in painwith anesthetic agent contraindicated in thispatient) and tonometry (when indicated). Atonometer measures the intraocular pressureby calculating the force required to depressthe cornea, a given amount with a tonometer.Intraocular pressure between 10 and20 mmHg is considered normal. Whenmechanical injuries of the globe occur, thetonometry is contraindicated.
If a corneal laceration or a postsurgicalwound leak is suspected, a Seidel test is per-formed. The examiner can by place a fluores-cein strip, moistened with topical anesthetic,directly to the area of the suspected rupture(Fig 3). The blue beam from the slit lamp willshow a dark stream of fluid originating fromthe rupture site with a greenish yellow stain-ing on either side. Table 3 lists the exami-nation findings for this patient with a globerupture after being examined under a slitlamp.
A fundoscopic examination will includeinspection of the optic nerve, disc, macula,retina, and blood vessels. This examinationis performed with the use of an ophthalmo-
scope. Visualization is easier with dilationof the pupils (instillation of mydriatic drops)but is not necessary. The drop effects maylast for hours to days and should be doc-umented carefully, especially in traumapatients (Pokhrel & Loftus, 2007). All theseinformation should be reported on the doc-umentation, dictations, and reports to theophthalmologist.
The size, shape, light reflexes, and affer-ent pupillary defect (APD) or Marcus Gunnpupil should be examined. The APD is anabnormal reflex response to light that is asign of nerve fiber damage due to optic neu-ritis. A pupil normally gets smaller whena light is shined either into that eye (di-rect response) or the other eye (indirect re-sponse). In an APD, there is a relative decreasein the direct response. This is most clearlydemonstrated by the “swinging flashlight test”(Harrahil, 2006).
SUMMARY
This case report presented a medical emer-gency of an open globe eye injury treated

LWW/AENJ AENJ-08-00029R2.rev January 21, 2009 19:44 Char Count= 0
January–March 2009 � Vol. 31, No. 1 Patient With a Globe Rupture 33
by an ACNP in the ED. The assessment,management, and evaluation of this eyeemergency were discussed. Pertinent clini-cal documentation was presented to ensureproper referral and key components of eval-uation and management code. Furthermore,this case report provides evidence-based re-search, which supports the need for an im-proved partnership and/or collaboration be-tween physicians and ACNPs alike in order toachieve broader medical care benefits.
REFERENCES
Centers for Disease Control and Prevention, National
Center for Health Statistics. (2008). National hos-pital ambulatory medical care survey 1995–2005.
Retrieved May 26, 2008, from http://www.cdc.gov/
nchs/about/major/ahcd/ahcd1.htm
Harrahill, M. M. (2006). A case report of traumatic eye
compartment syndrome. Journal of Emergency Nurs-ing, 1(32), 104–105.
Kuhn, F., Morris, R., Witherspoon, D. C., & Mann, L.
(2006). Epidemiology of blinding trauma in the United
States eye injury registry. Ophthalmic Epidemiology,
13(3), 209–216.
McGwin, G., & Owsley, C. (2005). Incidence of
emergency department–treated eye injury in the
United States. Archives of Ophthalmology, 123, 662–
663.
Pokhrel, P. K., & Loftus, S. A. (2007). Ocular emergencies.
American Family Physician, 76(6), 829–836.
Roberson, J. (2007). Globe rupture. Emedicine on-line. Retrieved June 6, 2008, from http://www.
emedicine.com/EMERG/topic218.htm
Schuler, M. F. (2007). Descemet membrane folds.
Emedicine online. Retrieved August 31, 2008, from
http://www.emedicine.com/oph/topic546.htm
Titcomb, L. (1999). Mydriatic–cycloplegic drugs and
corticosteroids. The Pharmaceutical Journal,263(7075), 900–905.