Embed Size (px)
Citation preview

Advanced Concept of Nursing- IIUNIT- IV
Advance Nursing Managementof Respiratory diseases.
In The Name of God
(A PROJECT OF NEW LIFE COLLEGE OF NURSING KARACHI)
UNIT- IVAdvance Nursing Management
of Respiratory diseases.Shahzad Bashir
RN, BScN, DCHN,MScN (Std.DUHS)Instructor
New Life College of NursingUpdated on April 18, 2016

Objectives
• At the end of the unit, students will be able to:1. Utilize Functional health pattern to identify patients problems
related to respiratory disorders including:1.Asthma2.Chronic obstructive pulmonary disorder (COPD)3.Pneumonia4.Pulmonary tuberculosis (TB)
2. Integrate pathophysiology and pharmacology concepts ofrespiratory disease
3. Apply nursing process with support on Evidence-Based Nursing(EBN) to provide to the clients with respiratory disorders
4. Discuss the holistic approach for nursing management of thepatient with respiratory diseases
5. Develop a teaching plan for a client experiencing disorders of therespiratory disorders.
• At the end of the unit, students will be able to:1. Utilize Functional health pattern to identify patients problems
related to respiratory disorders including:1.Asthma2.Chronic obstructive pulmonary disorder (COPD)3.Pneumonia4.Pulmonary tuberculosis (TB)
2. Integrate pathophysiology and pharmacology concepts ofrespiratory disease
3. Apply nursing process with support on Evidence-Based Nursing(EBN) to provide to the clients with respiratory disorders
4. Discuss the holistic approach for nursing management of thepatient with respiratory diseases
5. Develop a teaching plan for a client experiencing disorders of therespiratory disorders.
8/22/2016 2Shahzad Bashir NLCON

• Asthma is a chronic inflammatory pulmonarydisorder that is characterized by reversibleobstruction of the airways.
• Chronic inflammatory disorder of airways,which causes airway hyper responsivenessleading to Bronchospasm, wheezing,breathlessness, chest tightness, and cough
• Asthma is a chronic inflammatory pulmonarydisorder that is characterized by reversibleobstruction of the airways.
• Chronic inflammatory disorder of airways,which causes airway hyper responsivenessleading to Bronchospasm, wheezing,breathlessness, chest tightness, and cough
38/22/2016 Shahzad Bashir NLCON

• Allergens – 40% of all cases• Exposure to animal fur, pollen grains, mites.• Exercise, worse with exposure to cold air• Air pollutants – cigarette or wood smoke,
vehicle exhaust, sulfur dioxide (SO4), NO4
• Occupational factors• Respiratory infections• Nose and sinus problems
• Allergens – 40% of all cases• Exposure to animal fur, pollen grains, mites.• Exercise, worse with exposure to cold air• Air pollutants – cigarette or wood smoke,
vehicle exhaust, sulfur dioxide (SO4), NO4
• Occupational factors• Respiratory infections• Nose and sinus problems
48/22/2016 Shahzad Bashir NLCON

Cont…
• Drugs and Food– Asthma triad: nasal polyps, sensitivity to ASA and
NSAIDs, B-blockers, aerosol– Salicylates found in many foods and beverages– Most common in children
• GERD – exact mechanism unknown• Emotional stress – attacks can lead to panic
and anxiety.• Environmental factors
• Drugs and Food– Asthma triad: nasal polyps, sensitivity to ASA and
NSAIDs, B-blockers, aerosol– Salicylates found in many foods and beverages– Most common in children
• GERD – exact mechanism unknown• Emotional stress – attacks can lead to panic
and anxiety.• Environmental factors
58/22/2016 Shahzad Bashir NLCON
• 1. Brochospasm (immediate stage) AntigenInduced mast cell degranulation-release ofHistamine & other mediators, which eitherdirectly or through neuronal reflexesleads to Broncho spasm.
• 2. Inflammation (Late stage) Factors+Eosinophils +other inflamatory cells maycause damage to epithelium-producingChronic Inflamatory response.
• 1. Brochospasm (immediate stage) AntigenInduced mast cell degranulation-release ofHistamine & other mediators, which eitherdirectly or through neuronal reflexesleads to Broncho spasm.
• 2. Inflammation (Late stage) Factors+Eosinophils +other inflamatory cells maycause damage to epithelium-producingChronic Inflamatory response.
68/22/2016 Shahzad Bashir NLCON

1. Inflammatory cells and mediators• Airway smooth muscle contraction• Bronchospasm: largely reversible with
bronchodilators• Airway edema: increased microvascular
permeability
2. Increases in mucous production andinflammatory exudates may lead to airwayocclusion (“mucous plugging”)
1. Inflammatory cells and mediators• Airway smooth muscle contraction• Bronchospasm: largely reversible with
bronchodilators• Airway edema: increased microvascular
permeability
2. Increases in mucous production andinflammatory exudates may lead to airwayocclusion (“mucous plugging”)
78/22/2016 Shahzad Bashir NLCON

88/22/2016 Shahzad Bashir NLCON

8/22/2016 Shahzad Bashir NLCON 9

8/22/2016 Shahzad Bashir NLCON 10

118/22/2016 Shahzad Bashir NLCON

Pathophysiology
128/22/2016 Shahzad Bashir NLCON

Extrinsic Asthma• In which the asthmatic episode is typically
initiated by a type I hypersensitivity reactioninduced by exposure to an extrinsic antigen.
• Three types of extrinsic asthma are recognized:atopic asthma, occupational asthma (manyforms), and allergic bronchopulmonaryaspergillosis (bronchial colonization withAspergillus organisms followed bydevelopment of immunoglobulin E [IgE]antibodies).
• In which the asthmatic episode is typicallyinitiated by a type I hypersensitivity reactioninduced by exposure to an extrinsic antigen.
• Three types of extrinsic asthma are recognized:atopic asthma, occupational asthma (manyforms), and allergic bronchopulmonaryaspergillosis (bronchial colonization withAspergillus organisms followed bydevelopment of immunoglobulin E [IgE]antibodies).
138/22/2016 Shahzad Bashir NLCON

Cont….• Atopic asthma is the most common type of
asthma; its onset is usually in the first twodecades of life, and it is commonly associatedwith other allergic manifestations in the patientas well as in other family members.
• Serum IgE levels are usually elevated, as is theblood eosinophil count. This form of asthma isbelieved to be driven by CD4+ T cells.
• Atopic asthma is the most common type ofasthma; its onset is usually in the first twodecades of life, and it is commonly associatedwith other allergic manifestations in the patientas well as in other family members.
• Serum IgE levels are usually elevated, as is theblood eosinophil count. This form of asthma isbelieved to be driven by CD4+ T cells.
148/22/2016 Shahzad Bashir NLCON

Intrinsic asthma• In which the triggering mechanisms are
nonimmune.
• In this form, a number of stimuli that have little orno effect in normal subjects can triggerbronchospasm.
• Such factors include aspirin; pulmonaryinfections, especially those caused by viruses;cold; psychological stress; exercise; and inhaledirritants such as sulfur dioxide.
• In which the triggering mechanisms arenonimmune.
• In this form, a number of stimuli that have little orno effect in normal subjects can triggerbronchospasm.
• Such factors include aspirin; pulmonaryinfections, especially those caused by viruses;cold; psychological stress; exercise; and inhaledirritants such as sulfur dioxide.
158/22/2016 Shahzad Bashir NLCON

Cont…
• There is usually no personal or family historyof allergic manifestations, and serum IgElevels are normal. These patients are said tohave an asthmatic diathesis.
• There is usually no personal or family historyof allergic manifestations, and serum IgElevels are normal. These patients are said tohave an asthmatic diathesis.
168/22/2016 Shahzad Bashir NLCON
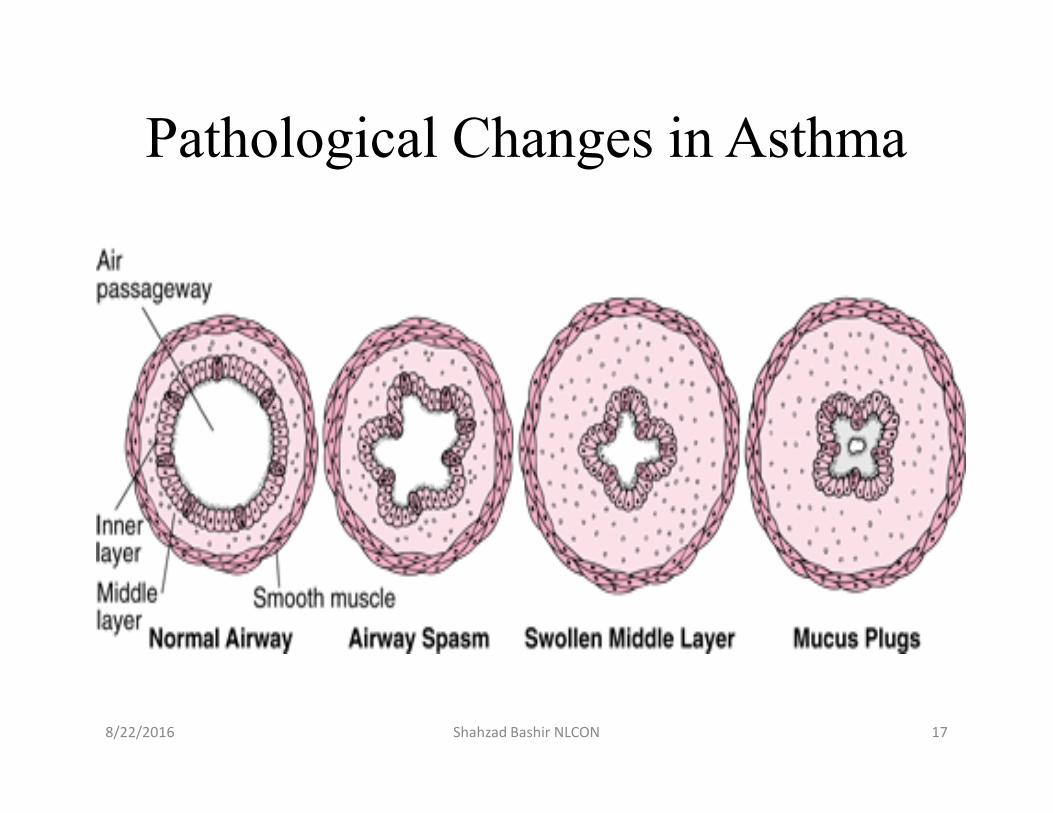
Pathological Changes in Asthma
178/22/2016 Shahzad Bashir NLCON

188/22/2016 Shahzad Bashir NLCON

• Coughing• Wheezing,• Prolong expiratory time [1:3 or 1:4]• Shortness of breath• Chest tightness.
• Coughing• Wheezing,• Prolong expiratory time [1:3 or 1:4]• Shortness of breath• Chest tightness.
198/22/2016 Shahzad Bashir NLCON

Four types:• Mild intermittent:
– Occurs in people with daytime symptoms thatoccur no more frequently than twice a week andnighttime symptoms that occur no more than twicea month. These people are usually asymptomatic.
• Mild persistent:– Characterized by daytime symptoms that occur
more than twice a week but less than once a daywith nighttime symptoms more frequent than twicea month. These people are asymptomatic but haveabnormal pulmonary function tests.
Four types:• Mild intermittent:
– Occurs in people with daytime symptoms thatoccur no more frequently than twice a week andnighttime symptoms that occur no more than twicea month. These people are usually asymptomatic.
• Mild persistent:– Characterized by daytime symptoms that occur
more than twice a week but less than once a daywith nighttime symptoms more frequent than twicea month. These people are asymptomatic but haveabnormal pulmonary function tests.
208/22/2016 Shahzad Bashir NLCON

Conti…• Moderate persistent:
– Occurs in people who have daytime symptomsevery day and nighttime symptoms more than oncea week. Exacerbations limit their activity andoccur at least twice a week, and may last forseveral days.
•Severe persistent (Status Asthmaticus):–Characterized by continual daytime symptoms and frequent
nighttime symptoms. They experience limited physicalactivity and exacerbations are frequent. These people oftentake two medications daily for long term control. Also usingmedications for quick relief on a daily basis indicates a needfor additional long term therapy.
• Moderate persistent:– Occurs in people who have daytime symptoms
every day and nighttime symptoms more than oncea week. Exacerbations limit their activity andoccur at least twice a week, and may last forseveral days.
•Severe persistent (Status Asthmaticus):–Characterized by continual daytime symptoms and frequent
nighttime symptoms. They experience limited physicalactivity and exacerbations are frequent. These people oftentake two medications daily for long term control. Also usingmedications for quick relief on a daily basis indicates a needfor additional long term therapy.
218/22/2016 Shahzad Bashir NLCON

COPD• COPD is a preventable and treatable disease state characterized
by chronic airflow limitation that is not fully reversible.• COPD is irreversible airflow limitation during forced exhalation
caused by loss of elastic recoil & airflow obstruction caused bymucus hyper secretion, & bronchospasm.
• The airflow limitation is usually progressive and associated withan abnormal inflammatory response of the lungs to noxiousparticles or gases, primarily caused by cigarette smoking.
• The irritating effect of the smoke causes hyperplasia of cells,including goblet cells, which subsequently results in increasedproduction of mucus.
• COPD patients may develop respiratory failure accompanied byhypoxemia, carbon dioxide retention resulting in respiratoryacidosis
• COPD is a preventable and treatable disease state characterizedby chronic airflow limitation that is not fully reversible.
• COPD is irreversible airflow limitation during forced exhalationcaused by loss of elastic recoil & airflow obstruction caused bymucus hyper secretion, & bronchospasm.
• The airflow limitation is usually progressive and associated withan abnormal inflammatory response of the lungs to noxiousparticles or gases, primarily caused by cigarette smoking.
• The irritating effect of the smoke causes hyperplasia of cells,including goblet cells, which subsequently results in increasedproduction of mucus.
• COPD patients may develop respiratory failure accompanied byhypoxemia, carbon dioxide retention resulting in respiratoryacidosis
8/22/2016 22Shahzad Bashir NLCON

Conti….• Used for two closely related diseases of the respiratory system,
chronic bronchitis and emphysema• Chronic bronchitis
– Narrowing of the large and small airways, making it moredifficult to move air in and out of the lungs
– Chronic bronchitis is the presence of chronic productivecough for 3 months in each of 2 consecutive years in apatient in whom other causes of chronic cough have beenexcluded.
• Emphysema– Permanent destruction of the alveoli because of irreversible
destruction of elastin, a protein in the lung that is importantfor maintaining the strength of the alveolar walls
• Used for two closely related diseases of the respiratory system,chronic bronchitis and emphysema
• Chronic bronchitis– Narrowing of the large and small airways, making it more
difficult to move air in and out of the lungs– Chronic bronchitis is the presence of chronic productive
cough for 3 months in each of 2 consecutive years in apatient in whom other causes of chronic cough have beenexcluded.
• Emphysema– Permanent destruction of the alveoli because of irreversible
destruction of elastin, a protein in the lung that is importantfor maintaining the strength of the alveolar walls
8/22/2016 Shahzad Bashir NLCON 23

Etiology• Cigarette Smoking (Passive)• Genetics (ATT, α 1 -Antitrypsin), The most
common genotype associated with ATTdisease is ZZ.
• Occupational Chemicals and Dusts.• Air Pollution.• Infections.• Aging.
• Cigarette Smoking (Passive)• Genetics (ATT, α 1 -Antitrypsin), The most
common genotype associated with ATTdisease is ZZ.
• Occupational Chemicals and Dusts.• Air Pollution.• Infections.• Aging.
8/22/2016 Shahzad Bashir NLCON 24

COPD Pathophysiology
• Walls of the small airways and alveoli losetheir elasticity and thicken
• Closes off some of the smaller air passagesand narrows the larger ones
• Air can enter the alveoli but becomestrapped due to the collapsed airways– Affects gas exchange and pathological changes
occur
• Walls of the small airways and alveoli losetheir elasticity and thicken
• Closes off some of the smaller air passagesand narrows the larger ones
• Air can enter the alveoli but becomestrapped due to the collapsed airways– Affects gas exchange and pathological changes
occur
8/22/2016 25Shahzad Bashir NLCON

COPD Pathophysiology• Blood is poorly oxygenated and tissue
perfusion is less efficient• Carbon dioxide may accumulate to critical
levels– Respiratory acidosis– Respiratory failure
• Strains the heart– Right ventricle can enlarge and thicken
• Blood is poorly oxygenated and tissueperfusion is less efficient
• Carbon dioxide may accumulate to criticallevels– Respiratory acidosis– Respiratory failure
• Strains the heart– Right ventricle can enlarge and thicken
8/22/2016 26Shahzad Bashir NLCON

8/22/2016 Shahzad Bashir NLCON 27

8/22/2016 Shahzad Bashir NLCON 28

8/22/2016 Shahzad Bashir NLCON 29

COPD Symptoms• Early
– Early morning cough with clear sputum– Periods of wheezing during or after colds– Shortness of breath on exertion
• Late– Mouth breathing– Puffing– Use of accessory muscles of breathing– Inability to finish sentence without catching one’s
breath– Sleep in semi-sitting position
• Early– Early morning cough with clear sputum– Periods of wheezing during or after colds– Shortness of breath on exertion
• Late– Mouth breathing– Puffing– Use of accessory muscles of breathing– Inability to finish sentence without catching one’s
breath– Sleep in semi-sitting position
8/22/2016 30Shahzad Bashir NLCON

Pneumonia• Lung inflammation caused by bacterial or viral
infection, in which the air sacs fill with pus andmay become solid. Inflammation may affectboth lungs ( double pneumonia ) or only one(single pneumonia ).
• Most common type of infectious disease of thelung
• Lung inflammation caused by bacterial or viralinfection, in which the air sacs fill with pus andmay become solid. Inflammation may affectboth lungs ( double pneumonia ) or only one(single pneumonia ).
• Most common type of infectious disease of thelung
8/22/2016 31Shahzad Bashir NLCON

Pneumonia Pathogens
• Streptococcus pneumonia• Haemophilus influenza• Staphylococcus aureus• Enterobacteriaceae
• Streptococcus pneumonia• Haemophilus influenza• Staphylococcus aureus• Enterobacteriaceae
8/22/2016 32Shahzad Bashir NLCON

Pneumonia Risk Factors
• History of nosocomialpneumonia within thelast 6 to 12 months
• Diagnosed lung disease(COPD)
• Recent hospitalization• Nursing home residence• Smoking• Alcoholism• Neurologic disease
• Immunosuppression• Severe protein-calorie
malnutrition• Heart failure• Eating dependency• Enteral feeding by
nasogastric tube.
• History of nosocomialpneumonia within thelast 6 to 12 months
• Diagnosed lung disease(COPD)
• Recent hospitalization• Nursing home residence• Smoking• Alcoholism• Neurologic disease
• Immunosuppression• Severe protein-calorie
malnutrition• Heart failure• Eating dependency• Enteral feeding by
nasogastric tube.
8/22/2016 33Shahzad Bashir NLCON

Pneumonia Symptoms
• Cough• Fever• Sputum production• Fever• Changes in function,• Appetite
• Cough• Fever• Sputum production• Fever• Changes in function,• Appetite
8/22/2016 34Shahzad Bashir NLCON

Tuberculosis (TB) Overview
• An infectious bacterial diseasecharacterized by the growth of nodules inthe tissues, especially the lungs.
• Spread by droplets when an infectedperson coughs, sneezes, speaks, sings, orlaughs
• Adequate ventilation is the mostimportant measure to prevent transmission
• An infectious bacterial diseasecharacterized by the growth of nodules inthe tissues, especially the lungs.
• Spread by droplets when an infectedperson coughs, sneezes, speaks, sings, orlaughs
• Adequate ventilation is the mostimportant measure to prevent transmission
8/22/2016 35Shahzad Bashir NLCON

8/22/2016 Shahzad Bashir NLCON 36

TB Risk Factors
• Living in an institution• Diabetes mellitus• Use of immunosuppressive drugs• Malignancy• Malnutrition• Renal failure
• Living in an institution• Diabetes mellitus• Use of immunosuppressive drugs• Malignancy• Malnutrition• Renal failure
8/22/2016 37Shahzad Bashir NLCON

Asthma Care• Assist the patient with spirometry testing• Educate the patient regarding proper Use
– Metered-dose inhaler– Nebulizer use– Spacer use– Peak flow meter– Care of the respiratory equipment
• Assist the patient with spirometry testing• Educate the patient regarding proper Use
– Metered-dose inhaler– Nebulizer use– Spacer use– Peak flow meter– Care of the respiratory equipment
8/22/2016 38Shahzad Bashir NLCON

Medications Used to Treat Asthma
• Inhaled corticosteroid therapy• Oral corticosteroids• Inhaled beta2-agonists• Methylxanthine (theophylline)• Ipratropium bromide
• Inhaled corticosteroid therapy• Oral corticosteroids• Inhaled beta2-agonists• Methylxanthine (theophylline)• Ipratropium bromide
8/22/2016 39Shahzad Bashir NLCON

Medications Used to Treat COPD• Are similar to those used to treat asthma
– Bronchodilators– Inhaled corticosteroids– Antibiotics– Influenza and pneumococcal vaccines– Expectorants– Other drugs to treat associated symptoms
such as diuretics, analgesics, coughsuppressants, and anxiolytics
• Are similar to those used to treat asthma– Bronchodilators– Inhaled corticosteroids– Antibiotics– Influenza and pneumococcal vaccines– Expectorants– Other drugs to treat associated symptoms
such as diuretics, analgesics, coughsuppressants, and anxiolytics
8/22/2016 40Shahzad Bashir NLCON

COPD Education• Additional methods used to help loosen
and remove secretions– Postural drainage– Chest percussion– Controlled coughing– Tracheal suctioning
• Smoking cessation
• Additional methods used to help loosenand remove secretions– Postural drainage– Chest percussion– Controlled coughing– Tracheal suctioning
• Smoking cessation
8/22/2016 41Shahzad Bashir NLCON

TB Treatment
• Several antibiotics that are prescribed for6 to 12 months
• Patients must take their medication at thesame time every day to prevent resistance
• Several antibiotics that are prescribed for6 to 12 months
• Patients must take their medication at thesame time every day to prevent resistance
8/22/2016 42Shahzad Bashir NLCON

• Detailed History and exposure• Pulmonary function tests• Peak flow monitoring• Chest X-ray• ABGs• Oximetry• Allergy testing• Blood testing• Sputum C & S
• Detailed History and exposure• Pulmonary function tests• Peak flow monitoring• Chest X-ray• ABGs• Oximetry• Allergy testing• Blood testing• Sputum C & S
438/22/2016 Shahzad Bashir NLCON

• Bronchodilators (Sympathomimetics)• Bronchodilators (Anticholinergics)• Inhaled Corticosteroids• Biologic Response Modifiers (Monoclonal
Antibodies)• Leukotriene Receptor Antagonists• Mast Cell Stabilizers• Methylxanthene Derivatives
• Bronchodilators (Sympathomimetics)• Bronchodilators (Anticholinergics)• Inhaled Corticosteroids• Biologic Response Modifiers (Monoclonal
Antibodies)• Leukotriene Receptor Antagonists• Mast Cell Stabilizers• Methylxanthene Derivatives
448/22/2016 Shahzad Bashir NLCON

• Albuterol• Salmeterol• Terbutalin• Ipratropium(anticholinnergic )
• Albuterol• Salmeterol• Terbutalin• Ipratropium(anticholinnergic )
458/22/2016 Shahzad Bashir NLCON

• Beclamethasone• Flunisolide• Triamcinalone
• Beclamethasone• Flunisolide• Triamcinalone
468/22/2016 Shahzad Bashir NLCON

• Montelukast• Zafirlukast• Montelukast• Zafirlukast
478/22/2016 Shahzad Bashir NLCON

Take History:• History• Occupation (certain occupations have
increased risk for lung disease related toenvironmental work conditions)
• Allergies• Recent pulmonary infection
Take History:• History• Occupation (certain occupations have
increased risk for lung disease related toenvironmental work conditions)
• Allergies• Recent pulmonary infection
488/22/2016 Shahzad Bashir NLCON

Assess S/S• Dyspnea• Decreased respiratory effort• Wheezing• Chest tightness• Accessory muscle use• Decreased breath sounds• Decreased oxygen saturation
Assess S/S• Dyspnea• Decreased respiratory effort• Wheezing• Chest tightness• Accessory muscle use• Decreased breath sounds• Decreased oxygen saturation
498/22/2016 Shahzad Bashir NLCON

• Ineffective breathing pattern R/Lbronchospasm.
• Ineffective airway clearance R/L accumulationof secretion in airway passage.
• Activity intolerance R/L decreased O2 supplyto the tissues of the body.
• Risk for infection
• Ineffective breathing pattern R/Lbronchospasm.
• Ineffective airway clearance R/L accumulationof secretion in airway passage.
• Activity intolerance R/L decreased O2 supplyto the tissues of the body.
• Risk for infection
508/22/2016 Shahzad Bashir NLCON

Desired out come– Control/eliminate symptoms– Attain normal lung function– Restore normal activities– Reduce/eliminate exacerbations and side effects
of meds
Desired out come– Control/eliminate symptoms– Attain normal lung function– Restore normal activities– Reduce/eliminate exacerbations and side effects
of meds
518/22/2016 Shahzad Bashir NLCON

• Mild intermittent and mild persistent– Avoid triggers of acute attacks– Premedicate before exercising
• Acute episode– Medications for daily control including names,
dosages, and frequencies– O2 should be started and monitored with pulse
oximetry or ABGs– Metered dose inhaler (MDI) with ß-adrenergic
agonists, and antiinflamatory
• Mild intermittent and mild persistent– Avoid triggers of acute attacks– Premedicate before exercising
• Acute episode– Medications for daily control including names,
dosages, and frequencies– O2 should be started and monitored with pulse
oximetry or ABGs– Metered dose inhaler (MDI) with ß-adrenergic
agonists, and antiinflamatory
528/22/2016 Shahzad Bashir NLCON

• Asthma Education• Cognitive Behavioral Therapy (New research)
– Relaxation Exercises
• Asthma Education• Cognitive Behavioral Therapy (New research)
– Relaxation Exercises
538/22/2016 Shahzad Bashir NLCON

References• Porter, P. A & Perry, A. G. (2003). Basic
Nursing: Essentials for practice (5th ed.) St.Louis: Mosby.
• Erb, G. K., (2000). Fundamentals of Nursing:Concept, process and practice (5th ed.).Addison: Wesley.
• Bruner, L.S., & Suddarth, D.S. (2001). Textbook of Medical-Surgical Nursing (9th Ed.).Philadelphia: Lippincott.
• Porter, P. A & Perry, A. G. (2003). BasicNursing: Essentials for practice (5th ed.) St.Louis: Mosby.
• Erb, G. K., (2000). Fundamentals of Nursing:Concept, process and practice (5th ed.).Addison: Wesley.
• Bruner, L.S., & Suddarth, D.S. (2001). Textbook of Medical-Surgical Nursing (9th Ed.).Philadelphia: Lippincott.
8/22/2016 54Shahzad Bashir NLCON

THANKSTHANKS THANKS
8/22/2016 55Shahzad Bashir NLCON





























