Embed Size (px)
Citation preview

Advanced ABG analysis for optimum clinical decision making
Case Moderator: Dr. Bhagya Gunnethillake
Consultant Anesthetist
Case presenter: Dr. M. F. M. Makarim
Senior registrar in Critical Care
Case 1
• A 22 year old female with type I DM, presents to the emergency department with a 1 day history of nausea, vomiting, polyuria, polydypsia and vague abdominal pain.
• O.E. noted for deep sighing breathing, orthostatic hypotension, and dry mucous membranes.

Case 1
Arterial blood gas analysis:
• Inspired oxygen 30% (FiO2 0.3)
• PaO2 129 mmHg
• pH 7.27
• PaCO2 23 mmHg
• HCO3- 11 mmol l-1
• BE - 15 mmol l-1

Case 1
Laboratory Ix:
• Na+ 132 mmol l-1
• K+ 4.0 mmol l-1
• Cl- 93 mmol l-1
• Glucose 420 mg dl-1
• Cr 1.2 mg dl-1
Urinary dipstix
• Ketones negative
• Glucose positive

Case 1A 22 year old female with type I DM, presents to the emergencydepartment with a 1 day history of nausea, vomiting, polyuria,polydypsia and vague abdominal pain.
O.E. noted for deep sighing breathing, orthostatic hypotension,and dry mucous membranes.
Arterial blood gas analysis:
• Insp O2 30% (FiO2 0.3)
• PaO2 129 mmHg
• pH 7.27
• PaCO2 23 mmHg
• HCO3- 11 mmol l-1
• BE - 15 mmol l-1
Laboratory Ix:
• Na 132 mmol l-1
• K 4.0 mmol l-1
• Cl 93 mmol l-1
• Glucose 420 mg dl-1
• Cr 2.6 mg dl-1
Urinary dipstix
• Ketones negative
• Glucose positive

What is the acid base disorder?
1. Elevated anion gap acidosis secondary to DKA
2. Normal anion gap acidosis secondary to DKA
3. Elevated anion gap acidosis secondary to DKA with metabolic alkalosis due to vomiting
4. Elevated anion gap acidosis secondary to lactic acidosis in the setting of vomiting and polyuria leading to hypovolaemia
5. Metabolic alkalosis in the setting of vomiting

Case 1
Expected learning outcomes:
• Using Winter’s formula to asses respiratory compensation in metabolic acidosis
• Calculation of anion gap & delta ratio
• Using anion gap and delta ratio in advanced ABG analysis for differential diagnosis

Case 1What is the acid base disorder?
Based on the clinical scenario, likely acid base disorders in this patient are:
1. Elevated anion gap acidosis secondary to DKA, or2. Elevated anion gap acidosis secondary to lactic
acidosis in the setting of vomiting and polyuria which may lead to hypovolaemia,
and/or 3. Metabolic alkalosis in the setting of vomiting

Case 1What is the acid base disorder?
Patient is acidaemic (pH 7.27).
A low HCO3- represents acidosis and is consistent with the pH; therefore it must be the initial change, I.e. Metabolic Acidosis.
Winter's formula; Expected PaCO2 = 1.5 × [HCO3-]) + 8 ± 2
= 1.5 ×11 + 8 ± 2 = (22.5 - 26.5) mmHg.
Actual PaCO2 was 23 mmHgI.e. adequate compensation and there is no separate respiratory
disorder present

Case 1What is the acid base disorder?
The anion gap is = Na - (Cl + HCO3-)= 132 - (93 + 11) = 28 mmol l-1
(high anion gap metabolic acidosis)
Delta ratio = ∆ Anion gap∆ [HCO3-]
= (AG - 12) _ = (28 - 12) = 16 = 1.2(24 - [HCO3-]) (24 - 11) 13
Since the delta ratio is between 1 and 2, we can deduce that this is a pure anion gap metabolic acidosis.

Case 1What is the acid base disorder?
In severe diabetic ketoacidosis, the acidosis causes acetoacetate to accept an H+ and become betahydroxybutyrate.
Since the nitroprusside reaction on dipstix detects acetoacetate but NOT betahydroxybutyrate, this can be deceptive in very acidotic patients.
Assessment: Compensated elevated anion gap acidosis most likely secondary to DKA

What is the acid base disorder?
1. Elevated anion gap acidosis secondary to DKA
2. Normal anion gap acidosis secondary to DKA
3. Elevated anion gap acidosis secondary to DKA with metabolic alkalosis due to vomiting
4. Elevated anion gap acidosis secondary to lactic acidosis in the setting of vomiting and polyuria leading to hypovolaemia
5. Metabolic alkalosis in the setting of vomiting

Case 2
• A 75-year-old woman is brought to ICUfollowing a VF cardiac arrest, witnessed in amedical ward. This had been preceded by 30min of severe central chest pain. Spontaneouscirculation restored after a shock, but thepatient remained apnoeic and unresponsive.The patient was intubated and handventilated with 100% oxygen until ICU bedwas available.
Case 2
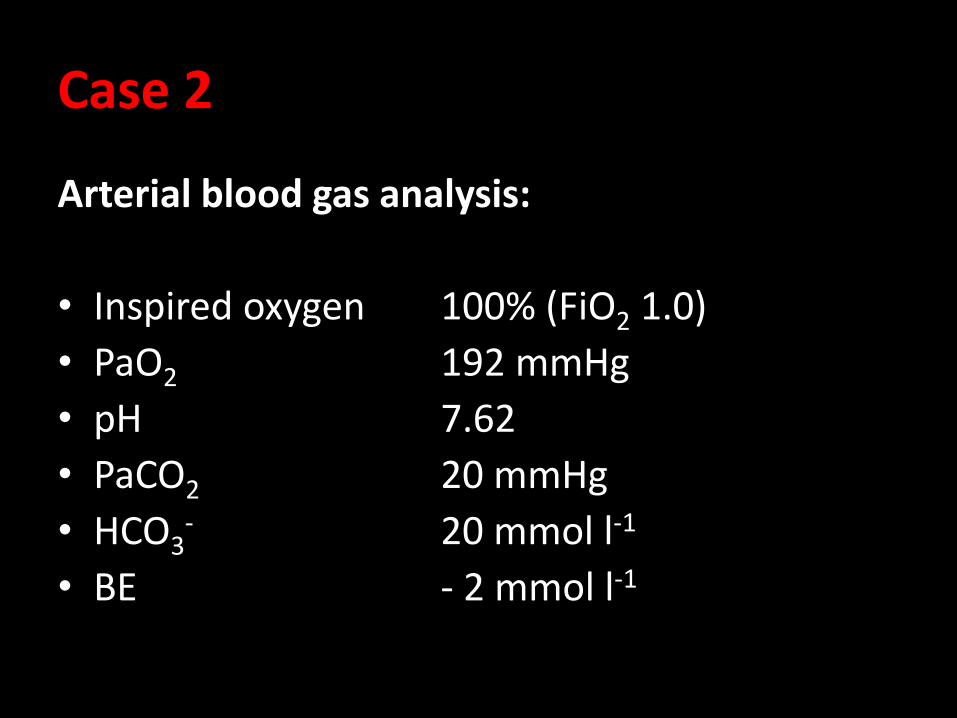
Arterial blood gas analysis:
• Inspired oxygen 100% (FiO2 1.0)
• PaO2 192 mmHg
• pH 7.62
• PaCO2 20 mmHg
• HCO3- 20 mmol l-1
• BE - 2 mmol l-1

Case 2A 75-year-old woman is brought to ICU following a VFcardiac arrest, witnessed in a medical ward. This hadbeen preceded by 30 min of severe central chest pain.Spontaneous circulation restored after a shock, but thepatient remained apnoeic and unresponsive. The patientwas intubated and hand ventilated with 100% oxygenuntil ICU bed was available.
Arterial blood gas analysis:– Inspired oxygen 100% (FiO2 1.0)– PaO2 192 mmHg – pH 7.62– PaCO2 20 mmHg– HCO3
- 20 mmol l-1
– BE - 2 mmol l-1
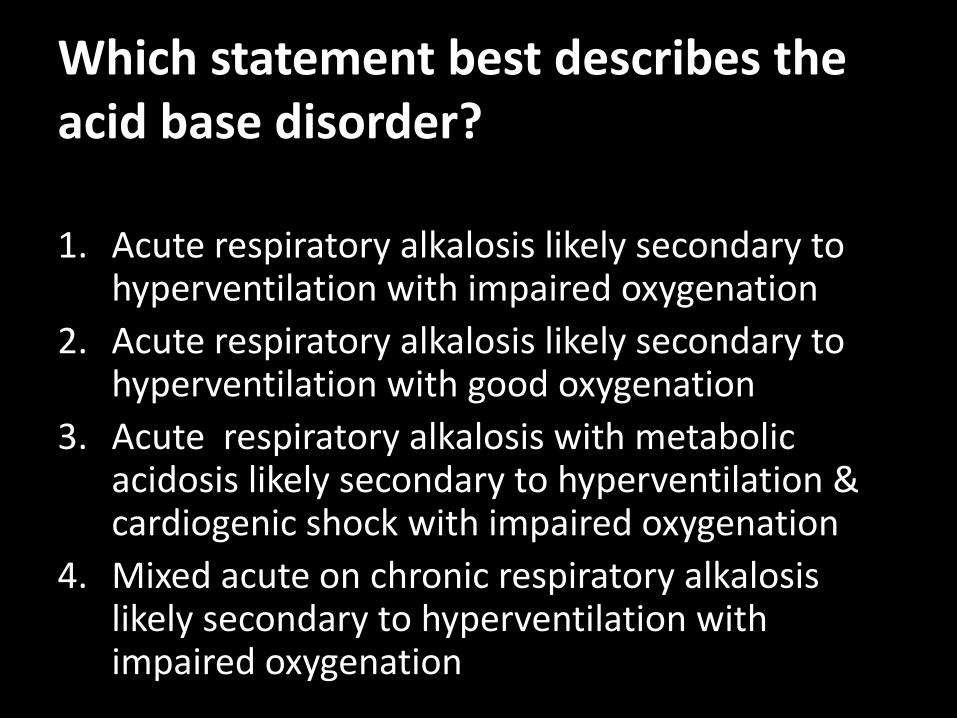
Which statement best describes the acid base disorder?
1. Acute respiratory alkalosis likely secondary to hyperventilation with impaired oxygenation
2. Acute respiratory alkalosis likely secondary to hyperventilation with good oxygenation
3. Acute respiratory alkalosis with metabolic acidosis likely secondary to hyperventilation & cardiogenic shock with impaired oxygenation
4. Mixed acute on chronic respiratory alkalosis likely secondary to hyperventilation with impaired oxygenation

Case 2
Expected learning outcomes:
• Using A-a gradient to assess oxygenation
• Asses renal compensation in respiratory alkalosis

Case 2Comment on oxygenation
• A-a Gradient = PAO2 - PaO2
= [FiO2 (Patm-PH2O) - PaCO2 / 0.8] - PaO2
= [1.0 (760 - 47) – 20 / 0.8] – 192
= 496 mmHg
• Normal A–a gradient is < [age in years + 10] / 4 + (add 5 – 7mmHg for each 10% rise of FiO2
= [75 + 10] / 4 + [6 x (100 – 20) / 10)
= 69.25mmHg

Case 2Comment on oxygenation
• The patient is not hypoxic, but there issignificant impairment of oxygenation asindicated by the gradient between inspiredoxygen and PaO2
• This would fit with aspiration or pulmonaryoedema.

Case 2What is the acid base disorder?
• The patient is alkalaemic
• PaCO2 is low and represents alkalosis and is consistent with the pH. Therefore it must be the initial change. The low HCO3- must be the compensatory response. Since the primary change involves PaCO2, this is a respiratory process, i.e. Respiratory Alkalosis.
Case 2What is the acid base disorder?
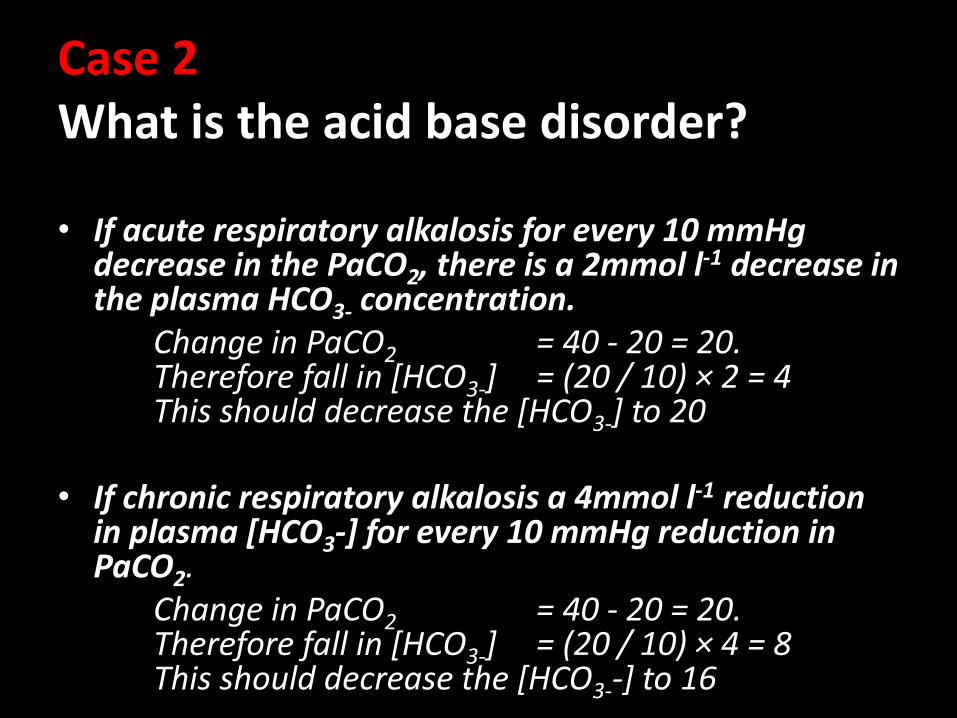
• If acute respiratory alkalosis for every 10 mmHg decrease in the PaCO2, there is a 2mmol l-1 decrease in the plasma HCO3- concentration.
Change in PaCO2 = 40 - 20 = 20.Therefore fall in [HCO3-] = (20 / 10) × 2 = 4This should decrease the [HCO3-] to 20
• If chronic respiratory alkalosis a 4mmol l-1 reduction in plasma [HCO3-] for every 10 mmHg reduction in PaCO2.
Change in PaCO2 = 40 - 20 = 20.Therefore fall in [HCO3-] = (20 / 10) × 4 = 8This should decrease the [HCO3--] to 16

Case 2What is the acid base disorder?
• Since the actual HCO3- is close to the estimated value of acute compensation, we can conclude that this is acute respiratory alkalosis.
• Assessment: Acute respiratory alkalosis likely secondary to hyperventilation with impaired oxygenation.

Which statement best describes the acid base disorder?
1. Acute respiratory alkalosis likely secondary to hyperventilation with impaired oxygenation
2. Acute respiratory alkalosis likely secondary to hyperventilation with good oxygenation
3. Acute respiratory alkalosis with metabolic acidosis likely secondary to hyperventilation & cardiogenic shock with impaired oxygenation
4. Mixed acute on chronic respiratory alkalosis likely secondary to hyperventilation with impaired oxygenation

Case 3
• A 65-year-old man with severe COPD has been found collapsed in the respiratory unit. On initial assessment by the medical officer he is apnoeicbut has an easily palpable carotid pulse.
• He attempted to ventilate his lungs with a bag-mask with oxygen and has called you.
• On your arrival:– Oropharyngeal airway, self inflating bag-mask
ventilation with 10 l min-1
– Carotid pulse palpable, 90 min-1, SpO2 99%– Comatose (GCS 3)

Case 3
Arterial blood gas analysis :
• Inspired oxygen 90% (FiO2 0.9)
• PaO2 147 mmHg
• pH 7.10
• PaCO2 90 mmHg
• HCO3- 34 mmol l-1
• BE - 5 mmol l-1

Case 3A 65-year-old man with severe COPD has been found collapsed in the
respiratory unit. On initial assessment by the medical officer he is apnoeicbut has an easily palpable carotid pulse.
He attempted to ventilate his lungs with a bag-mask and oxygen and has called you.
On your arrival:• Oropharyngeal airway, self inflating bag-mask ventilation with 10 l min-1
• Carotid pulse palpable, 90 min-1, SpO2 99%• Comatose (GCS 3)
Arterial blood gas analysis :
• Inspired oxygen 90% (FiO2 0.9)• PaO2 147 mmHg• pH 7.10 • PaCO2 90 mmHg• HCO3- 34 mmol l-1
• BE - 5 mmol l-1

What is the statement which best describes the acid base disorder?
1. Acute respiratory acidosis likely secondary to respiratory arrest with impaired oxygenation.
2. Chronic respiratory acidosis likely secondary to COPD with impaired oxygenation.
3. A pre-existing compensated chronic respiratory acidosis and an additional acute respiratory acidosis as a result of the respiratory arrest with impaired oxygenation.
4. Acute on chronic respiratory acidosis with an underlying metabolic acidosis with impaired oxygenation.

Case 3
Expected learning outcomes:
• Using A-a gradient to assess oxygenation.
• Asses metabolic compensation in respiratory acidosis.
• Utilizing clinical information for diagnosis in advanced ABG analysis

Case 3Comment on oxygenation
• A-a Gradient = PAO2 - PaO2
= [FiO2 (Patm - PH2O) - PaCO2 / 0.8 ] - PaO2
= [0.9 (760 - 47) – 90 / 0.8] – 147= 382.2 mmHg
• Normal A–a gradient is < [age in years + 10] / 4 + (add 5 – 7mmHg for each 10% rise of FiO2
= [65 + 10] / 4 + [6 x (85 – 20) / 10) = 57.75 mmHg
• The patient is not hypoxic, but there is significant impairment of oxygenation as indicated by the gradient between inspired
oxygen and PaO2

Case 3What is the acid base disorder?
From the history we would predict
• Pre-existing COPD to cause impaired oxygenation and a chronically increased PaCO2.
• The period of apnoea will have further increased his PaCO2, causing a respiratory acidosis.
• Underlying lactic acidosis due to hypoxia during arrest

Case 3What is the acid base disorder?
• Patient is acidaemic (pH 7.10).
• PaCO2 is high and represents acidosis and is consistent with the pH. Therefore it must be the initial change. The high HCO3- must be the compensatory response. Since the primary change involves PaCO2, this is a respiratory process, i.e. Respiratory Acidosis.

Case 3What is the acid base disorder?
• If acute, expected compensation is ↑[HCO3-] = 1 mmol l-1 for every 10 mmHg ∆PaCO2 .
Change in PaCO2 = 90 - 40 = 50 mmHg.Therefore elevation in [HCO3-] = 50/10 × 1 = 5 mmol l-1.This should increase the [HCO3-] to 29 mmol l-1.
• If chronic, expected compensation is ↑[HCO3-] = 3.5 mmol l-1 for every 10 mm Hg ∆PaCO2.
Change in PaCO2 = 90 - 40 = 50 mmHg.Therefore elevation in [HCO3-] = 50 / 10 × 3.5 = 17 .5 mmol l-1
This should increase the [HCO3-] to 41 .5 mmol l-1

Case 3What is the acid base disorder?
• The actual HCO3- is not suggestive of either pure acute respiratory acidosis or chronic respiratory acidosis. – The actual bicarbonate is higher than in pure acute
respiratory acidosis.– It’s lower than pure chronic respiratory acidosis and /
acute on chronic acidosis
• In the pre-existing compensated chronic respiratory acidosis, the pH would have been close to normal.

Case 3What is the acid base disorder?
• The significant acidaemia (pH 7.10) indicates an additional acute respiratory acidosis as a result of the respiratory arrest.
• There is also the possibility of an underlying metabolic acidosis due to hypoxia during arrest causing lactic acidosis explaining the actual bicarbonate level.

Case 3What is the acid base disorder?
• Mixed acute respiratory acidosis with a small metabolic alkalosis
• Assessment: In the presence of a pre-existing compensated chronic respiratory acidosis, an additional mixed acute respiratory acidosis with metabolic acidosis as a result of the respiratory arrest.

What is the statement which best describes the acid base disorder?
1. Acute respiratory acidosis likely secondary to respiratory with impaired oxygenation.
2. Chronic respiratory acidosis likely secondary to COPD with impaired oxygenation.
3. A pre-existing compensated chronic respiratory acidosis and an additional acute respiratory acidosis as a result of the respiratory arrest with impaired oxygenation.
4. Acute on chronic respiratory acidosis with an underlying metabolic acidosis with impaired oxygenation.

Case 4
• A 46 year old problem drinker with a past history of decompensated cirrhosis presents with nausea, vomiting with visual impairment. One of his colleagues confessed they had been celebrating together about 8-12 hours ago, with alcohol they bought illegally.
• On initial examination he is drowsy and he appeared "drunk". His BP was 80/40 mm Hg-1
with a regular heartbeat of 126 beats / min. Respiration rate was 30, but shallow.
Case 4
Arterial blood gas analysis on ADMISSION:
• Inspired oxygen 30% (FiO2 0.3)
• PaO2 92 mmHg
• pH 7.1
• PaCO2 19 mmHg
• HCO3- 6 mmol l-1
• BE - 21.5mmol l-1

Case 4
Laboratory Ix at ICU:
• Na 146 mmol l-1
• K 6.0 mmol l-1
• Cl 111 mmol l-1
• Glucose 4.6 mmol l-1
• Cr 1.1 mg dl-1
• BUN 5.8 mmol l-1
• S. albumin 2.0 g dl-1
• P. osmolarity 379 mOsm l-1

Case 4A 46 year old problem drinker with a past history of decompensatedcirrhosis presents with nausea, vomiting with visual impairment. One of his colleagues confessed they had been celebrating together about 8-12 hours ago, with alcohol they bought illegally. On initial examination he is drowsy and he appeared "drunk". His blood pressure was 80/40 mm/Hg with a regular heartbeat of 126 beats /min. Respiration rate was 30, but shallow.
Arterial blood gas analysis on ADMISSION:
• Insp O2 30% (FiO2 0.3)
• PaO2 92 mmHg
• pH 7.1
• PaCO2 19 mmHg
• HCO3- 6 mmol l-1
• BE - 21.5 mmol l-1
Laboratory Ix at ICU:
• Na 146 mmol l-1
• K 6.0 mmol l-1
• Cl 111 mmol l-1
• Glucose 4.6 mmol l-1
• Cr 1.1 mg dl-1
BUN 5.8 mmol l-1
• S. alb 2.0 g dl-1
• P. osm 379 mOsm l-1

What is the acid base disorder?
1. Elevated anion gap acidosis secondary to non diabetic ketosis.
2. Normal anion gap acidosis secondary to non diabetic ketosis.
3. Elevated anion gap acidosis secondary to non diabetic ketosis with metabolic alkalosis due to vomiting
4. Elevated anion gap acidosis secondary to lactic acidosis in the setting of vomiting and polyurialeading to hypovolaemia
5. Metabolic alkalosis in the setting of vomiting

Case 4
Expected learning outcomes:• Using Winter’s formula to asses respiratory compensation in metabolic
acidosis
• Calculation of anion gap & delta ratio
• Using anion gap and delta ratio in advanced ABG analysis for differential diagnosis
• Correction of anion gap for albumin
• Calculation of osmolarity & osmolar gap and use in differential diagnosis

Case 4What is the acid base disorder?
• Based on the clinical scenario, likely acid base disorders in this patient are:
1. Elevated anion gap acidosis secondary to non diabetic ketosis
or
2. Elevated anion gap acidosis secondary to lactic acidosis in the setting of vomiting and poor oral intake which may lead to hypovolemia
And / or
3. Metabolic alkalosis in the setting of vomiting

Case 4What is the acid base disorder?
• Patient is acidaemic (pH 7.10)
• A low HCO3- represents acidosis and is consistent with the pH; therefore it must be the initial change, I.e. Metabolic Acidosis.
• Winter's formula; Expected PaCO2 = 1.5 × [HCO3-]) + 8 ± 2
= 1.5 x 6 + 8 ± 2 = (15 – 19) mmHg.
Actual PaCO2 19 mmHg, I.e. adequate compensation and there is no separate respiratory disorder present.

Case 4What is the acid base disorder?
• The anion gap is = Na - (Cl + HCO3-) = 146 - (111 + 6) = 29 mmol l-1.
• The approximate correction is a reduction in the normal anion gap of 2.5 mmol l-1 for every 1g dl-1
decline in the plasma albumin concentration (normal value = 4 g dl-1)
• Adjusted normal anion gap = Normal anion gap – (reduction of albumin x 2.5)= 12 - [(4 – 2) × 2.5] = 7 mmol l-1.

Case 4What is the acid base disorder?
• A calculated anion gap of 29 is high when compared to the adjusted anion gap of 7 mmol l-1 (high anion gap metabolic acidosis)
• Delta ratio = ∆ Anion gap = (AG - 7)_ _∆ [HCO3-] (24 - [HCO3-])
= (29 - 7) = 22 = 1.22 (24 – 6) 18
• Since the delta gap is between 1 and 2, we can deduce that this is a pure metabolic acidosis.

Case 4What is the acid base disorder?
• Plasma osmolarity = (2 x Na) + glucose + BUN
= (2x146) + 4.6 + 5.8
= 302.4 mOsm l-1
• Osmolar Gap = Measured Posm – Calculated Posm
= 379 – 302.4 = 76.6 mOsml l-1

Case 4What is the acid base disorder?
• The normal osmolar gap is 10-15 mOsm l-1 .
• The osmolar gap is increased in the presence of low molecular weight substances that are not included in the formula for calculating plasma osmolarity.
• Common substances that increase the osmolar gap are ethylene glycol, methanol and propylene glycol
• Assessment: Compensated elevated anion gap acidosis most likely due to ketoacidosis secondary to methanol

What is the acid base disorder?
1. Elevated anion gap acidosis secondary to non diabetic ketosis.
2. Normal anion gap acidosis secondary to non diabetic ketosis.
3. Elevated anion gap acidosis secondary to non diabetic ketosis with metabolic alkalosis due to vomiting
4. Elevated anion gap acidosis secondary to lactic acidosis in the setting of vomiting and polyurialeading to hypovolaemia
5. Metabolic alkalosis in the setting of vomiting

References..
• Physiological approach to assessment of acid-basedisturbances. Berend K, de Vries AP, Gans RO. N EnglJ Med. 2014 Oct 9;371(15):1434-45.
• Acid Base Online Tutorial, Universi ty of Connecticut
– http://fitsweb.uchc.edu/student/selectives/TimurGraham/Welcome.html



Delta ratio Assessment Guidelines
< 0.4 Hyperchloremic normal anion gap acidosis
0.8 - 0.4 High AG & normal AG acidosis
1 to 2
• Pure Anion Gap Acidosis Lactic acidosis: average value 1.6 DKA more likely to have a ratio closer to 1 due to urine ketone loss
> 2High AG acidosis and a concurrent metabolic alkalosisor a pre-existing compensated respiratory acidosis

































