Embed Size (px)
Citation preview

ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6
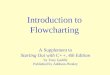
Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred inhaler choices
Patient is currently being prescribed a combination ICS/LABA inhaler that is not an ENHCCG preferred choice
If current Inhaler is:
Seretide Evohaler® MDI (fluticasone/salmeterol)
[125/25 or 250/25 strengths]
If current Inhaler is:
Symbicort Turbohaler® DPI (budesonide/formoterol)
[400/12 and 200/6 strengths]
Sirdupla® MDI (fluticasone/salmeterol)
[125/25 & 250/25 strengths] Generic equivalent that
contains the same ICS and LABA ingredients and is
therapeutically equivalent to corresponding strengths of
Seretide Evohaler®
See switch and step down algorithm on page 3
Flutiform® MDI (fluticasone/formoterol)
[50/5, 125/5 & 250/10 strengths]
Contains the same ICS dose to corresponding strengths of Seretide Evohaler® but contains a different LABA ingredient (formoterol)
See switch and step down
algorithm on page 4
Fostair® MDI (beclometasone
/formoterol) [100/6 strength]
Contains a different ICS (beclometasone) and LABA ingredient (formoterol) to
Seretide Evohaler® See switch and step down
algorithm on page 5
DuoResp Spiromax® DPI (budesonide/formoterol)
[320/9 and 160/4.5 strengths] Generic equivalent that contains
the same ICS and LABA ingredients and is therapeutically
equivalent to corresponding strengths of Symbicort
Turbohaler® DPI
See switch and step down algorithm on page 6
Assess if the patient is suitable to be considered for stepping DOWN treatment (see page 2) or if the patient can be switched to a
corresponding strength of an ENHCCG preferred inhaler choice
DuoResp Spiromax 320/9 provides a delivered dose of budesonide 320mcg and formoterol 9mcg. This is therapeutically equivalent to Symbicort Turbohaler 400/12 metered dose of budesonide 400mcg and formoterol 12mcg which also provides a delivered dose of budesonide 320mcg and formoterol 9mcg. DuoResp Spiromax 160/4.5 provides a delivered dose of budesonide 160mcg and formoterol 4.5mcg. This is therapeutically equivalent to Symbicort Turbohaler 200/6 metered dose of budesonide 200mcg and formoterol 6mcg which also provides a delivered dose of budesonide 160mcg and formoterol 4.5mcg.
MDI: Metered dose inhaler DPI: Dry powder inhaler ICS: Inhaled corticosteroid LABA: Long acting β2 -agonist

ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 2 of 6
YES
NO
NO
YES
NO
How to step adult patients down algorithm
Does the patient have an up to date asthma action plan? Has inhaler use (patient reported and Rx history), inhaler technique, smoking status, adherence, trigger factors, medication side-effects and use of rescue medication been checked? Check expected use of inhaler against patient reported use. Has asthma been completely controlled for at least 3 months?
LEVELS OF ASTHMA CONTROL - Assessment of current clinical control (preferably) over 4 weeks
Characteristic Completely Controlled Partly Controlled Uncontrolled
RCP 3 Questions
Daytime symptoms None (twice or less/week) >Twice/week Three or more features of partly controlled asthma
Limitation on activities None Any
Nocturnal symptoms/awakening None Any
Need for reliever/rescue treatment None (twice or less/week) >Twice/week
Lung Function (PEF or FEV1) Normal <80% predicted or personal best (if known)
Does the patient have any exclusion criteria?
Patient does not agree to step down
Excacerbation, oral steroid course, GP/hospital visit due to worsening asthma in past 6 months
Under respiratory specialist review or pregnant (only step down if agreed with specialist)
Significant adverse outcomes from previous step down attempts. Consider 25% dose reduction if previously unable to step down by 50%
Seasonal exacerbations. Reschedule step down review after season has ended
Lifestyle considerations where stability crucial e.g. impending exam
Maintenance and Reliever Therapy (MART) regime
DO NOT step patient down
Consider reason for poor control or exclusion criteria. Action as appropriate.
Consider STEP UP therapy for uncontrolled symptoms
STEP the patient DOWN – refer to ENHCCG Adult Asthma Guidelines and Step DOWN/Switch Algorithms: - 1. Consider reducing add on therapies before reducing ICS 2. Identify the combination inhaler and dose the patient is currently being
prescribed. Identify which step (3-5) this product and dose represents 3. Refer to the relevant Step DOWN/Switch algorithm for the ICS product 4. Consider switching to an equivalent strength ENHCCG approved lower cost
product for 1 month (to identify any issues/confirm stability) before stepping down. Ensure the patient is trained and can demonstrate they can use any potential new device. If issues with the new product identified return to original product before consideration for stepping down.
5. Reduce dose by 25% - 50%. The dose decrease is an individual clinical decision based on history of stability with respect to day to day symptoms, frequency of exacerbations and previous step down attempts. Consideration should be given to the current ICS dose and the inhaler product and strength that the patient is using. Keep the LABA dose the same when ICS dose when possible
6. Dose reductions of less than 50% may be complicated and may involve using combinations of separate inhalers. Further advice may be sought from respiratory specialist. Note: for patients at step 4 and 5: if also taking add-on therapies (e.g.montelukast, oral steroids), consider reducing/stopping these before attempting to reduce ICS dose. Seek further advice from specialist services.
Considerations for Clinician Patients achieve complete asthma control at different rates. Discuss with the patient to decide whether to trial the current therapy for longer or to step up-again. Suggested discussion points with patient: 1. Any factor affecting adherence e.g.
polypharmacy, social reasons or beliefs?
2. Any issues affecting ability to use inhaler e.g. dexterity?
3. Trigger factors e.g. smoking, pets, pollen, stress?
4. How long did it take the patient to achieve complete control last time?
5. What would be the potential consequences of an exacerbation and does the patient know what to do if this occurs?
6. What would the patient prefer to do? 7. Ensure patient has up to date self-
management/action plan. ACTION Clinicians should use their professional judgement to decide whether to continue trialling current therapy or to step up again. If continuing on current therapy, advise patient to monitor symptoms and reliever use and review again in one month. Advise patient to follow self-management plan if symptoms become problematic within this time. Refer to specialist service as necessary
Patient review at 3 months
Has the patient achieved complete asthma control in
the last 3 months? (see Table 1)
STEP the patient DOWN and repeat cycle
YES
Check & reinforce inhaler technique + /- spacer
Advise patient of importance of adherence
Ensure patient has current asthma action plan
Ensure patient understands if symptoms worsen when to increase dose and seek medical advice
Agree a review date for 3 months’ time
If unclear, advise patient to complete peak flow diary and then re-assess

ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 3 of 6
Key: There is not an equivalent strength Sirdupla® inhaler for Seretide 50 Evohaler®. Consider using Flutiform® 50 MDI which contains the equivalent fluticasone dose as Seretide 50 Evohaler® but a different LABA (formoterol) *Total daily dose inhaled corticosteroid (ICS), in terms of beclometasone dipropionate (BDP) equivalent Costs: 30 day costs (without a spacer) [Sep 2016]
Step down to lower strength Sirdupla®/Flutiform® MDI
Switch to equivalent strength Sirdupla®/ Flutiform® MDI (review after 1 month to identify any issues before consideration for step down. Switch back to Seretide if issues identified)
Step down to lower strength Seretide Evohaler® (if cannot use Sirdupla eg cannot have alcohol or Flutiform eg cannot have alcohol/formoterol or issues when switched to Sirdupla)
Ensure patient has achieved complete asthma control before stepping down (see Page 2)
Sirdupla® (fluticasone/salmeterol) MDI is a therapeutically equivalent alternative to Seretide Evohaler®. It is an ENHCCG approved lower cost ICS/LABA fixed dose combination MDI for asthma. It is lower cost for patients on Seretide Evohaler® (prescribed by brand or generic) to be switched to the equivalent corresponding strength Sirdupla® MDI. PRESCRIBE BY BRAND NAME
Seretide 250 Evohaler® [MDI] (fluticasone/salmeterol)
[1 puff = 500mcg BDP equiv.] 2 puffs bd (£59.48)
(2000mcg BDP* equiv/day + 100mcg salmeterol/day)
Step 4/5 - Up to 2000mcg BDP* equivalent/day - Addition of 4
th drug (e.g. montekukast, SR theophylline) } Consider reducing these
- Addition of 5th
drug – oral prednisolone [Step 5] } before reducing the ICS
Seretide 125 Evohaler® [MDI] (fluticasone/salmeterol)
[1 puff = 250mcg BDP equiv.] 2 puffs bd (£35.00)
(1000mcg BDP* equiv/day + 100mcg salmeterol/day)
Seretide 50 Evohaler® [MDI] (fluticasone/salmeterol)
[1 puff = 100mcg BDP equiv.] 2 puffs bd (£18.00)
(400mcg BDP* equiv/day + 100mcg salmeterol/day)
If patient is at Step 4/5, consider respiratory specialist advice on how to manage step down process, particularly if a more gradual ICS dose reduction (<50%) is required than the combination devices in the above algorithm allow. This may involve using combinations of different inhalers. If under respiratory specialist review - do not attempt step down without agreement of specialist.
Step 3 - Add long-acting beta2 agonist (LABA) - Up to 800mccg BDP* equivalent/day
Clenil Modulite® [MDI] 100mcg (beclometasone)
2 puffs bd (£4.45) OR
Qvar® [MDI] 50mcg (fine particle beclometasone)
2 puffs bd (£4.72) [NB Qvar® twice as potent as Clenil®)
OR Flixotide 50 Evohaler®
[MDI] (fluticasone) 2 puffs bd (£5.44)
(if the patient cannot tolerate a change in ICS
from fluticasone)
All patients with asthma should have an up to date asthma action plan and be provided with a short-acting beta2 agonist (salbutamol MDI or Easyhaler®) to aid in the event of an exacerbation.
Sirdupla ® 125 [MDI] (fluticasone/salmeterol)
[1 puff = 250mcg BDP equiv.] 2 puffs bd (£26.25)
(1000mcg BDP* equiv./day + 100mcg salmeterol/day)
Flutiform® 50 [MDI] (fluticasone/formoterol)
[1 puff = 100mcg BDP equiv.] 2 puffs bd (£14.40)
(400mcg BDP* equiv./day + 20mcg formoterol/day)
Sirdupla® 250 [MDI] (fluticasone/salmeterol)
[1 puff = 500mcg BDP equiv.] 2 puffs bd (£44.61)
(2000mcg BDP* equiv./day + 100mcg salmeterol/day)
Step 2 Standard dose ICS
[400mcg BDP* equivalent/day]
Asthma Step DOWN/Switch Algorithm for Seretide Evohaler® and Sirdupla® in Adults (>18yrs) (devised from BTS/SIGN guidance and the relevant Summary of Product Characteristics)

ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 4 of 6
Step down to lower strength Flutiform® MDI
Switch to equivalent strength Flutiform® MDI (review after 1 month to identify any issues before consideration for step down. Switch back to Seretide if issues identified)
Step down to lower strength Seretide Evohaler® (if cannot use Flutiform® eg cannot have alcohol or intolerant to formoterol or issues when switched to Flutiform)
Ensure patient has achieved complete asthma control before stepping down (see Page 2)
If patient is at Step 4/5, consider respiratory specialist advice on how to manage step down process, particularly if a more gradual ICS dose reduction (<50%) is required than the combination devices in the above algorithm allow. This may involve using combinations of different inhalers. If under respiratory specialist review - do not attempt step down without agreement of specialist.
Step 3 - Add long-acting beta2 agonist (LABA) - Up to 800mccg BDP* equivalent/day
Step 2 Standard dose ICS
[400mcg BDP* equivalent/day]
Key: If taking add-on therapies e.g. montelukast, oral prednisolone, consider reducing these before reducing the ICS.
* Total daily dose inhaled corticosteroid (ICS), in terms of beclometasone dipropionate (BDP) equivalent Costs: 30 day costs (without a spacer) [Sep 2016]
All patients with asthma should have an up to date asthma action plan and be provided with a short-acting beta2 agonist (salbutamol MDI or Easyhaler®) to aid in the event of an exacerbation.
Flutiform® 125/5 [MDI] (fluticasone/formoterol)
[1 puff = 250mcg BDP equiv.] 2 puffs bd (£28.00)
(1000mcg BDP* equiv./day + 20mcg formoterol/day)
Flutiform® 50/5 [MDI] (fluticasone/formoterol)
[1 puff = 100mcg BDP equiv.] 2 puffs bd (£14.40)
(400mcg BDP* equiv./day + 20mcg formoterol/day)
Flutiform® 250/10 [MDI] (fluticasone/fomoterol)
[1 puff = 500mcg BDP equiv.] 2 puffs bd (£45.56)
(2000mcg BDP* equiv./day + 40mcg formoterol/day)
Flutiform® (fluticasone propionate/formoterol) is an ENHCCG approved lower cost ICS/LABA fixed dose combination MDI for asthma. It contains the equivalent dose of fluticasone to Seretide Evohaler® but contains a different LABA (formoterol). It is lower cost for patients on Seretide Evohaler® (prescribed by brand or generic) to be switched to equivalent strength Flutiform® MDI. PRESCRIBE BY BRAND NAME
Asthma Step DOWN/Switch Algorithm for Seretide Evohaler® and Flutiform® in Adults (>18yrs) (devised from BTS/SIGN guidance and the relevant Summary of Product Characteristics)
Seretide 250 Evohaler® [MDI] (fluticasone/salmeterol)
[1 puff = 500mcg BDP equiv.] 2 puffs bd (£59.48)
(2000mcg BDP* equiv/day + 100mcg salmeterol/day)
Seretide 125 Evohaler® [MDI] (fluticasone/salmeterol)
[1 puff = 250mcg BDP equiv.] 2 puffs bd (£35.00)
(1000mcg BDP* equiv/day + 100mcg salmeterol/day)
Seretide 50 Evohaler® [MDI] (fluticasone/salmeterol)
[1 puff = 100mcg BDP equiv.] 2 puffs bd (£18.00)
(400mcg BDP* equiv/day + 100mcg salmeterol/day)
Step 4/5 - Up to 2000mcg BDP* equivalent/day - Addition of 4
th drug (e.g. montekukast, SR theophylline) }
- Addition of 5th
drug – oral prednisolone [Step 5] }
Clenil Modulite® [MDI] 100mcg (beclometasone)
2 puffs bd (£4.45) OR
Qvar® [MDI] 50mcg (fine particle beclometasone)
2 puffs bd (£4.72) [NB Qvar® twice as potent as Clenil®)
OR Flixotide 50 Evohaler®
[MDI] (fluticasone) 2 puffs bd (£5.44)
(if the patient cannot tolerate a change in ICS
from fluticasone)

ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 5 of 6
Step down to lower BDP equiv. strength Fostair® MDI
Switch to equiv. BDP strength Fostair® MDI (review after 1 month to identify any issues before consideration for step down. Switch back to Seretide if issues identified)
Step down to lower strength Seretide Evohaler® (if cannot use Fostair® eg cannot have alcohol / beclometasone / formoterol or issues when switched to Fostair)
Ensure patient has achieved complete asthma control before stepping down (see Page 2)
Asthma Step DOWN/Switch Algorithm for Seretide Evohaler® and Fostair® in Adults (>18yrs) (devised from BTS/SIGN guidance and the relevant Summary of Product Characteristics)
Seretide 250 Evohaler® (fluticasone/salmeterol)
[1 puff = 500mcg BDP equiv.] 2 puffs bd (£59.48)
(2000mcg BDP* equiv/day + 100mcg salmeterol/day)
Step 4/5 - Up to 2000mcg BDP* equivalent/day - Addition of 4
th drug (e.g. montekukast, SR theophylline)
- Addition of 5th
drug – oral prednisolone [Step 5]
Seretide 125 Evohaler® (fluticasone/salmeterol)
[1 puff = 250mcg BDP equiv.] 2 puffs bd (£35.00)
(1000mcg BDP* equiv/day + 100mcg salmeterol/day)
Seretide 50 Evohaler® (fluticasone/salmeterol)
[1 puff = 100mcg BDP equiv.] 2 puffs bd (£18.00)
(400mcg BDP* equiv/day + 100mcg salmeterol/day)
If patient is at Step 4/5, consider respiratory specialist advice on how to manage step down process, particularly if a more gradual ICS dose reduction (<50%) is required than the combination devices in the above algorithm allow. This may involve using combinations of different inhalers. If under respiratory specialist review - do not attempt step down without agreement of specialist.
Step 3 - Add long-acting beta2 agonist (LABA) - Up to 800mccg BDP* equivalent/day
Clenil Modulite® [MDI] 100mcg (beclometasone)
2 puffs bd (£4.45) OR
Qvar® [MDI] 50mcg (fine particle beclometasone)
2 puffs bd (£4.72) [NB Qvar® twice as potent as Clenil®)
OR Flixotide 50 Evohaler®
[MDI] (fluticasone) 2 puffs bd (£5.44)
(if the patient cannot tolerate a change in ICS
from fluticasone)
Step 2 Standard dose ICS
[400mcg BDP* equivalent/day]
Fostair® 100/6 MDI (beclometasone/formoterol) [1 puff = 250mcg BDP equiv.
+ 6 mcg formoterol]
2 puffs bd (£29.32)
(1000mcg BDP* equiv./day + 24mcg formoterol/day)
Fostair® 100/6 MDI (beclometasone/formoterol) [1 puff = 250mcg BDP equiv.
+ 6 mcg formoterol]
1 puff bd (£14.66)
(500mcg BDP* equiv./day + 12mcg formoterol/day)
Fostair® (beclometasone/formoterol) is an ENHCCG approved lower cost ICS/LABA fixed dose combination MDI for asthma and COPD. It contains a different IC and LABA to that contained in Seretide®. It is lower cost for patients on Seretide Evohaler® (prescribed by brand or generic) to be switched to equivalent strength Fostair® MDI. PRESCRIBE BY BRAND NAME
All patients with asthma should have an up to date asthma action plan and be provided with a short-acting beta2 agonist (salbutamol MDI or Easyhaler®) to aid in the event of an exacerbation.
Key: If taking add-on therapies e.g. montelukast, oral prednisolone, consider reducing these before reducing the ICS.
* Total daily dose inhaled corticosteroid (ICS), in terms of beclometasone dipropionate (BDP) equivalent Costs: 30 day costs (without a spacer) [Sep 2016]

ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 6 of 6
Step down to lower strength DuoResp Spiromax®
Switch to equivalent strength DuoResp Spiromax® (review after 1 month to identify any issues before consideration for step down. Switch back to Symbicort if issues identified)
Step down to lower strength Symbicort Turbohaler® (if cannot use DuoResp eg issues with new device when switched to DuoResp)
quivalent/day
Ensure patient has achieved complete asthma control before stepping down (see page 2)
DuoResp Spiromax®
Symbicort Turbohaler® 400/12
(budesonide/formoterol) [1 puff = 400mcg BDP equiv.]
2 puffs bd (£76.00)
(1600mcg BDP* equiv./day + 48mcg formoterol/day)
Symbicort Turbohaler® 400/12 (budesonide/formoterol)
[1 puff = 400mcg BDP equiv.] 1 puff bd (£38.00)
OR
Symbicort Turbohaler® 200/6 (budesonide/formoterol)
[1 puff = 200mcg BDP equiv.] 2 puffs bd (£38.00)
(800mcg BDP* equiv./day + 24mcg formoterol/day)
Symbicort Turbohaler® 100/6
(budesonide/formoterol) [1 puff = 100mcg BDP equiv.]
2 puffs bd (£33.00) (400mcg BDP* equiv/day + 24mcg formoterol/day)
Easyhaler® Beclometasone 200mcg [DPI] 1 puff bd (£4.48)
OR
Easyhaler® Budesonide 200mcg [DPI] 1 puff bd (£5.31)
Asthma Step Down/Switch Algorithm for Symbicort Turbohaler® and DuoResp Spiromax® in Adults (>18yrs) (devised from BTS guidance and the relevant Summary of Product Characteristics)
Step 4/5 - Up to 2000mcg BDP* equivalent/day - Addition of 4
th drug (e.g. montekukast, SR theophylline)
- Addition of 5th
drug – oral prednisolone [Step 5]
Step 3 - Add long-acting beta2 agonist (LABA) - Up to 800mcg BDP* equivalent/day
Step 2 Standard dose ICS
[400mcg BDP* equivalent/day]
DuoResp Spiromax® 320/9
(budesonide/formoterol) [1 puff = 400mcg BDP
equiv.
2 puffs bd (£59.94)
(1600mcg BDP* equiv./day + 48mcg formoterol/day)
DuoResp Spiromax® 320/9 (budesonide/formoterol)
[1 puff = 400mcg BDP equiv.] 1 puff bd (£29.97)
OR
DuoResp Spiromax® 160/4.5 (budesonide/formoterol)
[1 puff = 200mcg BDP equiv.] 2 puffs bd (£29.97)
(800mcg BDP* equiv/day + 24mcg formoterol/day)
DuoResp Spiromax® 160/4.5 (budesonide/formoterol)
[1 puff = 200mcg BDP equiv]
1 puff bd (£14.99) (400mcg BDP* equiv./day + 12mcg formoterol/day)
Symbicort Turbohaler® 200/6
(budesonide/formoterol) [1 puff = 200mcg BDP equiv.]
1 puff bd (£19.00) (400mcg BDP* equiv./day + 12mcg formoterol/day)
DuoResp Spiromax® (budesonide/formoterol) is an ENHCCG approved lower cost ICS/LABA fixed dose combination dry powder inhaler (DPI) for asthma and COPD. It is therapeutically equivalent to corresponding strengths of Symbicort Turbohaler®. It is lower cost for patients on Symbicort Turbohaler® (prescribed by brand or generic) to be switched to the equivalent strength DuoResp Spiromax® DPI. PRESCRIBE BY BRAND NAME
All patients with asthma should have an up to date asthma action plan and a short-acting beta2 agonist (salbutamol MDI or Easyhaler®) to aid in the event of an exacerbation.
If patient is at Step 4/5, consider respiratory specialist advice on how to manage step down process, particularly if a more gradual ICS dose reduction (<50%) is required than the combination devices in the above algorithm allow. This may involve using combinations of different inhalers. If under respiratory specialist review - do not attempt step down without agreement of specialist.
Key: If taking add-on therapies e.g.oral
prednisolone, montelukast, consider reducing these before reducing the ICS. * Total daily dose inhaled corticosteroid (ICS), in terms of beclometasone dipropionate (BDP) equivalent Costs: 30 days without a spacer [Sep2016]