Embed Size (px)
Citation preview
CASE REPORT
Adult patient with hemifacial microsomia treatedwith combined orthodontics and distractionosteogenesis
Sung-Hwan Choi,a Da-Young Kang,b and Chung-Ju Hwangc
Seoul, Korea
FromSeoulaPostgbResidcProfeAll autentiaSuppoYonseAddreInstitugu, SeSubm0889-Copyrhttp:/
72
Distraction osteogenesis is an alternative treatment option for patients with facial asymmetry andmandibular hy-poplasia. New bone is formed between bone segment surfaces that are gradually separated by incremental trac-tion. The purpose of this article is to report the treatment of a 22-year-old man with hemifacial microsomia, facialasymmetry, and a skeletal Class II profile. The patient's left mandibular ramus was lengthened with distractionosteogenesis, andminiscrew-assisted rapid palatal expansion was used to correct the maxillary transverse defi-ciency. Postoperative orthodontic treatment achieved tooth alignment and closure of the posterior open bite. Thetotal treatment period was 27 months. These therapeutic treatments improved the patient's facial appearance.(Am J Orthod Dentofacial Orthop 2014;145:72-84)
Hemifacial microsomia is the second mostfrequent form of isolated facial birth disorder,after cleft lip and palate. Hemifacial microsomia
is a congenital skeletal malformation in which there is adeficiency on 1 side of the face; characteristic featuresinclude maxillomandibular hypoplasia and facial asym-metry. It is primarily a syndrome of the first brachialarch, involving underdevelopment of the ear, mandible,maxilla, zygoma, temporal bone, and the associatedmusculature and soft tissues.1 The exact etiology ofhemifacial microsomia has not yet been determined,but laboratory studies suggest that the clinical featuresmight be caused by early loss of neural crest cell-related formation of the first brachial arch.2,3
In adults with hemifacial microsomia, mild skeletaldeformities—such as mandibular hypoplasia and facial
the Department of Orthodontics, College of Dentistry, Yonsei University,, Korea.raduate student.ent.ssor, Institute of Craniofacial Deformity Center.thors have completed and submitted the ICMJE Form for Disclosure of Po-l Conflicts of Interest, and none were reported.rted by the Institute of Craniofacial Deformity Center, College of Dentistry,i University, Seoul, Korea.ss correspondence to: Chung-Ju Hwang, Department of Orthodontics,te of Craniofacial Deformity Center, 134 Shinchon-dong, Seodaemun-oul 120-752, Korea; e-mail, [email protected], revised and accepted, February 2013.5406/$36.00ight � 2014 by the American Association of Orthodontists./dx.doi.org/10.1016/j.ajodo.2013.02.033
asymmetry—have traditionally been treated withbimaxillary surgery,4 whereas autogenous costochon-dral grafting is used for more severe malformations.5
In 1988, Ilizarov6,7 first described distractionosteogenesis, an alternative treatment process inwhich new bone is formed between bone segmentsurfaces that are gradually separated by incrementaltraction. In 1992, McCarthy et al8 used mandibularlengthening by distraction osteogenesis in patientswith hemifacial microsomia. Because of the slowlengthening procedure, the soft tissues adapt gradu-ally; this is advantageous because it minimizes therisk of relapse for hemifacial microsomia patientswho lack both bone and soft tissues.9,10
In this case report, we describe the treatment withthe combination of distraction osteogenesis and ortho-dontics, as well as miniscrew-assisted rapid palatalexpansion, for a man with a skeletal Class II malocclu-sion, hemifacial microsomia, and a maxillary transversedeficiency.
DIAGNOSIS AND ETIOLOGY
A 22-year-old man visited the orthodontic depart-ment at Yonsei University Dental Hospital in Seoul, Ko-rea, with a chief complaint of facial asymmetry. Theclinical and radiographic examination results indicatedthat he had Pruzansky-Kaban type I left hemifacial mi-crosomia with well-formed but small temporomandib-ular joint and ramus. His medical history included a
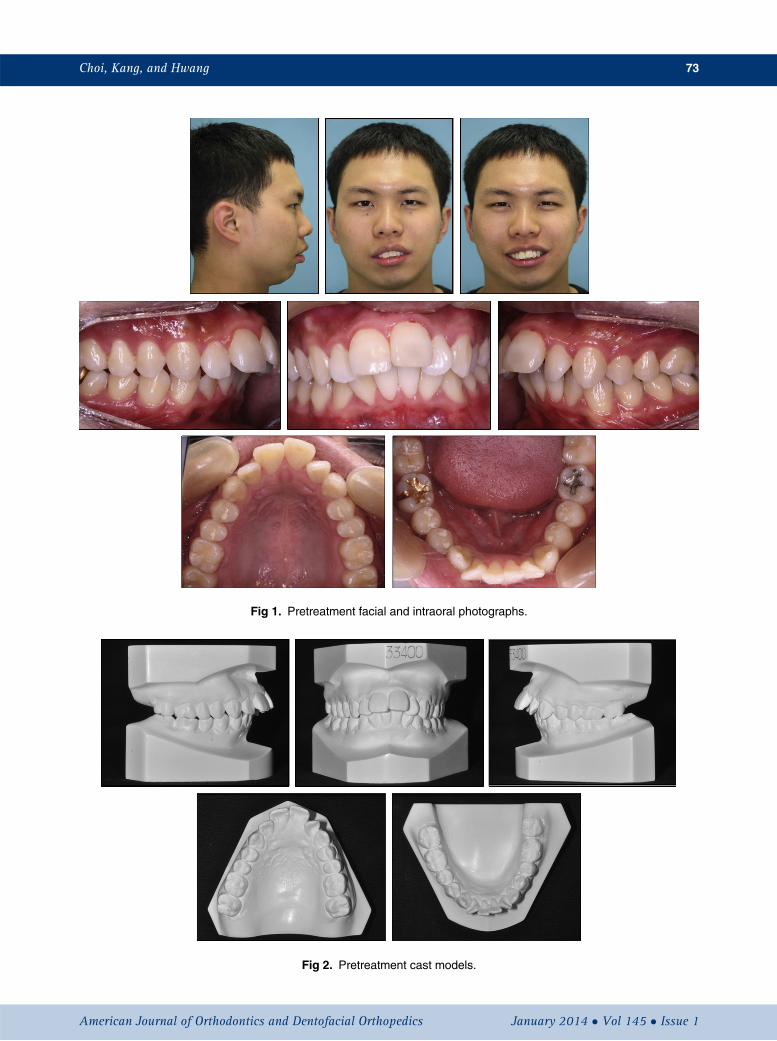
Fig 1. Pretreatment facial and intraoral photographs.
Fig 2. Pretreatment cast models.
Choi, Kang, and Hwang 73
American Journal of Orthodontics and Dentofacial Orthopedics January 2014 � Vol 145 � Issue 1
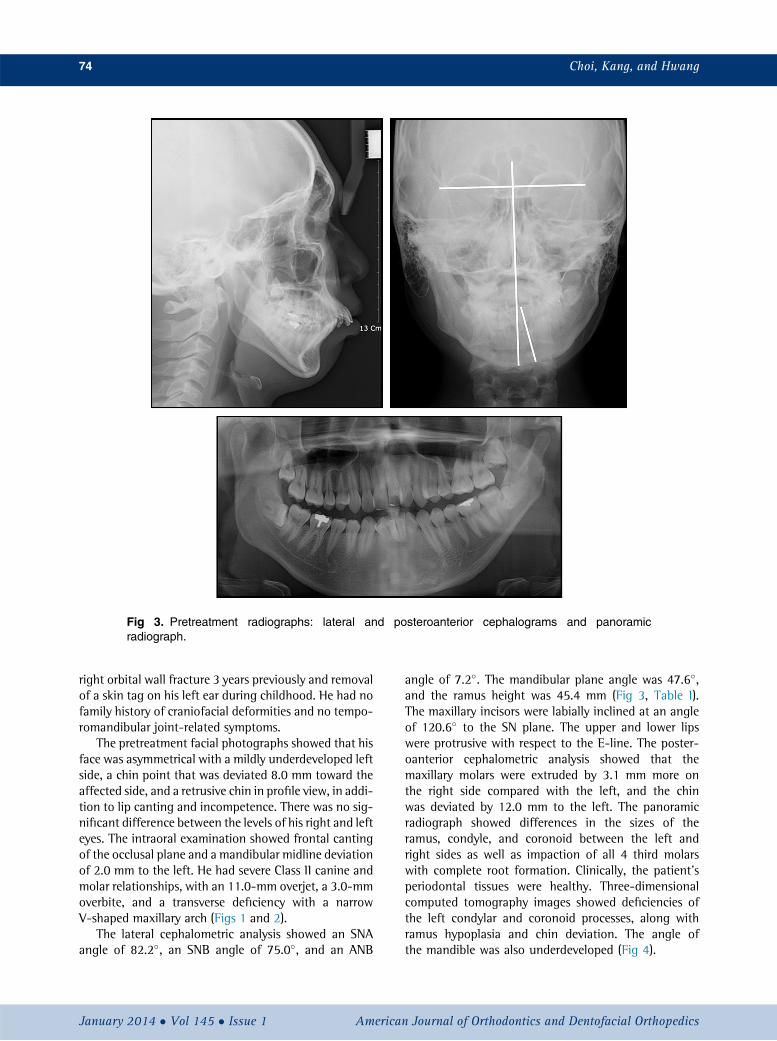
Fig 3. Pretreatment radiographs: lateral and posteroanterior cephalograms and panoramicradiograph.
74 Choi, Kang, and Hwang
right orbital wall fracture 3 years previously and removalof a skin tag on his left ear during childhood. He had nofamily history of craniofacial deformities and no tempo-romandibular joint-related symptoms.
The pretreatment facial photographs showed that hisface was asymmetrical with a mildly underdeveloped leftside, a chin point that was deviated 8.0 mm toward theaffected side, and a retrusive chin in profile view, in addi-tion to lip canting and incompetence. There was no sig-nificant difference between the levels of his right and lefteyes. The intraoral examination showed frontal cantingof the occlusal plane and a mandibular midline deviationof 2.0 mm to the left. He had severe Class II canine andmolar relationships, with an 11.0-mm overjet, a 3.0-mmoverbite, and a transverse deficiency with a narrowV-shaped maxillary arch (Figs 1 and 2).
The lateral cephalometric analysis showed an SNAangle of 82.2�, an SNB angle of 75.0�, and an ANB
January 2014 � Vol 145 � Issue 1 American
angle of 7.2�. The mandibular plane angle was 47.6�,and the ramus height was 45.4 mm (Fig 3, Table I).The maxillary incisors were labially inclined at an angleof 120.6� to the SN plane. The upper and lower lipswere protrusive with respect to the E-line. The poster-oanterior cephalometric analysis showed that themaxillary molars were extruded by 3.1 mm more onthe right side compared with the left, and the chinwas deviated by 12.0 mm to the left. The panoramicradiograph showed differences in the sizes of theramus, condyle, and coronoid between the left andright sides as well as impaction of all 4 third molarswith complete root formation. Clinically, the patient'speriodontal tissues were healthy. Three-dimensionalcomputed tomography images showed deficiencies ofthe left condylar and coronoid processes, along withramus hypoplasia and chin deviation. The angle ofthe mandible was also underdeveloped (Fig 4).
Journal of Orthodontics and Dentofacial Orthopedics
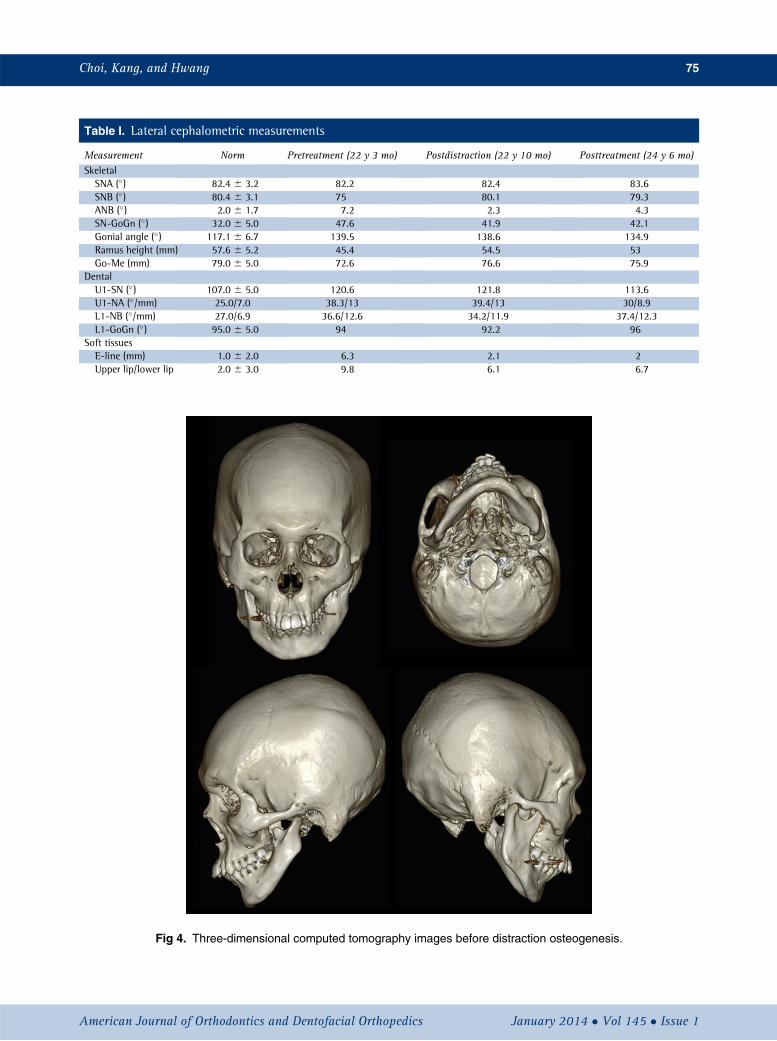
Table I. Lateral cephalometric measurements
Measurement Norm Pretreatment (22 y 3 mo) Postdistraction (22 y 10 mo) Posttreatment (24 y 6 mo)SkeletalSNA (�) 82.4 6 3.2 82.2 82.4 83.6SNB (�) 80.4 6 3.1 75 80.1 79.3ANB (�) 2.0 6 1.7 7.2 2.3 4.3SN-GoGn (�) 32.0 6 5.0 47.6 41.9 42.1Gonial angle (�) 117.1 6 6.7 139.5 138.6 134.9Ramus height (mm) 57.6 6 5.2 45.4 54.5 53Go-Me (mm) 79.0 6 5.0 72.6 76.6 75.9
DentalU1-SN (�) 107.0 6 5.0 120.6 121.8 113.6U1-NA (�/mm) 25.0/7.0 38.3/13 39.4/13 30/8.9L1-NB (�/mm) 27.0/6.9 36.6/12.6 34.2/11.9 37.4/12.3L1-GoGn (�) 95.0 6 5.0 94 92.2 96
Soft tissuesE-line (mm) 1.0 6 2.0 6.3 2.1 2Upper lip/lower lip 2.0 6 3.0 9.8 6.1 6.7
Fig 4. Three-dimensional computed tomography images before distraction osteogenesis.
Choi, Kang, and Hwang 75
American Journal of Orthodontics and Dentofacial Orthopedics January 2014 � Vol 145 � Issue 1
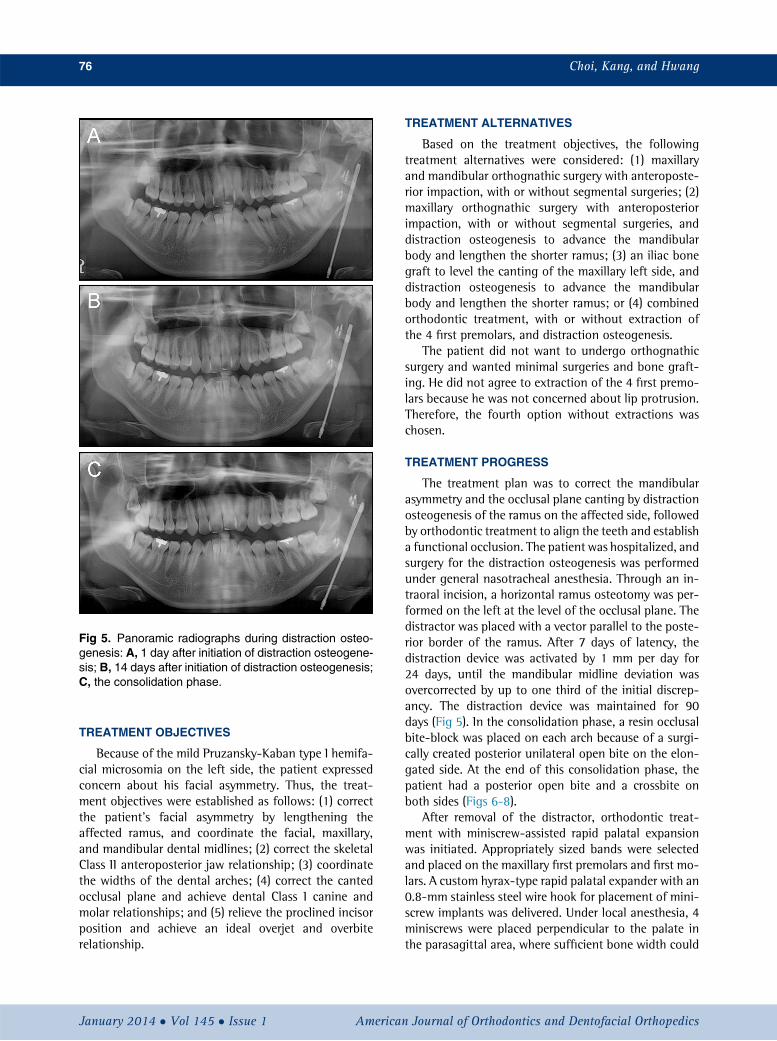
Fig 5. Panoramic radiographs during distraction osteo-genesis: A, 1 day after initiation of distraction osteogene-sis; B, 14 days after initiation of distraction osteogenesis;C, the consolidation phase.
76 Choi, Kang, and Hwang
TREATMENT OBJECTIVES
Because of the mild Pruzansky-Kaban type I hemifa-cial microsomia on the left side, the patient expressedconcern about his facial asymmetry. Thus, the treat-ment objectives were established as follows: (1) correctthe patient's facial asymmetry by lengthening theaffected ramus, and coordinate the facial, maxillary,and mandibular dental midlines; (2) correct the skeletalClass II anteroposterior jaw relationship; (3) coordinatethe widths of the dental arches; (4) correct the cantedocclusal plane and achieve dental Class I canine andmolar relationships; and (5) relieve the proclined incisorposition and achieve an ideal overjet and overbiterelationship.
January 2014 � Vol 145 � Issue 1 American
TREATMENT ALTERNATIVES
Based on the treatment objectives, the followingtreatment alternatives were considered: (1) maxillaryand mandibular orthognathic surgery with anteroposte-rior impaction, with or without segmental surgeries; (2)maxillary orthognathic surgery with anteroposteriorimpaction, with or without segmental surgeries, anddistraction osteogenesis to advance the mandibularbody and lengthen the shorter ramus; (3) an iliac bonegraft to level the canting of the maxillary left side, anddistraction osteogenesis to advance the mandibularbody and lengthen the shorter ramus; or (4) combinedorthodontic treatment, with or without extraction ofthe 4 first premolars, and distraction osteogenesis.
The patient did not want to undergo orthognathicsurgery and wanted minimal surgeries and bone graft-ing. He did not agree to extraction of the 4 first premo-lars because he was not concerned about lip protrusion.Therefore, the fourth option without extractions waschosen.
TREATMENT PROGRESS
The treatment plan was to correct the mandibularasymmetry and the occlusal plane canting by distractionosteogenesis of the ramus on the affected side, followedby orthodontic treatment to align the teeth and establisha functional occlusion. The patient was hospitalized, andsurgery for the distraction osteogenesis was performedunder general nasotracheal anesthesia. Through an in-traoral incision, a horizontal ramus osteotomy was per-formed on the left at the level of the occlusal plane. Thedistractor was placed with a vector parallel to the poste-rior border of the ramus. After 7 days of latency, thedistraction device was activated by 1 mm per day for24 days, until the mandibular midline deviation wasovercorrected by up to one third of the initial discrep-ancy. The distraction device was maintained for 90days (Fig 5). In the consolidation phase, a resin occlusalbite-block was placed on each arch because of a surgi-cally created posterior unilateral open bite on the elon-gated side. At the end of this consolidation phase, thepatient had a posterior open bite and a crossbite onboth sides (Figs 6-8).
After removal of the distractor, orthodontic treat-ment with miniscrew-assisted rapid palatal expansionwas initiated. Appropriately sized bands were selectedand placed on the maxillary first premolars and first mo-lars. A custom hyrax-type rapid palatal expander with an0.8-mm stainless steel wire hook for placement of mini-screw implants was delivered. Under local anesthesia, 4miniscrews were placed perpendicular to the palate inthe parasagittal area, where sufficient bone width could
Journal of Orthodontics and Dentofacial Orthopedics
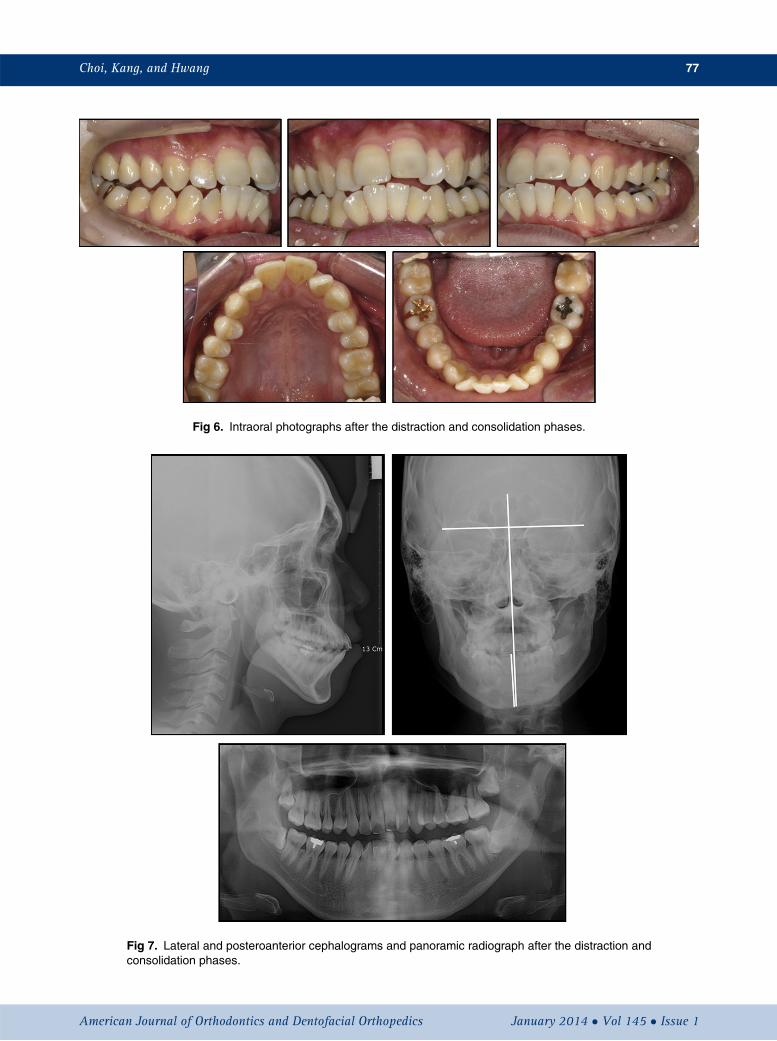
Fig 6. Intraoral photographs after the distraction and consolidation phases.
Fig 7. Lateral and posteroanterior cephalograms and panoramic radiograph after the distraction andconsolidation phases.
Choi, Kang, and Hwang 77
American Journal of Orthodontics and Dentofacial Orthopedics January 2014 � Vol 145 � Issue 1

Fig 8. Superimposition of the 3-dimensional computed tomography images at pretreatment and afterthe consolidation phase.
78 Choi, Kang, and Hwang
be obtained. After miniscrew placement, light-curedresin was used to connect the miniscrew heads andhooks to form a single unit (Fig 9). The appliance wasactivated at 0.25 mm per day. After achieving correctionof the transverse maxillary deficiency, the appliance wasmaintained for 3 months without activation. Afterremoval of the appliance, brackets were placed on themaxillary and mandibular arches for tooth alignmentand correction of the posterior open bite. During fixedorthodontic treatment, vertical elastics were used toclose the posterior open bite (Fig 10).
After 18 months of postdistraction orthodontic treat-ment, the fixed orthodontic appliances were removed(Figs 11-13). The total treatment period lasted 27months. Fixed lingual retainers were bonded to thelingual surfaces of the anterior teeth in both arches.
January 2014 � Vol 145 � Issue 1 American
Maxillary and mandibular circumferential retainerswere delivered with instructions to use them 24 hoursper day for the next 6 months.
RESULTS
The posttreatment photographs and radiographsshowed that facial symmetry and an ideal occlusionwith proper overjet and overbite were achieved. Themandibular dental midline coincided with the facialand maxillary midlines, and the occlusion was finishedto Angle Class I canine and molar relationships. Thepanoramic radiograph showed that new bone withthe same characteristics as adjacent bone was createdon the affected side by gradual separation of the2 bony segments that were surgically severed(Figs 11-13).
Journal of Orthodontics and Dentofacial Orthopedics
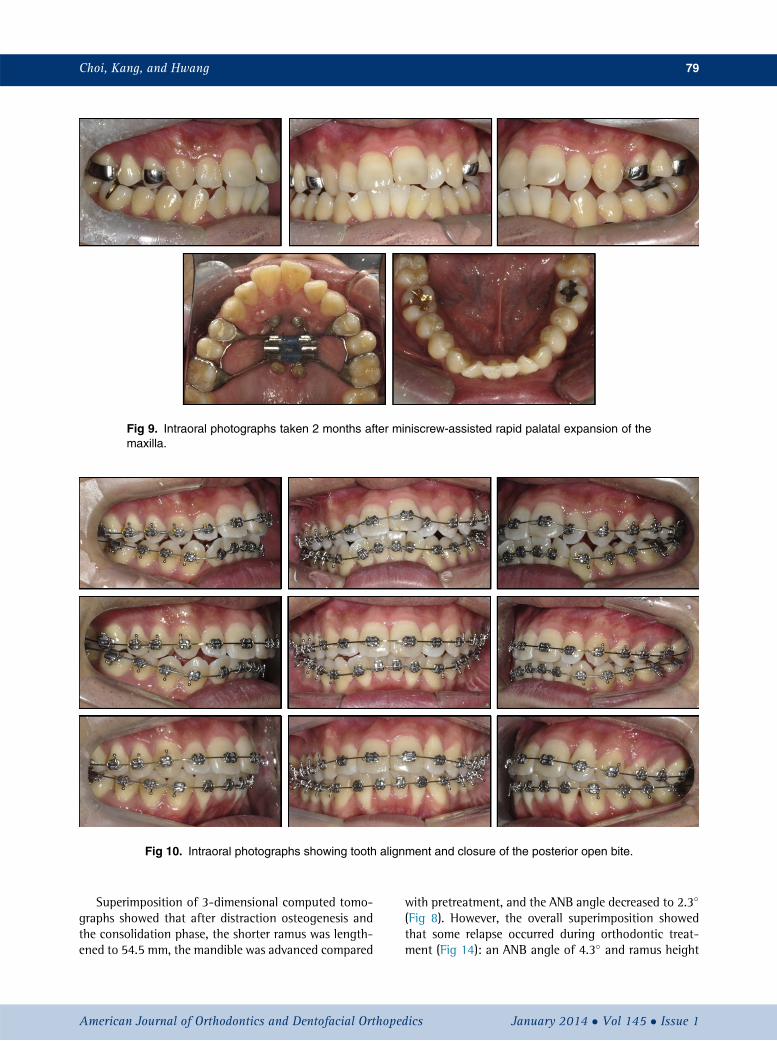
Fig 9. Intraoral photographs taken 2 months after miniscrew-assisted rapid palatal expansion of themaxilla.
Fig 10. Intraoral photographs showing tooth alignment and closure of the posterior open bite.
Choi, Kang, and Hwang 79
Superimposition of 3-dimensional computed tomo-graphs showed that after distraction osteogenesis andthe consolidation phase, the shorter ramus was length-ened to 54.5 mm, the mandible was advanced compared
American Journal of Orthodontics and Dentofacial Orthoped
with pretreatment, and the ANB angle decreased to 2.3�
(Fig 8). However, the overall superimposition showedthat some relapse occurred during orthodontic treat-ment (Fig 14): an ANB angle of 4.3� and ramus height
ics January 2014 � Vol 145 � Issue 1
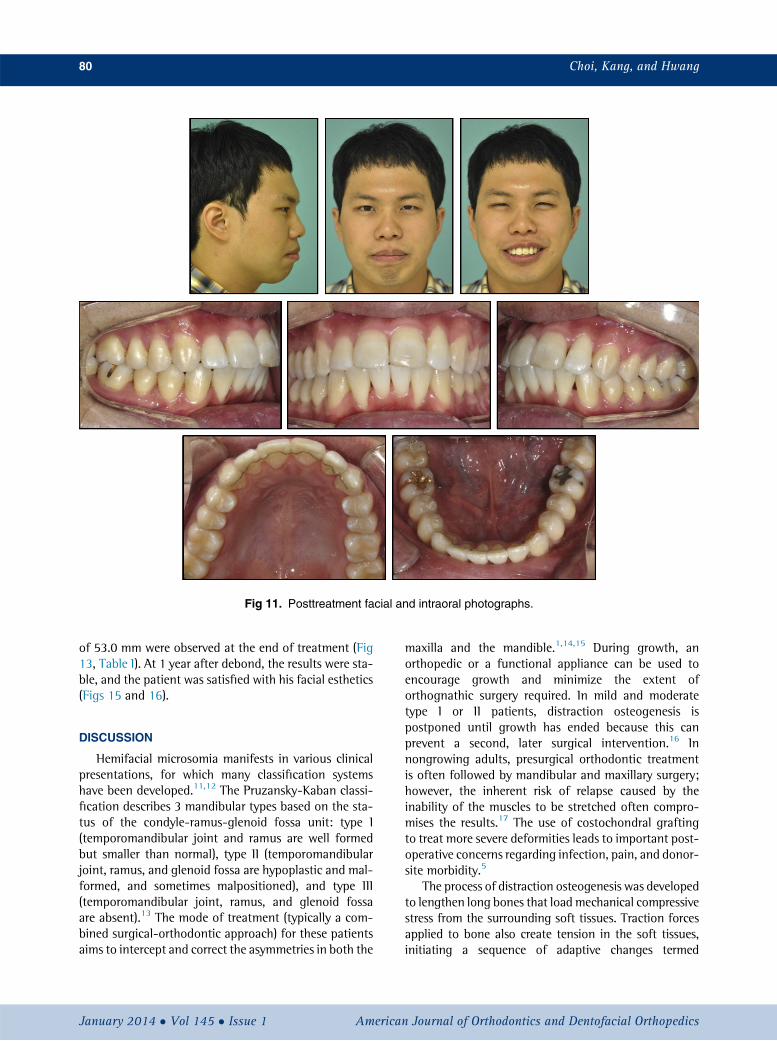
Fig 11. Posttreatment facial and intraoral photographs.
80 Choi, Kang, and Hwang
of 53.0 mm were observed at the end of treatment (Fig13, Table I). At 1 year after debond, the results were sta-ble, and the patient was satisfied with his facial esthetics(Figs 15 and 16).
DISCUSSION
Hemifacial microsomia manifests in various clinicalpresentations, for which many classification systemshave been developed.11,12 The Pruzansky-Kaban classi-fication describes 3 mandibular types based on the sta-tus of the condyle-ramus-glenoid fossa unit: type I(temporomandibular joint and ramus are well formedbut smaller than normal), type II (temporomandibularjoint, ramus, and glenoid fossa are hypoplastic and mal-formed, and sometimes malpositioned), and type III(temporomandibular joint, ramus, and glenoid fossaare absent).13 The mode of treatment (typically a com-bined surgical-orthodontic approach) for these patientsaims to intercept and correct the asymmetries in both the
January 2014 � Vol 145 � Issue 1 American
maxilla and the mandible.1,14,15 During growth, anorthopedic or a functional appliance can be used toencourage growth and minimize the extent oforthognathic surgery required. In mild and moderatetype I or II patients, distraction osteogenesis ispostponed until growth has ended because this canprevent a second, later surgical intervention.16 Innongrowing adults, presurgical orthodontic treatmentis often followed by mandibular and maxillary surgery;however, the inherent risk of relapse caused by theinability of the muscles to be stretched often compro-mises the results.17 The use of costochondral graftingto treat more severe deformities leads to important post-operative concerns regarding infection, pain, and donor-site morbidity.5
The process of distraction osteogenesis was developedto lengthen long bones that load mechanical compressivestress from the surrounding soft tissues. Traction forcesapplied to bone also create tension in the soft tissues,initiating a sequence of adaptive changes termed
Journal of Orthodontics and Dentofacial Orthopedics
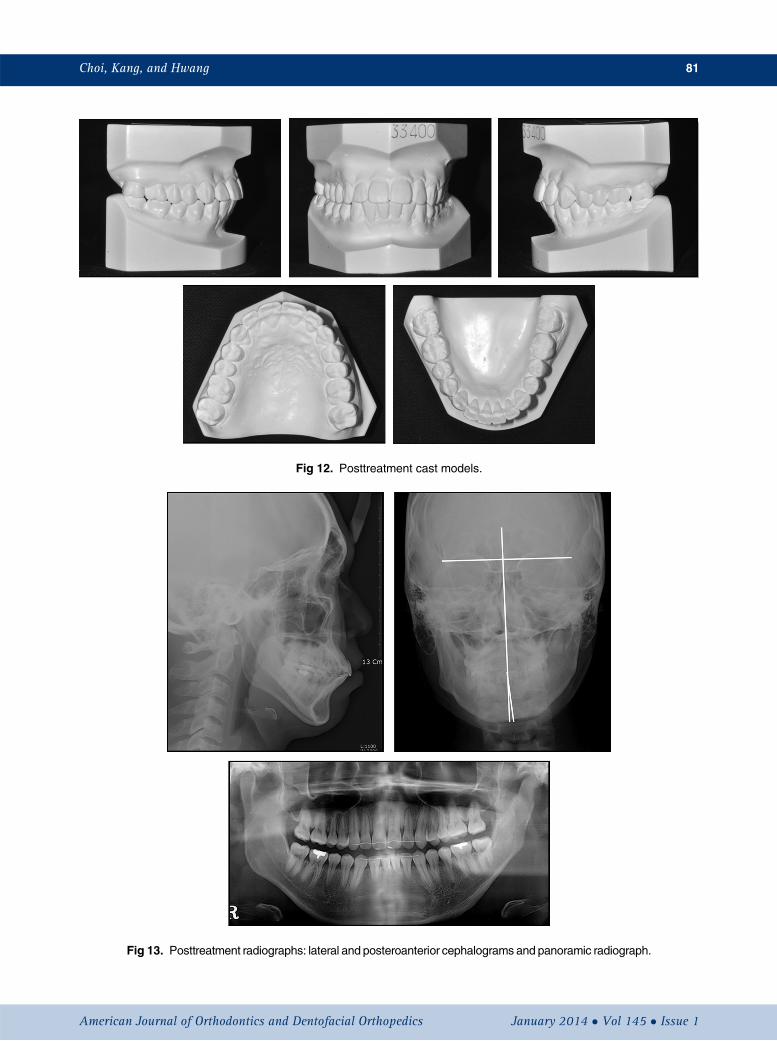
Fig 12. Posttreatment cast models.
Fig 13. Posttreatment radiographs: lateral and posteroanterior cephalograms and panoramic radiograph.
Choi, Kang, and Hwang 81
American Journal of Orthodontics and Dentofacial Orthopedics January 2014 � Vol 145 � Issue 1
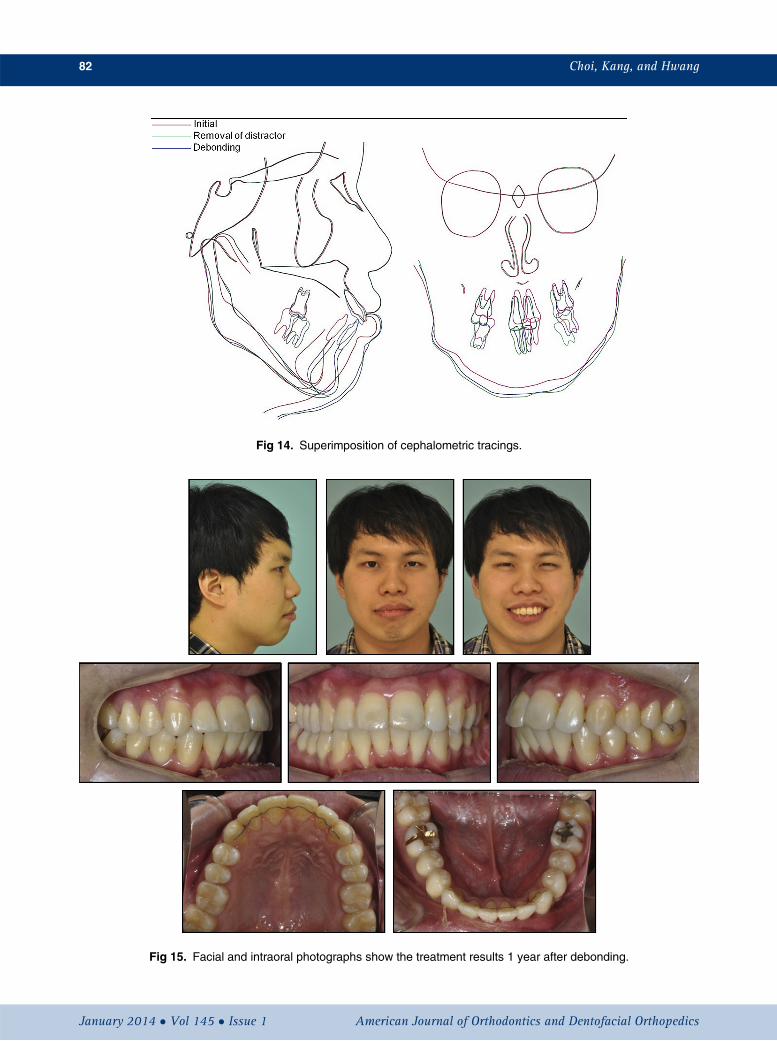
Fig 14. Superimposition of cephalometric tracings.
Fig 15. Facial and intraoral photographs show the treatment results 1 year after debonding.
82 Choi, Kang, and Hwang
January 2014 � Vol 145 � Issue 1 American Journal of Orthodontics and Dentofacial Orthopedics
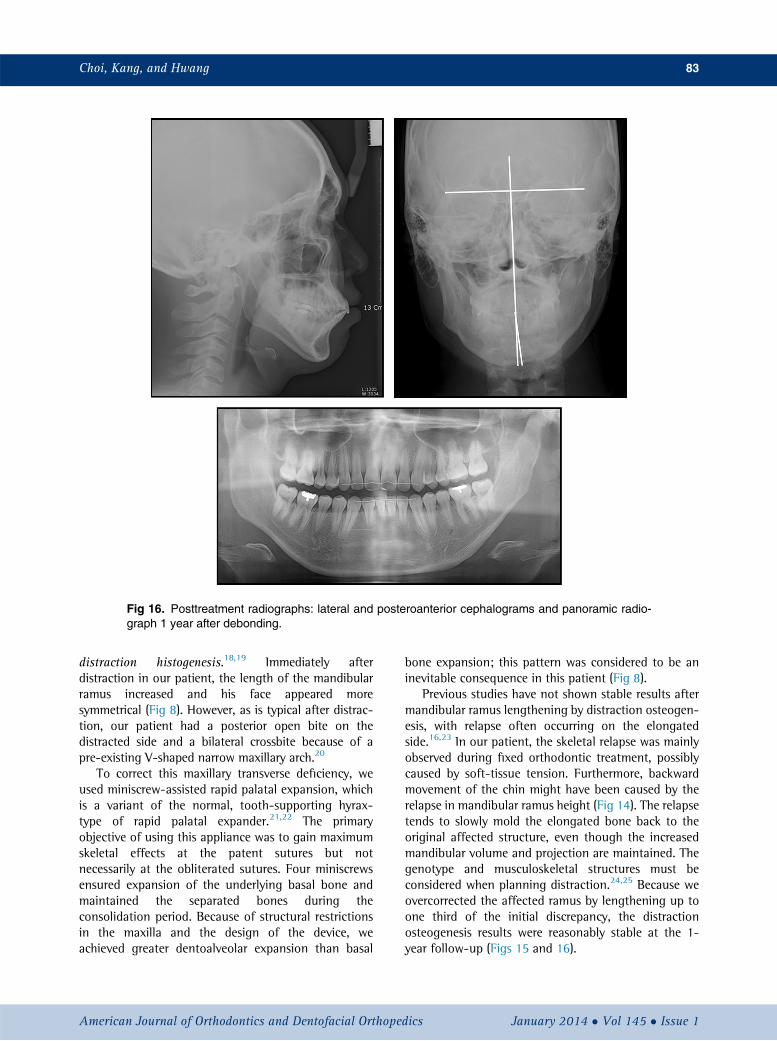
Fig 16. Posttreatment radiographs: lateral and posteroanterior cephalograms and panoramic radio-graph 1 year after debonding.
Choi, Kang, and Hwang 83
distraction histogenesis.18,19 Immediately afterdistraction in our patient, the length of the mandibularramus increased and his face appeared moresymmetrical (Fig 8). However, as is typical after distrac-tion, our patient had a posterior open bite on thedistracted side and a bilateral crossbite because of apre-existing V-shaped narrow maxillary arch.20
To correct this maxillary transverse deficiency, weused miniscrew-assisted rapid palatal expansion, whichis a variant of the normal, tooth-supporting hyrax-type of rapid palatal expander.21,22 The primaryobjective of using this appliance was to gain maximumskeletal effects at the patent sutures but notnecessarily at the obliterated sutures. Four miniscrewsensured expansion of the underlying basal bone andmaintained the separated bones during theconsolidation period. Because of structural restrictionsin the maxilla and the design of the device, weachieved greater dentoalveolar expansion than basal
American Journal of Orthodontics and Dentofacial Orthoped
bone expansion; this pattern was considered to be aninevitable consequence in this patient (Fig 8).
Previous studies have not shown stable results aftermandibular ramus lengthening by distraction osteogen-esis, with relapse often occurring on the elongatedside.16,23 In our patient, the skeletal relapse was mainlyobserved during fixed orthodontic treatment, possiblycaused by soft-tissue tension. Furthermore, backwardmovement of the chin might have been caused by therelapse in mandibular ramus height (Fig 14). The relapsetends to slowly mold the elongated bone back to theoriginal affected structure, even though the increasedmandibular volume and projection are maintained. Thegenotype and musculoskeletal structures must beconsidered when planning distraction.24,25 Because weovercorrected the affected ramus by lengthening up toone third of the initial discrepancy, the distractionosteogenesis results were reasonably stable at the 1-year follow-up (Figs 15 and 16).
ics January 2014 � Vol 145 � Issue 1

84 Choi, Kang, and Hwang
At the end of treatment, the patient's periodontalcondition was not ideal and included labial gingivalrecession and attachment loss of the mandibular lateralincisors (Fig 11); this might have been a result of age,oral hygiene, orthodontic proclination of the mandibularincisors in a patient with a thin gingival biotype, a nar-row zone of keratinized gingiva, or a combination ofthese factors.26-29 The patient chose not to undergomucogingival surgery after the treatment. To reduceplaque and gingival inflammation, he follows a strictoral hygiene program including brushing, rinsing, andprofessional cleaning at regular visits. The influence ofthe width of keratinized gingiva and gingival biotypeon the result of orthodontic treatment makes itadvisable to perform mucogingival surgery beforeorthodontic proclination of the mandibular incisors inat-risk patients.
CONCLUSIONS
Our results demonstrate that the combination ofdistraction osteogenesis and orthodontic treatment isan effective option for an adult with hemifacial microso-mia. The therapeutic results showed improvement of thepatient's facial appearance.
REFERENCES
1. Monahan R, Seder K, Patel P, Alder M, Grud S, O'Gara M. Hemifa-cial microsomia. Etiology, diagnosis and treatment. J Am Dent As-soc 2001;132:1402-8.
2. Johnston MC, Bronsky PT. Animal models for human craniofacialmalformations. J Craniofac Genet Dev Biol 1991;11:277-91.
3. Thomas IT, Frias JL. The heart in selected congenital malforma-tions. A lesson in pathogenetic relationships. Ann Clin Lab Sci1987;17:207-10.
4. Yamashiro T, Takano-Yamamoto T, Takada K. Case report: dento-facial orthopedic and surgical orthodontic treatment in hemifacialmicrosomia. Angle Orthod 1997;67:463-6.
5. Tehranchi A, Behnia H. Treatment of mandibular asymmetry bydistraction osteogenesis and orthodontics: a report of four cases.Angle Orthod 2000;70:165-74.
6. Ilizarov GA. The tension-stress effect on the genesis and growth oftissues. Part I. The influence of stability of fixation and soft-tissuepreservation. Clin Orthop Relat Res 1989;238:249-81.
7. Ilizarov GA. The tension-stress effect on the genesis and growth oftissues: part II. The influence of the rate and frequency of distrac-tion. Clin Orthop Relat Res 1989;239:263-85.
8. McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH.Lengthening the humanmandible by gradual distraction. Plast Re-constr Surg 1992;89:1-8.
9. Swennen G, Schliephake H, Dempf R, Schierle H, Malevez C.Craniofacial distraction osteogenesis: a review of the literature:part 1: clinical studies. Int J Oral Maxillofac Surg 2001;30:89-103.
10. Gosain AK. Plastic Surgery Educational Foundation Data Commit-tee. Distraction osteogenesis of the craniofacial skeleton. Plast Re-constr Surg 2001;107:278-80.
January 2014 � Vol 145 � Issue 1 American
11. Cousley RR. A comparison of two classification systems for hemi-facial microsomia. Br J Oral Maxillofac Surg 1993;31:78-82.
12. David DJ, Mahatumarat C, Cooter RD. Hemifacial microsomia: amultisystem classification. Plast Reconstr Surg 1987;80:525-35.
13. Pruzansky S. Not all dwarfed mandibles are alike. Birth Defects1969;4:120-9.
14. Melsen B, Bjerregaard J, Bundgaard M. The effect of treatmentwith functional appliance on a pathologic growth pattern of thecondyle. Am J Orthod Dentofacial Orthop 1986;90:503-12.
15. Ousterhout DK, Vargervik K. Surgical treatment of the jaw defor-mities in hemifacial microsomia. Aust N Z J Surg 1987;57:77-87.
16. Iseri H, Kisnisci R, Altug-Atac AT. Ten-year follow-up of a patientwith hemifacial microsomia treated with distraction osteogenesisand orthodontics: an implant analysis. Am J Orthod DentofacialOrthop 2008;134:296-304.
17. Schendel SA, Epker BN. Results after mandibular advancementsurgery: an analysis of 87 cases. J Oral Surg 1980;38:265-82.
18. Stewart KJ, Lvoff GO, White SA, Bonar SF, Walsh WR, Smart RC,et al. Mandibular distraction osteogenesis: a comparison ofdistraction rates in the rabbit model. J Craniomaxillofac Surg1998;26:43-9.
19. Triaca A, Minoretti R, Merz BR. Distraction osteogenesis of themandibular angle and inferior border to produce facial symmetry:case report. J Oral Maxillofac Surg 2000;58:1051-5.
20. Amm EW. Three-year follow-up of a patient with hemifacial mi-crosomia treated with distraction osteogenesis, temporaryanchorage devices, and orthodontics. Am J Orthod Dentofacial Or-thop 2012;142:115-28.
21. Lee KJ, Park YC, Park JY, Hwang WS. Miniscrew-assisted nonsur-gical palatal expansion before orthognathic surgery for a patientwith severe mandibular prognathism. Am J Orthod Dentofacial Or-thop 2010;137:830-9.
22. Choi SH, Cha JY, Kang DY, Hwang CJ. Surgical-orthodontic treat-ment for skeletal class II malocclusion with vertical maxillaryexcess, anterior open bite, and transverse maxillary deficiency. JCraniofac Surg 2012;23:e531-5.
23. Marquez IM, Fish LC, Stella JP. Two-year follow-up of distrac-tion osteogenesis: its effect on mandibular ramus height in hem-ifacial microsomia. Am J Orthod Dentofacial Orthop 2000;117:130-9.
24. Stelnicki EJ, Lin WY, Lee C, Grayson BH, McCarthy JG. Long-termoutcome study of bilateral mandibular distraction: a comparisonof Treacher Collins and Nager syndromes to other types of micro-gnathia. Plast Reconstr Surg 2002;109:1819-25.
25. Hopper RA, Altug AT, Grayson BH, Barillas I, Sato Y, Cutting CB,et al. Cephalometric analysis of the consolidation phase followingbilateral pediatric mandibular distraction. Cleft Palate Craniofac J2003;40:233-40.
26. Djeu G, Hayes C, Zawaideh S. Correlation between mandibularcentral incisor proclination and gingival recession during fixedappliance therapy. Angle Orthod 2002;72:238-45.
27. Melsen B, Allais D. Factors of importance for the development ofdehiscences during labial movement of mandibular incisors: aretrospective study of adult orthodontic patients. Am J OrthodDentofacial Orthop 2005;127:552-61.
28. Dorfman HS. Mucogingival changes resulting from mandibularincisor tooth movement. Am J Orthod 1978;74:286-97.
29. Coatoam GW, Behrents RG, Bissada NF. The width of keratinizedgingiva during orthodontic treatment: its significance and impacton periodontal status. J Periodontol 1981;52:307-13.
Journal of Orthodontics and Dentofacial Orthopedics









![CaseReport …[8] E.M.Ongkosuwito,J.vanVooren,J.W.vanNecketal., “Changes of mandibular ramal height, during growth in unilateral hemifacial microsomia patients and unaected](https://img.pdfslide.us/doc/110x75/60c4829f23e96b545e31e549/casereport-8-emongkosuwitojvanvoorenjwvannecketal-aoechanges-of-mandibular.jpg)