Embed Size (px)
Citation preview
/. ChiUl PsychoL Psychiat. Vol. 35, No. 7, pp. 1309-1319, 1994Elsevier Science Ltd
© 1994 .Association tor Child Psycholog>- and PsychiatryPrinted in Great Britain. All rights reserved
0021-9630/94 $7.00 + 0.00
0021-9630(94)00075-1
Adult Outcomes of Childhood andAdolescent Depression. Ill Links with
Suicidal Behaviours
Richard Harrington,* Diana Bredenkamp,tChristine Groothues,t Michael Rutter,t Hazel Fudget and
Andrew Picklest
Abstract—This study followed up into adulthood a group of child psychiatric patientssuffering from depressive disorders and a closely matched nondepressed child psychiatriccontrol group. Depression in childhood was a strong predictor of attempted suicide inadulthood. This predictive power was not due to the association between childhooddepression and other childhood risk factors such as conduct disorder or suicidality.Rather, it seemed mostly to reside in the association between depression in childhoodand major depression in adult life. These findings suggest that the pathways fromchildhood psychopathology to adult outcomes can be complex, and depend cruciallyon what happens later.
Keywords: Depression, conduct, child, adult, suicide
Introduction
Over the past 15 years there has been increasing recognition that depressivedisorders among children and adolescents constitute an important, and possiblygrowing (Ryan et al, 1992), public health problem. They tend to be recurrent(Harrington, 1992; Lewinsohn, Hops, Roberts, Seeley &: Andrews, 1993), they areassociated with much impairment of psychosocial functioning (Fleming, Boyle &:Offord, 1993; Puig-Antich et al, 1985) and, at least in clinical samples, they aredifficult to treat (Harrington, 1994).
The public health importance of depressive disorders among the young is furtherunderlined by the links with suicidal behaviours. Several studies have shown that
Accepted manuscript received 23 May 1994
*Royal Manchester Children's Hospital.tMRC Child Psychiatry Unit, Institute of Psychiatry, Camberwell, London SE5 8AF.Requests for reprints to: Professor Harrington, Department of Child and Adolescent Psychiatry, RoyalManchester Children's Hospital, Pendlebury, Manchester M27 lHA, U.K.
1309
1310 R. Harrington et al.
looking forwards, depressed young people are at increased risk of suicidality. Forinstance, Myers, McCauley, Calderon 8c Treder (1991) found that suicidality wasexpressed by around 70% of adolescents with major depression during a 3-yearlongitudinal study. Kovacs, Goldston and Gatsonis (1993) reported that around85% of children or adolescents with major depression and/or dysthymia had alifetime history of suicidal ideation and 32% had attempted suicide. In an importantpaper, Rao, Weissman, Martin and Hammond (1993) described preliminary findingsfrom their adult follow-up of children and adolescents with major depressivedisorders who had been systematically studied by Puig-Antich and his colleaguesmore than 10 years before (Puig-Antich et al, 1985; 1987; 1989). Seven out of the159 subjects who were successfully traced had committed suicide. This risk was farin excess of that found in the general population of young adults, and was significantlygreater than the risk for nondepressed psychiatric controls.
A similarly strong relationship between depression and suicidal behavioursamong the young has been found looking backwards. Thus, several psychologicalautopsy studies of adolescents who have killed themselves have found prevalencesof affective disorders in the range 51-61% (Marttunen, Aro 8c Lonnq\ist, 1993).Most (Andrews 8c Lewinsohn, 1992; Spirito, Brown, Overholser 8c Fritz, 1989; Taylor8c Stansfield, 1984), but not all (Hawton 8c Fagg, 1992) studies of adolescent suicideattempters have found high rates of depressive disorder.
Interpretation of the relationship between depression and suicidal behavioursamong the young is however complicated by a number of issues (Harrington 8cDyer, 1993). Amongst the most important is comorbidity. Virtually all studies ofearly-onset depressive conditions have found that these disorders very frequentlyoccur in conjunction with other kinds of psychiatric problems, especially anxietyand conduct disorders (Harrington, 1993). Similarly, studies of both completed(Marttunen et al, 1993) and attempted suicide (Spirito et al, 1989) among theyoung have found that there is a considerable association with nondepressivedisorders such as antisocial behaviours and drug or alcohol use. For instance, therate of behavioural problems among adolescents who have completed suicide hasbeen found in several studies to exceed 50% (Marttunen et al, 1993). There isalso an association between suicide and personality disorder in adult life (Hawton,1992).
The question therefore, arises as to whether the increased risk of subsequentsuicidal behaviour in depressed young people is mainly a function of the earlierdepression, or whether this risk is better understood as arising from the conditionsthat are frequently associated with the depression, such as behavioural problems,poor interpersonal relationships, or anxiety. This question is important becauseuntil we know which risk factors best predict subsequent suicidal behaviours it willbe difficult to target preventative interventions effectively.
Another important issue concerns the extent to which the risk for suicidalitylater in life is "driven" by the earlier risk factors (e.g. depression or conduct disorder)or by risk factors that are more proximal to the suicidal event. For instance, doesthe elevated risk for subsequent suicidality that seems to be associated with earlydepression stem directly from that depression, or does it stem from factors inadulthood that early depression predicts?
Childhood Depression and Suicidal Behaviours in Adulthood 1311
The Maudsley child-to-adult follow-up of children and adolescents with depressivedisorders (Harrington, Fudge, Rutter, Pickles 8c Hill, 1990) provides a goodopportunity to tackle these issues since (1) it utilized a design that matched carefullyfor the presence of nondepressive symptomatology in childhood; and (2) it collecteddata on a wide range of psychiatric and social problems in adulthood.
This paper therefore, examines the following questions: (1) is depression inyoung people associated with an increased risk of suicidality in adulthood?; (2) ifit is, how much does this increased risk stem from the early depression and howmuch from psychiatric disorder in adulthood?
Subjects and Methods
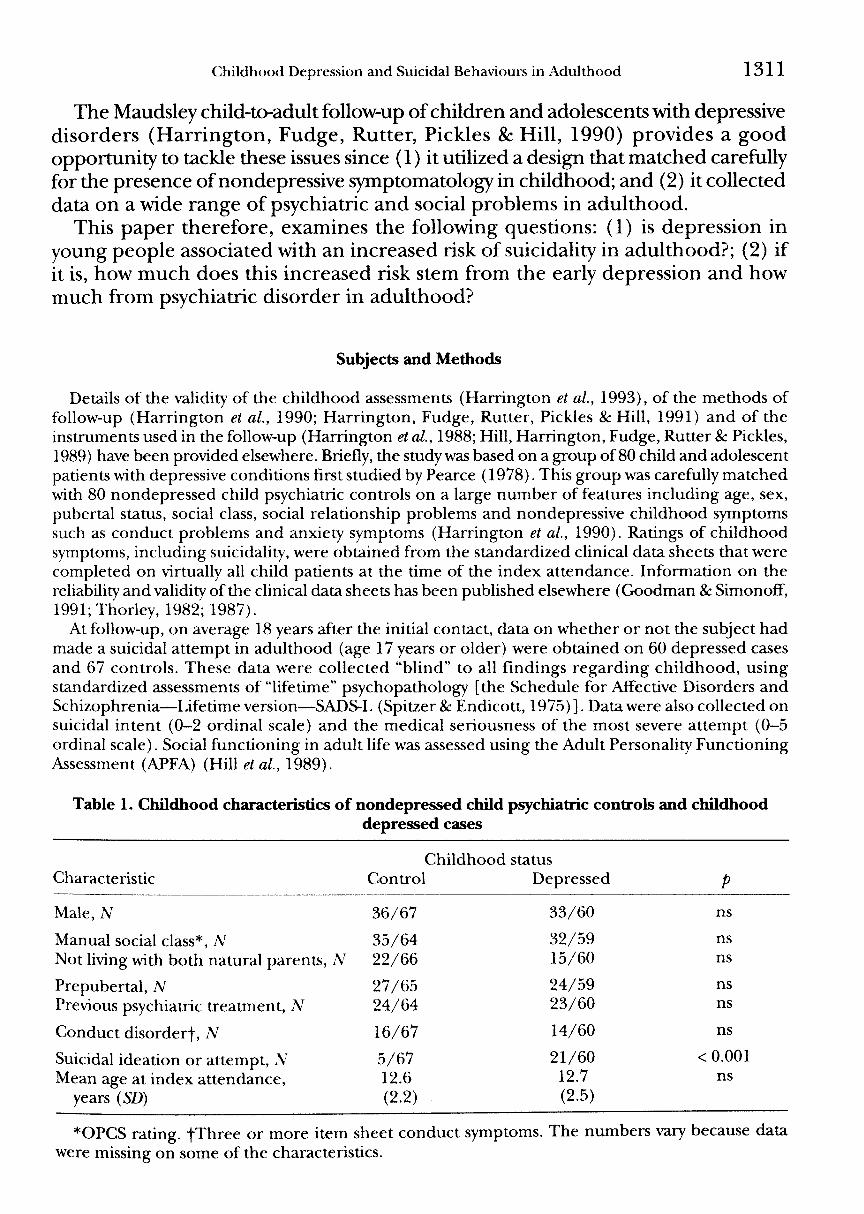
Details of the validity of the childhood assessments (Harrington et al., 1993), of the methods offollow-up (Harrington et al., 1990; Harrington, Fudge, Rutter, Pickles & Hill, 1991) and of theinstruments used in the follow-up (Harrington et al, 1988; Hill, Harrington, Fudge, Rutter & Pickles,1989) have been provided elsewhere. Briefly, the study was based on a group of 80 child and adolescentpatients with depressive conditions first studied by Pearce (1978). This group was carefully matchedwith 80 nondepressed child psychiatric controls on a large number of features including age, sex,pubertal status, social class, social relationship problems and nondepressive childhood symptomssuch as conduct problems and anxiety symptoms (Harrington et al, 1990). Ratings of childhoodsymptoms, including suicidality, were obtained from the standardized clinical data sheets that werecompleted on virtually all child patients at the time of the index attendance. Information on thereliability and validity of the clinical data sheets has been published elsewhere (Goodman & Simonoff",1991; Thorley, 1982; 1987).
At follow-up, on average 18 years after the initial contact, data on whether or not the subject hadmade a suicidal attempt in adulthood (age 17 years or older) were obtained on 60 depressed casesand 67 controls. These data were collected "blind" to all findings regarding childhood, usingstandardized assessments of "lifetime" psychopathology [the Schedule for Affective Disorders andSchizophrenia—Lifetime version—SADS-L (Spitzer & Endicott, 1975)]. Data were also collected onsuicidal intent (0-2 ordinal scale) and the medical seriousness of the most severe attempt (0-5ordinal scale). Social functioning in adult life was assessed using the Adult Personality FunctioningAssessment (APFA) (Hill etal, 1989).
Table L Childhood characteristics of nondepressed cMld psychiatric controls and childhooddepressed cases
Characteristic
Male, N
Manual social class*. A'Not living with both natural parents, N
Prepubertal, NPrevious psychiatric treatment. A"
Conduct disorder!, N
Suicidal ideation or attempt, .VMean age at index attendance,
years {SD)
ChildhoodControl
36/67
35/6422/66
27/6524/64
16/67
5/6712.6(2.2)
statusDepressed
33/60
32/5915/60
24/5923/60
14/60
21/6012.7(2.5)
Pns
nsns
nsns
ns
< 0.001ns
*OPCS rating. fThree or more item sheet conduct symptoms. The numbers vary because datawere missing on some of the characteristics.
1312 R. Harrington et al.
Table 1 shows the childhood characteristics of the subjects. The groups were well matched on allmajor childhood demographic variables. As expected, depression in childhood was significantlyassociated with suicidality (suicidal ideation or a suicidal attempt). The childhood depressed groupwas a little older than the nondepressed child psychiatric controls at the time of follow-up (meanages 31.4 years (SD3.0) and 30.2 years (SD3.0) respectively, (f = 2.2, df= 125, /?= 0.03).
Statistical methods
Contingency tables and y^ tests were used to calculate the significance of differences betweenrates of problems over the follow-up period. Survival models were not used because the duration offollow-up was similar in the childhood depressed and control groups and because such models maybe inaccurate if there have been secular changes in risk, as may have occurred in early-onset affectivephenomena such as depressive disorders and suicidal behaviour (Fombonne, 1993).
Analysis of possible risk factors for an attempt in adulthood was conducted in a series of steps(Schlesselman, 1982). First, we evaluated the effects of these factors one at a time and calculatedsimple odds ratios and their 95% confidence intervals (CI). Next, we investigated whether thepresence or absence of the major associations continued to appear when adjustment was made forother variables in 3-way contingency tables. Subsequently, the effects of the most important riskfactors as predictors of a suicidal attempt in adult life were examined simultaneously in a logisticregression model, obtained using GLIM (Baker & Nelder, 1978).
Results
Depression in childhood
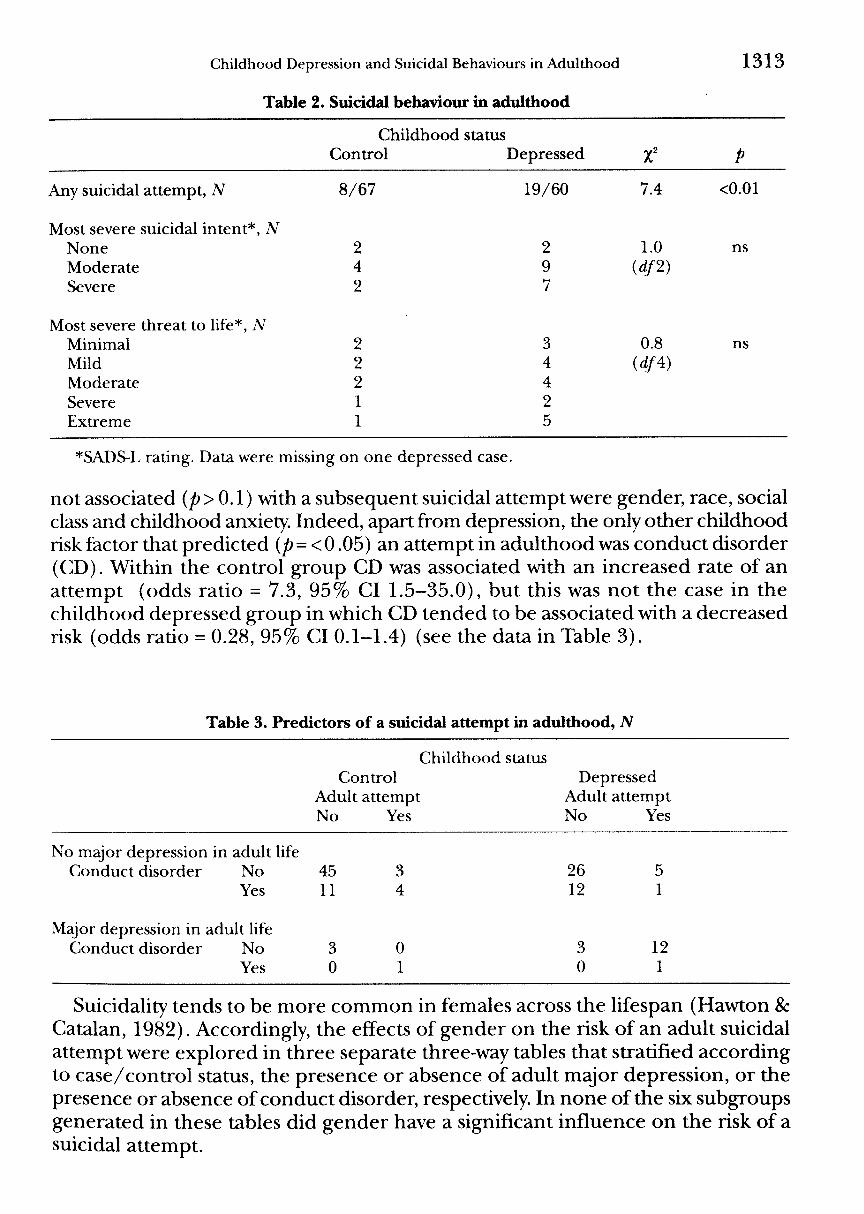
Nineteen (32%) of the 60 childhood depressed cases attempted suicide at leastonce during adulthood, and 12 of these 19 cases (63%) made at least one furtherattempt. The risk of a suicide attempt in adulthood was significantly lower in thecontrol group (8/67 or 12%; see Table 2), although the repetition rate in thecontrol group during the remainder of the follow-up (5/8 or 62%) was similar tothat in the childhood depressed group.
Within the depressed group who had made an attempt in adulthood, nearly90% had made at least one attempt of "moderate" suicidal intent, and more thana third had made an attempt of which the intent was judged to be "severe" (i.e.characterized by such features as using a method that was perceived as dangerous,careful planning, leaving a note, and so on). Five of the depressed group had madeat least one attempt with "extreme" threat to life. Of these, two had died (a verdictof suicide was returned by the coroner in both cases) and three required intensivemedical intervention. Within the control group, just one case made an attemptwith extreme threat to life (who died, verdict suicide). Although this case had notbeen depressed during the index episode, it is probably relevant that she developeda severe bipolar illness shortly after her initial presentation.
Other childhood risk factors
In addition to childhood case-control status, several other childhood risk factorsfor an attempt in adulthood were examined. Suicidal children tended to have ahigher rate of a suicidal attempt in adulthood than nonsuicidal children (9/26 or35%, vs 18/101 or 18%, respectively, x' = 3.5, df= \,p= 0.06). Factors that were
Childhood Depression and Suicidal Behaviours in Adulthood
Table 2. Suicidal behaviour in adulthood
1313
Childhood statusControl Depressed
Any suicidal attempt, N 8/67
Most severe suicidal intent*, ANoneModerateSevere
Most severe threat to life*, NMinimalMildModerateSevereExtreme
242
22211
19/60
297
3442
7.4
1.0(rf/2)
0.8idf4)
<0.01
ns
ns
*SADS-L rating. Data were missing on one depressed case.
not associated {p>0.1) with a subsequent suicidal attempt were gender, race, socialclass and childhood anxiety. Indeed, apart from depression, the only other childhoodrisk factor that predicted (/?= <0.05) an attempt in adulthood was conduct disorder(CD). Within the control group CD was associated with an increased rate of anattempt (odds ratio = 7.3, 95% CI 1.5-35.0), but this was not the case in thechildhood depressed group in which CD tended to be associated with a decreasedrisk (odds ratio = 0.28, 95% CI 0.1-1.4) (see the data in Table 3).
Table 3. Predictors of a suicidal attempt in adulthood, N
No major depression in adult lifeConduct disorder No
Yes
Major depression in adult lifeConduct disorder No
Yes
Childhood statusControl
Adult attemptNo Yes
4511
30
34
01
DepressedAdult attemptNo Yes
26 512 1
3 120 1
Suicidality tends to be more common in females across the lifespan (Hawton 8cCatalan, 1982). Accordingly, the effects of gender on the risk of an adult suicidalattempt were explored in three separate three-way tables that stratified accordingto case/control status, the presence or absence of adult major depression, or thepresence or absence of conduct disorder, respectively. In none of the six subgroupsgenerated in these tables did gender have a significant influence on the risk of asuicidal attempt.
1314 R. Harrington et al
A similar set of analyses was conducted to establish whether suicidality inchildhood, which the 2 x 2 table suggested was a surprisingly weak predictor ofsuicidality in adulthood, would be a stronger predictor in one of these subgroups.In none of the six subgroups generated in these tables did childhood suicidalityhave a significant infiuence on the risk of a suicide attempt.
Risk factors in adulthood
Were there any risk factors in adulthood that infiuenced the risk of a suicidalattempt? Table 3 shows that within the childhood depressed group major depressionin adulthood was very strongly associated with a suicidal attempt in adult life (oddsratio = 27.4, 95% CI 6.0-125.8). Of course, the strength of this relationship willbe infiated by the fact that a suicidal attempt is actually one of the criteria for majordepression. However, such an artifact cannot explain the finding that the singlesymptom of depression (the SADS-L screening question, "depressed mood for2 weeks") was also strongly associated with a suicidal attempt. Thus, for instance,within the childhood depressed group "depressed mood for 2 weeks" after the ageof 17 years was strongly associated with a suicidal attempt during the same ageperiod (odds ratio = 12.7, 95% CI 1.5-104.9).
Persistent difficulties in the APFA domain "work" [a rating of "3" or more (Hillet al, 1989) ] were also associated with an attempt in adulthood, although the effectwas relatively weak and only just reached statistical significance (odds ratio = 2.9,95% CI 1.2-7.0). Factors that were not significantly related to an attempt inadulthood included marital problems, anxiety disorder, antisocial personalitydisorder, a criminal conviction, alcohol abuse, and drug abuse.
Predictors of a suicidal attempt in adult life
It seemed, then, that there were risk factors in both childhood and adult lifethat were associated with a suicidal attempt in adulthood. The strongest risk factorin childhood was depression. Because depression in childhood was a strong predictorof major depression in adulthood and because major depression in adulthood wasstrongly associated with an adult attempt (Table 3), it would seem likely that thepredictive power of childhood depression resided to a large extent in its power topredict depression in adulthood. There was, however, some evidence that depressionin childhood also made an independent contribution to the risk of an attempt inadulthood. Thus, within the group who had had an episode of major depressionin adulthood (A = 20), subjects with depression in childhood tended to have ahigher risk of a suicidal attempt (13/16 or 81%) than subjects who had not beendepressed as children (1/4 or 25%). However, within the group who had not hadan episode of major depression in adulthood (A = 107), subjects with depressionin childhood had a risk of an attempt in adulthood (6/44 or 14%) that was nodifferent from subjects who had not been depressed as children (7/'63 or 11%).
These impressions from three dimensional contingency tables were tested in alogistic regression analysis in which the effects of the two significant childhoodrisk factors (depression and conduct disorder, plus their interaction) and the main
Cjhildhood Depression and Suicidal Behaviours in Adulthood 1315
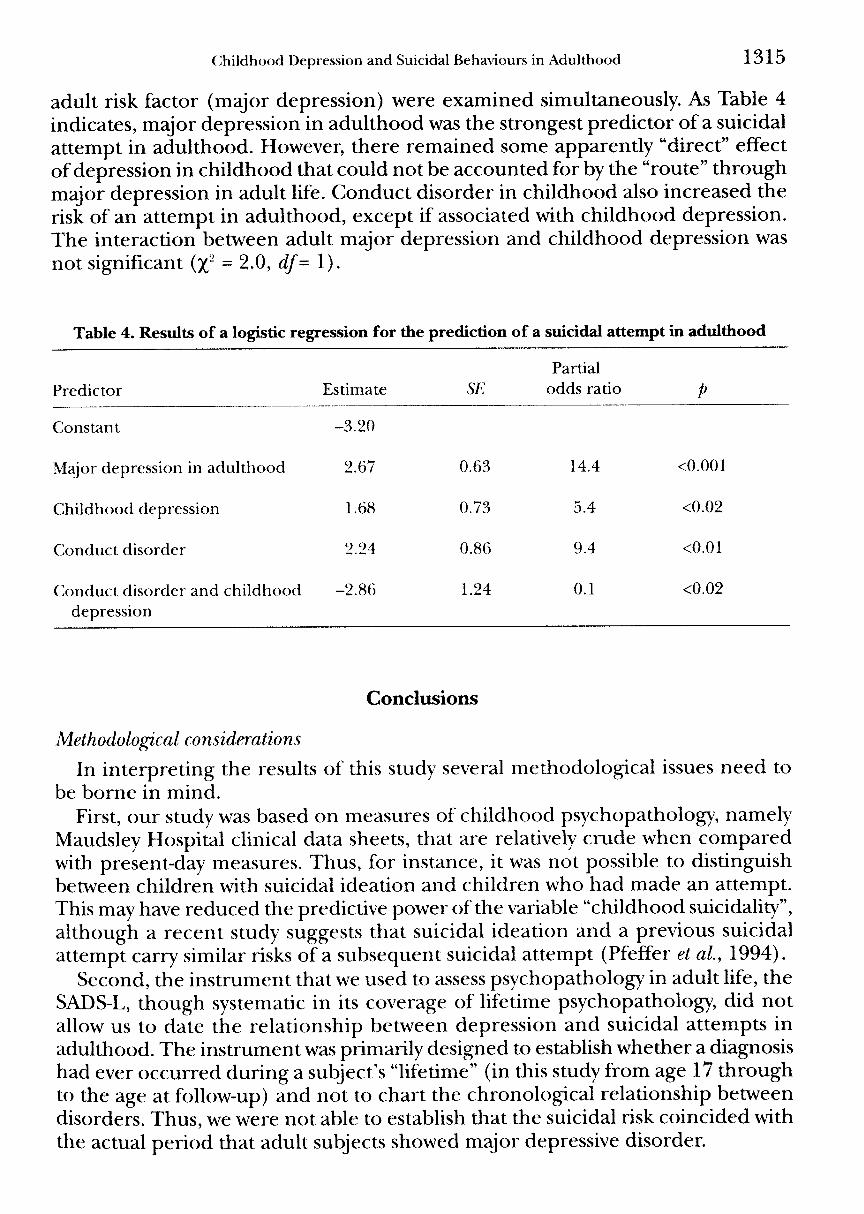
adult risk factor (major depression) were examined simultaneously. As Table 4indicates, major depression in adulthood was the strongest predictor of a suicidalattempt in adulthood. However, there remained some apparently "direct" effectof depression in childhood that could not be accounted for by the "route" throughmajor depression in adult life. Conduct disorder in childhood also increased therisk of an attempt in adulthood, except if associated with childhood depression.The interaction between adult major depression and childhood depression wasnot significant {y; = 2.0, df= 1).
Table 4. Results of a logistic regression for the prediction of a suicidal attempt in adulthood
Predictor
Constant
Major depression in adulthood
Childhood depression
Conduct disorder
Conduct disorder and childhooddepression
Estimate
-3.20
2.67
1.68
2.24
-2.86
SE
0.63
0.73
0.86
1.24
Partialodds ratio
14.4
5.4
9.4
0.1
P
<0.001
<0.02
<0.01
<0.02
Conclusions
Methodological considerations
In interpreting the results of this study several methodological issues need tobe borne in mind.
First, our study was based on measures of childhood psychopatholog)', namelyMaudsley Hospital clinical data sheets, that are relatively crude when comparedwith present-day measures. Thus, for instance, it was not possible to distinguishbetween children with suicidal ideation and children who had made an attempt.This may have reduced the predictive power of the variable "childhood suicidality",although a recent study suggests that suicidal ideation and a previous suicidalattempt carry similar risks of a subsequent suicidal attempt (Pfeffer et al, 1994).
Second, the instrument that we used to assess psychopathology in adult life, theSADS-L, though systematic in its coverage of lifetime psychopathology, did notallow us to date the relationship between depression and suicidal attempts inadulthood. The instrument was primarily designed to establish whether a diagnosishad ever occurred during a subject's "lifetime" (in this study from age 17 throughto the age at follow-up) and not to chart the chronological relationship betweendisorders. Thus, we were not able to establish that the suicidal risk coincided withthe actual period that adult subjects showed major depressive disorder.

1316 R. Harrington et al.
Predictors of a suicidal attempt in adulthood
Nevertheless, the findings of our study support the results of previous longitudinalstudies of depressed children and adolescents (Kovacs et al, 1993; Myers et al,1991; Rao et al, 1993) in showing that there is a strong association with subsequentsuicidal behaviour. The finding that childhood depression predicted adult suicidalattempts even when the effects of many other childhood variables were controlledby the case—control design, suggests that this risk is specifically linked to depression.It is not the result of the overlap of depression in childhood and other childhooddifficulties, such as problems of interpersonal relationships, suicidality or behaviouraldisturbances. It is the depressive disorder in childhood per se that creates the risk.
It is notable however that major depression in adult life was a stronger predictorof a suicidal attempt in adulthood than depression in childhood. This findinghighlights the fact that the pathways from childhood psychopathology to adultoutcomes are often complex, and depend crucially on what happens later. Wehave shown in a previous publication from this study that depression in childhoodwas a strong and specific predictor of depression in adult life (Harrington et al,1990). So, it seems likely that the risk for a suicidal attempt in adulthood thatstemmed from childhood depression depended for the most part on its associationwith depressive disorder in adulthood.
Depression and conduct disorder
It was also evident that other risk factors infiuenced the risk of a suicidal attemptin adulthood, particularly conduct disorder. This finding is consistent with theresults of numerous studies documenting an association between behaviouraldisorders and attempted suicide among the young (Spirito et al, 1989).
Since both childhood depression and conduct disorder were associated with anincreased risk of a suicidal attempt in adulthood, it may seem surprising that whenconduct disorder occurred in conjunction with childhood depression the risk ofan attempt tended to be reduced. However, it should be noted that we have shownin a previous paper that when childhood depression occurs in conjunction withconduct disorder it has a different meaning from when it occurs in its "pure" form(Harrington et al, 1991). In particular, it is associated with a lower risk of majordepression in adulthood. So, it may be that the lower risk of a suicidal attempt thatwas associated with the combination of depression and conduct disorder was partlyrelated to the lower risk of adult major depression. These findings support thedecision in ICD-10 to classify individuals with depression and conduct disorderin a separate category, namely "depressive conduct disorder" (World HealthOrganization, 1992).
Public health implications
There has been growing concern about the increase in rates of suicide amongyoung people in both North America and the U.K. (Harrington &: Dyer, 1993),where suicide is now the second most common principal cause of death among15-24-year-olds (Office of Population Census and Surveys, 1990). Attempts to

Childhood Depression and Suicidal Behaviours in Adulthood 1317
reduce the rate of suicide in this age group have so far been focused to a largeextent on identifying groups defined as "high risk" because of suicidal ideation ora previous suicidal attempt (Shaffer, Garland, Gould, Fisher 8c Trautman, 1988).However, the findings of the present study, together with those of other follow-upstudies of depressed young people, suggest that much greater attention needs tobe paid to the risks of completed suicide that are associated with child- andadolescent-onset depressive disorders. Indeed, although the data are not yet asextensive as we would wish, the mortality from suicide among child psychiatricpatients with depressive disorders seems to be at least 3% (see above, and Raoet al., 1993), which is, if anything, a little more than the mortality from suicide thatfollows a suicidal attempt in this age group (Spirito et al, 1989). We can concludethat effective treatments for juvenile depressive disorders could have a part to playin a public health programme that aims to reduce the rate of suicide among theyoung.
Acknowledgements—^This study was supported by a grant from the MacArthur Foundation Netuorkon Risk and Protective Factors in the Major Mental Disorders.
References
Andrews, J. A. & Lewinsohn, P. M. (1992). Suicidal attempts among older adolescents: prevalenceand co-occurrence with psychiatric disorders./owmaZ of the American Academy of Child Psychiatry,31, 655-662.
Baker, R. J. Sc Nelder, J. A. (1978). The GLIM system. Oxford: Numerical Algorithms Group.Fleming, J. E., Boyle, M. H. 8c Offord, D. R. (1993). The outcome of adolescent depression in the
Ontario Child Health Study follow-up./own?a/ of the American Academy of Child and AdolescentPsychiatry, 32, 28-33.
Fombonne, E. (1993). Depressive disorders: time trends and putative explanatory mechanisms. InM. Rutter 8c D. Smith (Ed.), Psychosocial disorder-s in young people: time trends and their origins.Chichester: John Wiley.
Goodman, R. 8c Simonoff, E. (1991). Reliability of clinical ratings by trainee child psychiatrists:a research note. Joumal of Child Psychology and Psychiatry, 32, 551-555.
Harrington, R. C (1992). Annotation: the natural history and treatment of child and adolescentaffective disorders. Joumal of Child Psychology and Psychiatry, 33, 1287-1302.
Harrington, R. C. (1993). Depressive disorder in childhood and adolescence. Chichester: John Wiley.Harrington, R. C. (1994). Affective disorders. In M. Rutter, E. Taylor & L. Hersov (Ed.), Child and
adolescent psychiatry: modem af^proaches. Third edition (pp. 330—350). Oxford: Blackwell Scientific.Harrington, R. C. 8c Dyer, L. (1993). Suicide and attempted suicide in adolescence. Current Opinion
in Psychiatry, 6, 467-469.Harrington, R. C, Hill, J., Rutter, M.,John, K., Fudge, H., Zoccolillo, M. 8c Weissman, M. M. (1988).
The assessment of lifetime psychopathology: a comparison of two interviewing styles. PsychologicalMedicine, 18, 487-493.
Harrington, R. C, Fudge, H., Rutter, M., Pickles, A. & Hill, J. (1990). Adult outcomes of childhoodand adolescent depression: I. Psychiatric status. Archives of General Psychiatry, 47, 465-473.
Harrington, R. C, Fudge, H., Rutter, M., Pickles, A. 8c Hill, J. (1991). Adult outcomes of childhoodand adolescent depression: II. Risk for antisocial disorders. /owrTirt/ of the American Academy ofChild Psychiatry, 30, 4?i4-4^9.
Harrington, R. C, Fudge, H., Rutter, M., Bredenkamp, D., Groothues, C. &Pridham,J. (1993).Child and adult depression: a test of continuities with data from a family study. Britishjoumalof Psychiatry, 162, 627-633.
1318 R. Harrington et al.
Hawton, K. (1992). Suicide and attempted suicide. In E. S. Paykel (Ed.), Handbook of affective disorders(2ndEd.) (pp. 635-650). Edinburgh: Churchill Livingstone.
Hawton, K 8c Catalan, J. (1982). Attempted suicide. Oxford: Oxford Medical Publications.Hawton, K. & Fagg, J. (1992). Deliberate self-poisoning and self-injury in adolescents. A study of
characteristics and trends in Oxford, 1976-89. British Joumal of Psychiatry, 161, 816-823.Hill,J., Harrington, R. C , Fudge, H., Rutter, M. & Pickles, A. (1989). Adult Personality Functioning
Assessment (APFA): an investigator based standardized interview. Britishjoumal of Psychiatry,155, 24-35.
Kovacs, M., Goldston, D. 8c Gatsonis, C. (1993). Suicidal behaviors and childhood-onset depressivedisorders: a longitudinal investigation. Joumal of the American Academy of Child Psychiatry, 32,8-20.
Lewinsohn, P. M., Hops, H., Roberts, R. E., Seeley, J. R. & Andrews, J. A. (1993). Adolescentpsychopathology: I. Prevalence and incidence of depression and other DSM-III-R disorders inhigh school students. Joumal of Abnormal Psychology, 102, 133-144.
Marttunen, M. J., Aro, H. M. 8c Lonnqvist, J. K. (1993). Adolescence and suicide: a review ofpsychological autopsy studies. European Child and Adolescent Psychiatry, 2, 10-18.
Myers, K, McCauley, E., Calderon, R. & Treder, R. (1991). The 3-year longitudinal course of suicidalityand predictive factors for subsequent suicidality in youths with major depressive disorder.yowma/of the American Academy of Child Psychiatry, 30, 804-810.
Office of Population Census and Surveys. (1990). 1990 Mortality Statistics. Cause: England and Wales.London: HMSO.
Pearce,J. B. (1978). The recognition of depressive disorder in children. Joumal of the Royal Society ofMedicine, 71, 494-500.
Pfeffer, C. R., Hurt, S. W., Kakuma, T., Peskin,J. R., Siefker, C. A. & Nagabhairava, S. (1994). Suicidalchildren grow up: suicidal episodes and effects of treatment during follow-up, /owrwa/ of theAmerican Academy of Child and Adolescent Psychiatry, 33, 225-230.
Puig-Antich, J., Goetz, D., Davies, M., Kaplan, T., Davies, S., Ostrow, L., Asnis, L., Twomey, J.,Iyengar, S. & Ryan, N. D. (1989). A controlled family history study of prepubertal major depressivedisorder. Archives of General Psychiatry, 46, 406-418.
Puig-Antich, J., Lukens, E., Davies, M., Goetz, D., Brennan-Quattrock, J. & Todak, G. (1985).Psychosocial functioning in prepubertal major depressive disorders. II. Interpersonal relationshipsafter sustained recover)'from affective episode. Archives of General Psychiatry, 42, 511-517
Puig-Antich, J., Perel, J. M., Lupatkin, W., Chambers, W. J., Tabrizi, M. A., King, J., Goetz, R.,Davies, M. 8c Stiller, R. L. (1987). Imipramine in prepubertal major depressive disorders. Archivesof General Psychiatry, 44, 81-89.
Rao, U., Weissman, M. M., Martin, J. A. 8c Hammond, R. W. (1993). Childhood depression and riskof suicide: preliminary report of a longitudinal study. Joumal of the American Academy of ChildPsychiatry, 32, 21-27.
Ryan, N. D., Williamson, D. E., Iyengar, S., Orvashel, H., Reich, T., Dahl, R. E. & Puig-Antich, J.(1992). A secular increase in child and adolescent onset affective disorder. Joumal of the AmericanAcademy of Child and Adolescent Psychiatry, 31, 600-605.
Schlesselman, J.J. (1982). Case-control Studies. New York: Oxford University Press.Shaffer, D., Garland, A., Gould, M., Fisher, P. & Trautman, P. (1988). Preventing teenage suicide:
a critical review. Joumal of the American Academy of Child and Adolescent Psychiatry, 27, 675—687.Spirito, A., Brown, L., Overholser, J. 8c Fritz, G. (1989). Attempted suicide in adolescence: a review
and critique of the literature. Clinical Psychology Review, 9, 335-363.Spitzer, R. L. 8c Endicott, J. (1975). Schedule for affective disorders and schizophrenia—lifetime version. New
York: Biometrics Research.Taylor, E. A. & Stansfield, S. A. (1984). Children who poison themselves: I. Clinical comparison with
psychiatric controls. British Joumal of Psychiatry, 145, 127-132.Thorley, G. (1982). The Bethlem Royal and Maudsley Hospitals' clinical data register for children
and adolescents. Joumal of Adolescence, 5, 179-189.

Childhood Depre.ssion and Suicidal Behaviours in Adulthood 1319
Thorley, G. (1987). Factor study of a psychiatric child rating scale: based on ratings made by clinicianson child and adolescent clinic attenders. Britishjoumal of Psychiatry, 150, 49-59.
World Health Organization. (1992). The ICD-10 Classification of Mental and Behavioural Disorders:Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organization.