Embed Size (px)
Citation preview
Substance Use & Misuse, 40:1955–1981Copyright © 2005 Taylor & Francis Inc.ISSN: 1082-6084 (print); 1532-2491 (online)DOI: 10.1080/10826080500294858
Adult ADHD and Substance Abuse: Diagnosticand Treatment Issues
APARNA S. KALBAG AND FRANCES R. LEVIN
New York State Psychiatric Institute and Department of Psychiatry, College ofPhysicians and Surgeons of Columbia University, New York, New York, USA
Attention deficit hyperactivity disorder (ADHD) is a neurobehavioral, developmentaldisorder most often diagnosed during childhood, marked by the core symptoms of inat-tention, hyperactivity, and impulsivity that results in social, academic, and occupationalunderachievement. Although the disorder has a prevalence of 3–9% in the general child-hood population and 1–5% in the general adult population, it affects between 11 and35% of “substance-abusing” adults, oftentimes complicating treatment response. Thepresent review discusses diagnostic assessment issues, prevalence, comorbidity, phar-macotherapy, and psychological interventions in substance-abusing adults with ADHD.
Keywords attention deficit hyperactivity disorder (ADHD); substance-user popula-tions; dual-diagnosis; assessment; treatment
What is ADHD?
Attention deficit hyperactivity disorder (ADHD) is a neurobehavioral, developmental dis-order most often diagnosed during childhood, marked by the core symptoms of inattention,hyperactivity, and impulsivity. During the past 2 decades, there has been an increasedawareness that many ADHD children do not “outgrow” ADHD once they reach adulthood(Barkley, 1995; Greenfield et al., 1988; Mannuzza et al., 1993, 1998) this, in turn, has ledto increased recognition of adult ADHD by clinicians and patients themselves. ADHD hashistorically referred to a syndrome of symptoms, including attentional difficulties, hyperac-tivity, and impulsive decision making. These symptoms can be obvious or subtle and oftenrequire an extensive evaluation that incorporates a comprehensive developmental history,determination of school and occupational functioning, learning difficulties, and psychiatricdiagnostic assessment. The addition of past or ongoing substance abuse/dependence cancomplicate this assessment but does not preclude the clinician’s ability to make an ADHDdiagnosis. Minimally, the diagnostician should be able to gather enough evidence to provideetiology or source of the dysfunctional ADHD symptoms, the clinical course of symptomsfrom childhood into adulthood, and the prognosis for respite from these troubling symptoms.
Diagnosis of ADHD in Adults with Substance Use Disorders
The criteria used to diagnose ADHD have changed repeatedly over the past 20 years. Ac-cording to the Diagnostic and Statistical Manual of Mental Disorder, 3rd edition (DSM-III)
Address correspondence to Frances R. Levin, M.D., 1051 Riverside Drive, Unit 66, New York,NY 10032, USA. E-mail: [email protected]
1955
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1956 Kalbag and Levin
(APA, 1980), (individuals with ADHD were described as having attention deficit disorderwith or without hyperactivity and needed to have three of five inattentive symptoms, threeof six impulsive symptoms, and two of five hyperactive symptoms. A diagnosis of ADD,residual type, required symptoms of ADD to be present in childhood and persist into adult-hood. With the advent of DSM-III-R (APA, 1987), hyperactive, impulsive, and inattentivesymptoms were combined into one criterion so that the diagnosis of ADHD required thepresence of 8 of 14 symptoms in childhood, but no adult diagnosis was specified. Instead,the diagnosis of Undifferentiated ADHD was specified, which could be applied to adultswith ADHD. However, the DSM-III-R cautioned that more “research is necessary to deter-mine if this is a valid diagnostic category and, if so, how it should be defined.” Contrastingthis, the latest edition of the DSM (version IV) (APA, 1994) recognizes that ADHD canpersist into adulthood. The current criteria require a child to have exhibited six of nineinattention and/or hyperactivity/impulsivity symptoms for at least 6 months. The adultdiagnosis requires persistence of childhood symptoms into adulthood. Inattentive symp-toms include difficulty listening to information and following through with instructions,difficulty organizing activities, memory problems, distractibility, and failure to give closeattention to details. Hyperactive-impulsive symptoms include frequent fidgeting, leaving asituation when required to remain seated, impatience, interrupting others when speaking orplaying a game, and excessive “on the go” behavior, including running and climbing. TheDSM-IV (APA, 1994) divides the diagnosis into three subtypes: predominantly inattentivetype, predominantly hyperactive-impulsive type, and combined type (both inattentive andhyperactive-impulsive types).
To be diagnosed with ADHD, these symptoms need to occur independent of otherAxis I disorders, cause significant distress to the individual and impair functioning inat least two settings (e.g., at school or work, at home, with peers). Furthermore, somehyperactive-impulsive or inattentive symptoms that cause impairment need to have beenpresent before the age of 7. This criterion is often difficult for an adult to endorse becauseof poor recollection of early childhood behaviors. Mannuzza and colleagues (1991) foundthat among individuals diagnosed with ADHD in childhood and followed into adulthood,a substantial minority of the sample could not recall their childhood ADHD symptoms asadults. Although it is a common strategy to obtain this retrospective information from theolder siblings or parents of adults who might possibly have ADHD, this is often difficult withsubstance-user populations. Oftentimes, either the patient is resistant to providing contactinformation or family members are not interested in participating in the diagnostic processbecause of constrained relationships. At times, a diagnostician can glean some informationby obtaining grades and teachers’ anecdotal reports of classroom behavior from old reportcards. By gathering as much objective evidence as possible, the diagnostician is more likelyto rule out other childhood disorders such as learning disabilities, depression, or conductdisorder, which may better explain these “ADHD-like” behaviors. Barkley and Biederman(1997) have questioned the validity of using an age-of-onset criterion, suggesting that havingimpairing symptoms during childhood, rather than having symptoms occur prior to the ageof 7, may be adequate in attaining a valid diagnosis. Clearly, a change of this criterion wouldfacilitate making the diagnosis in adults with and without substance abuse.
Another common diagnostic issue is whether the presence of less than the DSM-IVrequired minimum of 6 symptoms warrants clinical attention. Adults who endorse onlythree or four symptoms of childhood or adulthood ADHD may be diagnosed as ADHD-NOS, ADHD-in partial remission, or not diagnosed at all. Although these symptoms canbe quite impairing, clinicians may incorrectly assume that these individuals do not requiretreatment because they do not meet full diagnostic criteria (Mannuzza et al., 2003). Faraone
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

Adult ADHD and Substance Abuse 1957
and colleagues (2000) argue that the DSM-IV diagnosis of ADHD in adults may be moresensitive to reporting bias such that the symptoms needed for diagnosis are observable ratherthan experiential. For example, an individual being evaluated for ADHD is asked to qualita-tively evaluate his or her behavior (such as how well he/she follows directions or completestasks), whereas an individual with depression is asked about his or her subjective, internalstates (such as feelings of sadness or hopelessness) and tangible, behavioral manifestations(such as changes in sleep pattern or appetite). In addition, if an individual grew up in a homewhere psychiatric problems were unrecognized and untreated, it is highly unlikely that thisindividual would remember disruptive behaviors beginning in early childhood. This mayinadvertently result in an underreporting of ADHD symptoms and their sequelae.
Aside from these common diagnostic dilemmas, ADHD is often under-diagnosed insubstance user treatment settings not because of difficulties with the diagnostic criteria butbecause of the widespread lack of awareness of the diagnosis by clinicians and patients.If an individual with a substance use disorder and adult ADHD was not diagnosed as achild, it is not likely that the individual will explain his/her problematic behaviors as due tohaving ADHD. These patients may attribute their impatience, restlessness, or procrastinationto being “hot-headed,” “easily bored” or “lazy.” Second, many of the consequences ofADHD (such as work failure and poor educational attainment) also are associated withsubstance use disorders. Persons with a substance use disorder and undiagnosed ADHDmay assume that alcohol or drug use completely explain deficits in academic, vocational, andinterpersonal arenas. Furthermore, patients may have found ways to compensate for theirADHD symptoms by avoiding situations that require focused or sustained attention. Unlikedepression or psychosis, which may be incapacitating or require hospitalization, the negativeeffects of ADHD usually do not have such dramatic consequences and therefore may gounrecognized. Furthermore, an episodic change in functioning (as is seen in depression)rather than a chronic behavioral problem (as is seen in ADHD) is more likely to be noticedand attributed to a psychiatric disorder.
Another potential reason for under-diagnosis in both those with substance use disordersand without these disorders is the DSM-IV criterion that emphasizes that ADHD should notbe diagnosed if the observed symptoms are better accounted for by another mental disorder.Unfortunately, the wording of this description in the DSM-IV may lead some clinicians tointerpret this to mean that if an anxiety, depressive, or psychotic disorder is present, ADHDshould not be diagnosed at all. If ADHD co-occurs with other Axis I disorders, then bothshould be diagnosed. A final reason ADHD remains underdiagnosed and untreated is thatsome of the symptoms required by the DSM-IV may not be developmentally appropriateand may need to be modified to better characterize the difficulties experienced by adults.Although an adult diagnosis of ADHD is permitted, the behavioral markers identified withinDSM-IV are quite specific to childhood behavior, and at times no specific behavioral markersrelevant to adults are identified (e.g., often has difficulty playing or engaging in leisureactivities quietly). Future revisions of the DSM-IV will need to develop new criteria thatincorporate symptoms more relevant to the challenges encountered by adults. It is alsoimportant to recognize that although the core symptoms of ADHD remain a crucial elementof the adult disorder, additional psychiatric symptoms (and disorders) often are found amongadults with ADHD. For example, in a recent study of 46 methadone-maintained adults withADHD, 60% of participants were rated as having a problem with controlling temper “quitea bit of the time” or “very much of the time” and 49% were rated as having difficultywith depressed mood “quite a bit of the time” or “very much of the time” (Kalbag et al.,in preparation). Biederman et al. (2004) reported that 48% of adults with ADHD werefound to have two or more anxiety disorders and 30% of them were found to have major
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1958 Kalbag and Levin
depressive disorder during their lifetimes. Given these concerns, it is of utmost importancethat researchers and clinicians gain an understanding of the developmental course of ADHDand differentiate it from other comorbid conditions.
Although there are many possible reasons for underdiagnosis of ADHD, overdiagnosiscan also occur. Bipolar spectrum disorders and depressive disorders share numerous symp-toms with ADHD and these disorders may better explain the observable symptoms. Over-diagnosis may also occur when clinicians overlook the criterion of continuity of symptomsfrom childhood to adulthood or misattribute substance-induced or substance-withdrawalsymptoms as pure ADHD symptoms. In sum, as with any comprehensive diagnostic as-sessment, it is critical that the diagnostic process address developmental history, psychiatriccomorbidity, and pertinent family history, prior to initiating any pharmacotherapy.
Screening and Diagnostic Instruments
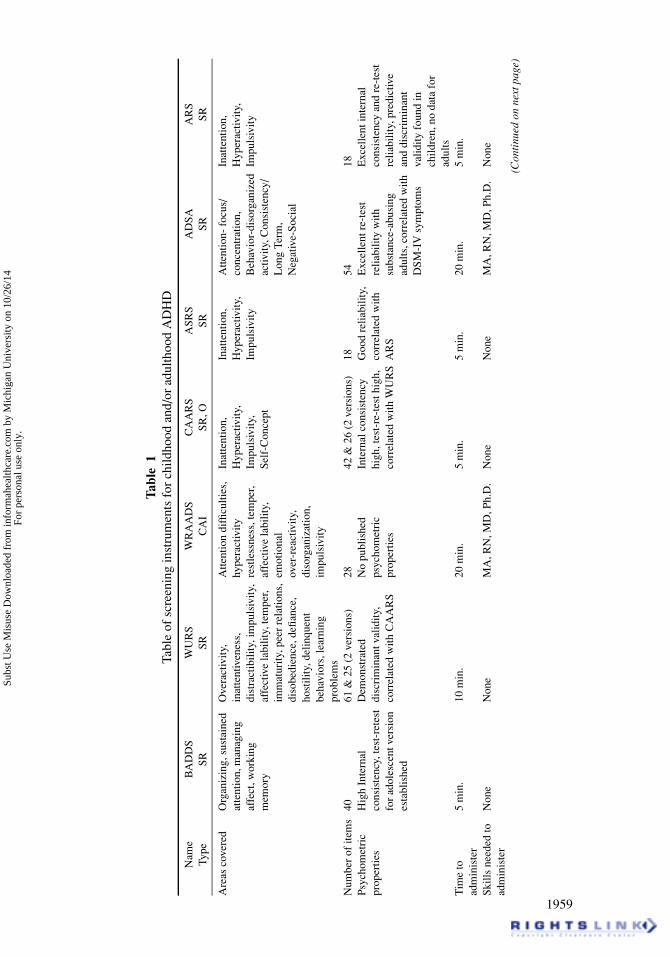
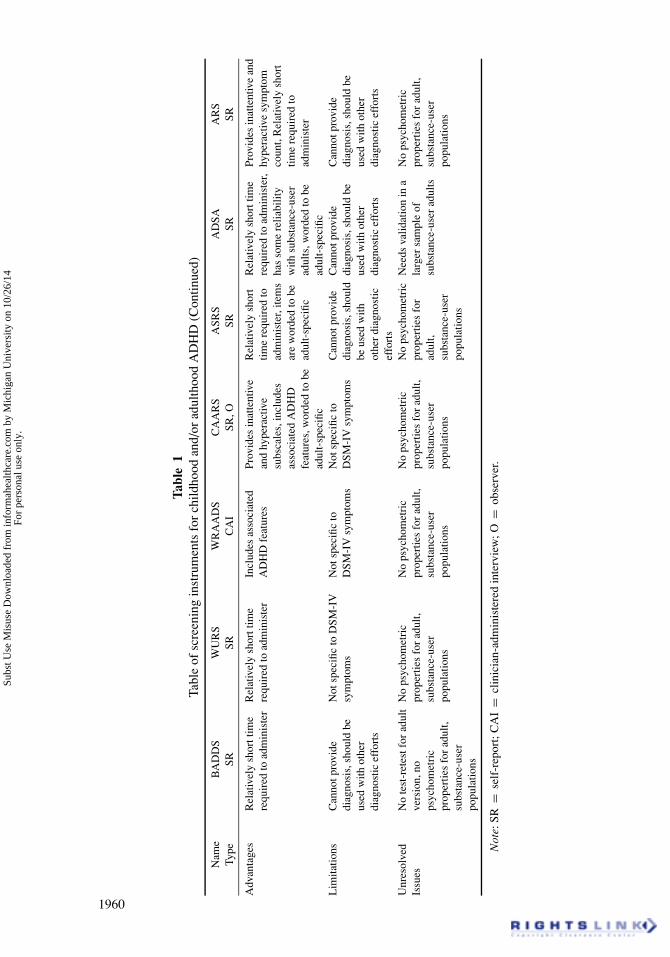
Over the past 10 years, several diagnostic systems have been developed to aid in identifyingand diagnosing adults with ADHD (Tables 1 and 2). The Brown Attention Deficit Disor-der Scales for Adults (BADDS) (Brown, 1996) is one of the earliest symptom checklistsavailable for adult populations. This scale assesses five dimensions of symptoms includ-ing sustained attention and concentration, alertness and effort, managing frustration andemotions, using working memory, and organizing work activities. Although this scale hasfairly good psychometric properties, it is not based on DSM-IV criteria and therefore, doesnot include questions about hyperactive symptoms. Therefore, its utility may be limited byunderdiagnosing ADHD in adults. Ward et al. (1993) have published a scale (Wender UtahRating Scale; WURS) widely used for screening adults for childhood ADHD symptoms.This scale, based on Wender’s Utah Criteria for ADHD (Wender, 1995; Wender et al.,2000), includes commonly observed symptoms found in children with ADHD, and is auseful screening tool. However, like many of these scales, it has not been adequately testedwith adult substance-user populations (West et al., 2003). Similarly, the Wender-ReimherrAdult Attention Deficit Disorder Scale (WRAADS) is designed to measure the severity ofadult ADHD symptoms using the Utah Criteria (Wender, 1995; Wender et al., 2000) in sevencategories: attention difficulties, hyperactivity/restlessness, temper, affective lability, emo-tional overreactivity, disorganization, and impulsivity. Unlike the Brown ADD Scales andthe WURS, this scale requires clinician ratings. The Conners Adult ADHD Rating Scales(CAARS) (Conners et al., 1999) allow for self-report and observer report and are availablein screening, short, and long versions. These scales include core DSM-IV symptoms butalso nonspecific ADHD symptoms such as mood dysregulation and low self-esteem, whichare frequently associated with an ADHD diagnosis. The Adult Self-Report Scale (ASRS)(Adler et al., 2003) and the ADHD Rating Scale–IV (ARS) (Dupaul et al., 1998) are twoother self-report measures that assess for the frequency of DSM-IV ADHD symptom cri-teria. Although both instruments have excellent interrater reliability, the reliability of theseinstruments has not been tested in substance-user adults with ADHD. The Attention DeficitScale for Adults (ADSA) (West et al., 2003), a 54-item self-report measure, is one instru-ment that has been tested in substance-user populations. West et al. (2003) found that theADSA, designed initially for use in non-substance-user populations, is a reliable and validmeasure of ADHD in adult substance-user populations.
Given the complexity of determining an ADHD diagnosis, no one scale can be used toprovide a definitive diagnosis of adult ADHD. Furthermore, when evaluating substance-userindividuals, there is a critical need to understand that the intoxication and withdrawal effectsof substances such as nicotine, alcohol, and cocaine (e.g., motor hyperactivity, agitation,
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.
Tabl
e1
Tabl
eof
scre
enin
gin
stru
men
tsfo
rch
ildho
odan
d/or
adul
thoo
dA
DH
D
Nam
eB
AD
DS
WU
RS
WR
AA
DS
CA
AR
SA
SRS
AD
SAA
RS
Type
SRSR
CA
ISR
,OSR
SRSR
Are
asco
vere
dO
rgan
izin
g,su
stai
ned
atte
ntio
n,m
anag
ing
affe
ct,w
orki
ngm
emor
y
Ove
ract
ivity
,in
atte
ntiv
enes
s,di
stra
ctib
ility
,im
puls
ivity
,af
fect
ive
labi
lity,
tem
per,
imm
atur
ity,p
eer
rela
tions
,di
sobe
dien
ce,d
efian
ce,
host
ility
,del
inqu
ent
beha
vior
s,le
arni
ngpr
oble
ms
Atte
ntio
ndi
fficu
lties
,hy
pera
ctiv
ityre
stle
ssne
ss,t
empe
r,af
fect
ive
labi
lity,
emot
iona
lov
er-r
eact
ivity
,di
sorg
aniz
atio
n,im
puls
ivity
Inat
tent
ion,
Hyp
erac
tivity
,Im
puls
ivity
,Se
lf-C
once
pt
Inat
tent
ion,
Hyp
erac
tivity
,Im
puls
ivity
Atte
ntio
n-fo
cus/
conc
entr
atio
n,B
ehav
ior-
diso
rgan
ized
activ
ity,C
onsi
sten
cy/
Lon
gTe
rm,
Neg
ativ
e-So
cial
Inat
tent
ion,
Hyp
erac
tivity
,Im
puls
ivity
Num
ber
ofite
ms
4061
&25
(2ve
rsio
ns)
2842
&26
(2ve
rsio
ns)
1854
18Ps
ycho
met
ric
prop
ertie
sH
igh
Inte
rnal
cons
iste
ncy,
test
-ret
est
for
adol
esce
ntve
rsio
nes
tabl
ishe
d
Dem
onst
rate
ddi
scri
min
antv
alid
ity,
corr
elat
edw
ithC
AA
RS
No
publ
ishe
dps
ycho
met
ric
prop
ertie
s
Inte
rnal
cons
iste
ncy
high
,tes
t-re
-tes
thig
h,co
rrel
ated
with
WU
RS
Goo
dre
liabi
lity,
corr
elat
edw
ithA
RS
Exc
elle
ntre
-tes
tre
liabi
lity
with
subs
tanc
e-ab
usin
gad
ults
,cor
rela
ted
with
DSM
-IV
sym
ptom
s
Exc
elle
ntin
tern
alco
nsis
tenc
yan
dre
-tes
tre
liabi
lity,
pred
ictiv
ean
ddi
scri
min
ant
valid
ityfo
und
inch
ildre
n,no
data
for
adul
tsT
ime
toad
min
iste
r5
min
.10
min
.20
min
.5
min
.5
min
.20
min
.5
min
.
Skill
sne
eded
toad
min
iste
rN
one
Non
eM
A,R
N,M
D,P
h.D
.N
one
Non
eM
A,R
N,M
D,P
h.D
.N
one
(Con
tinu
edon
next
page
)
1959
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.
Tabl
e1
Tabl
eof
scre
enin
gin
stru
men
tsfo
rch
ildho
odan
d/or
adul
thoo
dA
DH
D(C
ontin
ued)
Nam
eB
AD
DS
WU
RS
WR
AA
DS
CA
AR
SA
SRS
AD
SAA
RS
Type
SRSR
CA
ISR
,OSR
SRSR
Adv
anta
ges
Rel
ativ
ely
shor
ttim
ere
quir
edto
adm
inis
ter
Rel
ativ
ely
shor
ttim
ere
quir
edto
adm
inis
ter
Incl
udes
asso
ciat
edA
DH
Dfe
atur
esPr
ovid
esin
atte
ntiv
ean
dhy
pera
ctiv
esu
bsca
les,
incl
udes
asso
ciat
edA
DH
Dfe
atur
es,w
orde
dto
bead
ult-
spec
ific
Rel
ativ
ely
shor
ttim
ere
quir
edto
adm
inis
ter,
item
sar
ew
orde
dto
bead
ult-
spec
ific
Rel
ativ
ely
shor
ttim
ere
quir
edto
adm
inis
ter,
has
som
ere
liabi
lity
with
subs
tanc
e-us
erad
ults
,wor
ded
tobe
adul
t-sp
ecifi
c
Prov
ides
inat
tent
ive
and
hype
ract
ive
sym
ptom
coun
t,R
elat
ivel
ysh
ort
time
requ
ired
toad
min
iste
r
Lim
itatio
nsC
anno
tpro
vide
diag
nosi
s,sh
ould
beus
edw
ithot
her
diag
nost
icef
fort
s
Not
spec
ific
toD
SM-I
Vsy
mpt
oms
Not
spec
ific
toD
SM-I
Vsy
mpt
oms
Not
spec
ific
toD
SM-I
Vsy
mpt
oms
Can
notp
rovi
dedi
agno
sis,
shou
ldbe
used
with
othe
rdi
agno
stic
effo
rts
Can
notp
rovi
dedi
agno
sis,
shou
ldbe
used
with
othe
rdi
agno
stic
effo
rts
Can
notp
rovi
dedi
agno
sis,
shou
ldbe
used
with
othe
rdi
agno
stic
effo
rts
Unr
esol
ved
Issu
esN
ote
st-r
etes
tfor
adul
tve
rsio
n,no
psyc
hom
etri
cpr
oper
ties
for
adul
t,su
bsta
nce-
user
popu
latio
ns
No
psyc
hom
etri
cpr
oper
ties
for
adul
t,su
bsta
nce-
user
popu
latio
ns
No
psyc
hom
etri
cpr
oper
ties
for
adul
t,su
bsta
nce-
user
popu
latio
ns
No
psyc
hom
etri
cpr
oper
ties
for
adul
t,su
bsta
nce-
user
popu
latio
ns
No
psyc
hom
etri
cpr
oper
ties
for
adul
t,su
bsta
nce-
user
popu
latio
ns
Nee
dsva
lidat
ion
ina
larg
ersa
mpl
eof
subs
tanc
e-us
erad
ults
No
psyc
hom
etri
cpr
oper
ties
for
adul
t,su
bsta
nce-
user
popu
latio
ns
Not
e:SR
=se
lf-r
epor
t;C
AI
=cl
inic
ian-
adm
inis
tere
din
terv
iew
;O=
obse
rver
.
1960
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.
Adult ADHD and Substance Abuse 1961
Table 2Table of diagnostic systems for childhood and/or adulthood ADHD
Name Kiddie SADS KID-SCID CAADIDType CAI CAI CAI
Areas covered Inattention,Hyperactivity,Combinedsubtypes inchildhood
Inattention,Hyperactivity,Combined subtypesin childhood
Inattention,Hyperactivity,Combined subtypes inchildhood & adlthood
Number of items 18 18 36Psychometricproperties
Fair to goodinterrater andretest reliabilityacross alldiagnoses
Excellent ADHD retestreliability Fair toexcellent for otherdiagnoses
No published data
Time toadminister
20 min 20–30 min 60–90 min
Skills needed toadminister
MA, RN, MD, Ph.D. MA, RN, MD, Ph.D. MA, RN, MD, Ph.D.
Advantages Provides diagnosesfor other, possiblycomorbid/rule outchildhooddiagnoses
Relatively short timerequired to administer
Prompts for rule-outdiagnoses, includesadult-specificsymptoms
Limitations No adult-specificsymptoms
No adult-specificsymptoms
Time-consuming
Unresolved issues Psychometricproperties in adult,substance-userpopulation
Psychometricproperties in adult,substance-userpopulation
Psychometricproperties in adult,substance-userpopulation
Note: CAI = clinician-administered interview.
restlessness, irritability, difficulty concentrating) can often mimic ADHD symptoms (APA,1994). Therefore self-report measures should be used only to provide an initial screeningand should be followed by a thorough clinical examination, medical history, and psychiatricinterview, before providing a diagnosis.
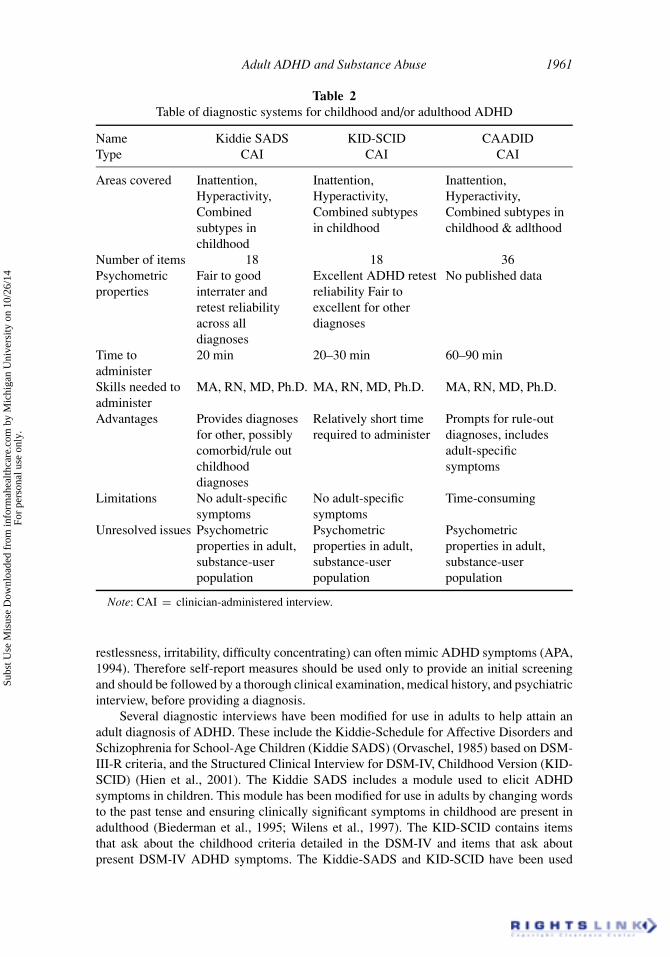
Several diagnostic interviews have been modified for use in adults to help attain anadult diagnosis of ADHD. These include the Kiddie-Schedule for Affective Disorders andSchizophrenia for School-Age Children (Kiddie SADS) (Orvaschel, 1985) based on DSM-III-R criteria, and the Structured Clinical Interview for DSM-IV, Childhood Version (KID-SCID) (Hien et al., 2001). The Kiddie SADS includes a module used to elicit ADHDsymptoms in children. This module has been modified for use in adults by changing wordsto the past tense and ensuring clinically significant symptoms in childhood are present inadulthood (Biederman et al., 1995; Wilens et al., 1997). The KID-SCID contains itemsthat ask about the childhood criteria detailed in the DSM-IV and items that ask aboutpresent DSM-IV ADHD symptoms. The Kiddie-SADS and KID-SCID have been used
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1962 Kalbag and Levin
with non-substance-user and substance-user populations to determine the prevalence ofadult ADHD as well as for attaining an adult ADHD sample for pharmacologic clinicaltrials. Although these instruments have been shown to be reliable in relatively small tomoderate samples (Biederman et al., 1995; Wilens et al., 1997; Levin et al., 1998), largereliability studies in substance-abusing populations have not been conducted.
More recently, Epstein and colleagues (2001) published a systematized diagnostic in-strument, the Conners’ Adult ADHD Diagnostic Interview for the DSM-IV (CAADID),which attempts to address a number of concerns that exist with other adult ADHD in-terviews. The CAADID is divided into two sections. Part one contains a developmentalhistory section dating from gestation to adulthood with appropriate flags indicating possi-ble ADHD risk factor(s) such as birth trauma, educational history, childhood physical orsexual trauma, family history of ADHD, and medical history. Part two contains diagnosticcriteria that requires the clinician to (1) collect information about the continuity of ADHDsymptoms from childhood into adulthood, (2) take comorbid diagnostic conditions suchas depression, mania, PTSD, anxiety, and psychosis into consideration, and (3) ensure thatreported symptoms are in fact age and context inappropriate (e.g., a 22-year-old femalewith two toddlers stating she feels overwhelmed and is easily distracted, may not be experi-encing ADHD symptoms). The CAADID has not been formally tested in adults or childrenmanifesting with substance use disorders. Ensuring the use of reliable and valid ADHDscreening and diagnostic measures for substance-user populations will provide us with amore accurate gauge of the prevalence of the disorder in this difficult-to-treat population.
Prevalence of ADHD in the General Population
Several large epidemiologic studies have found that 3–9% of children have ADHD(Szatmari, 1992). Given that 10–70% of children with ADHD continue to have symptomsinto late adolescence and adulthood (Mannuzza et al., Weiss and Hechtman, 1986; Wilenset al., 1995; Biederman et al., 2000), one would predict that the estimated rates for adultADHD in the general population would be less than 1–5%. Hill and Schoener (1996) useda mathematical model to calculate the expected prevalence rate for adult ADHD, based onthe available published literature. They posited an exponential decline in ADHD, such that99% of children would be likely to go into remission by age 20. Barkley (1997) reviewedthe assumptions underpinning this mathematical model and found several methodologicalproblems, including the fact that the authors included only studies that defined subjects ashaving persistent ADHD if they met full criteria for the disorder and excluded studies ofindividuals who manifested adult ADHD in partial remission. Clinical experience suggeststhat most patients do not meet full criteria in adulthood but do continue to have signif-icant impairment as a result of persistent ADHD symptoms. Thus, Hill and Schoener’scalculations may substantially underestimate the prevalence rates of adult ADHD. Further-more, there is evidence to suggest that the rates of adult ADHD may be even greater insubstance-abusing populations.
Prevalence of ADHD in Substance-Abusing Populations
ADHD and substance-use disorders may be related in a number of ways ( Levin and Kleber,1995). When the symptoms of ADHD are combined with those of substance-use disorders,it is likely that the severity of both disorders increases (Levin et al., 2002). Prevalencestudies using structured interviews based on the DSM-III-R and DSM-IV criteria have
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

Adult ADHD and Substance Abuse 1963
found elevated rates of childhood and adulthood ADHD among various groups of personsmanifesting substance use disorders (Eyre et al., 1982; Wood et al., 1983; Rounsavilleet al., 1991). For example, Wood and colleagues (1983) found that 33% of alcoholicsseeking treatment manifested residual attention deficit disorder (using DSM-III criteria).
Rounsaville and colleagues (1991) reported a 35% prevalence rate of childhood ADHDin a treatment-seeking cocaine-abusing population and a 22% prevalence rate of childhoodADHD in a nontreatment seeking cocaine-user sample. Levin et al. (1998) found that 20% ofcocaine-dependent individuals seeking treatment in an outpatient clinic manifested a child-hood ADHD diagnosis and 11–5% manifested adult ADHD. In a methadone-maintainedsample, King and colleagues (1999) found a 19% prevalence rate of childhood ADHD and a17% rate of adulthood ADHD. Clure and colleagues (1999) found that 15% of a substance-using sample (cocaine, alcohol) who reported symptoms in childhood, reported symptomsin adulthood as well. These rates across substance-user samples are all remarkably similar.
Researchers have observed that adult ADHD has been associated with poor treatmentcompliance and relapse to substance use in a cocaine-dependent population (Carroll andRounsaville, 1993). Furthermore, the presence of ADHD may increase the severity of thesubstance use disorder. Individuals who used cocaine and manifested childhood histories ofADHD were found to use cocaine earlier, use it more frequently and in greater amounts, andhave a greater number of treatment exposures than individuals without childhood historiesof ADHD (Carroll and Rounsaville, 1993). In adolescents, Wise et al. (2001) reported thathaving a comorbid diagnosis of ADHD impeded one’s ability to attain treatment goals ina residential setting such as attending required activities, identifying problem behaviors,making progress to change these behaviors, and maintaining positive relationships with thetreatment team and other adolescents. Levin et al. (2004) also found that adults diagnosedwith ADHD were less likely to successfully graduate from a therapeutic community programthan those without ADHD. These findings suggest that early identification and treatmentof ADHD in a substance-user population is of utmost clinical importance in successfullytreating the substance use disorder.
Prevalence of Substance Abuse/Dependence Among Adults with ADHD
Similar to the overrepresentation of ADHD in substance-user populations, there are highrates of substance abuse among the adult ADHD population. Both the EpidemiologicalCatchment Area Study and the National Comorbidity Study obtained prevalence rates forsubstance use disorders within the general population and found that lifetime rates ofsubstance abuse or dependence ranged from 17% to 27% (Regier et al., 1990; Kessleret al., 1994). Biederman and colleagues (1993) found that lifetime prevalence rates forsubstance use disorder among adults with ADHD was 52% compared with 27% in adultswithout ADHD. This elevated rate among individuals with adult ADHD is higher than therate expected on the basis of the NCS and ECA data. Nontreatment-seeking adults withADHD were also significantly more likely to have alcohol or drug use disorders than werenontreatment seeking adults who did not have histories of ADHD (Regier et al., 1990).Although our major focus thus far has been on the relationship between ADHD and alcoholand drugs, it needs to be mentioned that adults with ADHD also have higher rates ofnicotine dependence than the general population (40% vs. 26%) (Pomeraleau et al., 1995).In a prospective study, Lambert and Hartsough (1998) found that individuals with ADHDhad a significantly earlier onset of regular smoking and were more likely to smoke dailythan were adults without ADHD.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1964 Kalbag and Levin
The relationship between ADHD and substance abuse may be explained by a numberof mediating factors including the presence of conduct disorder or antisocial personalitydisorder, genetic factors, the need to self-medicate ADHD symptoms, personality factors,and low self-esteem related to poor school performance and/or negative peer evaluation.Although a thorough review of all these variables is beyond the scope of this article, wewill briefly review these factors.
Explanations of the ADHD-Substance Abuse Relationship
There is substantial evidence to suggest that children diagnosed with ADHD and comorbidconduct disorder (CD) and adults diagnosed with ADHD and comorbid antisocial person-ality disorder (ASP) are more likely to develop problems related to substance use thanthose without these comorbidities (Mannuzza et al., 1991, 1993; Biederman et al., 1995;Gittleman et al., 1985; Thompson et al., 1996; Milberger et al., 1997). One recent studyfound that young adults with CD and ADHD exhibited a greater tendency for marijuanadependence and other drug use and dependence than those with only CD (Flory et al., 2003).Although CD is strongly associated with “substance abuse” in adolescents, there is someevidence to suggest that ADHD increases the risk of substance use in adults even in theabsence of ASP (Biederman et al., 1995). Therefore, although CD may explain substanceuse in ADHD children and adolescents, ADHD may be a stronger predictor of substanceuse in adults. Another theory that may explain the ADHD-substance abuse relationship inadults is that persistent ADHD symptoms may lead to impairments in academic, occupa-tional, and interpersonal functioning. These impairments in turn may cause low self-esteemand/or depression and a propensity to use alcohol or other drugs to cope with deficits infunctioning.
An alternative plausible explanation is that stimulants, such as caffeine, nicotine, co-caine, and amphetamines, provide short-term relief for the symptoms of ADHD. For ex-ample, it has been hypothesized that individuals with ADHD may use cocaine to treat theirsymptoms of inattentiveness and hyperactivity. Nicotine, as another example, is an indirectdopamine agonist that shares certain properties with methylphenidate and amphetamine,two commonly used treatments for ADHD (Hoffman and Lefkowitz, 1996). Nicotine alsopromotes the release of acetylcholine, which plays a role in attentional processes (Wonnacottet al., 1989). Therefore, nicotine, which is more highly available and still more socially ac-ceptable than cocaine, may be the drug most likely to serve as an effective self-medicationoption for adults with ADHD. However, individuals with ADHD may be more likely touse any substance (e.g., marijuana, alcohol) that provides immediate symptom relief fromdistressing ADHD symptoms (e.g., inability to feel calm), rather than solely use drugs thatincrease their ability to concentrate (e.g., cocaine, nicotine). Unfortunately, over time, drugsused to self-medicate may cause more problems than they solve.
Some have posited that the cardinal symptom of ADHD, impulsivity, may cause in-dividuals to initially try a novel substance without thinking through the consequences ofinitiating such use. When interviewed about their experimentation with substances, someindividuals with persistent ADHD symptoms do not endorse ever having used substancesto ameliorate their psychiatric symptoms. Rather, they report that they tried drugs becauseof their impulsive behaviors and frequently associated with peers who facilitated their earlyuse of alcohol and illicit drugs.
There also, may be genetic factors that contribute toward the observed over-representation of substance abuse among adults with ADHD. Faraone and colleagues (1999)
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

Adult ADHD and Substance Abuse 1965
found that among 27 triads consisting of an adult with ADHD, his or her spouse, and theirchild with ADHD, the number of 7-repeat alleles of the Dopamine Receptor D4 (DRD4)gene predicted the diagnosis of ADHD in the adult parents. This finding supports earlierwork suggesting that the 7-repeat allele of the DRD4 may be over-represented in childrenwith ADHD (LaHoste et al., 1996). Because the DRD4 gene has been implicated in reducingpost-synaptic sensitivity to dopamine, the link between this gene and ADHD is consistentwith the hypothesis that ADHD symptoms are related to hypo-dopaminergic function (Sul-livan and Levin, 2001). Although the majority of data links the Dopamine D4 receptor(DRD4) gene to ADHD, a recent study has found that another dopamine receptor gene,DRD5, is more likely to be associated with the inattentive and combined subtypes thanthe hyperactive subtype of ADHD (Lowe et al., 2004). Dysregulation of the dopaminetransporter has also been implicated in the pathophysiology of ADHD and substanceabuse. The 10-repeat allele of the dopamine transporter gene has been found in greaterdensities in those with ADHD (Cook et al., 1995; Gill et al., 1997). Because it is wellestablished that substance use increases the amount of dopamine released into the nu-cleus accumbens (Wise, 1998; Beurrier and Malenka, 2002), it follows that substances thatincrease the amount of dopamine found in the synapse would be used to self-medicatesymptoms of ADHD (e.g., cocaine, nicotine).
A controversial but recently refuted explanation for the observed association betweenADHD and substance use is that exposure to stimulants—even those prescribed in controlleddoses by treatment providers—increases the likelihood that an individual will use and/ormisuse substances in adulthood. This heightened posited risk is thought to occur by (1)the process of behavioral sensitization or (2) the patients’ belief that, because a stimulantmedication has been prescribed, cocaine or other drugs can be used without risk of abuse.Although one study found that adults diagnosed with ADHD as children and had takenstimulant medications were more likely to be daily cigarette smokers than were those whohad not taken stimulants (Lambert and Hartsough, 1998), other studies suggest that treatingADHD children with stimulants reduces the risk of later alcoholism (Paternite et al., 1999)and other substance use disorders (Biederman et al., 1999; Biederman, 2003; Hechtmanand Greenfield, 2003; Mannuzza et al., 2003; Wilens et al., 2003). Biederman (2003) foundthat individuals who were treated for ADHD with a stimulant were 3–4 times less likelyto develop substance use disorders in adolescence than individuals not treated for theirADHD. A subsequent meta-analysis of six prospective, longitudinal studies have supportedthe finding that medication treatment for childhood ADHD reduces the risk of substanceuse in adolescence and/or adulthood (Wilens et al., 2003). Specifically, those not treatedwith pharmacotherapy in childhood for their ADHD symptoms were almost twice as likelyto develop a substance use disorder in young adulthood compared to those treated withstimulants.
Treatment for Substance Use Disorders and Adult ADHD
Given the negative effect that ADHD has on an individual’s social and occupational func-tioning (Mannuzza et al., 1991, 1993, 1997; Mannuzza and Klein, 2000; Weiss et al., 1999;Murphy et al., 2002), and the worse response that those who have substance use disordersand comorbid ADHD have in treatment (Clure et al., 1999; Carroll and Rounsaville, 1993),it is not surprising that, although in its infancy, the development of treatments targeting thisdually disordered population has begun. Compared with other patients with substance usedisorders, individuals with ADHD may have greater difficulties in processing information
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1966 Kalbag and Levin
and may have greater problems in sitting through group meetings—a common format formutual-help-based treatment such as Alcoholics Anonymous and Narcotics Anonymous.Because individuals with ADHD often act impulsively, they also may be more likely thanthose without ADHD to “drop out” of treatment (Carroll and Rounsaville, 1993). Coun-selors or other patients may find individuals with unrecognized ADHD to be “annoying”or “treatment-resistant” and may have less empathy for them than for those without thisdisorder. This attitude can increase the likelihood that patients with ADHD will terminatetreatment. By recognizing and treating the ADHD, the patients’ problems may be alleviatedand their treatment outcomes improved. For example, therapists who are trained to focusspecifically on “therapeutic engagement” rather than “skills-building” may find more suc-cess in retaining these patients in treatment. Future research on the effectiveness of matchingindividuals with ADHD and substance use disorders to treatments designed for their needsis warranted.
Although treatment of persons with substance use disorders and adult ADHD can becategorized as pharmacologic or nonpharmacologic, this is a somewhat artificial distinc-tion, because the two approaches often are used concurrently. Initially, the clinician mayopt for a nonpharmacologic intervention. However, if these interventions fail to improvesymptoms, a pharmacologic intervention may be added. By using pharmacologic interven-tions to reduce ADHD symptoms such as distractibility or restlessness, nonpharmacologictreatment approaches may be better used. It is also becoming increasingly clear that adultswith ADHD often have other comorbid conditions. It may be that adults with ADHD andcomorbid conditions will benefit from a regimen of more than one medication. Clearly,this can become complicated when such patients also have one or multiple substance usedisorders. When possible, it appears prudent to use a single medication to treat the con-dition that requires the most immediate attention. If the patient demonstrates substantialclinical improvement with the first medication, then another medication can be added asneeded for the other psychiatric condition, with appropriate caution due to possible druginteractions. The use of multiple medications requires close attention to side effects andpossible medication interactions. If certain comorbid conditions go untreated (e.g., bipolardisorder, depressive disorder), it is less likely that the patient will respond to treatment thattargets the ADHD symptoms.
Pharmacologic Interventions
Historically, treatment studies in adults with ADHD have not been designed to target sub-stance abuse disorders. In the following section we will review the literature for each classof medication with non-substance-user populations and also review existing studies (ifany) targeting substance users, most of which are open trials. Psychostimulants, particu-larly methylphenidate, are the most commonly prescribed and most efficacious medicationsfor both childhood and adulthood ADHD (Wilens et al., 1995; Barkley, 1979; Greenhill,1992). The majority of studies carried out with adults have reported benefits from stimu-lants, although the results have not been as robust as those found in children. The studiesthat have shown the best response in adults have used larger doses. Spencer and colleagues(1995) found that methylphenidate (up to 1.0 mg/kg per day) produced substantial improve-ment in ADHD symptoms in 78% of adults, compared to 4% of those receiving placebo.Two double-blind studies comparing methylphenidate to placebo for the treatment of adultADHD included a small number of persons who also manifested substance use disorders(Spencer et al., 1995; Mattes et al., 1984). The researchers found that those who manifestedboth substance use disorders and ADHD responded better to methylphenidate than did
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

Adult ADHD and Substance Abuse 1967
those without substance use disorders. However, the effect of the methylphenidate on thepatients’ substance use disorders was not described. Dexamphetamine is another stimulantthat has shown significant utility in reducing ADHD symptoms in those without substanceuse disorders within a double-blind placebo controlled trial (Patterson et al., 1999). Dexam-phetamine was well tolerated and the most significant reported side effect was weight loss.Modafinil, a novel psycho-stimulant, has been evaluated in children with ADHD (Ruginoand Samsock, 2003) and adults with ADHD (Taylor and Russo, 2000) with positive out-comes. Another stimulant, a mixture of amphetamine and dextroamphetamine (Adderall),was found to produce significant improvement in ADHD symptoms compared with placeboin adults with ADHD (Horrigan and Barnhill, 2000; Spencer et al., 2001). This medicationwas well tolerated in non-substance-user adults with ADHD. Wilens and colleagues (1999)found that moderate to high doses of pemoline were somewhat more effective than placeboin treating adult ADHD but given pemoline’s limited efficacy, tolerability, and associationwith hepatic dysfunction (particularly in persons with substance use disorders), the authorsrecommended pemoline as a second-line treatment for adult ADHD.
None of the trials mentioned above was designed to assess the effects of these med-ications on reducing drug use and ADHD symptoms in comorbid adults. To date, severalresearchers (Khantzian, 1983; Khantzian et al., 1984; Levin et al., 1998; Somoza et al.,2000; Schubiner et al., 2002) have provided some data suggesting that methylphenidate hasclinical utility as a treatment for adult ADHD in cocaine users seeking treatment. Levin et al.(1998) reported that ADHD symptoms and cocaine use decreased significantly in responseto divided daily doses ranging from 40 to 80 mg/day of sustained-release methylphenidate.Another pilot study also supports the hypothesis that methylphenidate might reduce cocaineuse and ADHD symptoms (Somoza et al., 2000). In the only (to date) double-blind trialin cocaine abusers, Schubiner et al. (2002) reported significant changes in physician andself-reported efficacy indices for ADHD with methylphenidate, but no significant change inADHD symptoms using a standard ADHD checklist was found. There also were no changesin cocaine use. These results need to be interpreted with caution given the relatively smallsample size used (n = 48).
At present, data to evaluate the efficacy of various other pharmacologic agents for adultADHD in persons with substance use disorders are limited. Bromocriptine has been given topersons with co-occurring ADHD and substance use disorders (primarily involving cocaineand/or marijuana abuse), with mixed results (Cocores et al., 1987; Cavanagh et al., 1989).Because most of the published data are derived from a small number of case reports andopen trials, it remains to be tested in double-blind trials.
Another promising agent, atomoxetine, (a nonstimulant, noradrenergic reuptake in-hibitor) has recently been approved for both childhood and adulthood ADHD (Spenceret al., 1998; Michelson et al., 2003). In fact, atomoxetine is the only FDA-approved non-stimulant medication for the treatment of adult ADHD. Given the increased risk of misuse ofstimulants, atomoxetine has become a common first choice in treating adults with ADHDand is likely to be the first-line treatment for adults manifesting substance use disordersand ADHD. There are laboratory data to support that it has low abuse liability and is welltolerated (Michelson et al., 2003).
Other nonstimulant medications that have been studied for the treatment of adult ADHD(mainly in those without substance use disorders) include desipramine (Wilens et al., 1996),bupropion (Wilens et al., 2001; Kuperman et al., 2001), venlafaxine (Wilens et al., 1995;Adler et al., 1995; Hedges et al., 1995; Findling et al., 1996), buspirone (Taylor and Russo,2001), guanfacine (Niederhofer, 2003), and ABT-418 (Wilens et al., 1999), a selectivecholinergic activating agent.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1968 Kalbag and Levin
Wilens and colleagues (1996) found that desipramine, a nonstimulant, produced a sig-nificant reduction in ADHD symptoms, compared with placebo. In a recent study, bupro-pion showed a clinical advantage over placebo in reducing symptoms in adults with ADHD(Wilens et al., 2001). Kuperman et al. (2001) studied whether bupropion or methylphenidatewas better than placebo at controlling ADHD symptoms in adults. He did not find significantdifferences between active and placebo conditions, but this may be due to the small numberof patients (total N = 30) enrolled in this study. In a small open study with cocaine users,Levin and colleagues (1995) found bupropion was similar to methylphenidate in reducingcocaine use and ADHD symptoms. However, this promising finding needs to be replicatedin larger, placebo-controlled trials.
Another medication approved for the treatment of depression that shows some promisefor the treatment of adult ADHD is venlafaxine. However, this medication has only beenevaluated in open trials (Wilens et al., 1995; Adler et al., 1995; Hedges et al., 1995; Findlinget al., 1996). Guanfacine, an alpha-agonist, was compared with dextroamphetamine byusing a crossover design with 17 non-substance-user adults (Taylor and Russo, 2001). Itwas found to be as effective as the stimulant in reducing self-reported and clinician-ratedADHD symptoms. Both medications demonstrated improvements in cognitive attentionaltasks. In a more recent pharmacotherapy pilot study, Niederhofer (2003) tested buspirone,an antianxiety agent that works as a serotonin antagonist and also works on the dopaminesystem. Niederhofer (2003) found significant improvements in Wender Utah ratings ofhyperactivity, inattention, and immaturity symptoms such as frustration tolerance in anopen trial with 8 adults, aged 15–34. Given its low abuse potential including its low sedativeeffect, buspirone’s utility for treatment of adult ADHD should be tested in larger, controlledtreatment trials.
Another interesting pharmacologic approach is to test medications with cholinergicactivity. Acetylcholine plays a role in attentional processes (Wonnacott et al., 1989) andlike other medications that modulate this system, it may improve ADHD symptoms. Using adouble-blind placebo-controlled design, Wilens and colleagues (1999) assessed the efficacyof ABT-418, a cholinergic activating agent delivered in a transdermal patch. Moderateimprovements were found in adults with ADHD who received the patch. Because ABT-418appeared to selectively improve attentional symptoms, rather than hyperactive or impulsivesymptoms, this medication might be targeted to patients with the inattentive subtype.
Treating the symptoms of ADHD can be a complicated process, especially within thosewith substance use disorders. Ideally, the medication(s) selected would be effective for thetreatment of ADHD, have low abuse potential, and be proven to be safe when combinedwith other psychoactive substances. At present, no single medication has been shown toadequately meet all of these criteria.
Cognitive and Behavioral Therapies
Compared with the pharmacologic treatment literature, there are even fewer clinical datato suggest which nonpharmacologic approaches work best for persons with substance usedisorders and adult ADHD. Addressing ADHD symptoms and substance use problemsin psychotherapy can provide new challenges to the therapeutic process. For example,frequently missed appointments could be the outcome of an unorganized schedule or aresult of an unplanned drug using and recovery episode. This can intentionally or un-intentionally affect the nature and strength of the alliance that develops between therapistand client. Below we examine the relevant literature on existing psychological therapiesfor ADHD and review the neurocognitive model of ADHD, including pertinent treatment
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

Adult ADHD and Substance Abuse 1969
strategies. In both the treatment literature for childhood ADHD and for substance usedisorders, positive outcomes are reported with the use of behavioral approaches. Suchapproaches include (1) contingency management, (2) cognitive-behavioral interventions,and (3) combined pharmacologic and behavioral interventions. It is of interest that theliterature on childhood ADHD suggests that negative contingencies may be a necessarycomponent of treatment (Pelham and Sams, 1992), whereas positive contingencies havebeen stressed as an appropriate treatment for adults with substance use disorders (Higginset al., 1994). To date, there have been no contingency management treatments targetedto persons with both adult ADHD and a substance use disorder. Although children withADHD may receive (or lose) a token for violation of a classroom rule, establishing a tokeneconomy system for ADHD behaviors manifested in adulthood would prove more difficult.
The use of cognitive interventions for children with ADHD has included verbalself-instructions, problem-solving strategies, cognitive modeling, self-evaluation, and self-reinforcement. In a recent collaborative study (MTA cooperative Group, 1999), childrenwith ADHD and anxiety responded nearly as well to behavioral treatment as they did to med-ication management or combined treatment. For those ADHD children without a comorbidanxiety disorder, medication or combined treatment was superior to behavioral treatmentalone. These data imply that adults with ADHD and co-morbid anxiety may do particularlywell with behavioral approaches. Given that some adults with substance use disorders andADHD have comorbid anxiety, it would not be surprising if behavioral interventions thattargeted both the ADHD symptoms and substance abuse might be an effective treatmentapproach for such complicated patients. Cognitive-behavioral therapy has become an inte-gral part of many substance user treatment programs. The question is whether this approachworks equally well for persons with comorbid ADHD and substance use disorders.
Weinstein (1994) has suggested that adults, in contrast to children, have a greaterpotential to understand the meaning of dysfunctional behavior and the effects of ADHDsymptoms on their lives and, therefore, may be better able to use cognitive-behavioralapproaches. Adapting the work of other investigators, Weinstein (1994) has suggestedseveral attention and memory strategies to help individuals cope with ADHD symptoms,including the use of organizers and calendars. However, cognitive-behavioral techniquesmay need to be modified for persons with ADHD and substance use disorders. For example,less emphasis may be placed on completion of homework tasks and more emphasis onsession work. These patients also are poor self-observers and have difficulty understandingwhy they behave in a certain way.
Aviram et al. (2001) reported that the goal of manualized relapse prevention therapy (acognitive-behavioral therapy) with a dually diagnosed population has to include identifyinglinks between ADHD and drug use. For example, a therapist may draw links between thelimitations placed by the sequelae of ADHD and feelings of negative self-worth that maylead to drug use. Drug use may then further limit the patient’s coping abilities and reinforcethe drug use. The authors maintain that these limitations must be countered in treatment byproviding tangible coping skills and strategies, many of which can be incorporated into therelapse prevention model.
Another common therapeutic dilemma is that adults with ADHD, as well as those withsubstance use disorders, are oftentimes angry and irritable and have unstable interpersonalrelationships. These emotional outbursts can impede learning skills taught in therapy. Thetask of the clinician with such a patient is to understand the emotional nature of the patient’sresponse and teach the patient to mitigate their initial angry response. Clinical experienceand empirical evidence suggests that by validating emotions, especially negative emotionssuch as anger, frustration, and irritability, clinicians can provide a therapeutic environment in
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.
1970 Kalbag and Levin
which cognitive tasks are more likely to be attempted and successfully completed (Linehanet al., 1991, 1999). In addition, therapists can help patients understand their anger as a sourceof energy to make or request necessary changes in their environments. Dialectical BehaviorTherapy (DBT) (Linehan et al., 1991, 1999) is one approach that encourages therapists tovalidate emotional experience while supporting the patient in engaging in cognitive taskssuch as effective problem solving or learning communication skills.
Emotional validation techniques include active observing, reflection, and the directvalidation of emotionally laden verbalizations or behaviors. By validating these emotions(and not the irrational behaviors that often stem from negative emotions), patients will bemore likely to use effective problem-solving strategies. Hesslinger and colleagues (2002)tested whether DBT successfully treated the symptoms of ADHD in an uncontrolled pilottrial with a sample of eight adult (non-substance-user) ADHD individuals. The researchersprovided 13 two-hour group DBT sessions over a period of 3 months. In this trial, theauthors found that despite enrolling relatively few subjects, overall improvement in ADHDand depression symptoms was significant at post-intervention. In those with substanceuse disorders with ADHD, it is likely that emotional reactions trigger impulsive decisionmaking including drug use behavior. By teaching these individuals to control their emotionalreactions, reduce feelings of being overwhelmed by negative life events, and productivelysolve their problems, reliance on drug use as a coping mechanism will reduce.
Although cognitive-behavioral therapy has shown to have some clinical benefit insubstance-user ADHD individuals, it may be inappropriate for individuals who are not ableto comprehend or use didactic or highly verbal therapeutic material. The neurobiologicalnature of ADHD lends itself to a treatment that relies on cognitive restructuring. Below, thefeatures of the neurocognitive model of ADHD and specific cognitive retraining therapytechniques that have been adapted into practice to address the neuropsychological deficitsmost commonly found in those with substance use disorders with ADHD, are presented.
Neurocognitive Deficit Model
The classic neuropsychological profile of an individual with ADHD is characterized by aninability to sustain attention, a tendency to shift focus to irrelevant cues in the environment,and difficulty regulating immediate initiation of a response to stimuli (2001). Althoughpharmacological interventions may decrease the frequency of core ADHD symptoms (inat-tention, hyperactivity, and impulsivity), psychological interventions can help an individuallearn socially appropriate behaviors to replace maladaptive behavior patterns. Researchersagree that ADHD is a developmental, neurobiological disorder. Although not specific toADHD, research has consistently demonstrated that the neurological difficulty underlyingADHD points to dysfunction in corticostriatal pathways that cause either inactivation orinsufficient engagement of the striatum, prefrontal lobes, and the dorsal anterior cingulatecortex (Zametkin et al., 1990, 1993; Schweitzer et al., 2000; Ernst et al., 1998; Bush et al.,1999; Vaidya et al., 1998; Rubia et al., 1999). When the dorsal anterior cingulate cortexfunctions properly, it plays a key role in the self-control of impulsive behaviors. Thus far, re-search into the neurocognitive functioning of individuals with ADHD has implicated deficitsin executive function, including deficits in attention and response regulation as responsiblefor ADHD symptoms. Broadly speaking, executive dysfunction includes problems withplanning (sequencing, temporal organization, and prioritizing), goal setting, working mem-ory, and set flexibility. Deficits in these areas characterize the neuropsychological profile ofADHD adults.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

Adult ADHD and Substance Abuse 1971
Disruption of selective attention is one area of cognitive functioning implicated inADHD symptoms. Despite the lack of a distinct neuropsychological marker of ADHD,there is clear evidence that adults with ADHD suffer from an inability to sustain atten-tion on relevant stimuli, in which the individual moves mentally to another task beforecompleting the initial task (Carter et al., 1995). Selective inattention is the inability to dis-criminate relevant data from irrelevant data in the stimuli field. A consistent observationin children and adults with ADHD is that they often fail to complete important tasks be-cause they switch their attention too quickly from the target stimuli whether written orauditory. Neuropsychological testing of children with ADHD has found defective inhibi-tion of attention by the right hemisphere (Carter et al., 1995). Seidman and colleagues(1998) found that adults with ADHD demonstrated impaired sustained auditory attentionand impaired ability with computing numbers compared with adults without ADHD, overand above the effects of age, gender, the presence of learning disabilities, and psychi-atric comorbidity. Most disturbing is the fact that these deficits are directly associatedwith difficulties with problem solving and with navigating educational, occupational, andsocial tasks.
Response disinhibition, another area of executive functioning implicated in causingADHD symptoms, is the failure to suppress inappropriate responding to stimuli. Impair-ments in psychomotor speed and committing errors of commission on timed performancetasks operationalize this deficit (Grodzinsky and Barkley, 1999; Lovejoy et al., 1999). Forexample, Brooks and colleagues (2004) found that methadone-maintained individuals withADHD and cocaine dependence committed more errors on attention tasks than individualswho manifested neither ADHD nor cocaine dependence or individuals who were diagnosedwith only cocaine dependence. Therefore, therapists working with those with substance usedisorders and ADHD should help these individuals develop skills to control or slow downimmediate responses to stimuli. They should teach individuals to understand how impul-sive behavior operates, how to avoid environmental situations that make impulsive decisionsmore likely, and how to remind oneself about the long-term negative consequences of theirdrug use behavior.
Often, ADHD adults also have difficulty recognizing social cues and appropriatelyresponding to them. When a therapist stands up to signal the end of a session, many ADHDindividuals continue to speak until salient, directive statements are made to stop talkingand end the session. Clinicians should incorporate exercises that help identify relevantsocial cues and socially acceptable responses to those cues. Often, those with substance usedisorders and prolonged histories of drug use also have deficits in social functioning. Eitherbecause of a disregard for conventional societal norms, never learning appropriate socialgraces, and/or an inability to control impulsive behavior, drug users often find themselvesrejected by society.
Several clinicians have described other cognitive remediation tasks that can be usedin clinical practice that aid those with cognitive deficits and regain a mastery over externalstimuli (Weinstein, 1994; Sohlberg and Mateer, 2001; Dansereau et al., 1995; Stevensonet al., 2002). Node-link mapping is an established technique that has demonstrated clinicalutility with drug users who suffer from attention difficulties and may have use in those withsubstance use disorders and ADHD. This technique, an example of a visual representationsystem of clients’ identified problems, is used as a nonverbal problem-solving strategy.Dansereau and colleagues (1995) showed that when node-link mapping was provided toopiate-dependent individuals who also used cocaine and who manifested general attentiondifficulties (not necessarily diagnosed with ADHD), they were less likely to “drop out” oftreatment, had greater self-confidence, had greater rapport with their counselors, and had
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1972 Kalbag and Levin
fewer opiate or cocaine positive urine specimens than opiate-dependent individuals whodid not receive this treatment.
Stevenson and colleagues (2002) tested a cognitive remediation program aimed attargeting ADHD symptoms. In a randomized clinical trial (N = 43) with non-substance-user adults with ADHD, they found that those who received eight 2-hour group therapysessions reported reductions in core ADHD symptoms, improved organizational skills, anddecreased trait anger, compared with waitlisted controls. Cognitive remediation techniquesaimed at those with substance use disorders with ADHD can be designed to address deficitscaused by both ADHD and long-term substance use. A major goal of any psychotherapeuticapproach with those with substance use disorders and ADHD has to include practicingand improving cognitive skills. In sum, providing targeted therapeutic strategies for theneuropsychological deficits found in ADHD individuals may provide advantages not foundwhen using broad cognitive or behavioral therapeutic approaches.
Summary
Clearly, many questions still need to be answered regarding the diagnosis and treatmentof persons with cooccurring adult ADHD and substance use disorder. The criteria for di-agnosis and the reliability and validity of screening instruments for adult ADHD have yetto be established. Although stimulant and nonstimulant medications have been shown tobe useful in treating patients with adult ADHD, their effect on ADHD symptoms and co-occurring substance use disorders requires further investigation using controlled studies.There are even fewer empirical data evaluating the use of nonstimulant agents or non-pharmacologic treatment strategies for adults with ADHD and substance use disorders.However, the lower abuse liability of nonstimulant medication and possible benefit of psy-chotherapeutic approaches make these treatment strategies intriguing possibilities. Giventhe substantial subpopulation of persons with substance use disorders and adult ADHD,further research on pharmacological and psychological treatments is warranted.
RESUME
Le Desordre d’Hyperactivite de Deficit d’Attention (ADHD) est un neurobehavioral, ledesordre du developpement le plus souvent diagnostique pendant l’enfance, marquee parles symptomes de base d’inattention, hyperactivite et impulsivity qui s’ensuit dans under-achievement social, theorique et du metier. Bien que le desordre ait une predominancede 3%–9% dans la population d’enfance generale et 1%–5% dans la population adultegenerale, il affecte entre 11%–35% d’adultes abusant de substance, souvent les temps encompliquant la reponse de traitement. La presente revision discute des editions d’evaluationdiagnostiques, une predominance, comorbidity, pharmacotherapy et des interventions psy-chologiques dans les adultes abusant de substance avec ADHD.
RESUMEN
El Desorden de Hiperactividad de Deficit de Atencion (ADHD) es un neurobehavioral,desorden del desarrollo el mas a menudo diagnosticado durante la infancia, marcada porlos sıntomas principales de falta de atencion, hiperactividad, e irreflexion que causa under-achievement social, academico y ocupacional. Aunque el desorden tenga un predominio del
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.
Adult ADHD and Substance Abuse 1973
3%–9% en la poblacion de infancia general y el 1%–5% en la poblacion general adulta, estoafecta entre el 11%–35% de adultos que abusan de sustancia, a menudo tiempos compli-cando la respuesta de tratamiento. La revision presente habla de cuestiones de evaluaciondiagnosticas, predominio, comorbidity, farmacoterapia, e intervenciones psicologicas enadultos que abusan de sustancia con ADHD.
THE AUTHORS
Aparna S. Kalbag, Ph.D., is a Research Scientist atthe New York State Psychiatric Institute, Columbia-Presbyterian Medical Center who completed her doctoratein Clinical Psychology from the University of Colorado atBoulder in 2001. Her research interests are in the areas ofcomorbidity between ADHD and cocaine and heroin de-pendence and comorbidity between depression and mar-ijuana dependence. She also has a strong interest in therole of family factors in substance use disorders and in de-veloping culturally sensitive psychological therapies forthose with substance use disorders. She has authored 3peer-reviewed papers and 13 scientific presentations. Shecurrently is the recipient of a National Institutes of Health
Loan Repayment Program award and has been a past recipient of a National Institute ofMental Health Grant, Research Supplement for a project entitled “Classifying Course ofIllness in Bipolar Disorder.”
Frances R. Levin, M.D., is a Research Psychiatrist atthe New York State Psychiatric Institute, Associate Di-rector of Substance Abuse Education at the NYSPI andQ. J. Kennedy Associate Professor and Director of theAddiction Psychiatry Fellowship Program at the Collegeof Physicians and Surgeons of Columbia University. Dr.Levin graduated Phi Beta Kappa from Brown University.She received her medical training at Cornell UniversityMedical College and her psychiatric residency at NewYork Hospital-Payne Whitney Clinic and completed acombined research and clinical substance abuse fellow-ship at the National Institute on Drug Abuse and the Uni-versity of Maryland. Dr. Levin has numerous presenta-
tions and publications to her credit in the fields of substance abuse and dual diagnosisdisorders and has served on several governmental advisory panels. Dr. Levin is the directorof three multiple-site NIH-funded research studies to develop and evaluate new medicationsfor the treatment of drug abuse. Her research interests include medications for cocaine abuseand treatment of patients who abuse drugs and also have psychiatric problems. Dr. Levin isa national expert on the treatment of drug abusers with adult attention-deficit hyperactivitydisorder (ADHD).
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1974 Kalbag and Levin
Glossary
abuse liability a measure of the likelihood that a substance’s use will result in drug addictionbehavioral marker An observable indication that changes may be occurring at the cellular
or molecular level of brain circuitsbehavioral sensitization the progressive augmentation of behavioral responses to psychomo-
tor stimulants that develops during their repeated administration and persists for longperiods
node link mapping a simple visual representation technique used to depict and exploredrug abuse recovery issues in counseling sessions originally developed as a cognitiveenhancement technique in educational settings
open trials a clinical trial in which the investigator and participant are aware which inter-vention is being used for which participant (i.e., not double blind). Random allocationmay or may not be used in such trials.
response disinhibition a form of impulsivity defined either as making responses that arepremature or as the inability to withhold a response.
selective inattention an inconsistency in attentional processes characterized by hyper-focused attention on certain stimuli (e.g., video games, TV) and an unfocused attentionto other stimuli (e.g., reading).
References
Adler, L. A., Kessler, R. C., Spencer, T. (2003). Adult ADHD Self-Report Scale-v1.1 (ASRS-v1.1)Symptom Checklist. New York, NY: World Health Organization. (http://www.med.nyu.edu/Psych/training/adhd.html). Accessed April 8, 2004.
Adler, L. A., Resnick, S., Kunz, M., Devinsky, O. (1995). Open-label trial of venlafaxine in adultswith attention-deficit disorder. Psychopharmacol Bulletin 31(4):785–758.
American Psychiatric Association. (1980). Diagnostic and Statistical Manual of Mental Disorders,version III. Washington, DC: American Psychiatric Press.
American Psychiatric Association. (1987). Diagnostic and Statistical Manual of Mental Disorders,version III-R. Washington, DC: American Psychiatric Press.
American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders,version IV. Washington, DC: American Psychiatric Press.
Armstrong, C. L., Hayes, K. M., Martin, R. (2001). Neurocognitive problems in attention deficitdisorder. Alternative concepts and evidence for impairment in inhibition of selective attention.Annals of the New York Academy of Sciences 931:196–215.
Aviram, R. B., Rhum, M., Levin, F. R. (2001). Psychotherapy of adults with comorbid attention-deficit/ hyperactivity disorder and psychoactive substance use disorder. Journal of PsychotherapyPractice and Research 10(3):179–186.
Barkley, R. (1995). Taking Charge of ADHD: The Complete Authoritative Guide for Parents. NewYork: Guilford Press.
Barkley, R. A. (1977). A review of stimulant drug research with hyperactive children. Journal of ChildPsychology and Psychiatry 18(2):137–165.
Barkley, R. A. (1997). Advancing age, declining ADHD. American Journal of Psychiatry154(9):1323–1325.
Barkley, R. A., Biederman, J. (1997). Toward a broader definition of the age-of-onset criterion forattention-deficit hyperactivity disorder. Journal of American Academy of Child and AdolescentPsychiatry 36(9):1204–1210.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

Adult ADHD and Substance Abuse 1975
Beurrier, C., Malenka, R. C. (2002). Enhanced inhibition of synaptic transmission by dopaminein the nucleus accumbens during behavioral sensitization to cocaine. Journal of Neuroscience22(14):5817–5822.
Biederman, J. (2003). Pharmacotherapy for attention-deficit/hyperactivity disorder (ADHD) decreasesthe risk for substance abuse: findings from a longitudinal follow-up of youths with and withoutADHD. Journal of Clinical Psychiatry 64(Supp.) 11:3–8.
Biederman, J. (2004). Impact of comorbidity in adults with attention-deficit/hyperactivity disorder.Journal of Clinical Psychiatry 65 (Suppl. 3):3–7.
Biederman, J., Faraone, S. V., Spencer, T., Wilens, T., Norman, D., Lapey, K. A., Mick, E., Lehman,B. K., Doyle, A. (1993). Patterns of psychiatric comorbidity, cognition, and psychosocial func-tioning in adults with attention deficit hyperactivity disorder. American Journal of Psychiatry150(12):1792–1798.
Biederman, J., Mick, E., Faraone, S. V. (2000). Age-dependent decline of symptoms of attention deficithyperactivity disorder: impact of remission definition and symptom type. American Journal ofPsychiatry 157(5):816–818.
Biederman, J., Wilens, T., Mick, E., Milberger, S., Spencer, T. J., Faraone, S. V. (1995). Psychoactivesubstance use disorder in adults with attention deficit hyperactivity disorder (ADHD): effects ofADHD and psychiatric comorbidity. American Journal of Psychiatry 152(11):1652–1658.
Biederman, J., Wilens, T., Mick, E., Spencer, T., Faraone, S. V. (1999). Pharmacotherapy of attention-deficit hyperactivity disorder reduces risk for substance use disorder. Pediatrics 104(2):20.
Brooks, D. B., Kalbag, A. S., Vosburg, S. K., Evans, S. M., Levin, F. R. Assessment of CognitiveFunctioning of Methadone-Maintenance Patients: Impact of Adult ADHD and Current CocaineDependence. (Manuscript submitted, 2005).
Brown, T. E. (1996). Brown Attention-Deficit Disorder Scales. San Antonio, TX: The PsychologicalCorporation.
Bush, G., Frazier, J. A., Rauch, S. L., Seidman, L. J., Whalen, P. H., Jenike, M. A., Rosen, B. R.,Biederman, J. (1999). Anterior cingulated cortex dysfunction in attention-deficit hyperactivitydisorder revealed by fMRI and the counting stroop. Biological Psychiatry 45(12):1542–1552.
Carroll, K. M., Rounsaville, B. J. (1993). History and significance of childhood attention deficitdisorder in treatment-seeking cocaine abusers. Comprehensive Psychiatry 34(2):75–82.
Carter, C. S., Krener, P., Chaderjian, M., Northcutt, C., Wolfe, V. (1995). Asymmetrical visual-spatialattentional performance in ADHD: evidence for a right hemispheric deficit. Biological Psychiatry37(11):789–797.
Cavanagh, R., Clifford, J. S., Gregory, W. L. (1989). The use of bromocriptine for the treatment ofattention deficit disorder in two chemically dependent patients. Journal of Psychoactive Drugs21(2):217–220.
Clure, C., Brady, K. T., Saladin, M. E., Johnson, D., Waid, R., Rittenbury, M. (1999). Attention-deficit/hyperactivity disorder and substance use: symptom pattern and drug choice. AmericanJournal of Drug and Alcohol Abuse 25(3):441–448.
Cocores, J. A., Davies, R. K., Mueller, P. S., Gold, M. S. (1987). Cocaine abuse and adult attentiondeficit disorder. Journal of Clinical Psychiatry 48(9):376–377.
Conners, C. K., Erhart, D., Sparrow E. (1999). Conners’Adult ADHD Rating Scales, Technical Manual.New York: Multi-Health Systems.
Cook, E. H. Jr., Stein, M. A., Krasowski, M. D., Cox, N. J., Olkon, D. M., Kieffer, J. E., Leventhal, B.L. (1995). Association of attention-deficit disorder and the dopamine transporter gene. AmericanJournal of Human Genetics 56(4):993–998.
Dansereau, D. F., Joe, G. W., Simpson, D. D. (1995). Attentional difficulties and the effectivenessof a visual representation strategy for counseling drug-addicted clients. International Journal ofthe Addictions 30(4):371–86.
Dupaul, G., Power, T., Anastopoulos, A., Reid, R. (1998). ADHD Rating Scale, IV: Checklists, Normsand Clinical Interpretation. New York: Guilford Press.
Epstein, J. N., Johnson, D. E., Conners, C. K. (2001). Conners’ Adult ADHD Diagnostic Interviewfor DSM-IV (CAADID). North Tonawanda, NY: Multi-Health Systems Inc.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1976 Kalbag and Levin
Ernst, M., Zametkin, A. J., Phillips, R. L., Cohen, R. M. (1998). Age-related changes in brain glu-cose metabolism in adults with attention-deficit hyperactivity disorder and control subjects.Journal of Neuropsychiatry and Clinical Neurosciences 10(2):168–177.
Eyre, S. L., Rounsaville, B. J., Kleber, H. D. (1982). History of childhood hyperactivity in a clinicpopulation of opiate addicts. Journal of Nervous and Mental Disease 170(9):522–529.
Faraone, S. V., Biederman, J., Spencer, T., Wilens, T., Seidman, L. J., Mick, E., Doyle, A. E. (2000).Attention-deficit/ hyperactivity disorder in adults: an overview. Biological Psychiatry 48(1):9–20.
Faraone, S. V., Biederman, J., Weiffenbach, B., Keith, T., Chu, M. P., Weaver, A., Spencer, T. J.,Wilens, T. E., Frazier, J., Cleves, M., Sakai, J. (1999). Dopamine D4 gene 7-repeat allele andattention deficit hyperactivity disorder. American Journal of Psychiatry 156(5):768–770.
Findling, R. L., Schwartz, M. A., Flannery, D. J., Manos, M. J. (1996). Venlafaxine in adults withattention-deficit hyperactivity disorder an open clinical trial. Journal of Clinical Psychiatry57(5):184–189.
Flory, K., Milich, R., Lynam, D. R., Leukefeld, C., Clayton, R. (2003). Relation between childhooddisruptive behavior disorders and substance use and dependence symptoms in young adulthood:individuals with symptoms of attention-deficit hyperactivity disorder and conduct disorder areuniquely at risk. Psychology of Addictive Behaviors 17(2):151–158.
Gill, M., Daly, G., Heron, S., Hawi, Z., Fitzgerald, M. (1997). Confirmation of association betweenattention deficit hyperactivity disorder and a dopamine transporter polymorphism. MolecularPsychiatry 2(4):311–313.
Gittleman, R., Mannuzza, S., Shenker, R., Bonagura, N. (1985). Hyperactive boys almost grown up.I. Psychiatric status. Archives of General Psychiatry 42(10):937–947.
Greenfield, B., Hechtman, L., Weiss, G. (1988). Two subgroups of hyperactives as adults: correlationsof outcome. Canadian Journal of Psychiatry 33(6):505–508.
Greenhill, L. L. (1992). Pharmacologic treatment of attention deficit hyperactivity disorder. Psychi-atric Clinics of North America 15(1):1–27.
Grodzinsky, G. M., Barkley, R. A. (1999). Predictive power of frontal lobe tests in the diagnosis ofattention-deficit hyperactivity disorder. Archives of Clinical Neuropsychology 13(1):12–21.
Hechtman, L., Greenfield, B. (2003). Long-term use of stimulants in children with attention deficithyperactivity disorder: safety, efficacy, and long-term outcome. Pediatric Drugs 5(12):787–794.
Hedges, D., Reimherr, F. W., Rogers, A., Strong, R., Wender, P. H. (1995). An open trial of venlafax-ine in adult patients with attention- deficit hyperactivity disorder. Psychopharmacol Bulletin31(4):779–783.
Hesslinger, B., Tebartz van Elst, L., Nyberg, E., Dykierek, P., Richter, H., Berner, M., Ebert, D.(2002). Psychotherapy of Attention deficit hyperactivity disorder in adults: a pilot study using astructured skills training program. European Archives of Psychiatry and Clinical Neuroscience252(4):177–184.
Hien, D., Matzner, F., First, M., Spitzer, R., Williams, J., Gibbon, M. (2001). The Structured ClinicalInterview for DSM-IV, Childhood version (KID-SCID). Unpublished instrument, 2001 (revised).
Higgins, S. T. Budney, A. J. Bickel, W. K. Foerg, F. E. Donham, R., Badger, G. J. (1994). Incentivesimprove outcome in outpatient behavioral treatment for cocaine dependence. Archives of GeneralPsychiatry 51(7):568–576.
Hill, J. C., Schoener, E. P. (1996). Age-dependent decline of attention deficit hyperactivity disorder.American Journal of Psychiatry 153(9):1143–1146.
Hoffman, B. B., Lefkowitz, R. J. (1996). Catecholamines, sympathomimetic drugs and adrenergicreceptor agonists. In Jardman, J. G., et al., eds. Goodman & Gilman’s The PharmacologicalBasis of Therapeutics. New York: McGraw-Hill, pp. 199–263.
Horrigan, J. P., Barnhill, L. J. (2000). Low-dose amphetamine salts and adult attention-deficit/hyperactivity disorder. Journal of Clinical Psychiatry 61(6):414–417.
Kalbag, A. S., Brooks, D. J., Evans, S. M., Nunes, E. V., Levin, F. R. The relationship between thespecific and non-specific ADHD symptoms and addiction severity in a methadone-maintainedsample of adults with ADHD. Manuscript in preparation.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

Adult ADHD and Substance Abuse 1977
Kessler, R.C., McGonagle, K. A., Shao, S., Nelson, C. B., Hughes, M., Eshleman, S., Wittchen, H. U.,Kendler, K. S. (1994). Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders inthe United States. Results from the National Comorbidity Survey. Archives of General Psychiatry51(1):8–19.
Khantzian, E. J. (1983). An extreme case of cocaine dependence and marked improvement withmethylphenidate treatment. American Journal of Psychiatry 140(6):784–785.
Khantzian, E. J., Gawin, F., Kleber, H. D., Riordan, C. E. (1984). Methylphenidate (Ritalin) treatmentof cocaine dependence a preliminary report. Journal of Substance Abuse Treatment 1(2):107–112.
King, V. L., Brooner, R. K., Kidorf, M. S., Stoller, K. B., Mirsky, A. F. (1999). Attention deficithyperactivity disorder and treatment outcome in opioid abusers entering treatment. Journal ofNervous and Mental Disease 187(8):487–495.
Kuperman, S., Perry, P., Gaffney, G., Lund, B., Bever-Stille, K., Arndt, S., Holman, T. L., Moser, D.,Paulsen, J. (2001). Bupropion SR vs. methylphenidate vs. placebo for attention deficit hyperac-tivity disorder in adults. Annals of Clinical Psychiatry 13(3):129–134.
LaHoste, G. J., Swanson, J. M., Wigal, S. B., Glabe, C., Wigal, T., King, N., Kennedy, J. L. (1996).Dopamine D4 receptor gene polymorphism is associated with attention deficit hyperactivitydisorder. Molecular Psychiatry 1(2):121–124.
Lambert, N. M., Hartsough, C. S. (1998). Prospective study of tobacco smoking and substance depen-dencies among samples of ADHD and non-ADHD participants. Journal of Learning Disabilities31(6):533–544.
Levin, F. R., Evans, S. M., Kleber, H. D. (1998). Prevalence of adult attention-deficit hyperactivitydisorder among cocaine abusers seeking treatment. Drug and Alcohol Dependence 52(1):15–25.
Levin, F. R., Evans, S. M., McDowell, D. M., Brooks, D. J., Nunes, E. (2002). Bupropion treatmentfor cocaine and adult attention-deficit hyperactivity disorder. Journal of Addictive Disorders21(2):1–16.
Levin, F. R., Evans, S. M., McDowell, D. M., Kleber, H. D. (1998). Methylphenidate treatmentfor cocaine abusers with adult attention-deficit/hyperactivity disorder: a pilot study. Journal ofClinical Psychiatry 59(6):300–305.
Levin, F. R., Evans, S. M., Vosburg, S. K., Horton, T., Brooks, D., Ng, J. (2004). Impact of attentiondeficit hyperactivity disorder and other psychopathology on treatment retention among cocaineabusers in a therapeutic community. Addictive Behaviors 29(9):1875–1882.
Levin, F. R., Kleber, H. D. (1995). Attention-deficit hyperactivity disorder and substanceabuse: relationship and implications for treatment. Harvard Review of Psychiatry 2(5):246–258.
Linehan, M. M., Armstrong, H. E., Suarez, A., Allmon, D., Heard, H. L. (1991). Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Archives of General Psy-chiatry 48(12):1060–1064.
Linehan, M. M., Schmidt, H. 3rd, Dimeff, L. A., Craft, J. C., Kanter, J., Comtois, K. A. (1999). Di-alectical behavior therapy of patients with borderline personality disorder and drug-dependence.American Journal on Addictions 8(4):279–292.
Lovejoy, D. W., Ball, J. D., Keats, M., Stutts, M. L., Spain, E. H., Janda, L., Janusz, J. (1999). Neu-ropsychological performance of adults with attention-deficit hyperactivity disorder (ADHD):diagnostic classification estimates for measures of frontal lobe/executive functioning. J Int Neu-ropsychol Soc 5(3):222–233.
Lowe, N., Kirley, A., Hawi, Z., Sham, P., Wickham, H., Kratochvil, C. J., Smith, S. D., Lee, S. Y.,Levy, F., Kent, L., Middle, F., Rohde, L. A., Roman, T., Tahir, E., Yazgan, Y., Asherson, P.,Mill, J., Thapar, A., Payton, A., Todd, R. D., Stephens, T., Ebstein, R. P., Manor, I., Barr, C.L., Wiggs, K. G., Sinke, R. J., Buitelaar, J. K., Smalley, S. L., Nelson, S. F., Biederman, J.,Faraone, S. V., Gill, M. (2004). Joint analysis of the DRD5 marker concludes associations withattention-deficit hyperactivity disorder confined to the predominantly inattentive and combinedsubtypes. American Journal of Human Genetics 74(2):348–356.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1978 Kalbag and Levin
Mannuzza, S., Klein, R. G. (2000). Long-term prognosis in attention-deficit hyperactivity disorder.Child and Adolescent Pediatric Clinics of North America 9(3):711–726.
Mannuzza, S., Klein, R. G., Bessler, A., Malloy, P., Hynes, M. E. (1997). Educational and occupationaloutcome of hyperactive boys grown up. Journal of American Academy of Child AdolescentPsychiatry 36(9):1222–1227.
Mannuzza, S., Klein, R. G., Bessler, A., Malloy, P., LaPadula, M. (1993). Adult outcome of hyperactiveboys. Educational achievement, occupational rank, and psychiatric status. Archives of GeneralPsychiatry 50(7):565–576.
Mannuzza, S., Klein, R. G., Bessler, A., Malloy, P., LaPadula, M. (1998). Adult psychiatric status ofhyperactive boys grown up. American Journal of Psychiatry 155(4):493–498.
Mannuzza, S., Klein, R. G., Bonagura, N., Malloy, P., Giampino, T. L., Addalli, K. A. (1991). Hyper-active boys almost grown up. V. Replication of psychiatric status. Archives of General Psychiatry48(1):77–83.
Mannuzza, S., Klein, R. G., Moulton, J. L. (2003). Does stimulant treatment place children at riskfor adult substance abuse? A controlled, prospective follow-up study. Journal of Child andAdolescent Psychopharmacology 13(3):273–282.
Mannuzza, S., Klein, R. G., Moulton, J. L. (2003). Persistence of attention-deficit/hyperactivity dis-order into adulthood: what have we learned from the prospective follow-up studies? Journal ofAttention Disorders 7(2):93–100.
Mattes, J. A., Boswell, L., Oliver, H. (1984). Methylphenidate effects on symptoms of attention deficitdisorder in adults. Archives of General Psychiatry 41(11):1059–1063.
Michelson, D., Adler, L., Spencer, T., Reimherr, F. W., West, S. A., Allen, A. J., Kelsey, D., Wernicke,J., Dietrich, A., Milton, D. (2003). Atomoxetine in adults with ADHD: two randomized, placebo-controlled studies. Biological Psychiatry 53:112–120.
Milberger, S., Biederman, J., Faraone, S. V., Wilens, T., Chu, M. P. (1997). Associations betweenADHD and psychoactive substance use disorders. Findings from a longitudinal study of high-risk siblings of ADHD children. American Journal on Addictions 6(4):318–329.
MTA cooperative group. (1999). A 14-month randomized clinical trial of treatment strategies forattention-deficit/hyperactivity disorder. The MTA cooperative group. Multimodal treatmentstudy of children with ADHD. Archives of General Psychiatry 56(12):1073–1086.
Murphy, K. R., Barkley, R. A., Bush, T. (2002). Young adults with attention-deficit hyperactivitydisorder: subtype differences in comorbidity, educational and clinical history. Journal of Nervousand Mental Disease 190(3):147–157.
Niederhofer, H. (2003). An open trial of busiprone in the treatment of attention-deficit disorder. HumanPsychopharmacology 18(6):489–492.
Orvaschel, H. (1985). Psychiatric interviews suitable for use in research with children and adolescents.Psychopharmacol Bulletin 21(4):737–745.
Paternite, C. E., Loney, J., Salisbury, H., Whaley, M. A. (1999). Childhood inattention-overactivity,aggression, and stimulant medication history as predictors of young adult outcomes. Journal ofChild and Adolescent Psychopharmacology 9(3):169–184.
Paterson, R., Douglas, C., Hallmayer, J., Hagan, M., Krupenia, Z. (1999). A randomized, double-blind, placebo-controlled trial of dexamphetamine in adults with attention deficit hyperactivitydisorder. Australian and New Zealand Journal of Psychiatry 33(4):494–502.
Pelham, W. E., Sams, S. E. (1992). Behavior modification. In G Weiss, ed. Child and AdolescentPsychiatric Clinics of North America. Philadelphia, PA: W. B. Saunders, pp. 505–518.
Pomeraleau, O. F., Downey, K. K., Stelson, F. W., Pomeraleau, C. S. (1995). Cigarette smoking inadult patients diagnosed with attention deficit hyperactivity disorder. Journal of Substance Abuse7(3):373–378.
Regier, D.A., Farmer, M. E., Rae, D. S., Locke, B. Z., Keith, S. J., Judd, L. L., Goodwin, F. K. (1990).Comorbidity of mental disorders with alcohol and other drug abuse. Results form the Epidemi-ologic Catchment Area (ECA) Study. Journal of American Medical Association 264(19):2511–2518.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

Adult ADHD and Substance Abuse 1979
Rounsaville, B. J., Anton, S. F., Carroll, K., Budde, D., Prusoff, B. A., Gawin, F. (1991). Psychiatricdiagnosis of treatment-seeking cocaine abusers. Archives of General Psychiatry 48(1):43–51.
Rubia, K., Overmeyer, S., Taylor, E., Brammer, M., Williams, S. C., Simons, A., Bullmore, E. T.(1999). Hyprofrontality in attention-deficit hyperactivity disorder during higher-order motorcontrol, a study with functional MRI. American Journal of Psychiatry 156(6):891–896.
Rugino, T. A., Samsock, T. C. (2003). Modafinil in children with attention-deficit hyperactivitydisorder. Pediatric Neurology 29(2):136–142.
Schubiner, H., Saules, K. K., Arfken, C. L., Johanson, C. E., Schuster, C. R., Lockhart, N., Edwards,A., Donlin, J., Philgren, E. (2000). Double-blind placebo-controlled trial of methylphenidate inthe treatment of adult ADHD patients with comorbid cocaine dependence. Experimental andClinical Psychopharmacology 10(3):286–294.
Schweitzer, J. B., Faber, T. L., Grafton, S. T., Tune, L. E., Hoffman, J. M., Kilts, C. D. (2000).Alterations in the functional anatomy of working memory in adult attention deficit hyperactivitydisorder. American Journal of Psychiatry 157(2):278–280.
Seidman, L. J., Biederman, J., Weber, W., Hatch, M., Faraone, S. V. (1998). Neuropsychologicalfunction in adults with attention-deficit hyperactivity disorder. Biological Psychiatry 44(4):260–268.
Sohlberg, M. M., Mateer, C. A. (2001). Improving attention and managing attentional problems.Adapting rehabilitation techniques to adults with ADD. Annals of the New York Academy ofSciences 931:359–375.
Somoza, E., Bridge, P., Winhusen, T., Rotrosen, J., Vanderburg, D., Harrer, J., Mezinskis, J.,Montgomery, A., Leiderman, D., Locastro, J., Wulsin, L., Barrett, J. (2000). An open-labelpilot study of methylphenidate in the treatment of cocaine-dependence patients with attentiondeficit hyperactivity disorder. Drug and Alcohol Dependence 60(1):S208.
Spencer, T., Biederman, J., Wilens, T., Faraone, S., Prince, J., Gerard, K., Doyle, R., Parekh, A.,Kagan, J., Bearman, S. K. (2001). Efficacy of a mixed amphetamine salts compound in adultswith attention-deficit hyperactivity disorder. Archives of General Psychiatry 58(8):775–782.
Spencer, T., Biederman, J., Wilens, T., Prince, J., Hatch, M., Jones, J., Harding, M., Faraone, S. V.,Seidman, L. (1998). Effectiveness and tolerability of tomoxetine in adults with attention-deficithyperactivity disorder. American Journal of Psychiatry 155(5):693–695.
Spencer, T., Wilens, T., Biederman, J., Faraone, S. V., Ablon, J. S., Lapey, K. (1995). A double-blind, crossover comparison of methylphenidate and placebo in adults with childhood-onsetattention-deficit hyperactivity disorder. Archives of General Psychiatry 52(6):434–443.
Stevenson, C. S., Whitmont, S., Bornholt, L., Livesey, D., Stevenson, R. J. (2002). A cognitiveremediation programme for adults with attention-deficit hyperactivity disorder. Australian andNew Zealand Journal of Psychiatry 36(5):610–616.
Sullivan, M., Levin, F. R. (2001). Attention deficit/hyperactivity disorder and substance abuse: diag-nostic and therapeutic considerations. In Adult Attention Deficit Disorder: Brain Mechanismsand Life Outcomes. J. Wasserstein, Wolf, L. E., Lefever, F. F., (eds). Annals of the New YorkAcademy of Sciences 931:251–270.
Szatmari, P. (1992). The epidemiology of attention-deficit hyperactivity disorder. In G. Weiss, guested. Child and Adolescent Psychiatric Clinics of North America pp. 361–384.
Taylor, F. B., Russo, J. (2000). Efficacy of modafinil compared to dextroamphetamine for the treatmentof attention deficit hyperactivity disorder in adults. Journal of Child and Adolescent Psychophar-macology 10(4):311–320.78.
Taylor, F., Russo, J. (2001). Comparing guanfacine and dextroamphetamine for the treatment of adultattention-deficit/hyperactivity disorder. Journal of Psychopharmacology 21(2):223–228.
Thompson, L. L., Riggs, P. D., Mikulich, S. K., Crowley, T. J. (1996). Contribution and ADHDsymptoms to substance problems and delinquency conduct-disordered adolescents. Journal ofAbnormal Child Psychology 24(3):325–347.
Vaidya, C. J., Austin, G., Kirkorian, G., Ridlehuber, H. W., Desmond, J. E., Glover, G. H., Gabrieli,J. D. (1998). Selective effects of methylphenidate in attention-deficit hyperactivity disorder: a
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

1980 Kalbag and Levin
functional magnetic resonance study. Proceeding of the National Academy of Sciences of theUnited States of America 95(24):14494–14499.
Ward, M. F., Wender, P. H., Reimherr, F. W. (1993). The Wender Utah Rating Scale: an aid in theretrospective diagnosis of childhood attention deficit hyperactivity disorder. American Journalof Psychiatry 150(6):885–890.
Weinstein, C. S. (1994). Cognitive remediation strategies: an adjunct to the psychotherapy of adultswith attention-deficit hyperactivity disorder. Journal of Psychotherapy Practice and Research,3:44–57.
Weiss, G., Hechtman, L. T. (1986). Adult hyperactive subjects’ view of their treatment in child-hood and adolescence. In Hyperactive Children Grown Up: Empirical Finding and TheoreticalConsiderations. Guilford. New York: pp. 293–300.
Weiss, M., Hechtman, L. T., Weiss, G. (1999). ADHD in Adulthood: A Guide to Current Theory,Diagnosis, and Treatment. Baltimore, MD: The Johns Hopkins University Press.
Wender, P. H. (1995). Attention-Deficit Hyperactivity Disorder in Adults. New York: Oxford UniversityPress.
Wender, P. H., Ward, M. F., Reimherr, F. W., Marchant, B. K. (2000). ADHD in adults. Journal ofAmerican Academy of Child Adolescent Psychiatry 39(5):543.
West, S. L., Mulsow, M., Arrendondo, R. (2003). Factor analysis of attention deficit scales for adults(ADSA) in a clinical sample of outpatient substance abusers. American Journal on Addictions12(2)159–165.
Wilens, T. E., Biederman, J., Abrantes, A. M., Spencer, T. J. (1997). Clinical characteristics ofpsychiatrically referred adolescent outpatients with substance use disorder. Journal of AmericanAcademy of Child Adolescent Psychiatry 36:941–947.
Wilens, T. E., Biederman, J., Prince, J., Spencer, T. J., Faraone, S. V., Warburton, R., Schleifer, D.,Harding, M., Linehan, C., Geller, D. (1996). Six-week, double-blind, placebo-controlled studyof desipramine for adult attention deficit hyperactivity disorder. American Journal of Psychiatry153(9):1147–1153.
Wilens, T. E., Biederman, J., Spencer, T. J. (1995). Venlafaxine for adult ADHD. American Journalof Psychiatry 152(7):1099–1100.
Wilens, T. E., Biederman, J., Spencer, T. J., Bostic, J., Prince, J., Monuteaux, M. C., Soriano, J.,Fine, C., Abrams, A., Rater, M., Polisner, D. (1999). A pilot controlled clinical trial of ABT-418, a cholinergic agonist in the treatment of adults with attention deficit hyperactivity disorder.American Journal of Psychiatry 156(12):1931–1937.
Wilens, T. E., Biederman, J., Spencer, T. J., Frazier, J., Prince, J., Bostic, J., Rater, M., Soriano, J.,Hatch, M., Sienna, M., Millstein, R. B., Abrantes, A. (1999). Controlled trial of high doses ofpemoline for adults with attention deficit/hyperactivity disorder. Journal of Clinical Psychophar-macology 19(3):257–264.
Wilens, T. E., Biederman, J., Spencer, T. J., Prince, J. (1995). Pharmacotherapy of adult attentiondeficit-hyperactivity disorder: a review. Journal of Clinical Psychopharmacology 15(4):270–279.
Wilens, T. E., Faraone, S. V., Biederman, J., Gunawardene, S. (2003). Does stimulant therapy ofattention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review ofthe literature. Pediatrics 111(1):179–185.
Wilens, T. E., Spencer, T. J., Biederman, J., Girard, K., Doyle, R., Prince, J., Polsiner, D., Sohlkhah,R., Comeau, S., Monuteaux, M. C., Parekh, A. (2001). A controlled clinical trial of bupropion forattention deficit hyperactivity disorder in adults. American Journal of Psychiatry 158(2):282–288.
Wise, B. K., Cuffe, S. P., Fischer, T. (2001). Dual Diagnosis and successful participation of adolescentsin substance abuse treatment. Journal of Substance Abuse Treatment 1:161–165.
Wise, R. A. (1998). Drug-activation of brain reward pathways. Drug and Alcohol Dependence 51(1–2):13–22.
Wonnacott, S., Irons, J., Rapier, C., Thorne, B., Lunt, G. G. (1989). Presynaptic modulation oftransmitter release by nicotinic receptors. Progress in Brain Research 79:157–163.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.

Adult ADHD and Substance Abuse 1981
Wood, D., Wender, P. H., Reimherr, F. W. (1983). The prevalence of attention deficit disorder, residualtype, or minimal brain dysfunction, in a population of male alcoholic patients. American Journalof Psychiatry 140(1):95–98.
Zametkin, A. J., Liebenauer, L. L., Fitzgerald, G. A., King, A. C., Minkunas, D. V., Herscovitch,P., Yamada, E. M., Cohen, R. M. (1993). Brain metabolism in teenagers with attention-deficithyperactivity disorder. Archives of General Psychiatry 50(5):333–340.
Zametkin, A. J., Nordahl, T. E., Gross, M., King, A. C., Semple, W. E., Rumsey, J., Hamburger, S.,Cohen, R. M. (1990). Cerebral glucose metabolism in adults with hyperactivity for childhoodonset. New England Journal of Medicine 323(20):1361–1366.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
6/14
For
pers
onal
use
onl
y.














