Embed Size (px)
Citation preview

790
Adrenergic Effects on the Biology of the AdultMammalian CardiocyteDouglas L. Mann, MD; Robert L. Kent, PhD;
Bruce Parsons, PhD; and George Cooper IV, MD
Background. To delineate the mechanism(s) of catecholamine-mediated cardiac toxicity, weexposed cultures of adult cardiac muscle cells, or cardiocytes, to a broad range of norepineph-rine concentrations.Methods and Results. Norepinephrine stimulation resulted in a concentration-dependent
decrease in cardiocyte viability, as demonstrated by a significant decrease in viable rod-shapedcells and a significant release of creatine kinase from cells in norepinephrine-treated cultures.Norepinephrine-mediated cell toxicity was attenuated significantly by ,-adrenoceptor blockadeand mimicked by selective stimulation of the ,B-adrenoceptor, whereas the effects mediated bythe a-adrenoceptor were relatively less apparent. When norepinephrine stimulation wasexamined in terms of cardiocyte anabolic activity, there was a concentration-dependentdecrease in the incorporation of [3H]phenylalanine and [3H]uridine into cytoplasmic proteinand nuclear RNA, respectively. The decrease in cytoplasmic labeling was largely attenuated byf-adrenoceptor blockade and mimicked by selective stimulation of the ,B-adrenoceptor, buta-adrenoceptor stimulation resulted in relatively minor decreases in cytoplasmic labeling. Thenorepinephrine-induced toxic effect appeared to be the result of cyclic AMP-mediated calciumoverload of the cell, as suggested by studies in which pharmacological strategies that increasedintracellular cyclic AMP led to decreased cell viability, as well as studies that showed that influxof extracellular calcium through the verapamil-sensitive calcium channel was necessary for theinduction of cell lethality. Additional time-course studies showed that norepinephrine caused a
rapid, fourfold increase in intracellular cyclic AMP, followed by a 3.2-fold increase inintracellular calcium ([Ca2+]i).
Conclusions. These results constitute the initial demonstration at the cellular level thatadrenergic stimulation leads to cyclic AMP-mediated calcium overload of the cell, with a
resultant decrease in synthetic activity and/or viability. (Circulation 1992;85:790-804)
It is well recognized that the sympathetic nervoussystem has a major role in the cardiovascularresponse to stress.' However, a number of
studies have shown that excessive adrenergic stimu-lation can aggravate or even produce, rather thanameliorate, various manifestations of cardiovascular
From the Cardiology Section of the Department of Medicineand the Department of Physiology, Gazes Cardiac ResearchInstitute Medical University of South Carolina; and the VeteransAdministration Medical Center, Charleston, S.C.
Supported by National Institutes of Health grants HL-29146,HL-38124, and HL-39176 and by research funds from the VeteransAdministration. D.L.M. is the recipient of a Clinical InvestigatorAward from the National Heart, Lung, and Blood Institute. G.C.is the recipient of a Clinical Investigator Award from the VeteransAdministration.Address for correspondence: Douglas L. Mann, MD, Cardiology
Section, VA Medical Center, 2002 Holcombe Blvd., Houston, TX,77030.Address for reprints: George Cooper IV, MD, Cardiology Sec-
tion, VA Medical Center, 109 Bee Street, Charleston, SC 29403.Received September 12, 1990; revision accepted October 1, 1991.
disease. Catecholamine-mediated myocardial injuryhas been documented in patients with pheochromo-cytoma,2 hyperthyroidism,3 myocardial infarction,4.5and, more recently, congestive heart failure.6 Giventhe potential importance of catecholamine-mediatedcardiotoxic effects in humans, a number of experi-mental studies have sought to determine the mecha-nism(s) responsible for catecholamine-induced car-diac injury.7-29 However, although these in vivostudies have yielded important insights into the gen-esis of catecholamine cardiotoxicity, no definitivemechanism has been identified.One of the major problems in defining the mech-
anism(s) of catecholamine cardiotoxicity in vivo is thecomplex alterations in cardiac loading and blood flowinherent in all such in vivo experimental models.Thus, one cannot fully dissociate any direct toxiceffects of the catecholamine from any concurrentcardiac injury that may be produced by mechanicaloverloading and/or ischemia. A second major prob-
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

Mann et al Cardiocyte Adrenergic Regulation 791
lem in defining these mechanism(s) results from thecomplexity of cardiac tissue, which comprises cardiacmuscle cells, or cardiocytes, admixed with interstitial,neural, and vascular cells. Given that adrenergicstimulation could lead to multiple cell-cell interac-tions, it becomes very difficult to isolate and preciselydefine the direct biological effects of catecholamineson the cardiocyte component of the heart.To provide a more focused approach to defining the
proximate mechanism(s) causing catecholamine-induced toxicity, we used a very simple experimentalpreparation-the isolated cultured adult mammaliancardiocyte-to examine the direct effects of norepi-nephrine on the biology of this cell. The results of thepresent study directly support the view that catechol-amine cardiotoxicity is the result of cyclic AMP(cAMP) -mediated calcium overload of the cardiocyte.
MethodsCardiocyte IsolationWith the exceptions noted below, the methods
used to obtain reproducible yields of calcium-toler-ant cardiocytes have been described previously.30Briefly, adult cats of either sex, weighing 1.4-3.8 kg,were anesthetized with ketamine hydrochloride (50mg/kg i.m.) and acepromazine maleate (5 mg/kgi.m.) and submitted to rapid cardiectomy understerile conditions. The aorta was then cannulated,and the coronary arteries were perfused retrogradefor 10 minutes with a recirculating modified Krebs-Henseleit buffer (KHB) of the following composition(mm): NaCl 130.0, KCI 4.8, MgSO4 1.2, NaH2PO4 1.2,NaHCO3 4.0, CaCl2 0.5, HEPES 10.0, and glucose12.5. This was followed by a nonrecirculating bufferof the same composition but without supplementalcalcium and concluded with a nonrecirculating calci-um-free buffer supplemented with type II collagen-ase (155 units/ml). Perfusion was terminated whenthe heart was flaccid. The heart was then removedfrom the cannula, the ventricles were separated fromthe atria, and the ventricular cardiocytes were iso-lated as described previously.30
Cardiocyte CultureThe characteristics of the cell culture system used
herein have been reported in detail.30 An importantfeature of this model that bears emphasis is thatadult feline cardiocytes remain quiescent (noncon-tracting) for extended periods of time when main-tained in standard serum-free culture conditions.Indeed, the initiation of spontaneous contractions inthese cells usually indicates that they have becomenonviable.31
Unless specified otherwise, the culture medium usedwas medium 199 (Earle's salts, 0.30 mM DL-phenylala-nine, 1.8 mM calcium) supplemented with 10-6 Minsulin, 6.25 ,g/ml transferrin, 6.25 ng/ml selenium,5.35 1£g/ml linoleic acid, 1.2 p£g/ml albumin, 100units/ml penicillin, and 6.8x 10` M streptomycin. Ateach medium change, 100 /M ascorbic acid was added
to retard oxidation of any added catecholamine. Tominimize fibroblast contamination, selective adhesiontechniques were used; fibroblast contamination is <2%with this method.30 Cardiocytes were kept in a 37°Chumidified incubator equilibrated with 5% CO2 toachieve a final medium pH of 7.30-7.35.
Experimental ProtocolsTo determine the effects of norepinephrine expo-
sure in vitro, cell cultures were treated continuouslyfor 72 hours with graded concentrations of adrener-gic agonists and antagonists. The selected range ofadrenergic agonist concentrations was based on pre-vious reports that showed that such levels are attain-able at the neural cleft or available as circulatinglevels under certain pathological conditions.32-34 Foradrenergic antagonists, the selected concentrationswere based on reported values,35,36 as well as onstudies described below in which we determined theconcentration of antagonist necessary to block thenorepinephrine-mediated increase in cAMP.A 2-ml suspension of freshly isolated cardiocytes
was plated at a final concentration of 1x 104 cells/mlonto laminin-coated (20 ,ug/ml) coverslips in 35 mmpolystyrene petri dishes. Beginning on the first day inculture, the cardiocytes were exposed continuously toconcentrations of norepinephrine ranging from 10`to 10-6 M; each dish was treated with a singleconcentration of norepinephrine. Control cultureswere treated with an equal volume of diluent. Me-dium changes were performed on the first and seconddays of culture, at which time freshly prepared ad-renergic agents or a diluent was added. After 24hours, the norepinephrine concentration as mea-sured by high-performance liquid chromatographyremained at least 80% of the original value. On thethird day of culture, all dishes were labeled eitherwith 40 ,Ci/ml [3H]phenylalanine or 5 ,uCi/ml [3H]u-ridine to determine their incorporation into cellularprotein or nuclear RNA, respectively.
In a second series of experiments, we examined theeffect of norepinephrine on cardiocytes whose 13-and/or a-adrenoceptors were blocked before adren-ergic stimulation. For these experiments, the cellswere pretreated for 1 hour with the nonselective13-antagonist propranolol (range, 10-9 to 10-6 M) orwith the nonselective a-antagonist phentolamine(range, 10-8 to 10` M); for studies using combined,B- and a-adrenergic blockade, the cells were pre-treated for 1 hour with both 10-6 M propranolol and10-5 M phentolamine. After adrenoceptor blockade,the cells were treated with 1 gM norepinephrine; themedium was changed on the first and second days inculture, and fresh solutions of adrenergic agonistsand antagonists were applied. Each experimental setin this series comprised a negative control grouptreated with diluent only, a control group treatedwith the maximum concentration of adrenergic an-tagonist(s) used, and additional groups that receivedboth 1 gM norepinephrine and incremental concen-trations of adrenergic antagonists; each culture dish
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

792 Circulation Vol 85, No 2 February 1992
was treated with a single concentration of adrenergicagonist and antagonist. After 72 hours of continuoustreatment with adrenergic agonists and antagonists,the cells were labeled for 6 hours with 40 ,uCi/ml[3H]phenylalanine.
In a third series of experiments, designed to ad-dress the separate effects of /3- or a-adrenoceptorstimulation, the cardiocytes were stimulated withincremental concentrations of the nonselective /3-ad-renergic agonist isoproterenol (range, 10-10 to 10`M) or incremental concentrations of the a1-adrener-gic agonist phenylephrine (range, 10`8 to 10` M);control cultures were treated with an equal volume ofdiluent. Each experimental set always consisted of acontrol group and an experimental group treatedwith an adrenergic agonist. The preparation, main-tenance, and labeling with [3H]phenylalanine wereidentical to those in the protocols described above.
Cardiocyte EvaluationCell viability. For the studies in which cells were
exposed continuously to adrenergic agonists and/orantagonists, we examined two viability indexes: thepercentage of quiescent rod-shaped cells in 10 ran-domly chosen lxl-mm fields enumerated seriallyover the second and third days in culture and therelease of creatine kinase37 into the medium after24-hour exposure to 10` to 10` M norepinephrine.For the creatine kinase release studies, we alsoexamined norepinephrine-treated (10` to 10` M)cells isolated from rat38 and canine39 hearts to deter-mine that the results were not species dependent.
Biochemistry. Cardiocyte RNA and protein synthe-sis were examined by autoradiography; specifically,we measured the incorporation of [3H]phenylalanineinto cytoplasmic protein and the incorporation of[3H]uridine into nuclear RNA.
Protein labeling. [3H]Phenylalanine incorporationinto cardiocyte cytoplasmic proteins was measured inthree experiments. First, [3H]phenylalanine incorpo-ration was examined after 72 hours of continuousexposure to 10-9 to 106 M norepinephrine. Second,the cells were pretreated either with 10-9 to 106 Mpropranolol or 10` to 10` M phentolamine and thenexposed to 1 ,M norepinephrine for 72 hours. Third,cells were treated for 72 hours with either 10`1 toi0` M isoproterenol or 10-8 to 10` M phenyleph-rine. After 72 hours of exposure to adrenergic ago-nists and/or antagonists, the cells were labeled with40 gCi/ml [3H]phenylalanine (110.4 Ci/mmol) for 6hours, washed three times with a balanced salt solu-tion containing 10 mM cold phenylalanine, and fixedin a 3:1 solution of ethanol:acetic acid before airdrying. Autoradiography was performed as we havedescribed30; experimental and control slides weretreated identically.For the above studies, [3H]phenylalanine incorpo-
ration into cardiocyte cytoplasmic proteins was mea-sured using a previously validated30 computer-as-sisted microscopic image analysis technique. Briefly,the computer program quantifies both cell surface
area and the optical density of silver grains over eachcell and then integrates the optical grain density overthe entire cytoplasmic area of each cell to provide anintegrated grain density per unit area of the cell. Wehave shown30 that there is a linear correlation(r=0.98) between the autoradiographic grain densityand scintillation counting of labeled cardiocyte pro-tein. The distinct advantage of this technique is thatit allows only viable rod-shaped cardiocytes to bestudied, rather than including nonviable hypercon-tracted cells in the analysis.RNA labeling. The method used to quantitate
[3H]uridine incorporation into nuclear RNA is stan-dard in our laboratory30'40 and was used here after 72hours of exposure of the cardiocytes to 10` to 10-6 Mnorepinephrine. At this time, the cells were exposedto 5 ,Ci/ml ['Hluridine (28.5 Ci/mmol) for 2 hours,washed three times with a balanced salt solutioncontaining 10 mM cold uridine, and fixed in 3:1ethanol: acetic acid before air drying. Nuclear graindensity in excess of that over a background area wasenumerated over the nuclei of control and norepi-nephrine-treated cardiocytes and expressed as thetotal nuclear grain density per cell. Autoradiographywas performed as described before.30
Catecholamine-Mediated Toxicity: InVitro MechanismsDuring these studies, we noted that exposure to
>10-8 M norepinephrine for 15-20 minutes causednormally quiescent cells to contract spontaneously(see Table 4). This induction of spontaneous beatingcould be aborted by either removing norepinephrinefrom the medium or pretreating the cells with pro-pranolol, suggesting that continuous occupancy ofthe /3-receptor was necessary for this result. Further,such spontaneously beating cells would invariablyundergo irreversible lethal hypercontracture withinhours. Given the striking parallel between these invitro events and the development of contraction bandnecrosis in vivo, we made a number of direct andindirect measurements to test the hypothesis18 that/3-adrenoceptor stimulation causes cAMP-mediatedcalcium overload of the cardiocyte and that calciumoverload is the proximate cause of catecholamine-mediated cell lethality. For each of the indirectbiological studies detailed below, either the inductionor complete inhibition of spontaneous cardiocytebeating was used as the end point. To confirm theseindirect studies, we directly measured both cAMPand [Ca2"]i.cAMP elevation. Three separate studies were done to
evaluate the role of cAMP production in inducingspontaneous beating. First, cAMP production wasblocked 30 minutes before 1 ,uM norepinephrine expo-sure by pretreating the cells with 10-4 to 10-9 M2'5'-dideoxyadenosine, a P-site agonist that inhibits thecatalytic activity of adenylate cyclase.41,42 Second,cAMP production was stimulated through a non-/-receptor-mediated pathway; this was accomplished bydirect activation of the catalytic subunit of adenylate
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

Mann et al Cardiocyte Adrenergic Regulation 793
cyclase43 through the application of 10`8 to 10- Mforskolin for 30 minutes. Third, we treated the cells for60 minutes with 10-6 to 10-2 M dibutyryl cAMP, acAMP analogue that diffuses readily across cell mem-branes and mimics many actions of the endogenouslystimulated cyclic nucleotide.To confirm that sustained elevation of cAMP
caused the induction of spontaneous beating, weexamined the time course of cAMP elevation afternorepinephrine stimulation. For these studies, paral-lel cultures of cardiocytes were stimulated with 1 ,uMnorepinephrine for 1, 5, 15, and 30 minutes; controltime 0 cultures were treated with diluent. To termi-nate the studies, the culture medium was removedand replaced with cold 0.1N HCl. Cyclic nucleotideswere extracted in 0.1N HCl for 5 minutes, the HClwas aspirated, and cardiocyte proteins were solubi-lized with buffered 0.02% sodium dodecyl sulfate(SDS). cAMP was measured by radioimmunoassay asdescribed before,44 with minor modifications asnoted. cAMP samples were lyophilized and reconsti-tuted in 0.05 M acetate buffer containing 1% thimer-sol. Duplicate samples were mixed with equal vol-umes of a cAMP tracer consisting of succinyl-3-[1'I]iodotyrosine methyl ester in 0.05 M acetatebuffer containing 1% thimersol and cAMP rabbity-globulin antiserum. All samples were incubated for3 hours at 4°C, allowed to come to room tempera-ture, and incubated for 10 minutes with a secondantibody. The antibody-bound fraction was centri-fuged at 1,500g, the supernatant was aspirated, andthe amount of radioactivity remaining in the pelletwas counted in a gamma scintillation counter for 1minute. Cardiocyte protein per dish was measuredusing the bicinchoninic acid assay45 after acid precip-itation of the SDS samples; bovine serum albuminwas used as a standard. Results were expressed asnanograms of cAMP per milligram of cardiocyteprotein.
Calcium influx. Given the well-recognized associa-tion between cAMP and activation of the calciumchannel,4647 we asked whether continuous norepi-nephrine exposure caused influx of extracellular cal-cium through the verapamil-sensitive calcium chan-nel and whether sustained elevation of [Ca2"]i wascausally related to the development of spontaneousbeating and lethal cell hypercontracture.To determine if influx of extracellular calcium was
important in the induction of spontaneous beating,cardiocytes were incubated for 30 minutes in a nomi-nally calcium-free buffer containing 1 mM EGTA or abuffer containing 2.5 mM CaCl2; the cells were thenstimulated with 1 ,uM norepinephrine. To testwhether the fast sodium channel or the slow calciumchannel was important in the induction of catechol-amine-mediated spontaneous beating, we blockedboth types of channels. First, cardiocytes were pre-treated for 30 minutes with 10-9 to 10-4 M verapamil,a relatively specific slow calcium channel blocker, or10-7 to 10-2 M cobalt chloride, a nonspecific cationicblocker of the slow calcium channel.48,49 Second, the
cells were pretreated for 30 minutes with 10-6 to 10`'M tetrodotoxin, a selective inhibitor of the fast sodiumchannel,50,51 or 10`6 to 10-3 M lidocaine, a fairlyspecific fast sodium channel blocker when used atconcentrations <10-3 M.52 After each of the abovetreatments, the cells were stimulated for 30 minuteswith 1 ,uM norepinephrine. Finally, the cells weretreated with both 10-3 M dibutyrl cAMP and 10` to1-4 M verapamil.Mechanical stimulation. To confirm that norepi-
nephrine stimulation caused calcium overload of thecell, we made direct measurements of [Ca2+]i inpopulations of cells using the tetracarboxylate cal-cium indicator fura-2, as well as in single cells usingfluo-3. For the former studies, freshly isolated cardi-ocytes were plated onto laminin-coated plasticsleeves and maintained under sterile conditions for atleast 24 hours before experimentation. On the day ofstudy, the cardiocytes were washed in KHB, and thelaminin-coated plastic sleeve containing the cardio-cytes was fixed vertically at a 450 angle in a quartzcuvette containing 2 ml of KHB. Fluorescence mea-surements were performed using a fluorometerequipped with a xenon lamp and a water jacket thatmaintained the cells at 37°C. After 15 minutes ofequilibration, the extent of cardiocyte autofluores-cence was determined at an emission wavelength of510 nm using excitation wavelengths of 340 and 380nm. In control studies, we determined that theamount of autofluorescence from the plastic sleeveitself was negligible (<5%). The cells were loadedwith 20 ,uM fura-2 acetomethoxy ester (AM) for 1hour53 and then washed with KHB buffer to removeany extracellular fura-2 AM. After fura-2 loading, thecardiocytes were equilibrated for an additional 30minutes to permit complete hydrolysis of any remain-ing intracellular acetomethoxy ester. The 4 mMfura-2 AM stock solutions were made in a DMSOvehicle and stored in a dark container at -70°C.Adenosine tniphosphate measurements. Norepineph-
rine at a final concentration of 1 ,uM was added tothe KHB, and the resulting change in cardiocytefluorescence was measured continuously for 1 minuteto identify the time course of any increase in [Ca2+]i.After it was determined that no experiment involvedvery rapid transients, the emission spectrum waschecked every 3 minutes for a total of 30 minutes.The brightness of the fura-2 emission signal at 510nM was calculated using excitation spectra of 340 and380 nM, and the level of [Ca21]i determined as the340/380 ratio of fura-2 brightness54; these values werecorrected for background autofluorescence as de-scribed by Bruschi et al.53Two additional experiments were done to better
define the norepinephrine effect on [Ca21]i. First, therole of 8-adrenoceptor activation was assessed byrepeating the above studies after pretreating the cellswith 1 ,M propranolol for 1 hour. Second, to deter-mine the role of influx of extracellular calcium, thecardiocytes were studied in a nominally calcium-freeKHB buffer containing 1 mM EGTA. With the
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

794 Circulation Vol 85, No 2 February 1992
exceptions just noted, the conditions for the lattertwo studies were identical to those described above.To better address the question of whether calcium
influx preceded cell injury or whether instead cellinjury was the primary event with secondary influx ofcalcium, the above studies were repeated in individualcells using digital imaging fluorescence microscopy.For the present study, we used a relatively newfluorophore, fluo-3, which has an excitation peak at503-506 nm and an emission peak at 526 nm.55 Fluo-3has two unique advantages over the traditional ultra-violet (UV) excited indicators. First, this fluorophorehas a very large (-40-fold) enhancement in fluores-cent intensity upon binding Ca2`. Second, fluo-3 has arelatively weaker affinity for calcium, thus permittingmeasurement of higher levels of [Ca2"]i. For thestudies in individual cells, the preparation of thecardiocytes was exactly the same as that describedabove for the fura-2 experiments, with the exceptionthat the cells were maintained in culture on laminin-coated petri dishes. On the day of study, the cardio-cytes were washed, and the cells were loaded for 60minutes with 20 ,um of fluo-3 acetomethoxy esther. Tofacilitate solubilization of the acetomethoxy esther,0.5-1 g1 of25% (wt/wt) Pluronic F-127 in dry dimethylsulfoxide was mixed with every 10 nM ofAM and theresulting solution thoroughly dispersed in the culturemedium.55 After loading, the cells were washed threetimes and then equilibrated for an additional 30minutes to permit complete hydrolysis of any remain-ing intracellular AM.
Norepinephrine at a final concentration of 1 ,Mwas added to the culture medium, and the resultingchange in cardiocyte fluorescence was measured 30minutes later. Control cells were treated with diluent.Fluorescent brightness was measured using a mi-crospectrofluorometer equipped with a xenon bulb.The filter sets used delivered 490 nm excitation light;emission was measured using a barrier filter thatpassed light at wavelengths >520 nm. The resultingfluorescence image (x400) was analyzed by digitalimaging microscopy, which integrates the intensity offluorescence brightness over the surface area of anindividual cardiocyte and then normalizes this valueby the surface area of the cell (,am2); this accountedfor any variations in fluorescence brightness thatmight occur on the basis of cell size alone (expressedas arbitrary units fluorescence brightness/gm2 cell).Nonspecific background fluorescence was eliminatedby a background subtraction routine; autofluores-cence was not detectable at the low visible light levelsused in the present study.Two additional fluorescence microscopy experi-
ments were done to further define the norepineph-rine effect on [Ca2"]i. First, the role of ,B-adrenocep-tor activation was assessed by repeating the aboveexperiments after pretreating the cells with 1 ,uMpropranolol for 1 hour. Second, to determine the roleof influx of extracellular calcium, the cardiocyteswere pretreated with 1 ,M verapamil for 1 hour, andthe above experiments were repeated. With the
exceptions just noted, the conditions for the lattertwo experiments were identical to those describedabove.To be certain that norepinephrine-mediated hy-
percontracture that followed the induction of spon-taneous cardiocyte beating was the result of calciumoverloading of the cell and not simply the result ofexcessive mechanical stimulation, we performed anadditional control study in which cell viability wasassessed after electrical stimulation at a frequencysimilar to that of the norepinephrine-induced spon-taneous beating. For these experiments, freshly iso-lated cardiocytes were continuously paced electri-cally for 30 minutes with a pair of platinum wireelectrodes using 0.33-Hz, 100-,A DC pulses of al-ternating polarity with no voltage offset betweenpulses; the latter two stimulation conditions wereused to minimize electrolysis. The percentage ofviable rod-shaped cardiocytes was determined beforeand 30 minutes after continuous pacing. The extentof creatine kinase release was measured at 24 hoursin the cultures that were electrically stimulated, aswell as in a group of control cultures that were notelectrically stimulated.To determine whether the norepinephrine-medi-
ated toxic effect was secondary to ATP depletion, wemeasured intracellular ATP levels in vitro. Prepara-tion and maintenance of the cultures were exactly asdescribed above. On the first day in culture, the cellswere stimulated with 1 gm norepinephrine for 0, 15,and 60 minutes and 24 hours; the appropriate controlgroups for this experiment consisted of parallel cul-tures treated at identical time points with diluentonly. At the end of each indicated time point, thecultures were washed three times with cold KHBbuffer and intracellular ATP extracted for 10 minuteswith cold 12% trichloroacetic acid. The samples werethen ether-extracted five times, and the pH wasadjusted to 7.8. Intracellular levels of ATP weremeasured using the luciferease assay according to themethod of Lundin et al.56,57 The amount of cellularprotein per sample was determined using the bicin-choninic assay.58 The level ofATP in the norepineph-rine and control cultures was expressed in nanomolesof ATP per milligram of cardiocyte protein.
DrugsL-Isomers were used except as specifically indicated.
Sources of adrenergic agents were norepinephrine,phenylephrine, isoproterenol (Sigma Chemical); pro-pranolol (a gift from Ayerst); and phentolamine (a giftfrom CIBA-GEIGY). Other sources were (±)-vera-pamil, tetrodotoxin, dibutyryl cAMP, forskolin (Sig-ma), lidocaine (Astra); 2'5'-dideoxyadenosine (Phar-macia); fura-2 AM (Calbiochem); L-[ring-2,3,4,5,6-3H]phenylalanine and [5 -3H]uridine (New EnglandNuclear); NTB3 emulsion (Kodak); medium 199 withEarle's salts (GIBCO); and medium supplements(Collaborative Research).
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

Mann et al Cardiocyte Adrenergic Regulation 795
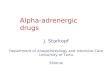
FIGURE 1. Photomicrographs ofcardi-ocyte morphology before and after nor-epinephrine exposure. Panel A: Appear-ance of a typical rod-shaped cardiocytein culture. Panel B: Appearance of apartially contracted cardiocyte after 30minutes of exposure to 1 AM norepi-nephrine. Panel C: Typical appearanceof a fully hypercontracted cardiocyte af-ter 60 minutes of exposure to 1 uMnorepinephrine.
Statistical AnalysisEach value is expressed as mean±SEM. Specific
adrenergic agonist and antagonist effects on cellviability were examined by two-way ANOVA, withtesting for differences within experimental groups onthe second and third days in culture. One-wayANOVA was used to test for overall differences inthe extent of [3H]phenylalanine or [3H]uridine incor-poration in norepinephrine-treated cells; where ap-propriate, Dunnett's multiple comparison59 was usedto test for specific differences between control andexperimental groups. A difference was said to besignificant at p<0.05.
ResultsCell ViabilityAn important finding of the present study was that
norepinephrine stimulation led to a striking, concen-tration-dependent decrease in cardiocyte viability.That is, when rod-shaped cardiocytes were exposedto norepinephrine, a large proportion of these nor-mally quiescent cells began to contract spontaneouslywithin 15-30 minutes. When followed over time,virtually all such cells developed irreversible hyper-contracture. Figure 1 (upper panel) shows the mor-phology of a rod-shaped cardiocyte and (lower panel)of a hypercontracted cardiocyte exposed to 1 ,uMnorepinephrine. Figure 2 summarizes the results ofthe cell morphology studies and shows that norepi-nephrine treatment caused a major decrease in the
percentage of viable rod-shaped cells as a function ofincreasing agonist concentration. Two-way ANOVAshowed that this catecholamine-mediated toxic effectwas both concentration and time dependent
110
60
a)ui
0
W0-
-cc
UJ
20
DURATION OFTREATMENT* 48 Hours
E] 72 Hours
*
CONTROL 0.0 0 1 0.01 0.1 1
[NOREPINEPHRINE] [tM
FIGURE 2. Bar graph of effect of norepinephrine on cardio-cyte viability. For each concentration of norepinephrine shown,the data represent mean +SEM values for a minimum of 16dishes obtained from a minimum offour primary cardiocyteisolations. Cardiocyte viability, expressed in terms of the per-centage ofrod-shaped cells in culture, was adversely affected byincreasing concentrations of norepinephrine. Analysis of vari-ance indicated that this catecholamine-mediated toxic effectwas both concentration and time dependent. Each asterisk (*)indicates a significant difference (p<O.OS) from the controlvalue by Dunnett's test.
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

796 Circulation Vol 85, No 2 February 1992
A. 80
0Ui 60
_i-aWUl0.9 40-
U,CS0
o, 20'
B.
A. so
!560-IwA
0aw6.40,c
00M
20.
[PHENTOLAMINE] pM
-J
U)
Ci0
a.
0cc
CONTROL 1 0.001 0.01 0.1 1
[PROPRANOLOL] pM et+ B
FIGURE 3. Bar graphs of effect of a- and 3-adrenergicantagonists on cardiocyte viability. For each concentration ofadrenergic antagonist shown, the data represent themean+SEM values for 12-15 dishes obtained from three or
fourprimary cardiocyte isolations. Panel A: Phentolamine didnot significantly block the toxic effects of norepinephrine (1MM) on cell viability, regardless of the concentration used.Panel B: Propranolol largely attenuated but did not completelyblock the toxic effect of norepinephrine (1 pM), even at a
propranolol concentration of 1 gM. Because membrane sta-bilizing effects can occur with 106 Mpropranolol, we cannotexclude that some protective effect may have been frommembrane stabilization. Nevertheless, the combination of 10pM phentolamine with 1 pM propranolol (a plus 13) com-
pletely prevented the norepinephrine-mediated decrease inrod-shaped cardiocytes. Each asterisk (*) indicates a signifi-cant difference (p<0.05) from control by Dunnett's test.
(p<0.001); that is, for each norepinephrine concen-tration used, there was a significant decline in thepercentage of rod-shaped cells from the secondthrough the third day in culture.Two pharmacological approaches were taken in
determining the mechanisms for this norepinephrineeffect. Figure 3 summarizes the results of the firststudy, in which we studied the prevention of norepi-nephrine toxicity by a- and/or 13-adrenoceptor block-ade. Panel A shows that pretreatment with phento-lamine did not significantly attenuate the toxic effectof norepinephrine on cell viability; only with verylarge (10 ,M) concentrations of phentolamine wasthere a slight protective effect. In contrast, panel Bshows that propranolol antagonized the toxic effectsof norepinephrine over the full range of concentra-tions used. Two-way ANOVA showed that this pro-tective effect persisted from the second through the
D. 80 1
01UX,J 60 l_ia.
9 40m0O
DURATION OFTREATMENT* 48 HoursE 72 Hours
CONTROL 0.01 0.1 1 10
[PHENYLEPHRINEJ pM
*
*
*20
0111CONTROL 0.0001 0.001 0.01 0.1
[ISOPROTERENOL] pM
FIGURE 4. Bar graphs of effect of a- and /3-adrenergicagonists on cardiocyte viability. For each concentration ofadrenergic agonist shown, the data represent the mean±SEMvalues for 12-15 dishes obtained from three or four primarycardiocyte isolations. Panels A and B: Effects of gradedconcentrations of phenylephrine and isoproterenol, respec-tively, on cardiocyte viability. Panel A shows that with phen-ylephrine there was a slight but significant (p<0.001) overalldecrease in cell viability; this effect was significantly differentfrom that ofcontrolfor concentrations ofphenylephrine .10-7M Of note, the effect of phenylephrine was not attenuatedsignificantly (p=O.66) by pretreatment with 106 M propran-olol. Panel B shows that there was a striking overall decrease(p<O.OOl) in the percentage of rod-shaped cells after stimu-lation with isoproterenol; this effect was significantly differentfrom that ofcontrolfor concentrations ofisoproterenol .10-10M. Each asterisk (*) indicates a significant difference(p<O.05) from control by Dunnett's test.
third day in culture. As shown, 1 jaM propranololgreatly attenuated but did not fully prevent the toxiceffect of norepinephrine. Thus, in an additionalexperiment the cells were pretreated with both 1 ,uMpropranolol and 10 ,uM phentolamine before norepi-nephrine treatment. Figure 3B shows that combineda- and 83-adrenoceptor blockade completely pre-vented the norepinephrine-mediated decrease in cellviability.
Figure 4 summarizes the second pharmacologicalapproach, in which cells were treated with phenyleph-rine or isoproterenol to study the respective effects ofeither a- or ,B-adrenoceptor stimulation on cardiocyteviability. Panel A of Figure 4 shows that phenyleph-rine treatment resulted in a very small but significantdecline in the percentage of rod-shaped cardiocytes;
'1
D S..
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

Mann et al Cardiocyte Adrenergic Regulation 797
O E RODENTE= * FELINE * *8 U CANINE r- i
0IL
0
09
z .001 . 01 1 0
1)0
0.001 0.01 0.1 1 1 0
[NOREPINEPHRINEJ rM
FIGURE 5. Bar graph of effect of norepinephrine treatment(24 hours) on creatine kinase release in rat, cat, and dogcardiocytes. The values shown for each norepinephrine con-centration represent mean +SEM values obtainedfrom four tosix culture dishes and are expressed as a percent increase fromcontrol values. There was a concentration-dependent increasein creatine kinase released into the medium for norepineph-rine-treated (24 hours) cells. This effect was much morepronounced for the cat and dog cardiocytes than it was for therat cardiocytes. ANOVA testing for each species showed thatthis overall difference was significant statistically (p<0.001).Each asterisk (*) indicates a significant difference (p<0.01)from controL
Dunnett's post-ANOVA showed this to be significantfor phenylephrine concentrations 210` M. Two-wayANOVA further showed that this effect was concen-tration dependent (p<0.001) but not time dependent;that is, there was no further decline in the percentageof rod-shaped cells from the second through the thirdday in culture. In contrast to the findings witha-adrenoceptor stimulation, panel B of Figure 4 showsthat isoproterenol stimulation caused an obvious de-crease in the percentage of rod-shaped cells; thiseffect was very similar to the norepinephrine effectshown in Figure 1. Indeed, two-way ANOVA showedthat the isoproterenol effect was both concentrationand time dependent (p<0.001).To confirm that the decline in the number of
rod-shaped cells reflected diminished cell viability,we measured the amount of creatine kinase releasein cardiocyte cultures treated for 24 hours with 10`to 10-5 M norepinephrine. Figure 5 shows that therewas a stepwise increase in creatine kinase release asa function of increasing norepinephrine concentra-tion. ANOVA indicated that these overall differ-ences in creatine kinase release were statisticallysignificant (p<0.001); post-ANOVA comparison in-dicated that there were significant differences fromcontrol for norepinephrine concentrations .10`7 M.Linear regression analysis was also done to deter-mine whether there was a relation between thenorepinephrine-mediated decrease in cell viabilityand the amount of creatine kinase release. Thisanalysis showed that after exposure to 10-9 to 10-5 Mnorepinephrine for 24 hours, there was a significant
z
I-
0
0.00z
z
zW.
10t
so -
DURATION OFTREATMENTa nNours
*
*
_ - -'_ _CONTROL 0.001 0.01 0.1 1
[NOREPINEPHRINEJ M
FIGURE 6. Bar graph of effect of norepinephrine on[3H]phenylalanine incorporation into cardiocyte protein. Cy-toplasmic grain density is shown as the integrated grain densityper cell area in mim2XiO3. For each norepinephrine concen-tration, the data represent the mean±SEM values for 100consecutively studied rod-shaped cardiocytes. In preliminarycontrol experiments, we established that [3H]phenylalanineincorporation was linear during the 6-hour period of labeling.As shown, exposure to norepinephrine caused a significant(p<O.OOl) concentration-dependent decrease in the extent of[3H]phenylalanine incorporation into cytoplasmic protein.Each asterisk (*) indicates a significant difference (p<0.01)from control values by Dunnett's test.
linear relation (r=0.92, p<0.001) between the per-centage of hypercontracted cardiocytes relative toviable, rod-shaped cells and the percent increase increatine kinase release.To be certain that norepinephrine-mediated cardi-
ocyte toxicity was not a strictly species-dependentphenomenon, we repeated these studies using cellsisolated from adult rat and canine hearts. Figure 5shows that norepinephrine treatment led to an over-all significant (p<0.001 for both) release of creatinekinase from both rodent and canine cardiocytes,albeit to a lesser extent in the rat. For caninecardiocytes, post-ANOVA testing indicated thatthere were significant differences from control fornorepinephrine concentrations >10` M, whereas forrodent cardiocytes there were significant differencesfor norepinephrine concentrations > 10- M.
BiochemistryAdrenergic effects on cardiocyte synthetic activity
were assessed in two separate autoradiographic stud-ies of [3H]phenylalanine incorporation into cytoplas-mic proteins and [3H]uridine incorporation into nu-clear RNA.
Protein labeling. A second important finding of thepresent study was that continuous stimulation withnorepinephrine resulted in a concentration-depen-dent decrease in [3H]phenylalanine incorporationinto viable rod-shaped cardiocytes. Figure 6 showsthe results of exposing cardiocytes for 72 hours tonorepinephrine concentrations ranging from 10` to10`6 M. The salient finding is the striking decrease incytoplasmic labeling with increasing norepinephrine
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

798 Circulation Vol 85, No 2 February 1992
TABLE 1. Effect of Adrenergic Antagonists on [3H]PhenylalanineIncorporation Into Cardiocyte Cytoplasmic Protein
Change fromTreatment (72 hr) control (%)10-6 M norepinephrine -66.9±+ 1.5*10-6 M norepinephrine+10-9 M propranolol -65.2±2.2*10-6 M norepinephrine+108 M propranolol -52.4±2.3*10-6 M norepinephrine+107 M propranolol -36.5±3.4*10-6 M norepinephrine+10-6 M propranolol -18.8±4.6t10-6 M norepinephrine+10-8 M phentolamine -67.1±1.8*10-6 M norepinephrine+10-7 M phentolamine -58.8±2.0*10-6 M norepinephrine+10-6 M phentolamine -61.3±2.3*10-6 M norepinephrine+10-5 M phentolamine -62.2±2.3*10-6 M norepinephrine+10-5 M phentolamine
+106 M propranolol -2.8±4.7Each value is expressed as the mean±SEM of the percent
change from control in the extent of cytoplasmic labeling. For eachof the treatments noted above, the data were obtained from aminimum of 100 consecutively studied rod-shaped cardiocytes;nonviable ball-shaped cardiocytes were excluded from the analysis.Norepinephrine treatment (1 lM) led to a significant decline inthe extent of cytoplasmic labeling. One-way ANOVA indicatedthat propranolol exerted a significant concentration-dependent"sparing" of the norepinephrine-mediated decrease in [3H]pheny-lalanine incorporation; at 10-6 M propranolol, the effects ofnorepinephrine were largely, but not completely, attenuated.There was, however, no significant concentration-dependent"sparing" effect after pretreatment with phentolamine. The com-bination of 10-5 M phentolamine and 10-6 M propranolol fullyblocked the norepinephrine-mediated effects on cardiocyte pro-tein synthesis. Treatment of cardiocytes with adrenergic antago-nists alone did not lead to a significant change in the extent ofcytoplasmic labeling compared with control cardiocytes (10-6 Mpropranolol, -6.6±3.6%, p=NS; 10-5 M phentolamine,-1.5±3.8%,p=NS; 10- M phentolamine± 10-6 M propranolol,-4.8±4.9%, p=NS).*p<0.01 compared with control by Dunnett's test.tp<0.05 compared with control by Dunnett's test.
concentrations. ANOVA indicated that these overalldifferences were significant (p<0.001); Dunnett'spost-ANOVA comparison showed that this catechol-amine-mediated effect was significantly differentfrom control for norepinephrine concentrations>10-8 M.Table 1 is a summary of the results of autoradio-
graphic studies in which cells were exposed to nor-epinephrine in the presence of a- and/or f3-adrener-gic antagonists. The extent of cytoplasmic proteinlabeling was expressed as a percentage of control.When the cells were pretreated with concentrationsof propranolol ranging from i0` to 10-6 M, there wasa concentration-dependent amelioration of the nore-pinephrine-mediated decrease in protein labeling.Nevertheless, the norepinephrine effect was still ev-ident in the cells treated with 1 ,uM propranolol,albeit to a much lesser extent. In contrast to thefindings with ,3-adrenoceptor blockade, phentola-mine did not appreciably block the norepinephrine-mediated decrease in [3H]phenylalanine incorpo-ration. However, the combination of a- andf3-adrenoceptor blockade completely blocked the
TABLE 2. Effect of Adrenergic Agonists on [3HlPhenylalanineIncorporation Into Cardiocyte Cytoplasmic Protein
Change fromTreatment (72 hr) control (%)
10-10 M isoproterenol -10.1+5.610-9 M isoproterenol -21.9-+-6.3*10-8 M isoproterenol -46.7+2.7t10-7 M isoproterenol -60.9±2.9t10`8 M phenylephrine -0.2±3.810` M phenylephrine -2.3±4.310-6 M phenylephrine -7.5±3.510-5 M phenylephrine -13.7+3.6*10-5 M phenylephrine+ 10` M phentolamine 1.4±3.5Each value is expressed as the mean±SEM of the percent
change from control in the extent of cytoplasmic labeling. For eachof the treatments given above, data were obtained from a mini-mum of 100 consecutively studied rod-shaped cardiocytes; nonvi-able ball-shaped cardiocytes were excluded from the analysis.ANOVA showed that treatment with isoproterenol resulted in ahighly significant (p<0.001) concentration-dependent decrease in[3H]phenylalanine incorporation; post-ANOVA comparisonshowed that the isoproterenol-mediated effect was significantlydifferent from control for concentrations of isoproterenol >10`10M. There was also a small but statistically significant decrease inthe [3H]phenylalanine incorporation in the phenylephrine-treatedcells; post-ANOVA comparison indicated that the phenylephrine-mediated effect was not significantly different from control untilvery large concentrations (10-5 M) of phenylephrine were used.This phenylephrine-mediated effect on protein synthesis could beblocked by pretreating the cells with 10-5 M phentolamine.
*p<0.05 compared with control by Dunnett's test.tp<0.01 compared with control by Dunnett's test.
norepinephrine-mediated reduction in cytoplasmiclabeling.To further define the mechanism(s) for catechol-
amine-mediated effect(s) on protein synthesis, westudied the effects of a- or /8-adrenoceptor agonistson cytoplasmic protein labeling. Table 2 shows that72 hours of continuous exposure to 10-10 to 10-7 Misoproterenol caused a concentration-dependent de-crease in cytoplasmic labeling that was similar to thenorepinephrine effect. ANOVA showed that theseoverall differences were highly significant (p<0.001);Dunnett's post-ANOVA testing indicated that thiseffect was significantly different from control forisoproterenol concentrations >10-10 M. In contrastto the findings with selective ,B-adrenoceptor stimu-lation, exposure to phenylephrine caused a small butsignificant (p<0.05) decrease in [3H]phenylalanineincorporation. Dunnett's post-ANOVA testingshowed that the phenylephrine effect was not signif-icantly different from control until very large concen-trations (10-` M) were used. Blockade of the phe-nylephrine-treated cells with 10 ,uM phentolamineprevented the decrease in cytoplasmic labeling.RNA labeling. Table 3 shows the effects of 72 hours
of continuous norepinephrine treatment on cardio-cyte nuclear RNA labeling. There was a decrease innuclear labeling as a function of increasing norepi-nephrine concentration. ANOVA showed that theoverall differences were significant (p<0.001); post-
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

Mann et al Cardiocyte Adrenergic Regulation 799
TABLE 3. Nuclear [3H]Uridine Incorporation in Control and Norepinephrine-Treated Cardiocytes
Norepinephrine concentration
Control 10-9M 10-8 M 10-7 M 10-6 M
Grains per cell 19.6± 1.2 19.4±1.3 16.9±1.4 12.7±0.9* 6.4±0.7*Grains per nucleus 9.9±0.5 9.9±0.6 9.1±0.6 7.9±0.4* 3.6±0.3*
Each value is expressed as mean±SEM. Nucleoplasmic grain density is given for rod-shaped control andnorepinephrine-treated (72 hours) cardiocytes. ANOVA indicated an overall significant decrease in both the numberof total nuclear grains per cell and the grains per nucleus as a function of increasing norepinephrine concentration;post-ANOVA comparison testing indicated that the norepinephrine-mediated effect was significantly different fromcontrol for concentrations .10-8 M.
*p<0.01 compared with control by Dunnett's test.
ANOVA comparison showed that this catechol-amine-mediated effect was significantly different(p<0.01) from control for norepinephrine concen-
trations >10` M. To be certain that these differ-ences in nuclear grains per cell were not due to a
greater frequency of multinucleated cells in the con-trol group, we compared the grains per nucleus inboth control and norepinephrine-treated cells. Foreach of the experimental groups, there was again asignificant (p<0.001) concentration-dependent de-crease in the extent of nuclear labeling as a functionof increasing norepinephrine concentration.
Catecholamine-Mediated Toxicity: InVitro MechanismscAMP elevation. Table 4 summarizes the results of
the three studies showing that cAMP elevation in-duced spontaneous cardiocyte beating that, overtime, led to the cell hypercontracture depicted inFigures 1 and 2. Although a range of concentrationswas tested for each agent shown in Table 4, for thesake of simplicity only the lowest drug concentrationthat produced the indicated effect is reported. First,the use of 10-` M 2'5'-dideoxyadenosine to blockcAMP production prevented induction of spontane-ous beating by 1 ,M norepinephrine. Second, whencAMP production was stimulated through a non-,8-adrenoceptor mechanism by 10`6 M forskolin, spon-taneous cardiocyte beating occurred within 30 min-utes. Third, when 10-3 M dibutyryl cAMP, a cAMPanalogue, was added to the culture dishes, the cellsbegan to beat spontaneously within 60 minutes.
Figure 7 shows the results of studies in which thetime course of cAMP elevation was measured afterstimulation with 1 ,M norepinephrine. There was a
sustained fourfold increase in cAMP production af-ter norepinephrine stimulation. Furthermore, pre-treatment with 1 .M propranolol for 60 minuteslargely abolished the norepinephrine-induced in-crease in cAMP.
Calcium influx. Table 4 also is a summary of theresults of studies of the role of calcium influx ininducing spontaneous cardiocyte beating and hyper-contracture. Although a range of concentrations wastested for each agent, only the lowest drug concen-
tration that produced the indicated effect is reported.First, although norepinephrine-induced spontaneousbeating was readily induced in cardiocytes in 2.5 mM
calcium buffer, this was not seen in norepinephrine-stimulated cells in a calcium-free 10` M EGTAbuffer. Furthermore, the absence of norepinephrine-induced spontaneous beating in the EGTA-treatedcells was not secondary to damage to cell membranesbecause the EGTA-treated cells began to contractspontaneously when placed in a 2.5 mM calciumsolution and restimulated with 1 ,M norepinephrine.Second, both verapamil (.1 ,M) and cobalt chloride(.10 mM) suppressed spontaneous beating com-pletely at concentrations that block the slow calciumchannel.48,60 Third, neither 10 ,uM tetrodotoxin nor
TABLE 4. Induction of Spontaneous Cardiocyte Beating
Spontaneouslybeating rods
Treatment (%)
Diluent (control) 010-6 M norepinephrine 20.9+2.510-5 M dideoxyadenosine + norepinephrine 010-6 M forskolin 12.5±4.110 M dibutyryl cyclic AMP 20.5±4.610`3 M EGTA + norepinephrine 010-6 M verapamil + norepinephrine 010-2 M cobalt + norepinephrine 0105 M lidocaine + norepinephrine 20.2±3.410-5 M tetrodotoxin + norepinephrine 20.8±3.110 M dibutyryl cyclic AMP + 10-6 M verapamil 0
Each value is expressed as mean±SEM. Day 1 cultures wereexposed to one or more treatments as detailed in the left column,and the percentage of spontaneously contracting cells was quan-tified 30 minutes after stimulation; however, for dibutyryl cyclicAMP, the percentage of spontaneously contracting rods wasquantified 60 minutes after stimulation. For each of the studiesdetailed above, either the induction or the complete inhibition ofspontaneous beating was used as the physiological end point.Although a range of concentrations was tested for each agent, onlythe lowest drug concentration that produced the indicated effect isreported in the left column. Contracting rods were quantified infive randomly picked fields (x 200 magnification) per dish, using aminimum of eight dishes for each concentration of drug tested.Unless specified, agents were always applied to the cells for aperiod of 30 minutes; control cells received diluent only. Theconcentration of norepinephrine used throughout these studieswas 1 gM. As shown, experimental conditions that are known toincrease cyclic AMP led to the development of spontaneousbeating. This norepinephrine-mediated effect could be preventedby removing extracellular calcium or blocking the slow calciumchannel; pharmacological blockade of the fast sodium channel hadno effect on the induction of spontaneous beating.
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

800 Circulation Vol 85, No 2 February 1992
Z0 150
L
CD
C 100
C.)
A 1 1 NEA 1 pM NE + 1 Propanid
e
OL
0 5 10 15 20 25 30TIME (min)
FIGURE 7. Plots of time course of cyclic AMP elevation innorepinephrine (NE)-stimulated cells. Each data point repre-sents six to eight culture dishes from two primary cardiocyteisolations. Stimulation with 1 pM NE led to a rapid andsustained fourfold increase in cyclic AMP. As shown, pretreat-ment with 1 pM propranolol significantly attenuated theNE-mediated effect on cyclic AMP.
10 ,M lidocaine prevented the induction of norepi-nephrine-induced spontaneous cardiocyte beating atconcentrations that block the fast sodium chan-nel.50-52 Finally, verapamil (. 1 ,M) completely sup-pressed the spontaneous cardiocyte beating inducedby the 10' M dibutyryl cAMP.
Figure 8 shows the effect of norepinephrine stim-ulation on [Ca2]i, expressed as an absolute increasein the 340/380 ratio of fura-2 brightness. The salient
0.12CD 0a) 0.10ZZ
z C 0.08
C ° 0.06
,k U 0.04
L < 0.02
0.00
-0.02
& 1 uM NE
A 1 gM NE + 1iM Propranolol0 lgMNE+1mMEGTA
AkA d
.L~~~~~~~~~~~~~~~
0 1 0 20 30
TIME (min)
FIGURE 8. Plots of time course of [Ca`+]i elevation innorepinephrine (NE)-stimulated cardiocytes. Direct measure-
ments of [Ca2`1i were performed using the calcium indicatorfura-2. Data are expressed as the absolute increase in the340/380 ratio of fura-2 brightness after correcting for initialcardiocyte brightness. Each data point shown representsmean +SEM values offive separate experiments. Continuousstimulation with 1 ,M NE led to a gradual and progressive
increase in fura-2 brightness as a function of time, which was
attenuated significantly by pretreating the cells with 1 pMpropranolol. In the presence of 1 mM EGTA, there was no
increase in intracellularfura-2 brightness afterNE stimulation.Each asterisk (*) indicates a significant difference (p<0.05)from control.
finding is that continuous stimulation with 1 ,uMnorepinephrine resulted in a gradual and progressiveincrease in the 340/380 ratio of fura-2 brightness withtime. Two-way ANOVA indicated significant(p<0.001) overall differences between control andnorepinephrine-treated cells; post-ANOVA compar-ison demonstrated significant differences from con-trol beyond 12 minutes. A second important findingwas that norepinephrine stimulation did not cause asignificant (p>0.05) increase in fura-2 brightness forcardiocytes pretreated with 1 ,uM propranolol. Fi-nally, to determine whether the norepinephrine-mediated increase in fura-2 brightness was caused bycalcium influx rather than calcium release from in-tracellular stores, these experiments were repeatedin an EGTA buffer. As shown, in the absence ofextracellular calcium, there was no significant(p>0.05) increase in intracellular fura-2 brightnessafter norepinephrine stimulation.
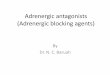
Digital imaging fluorescence microscopy confirmedthat this increase in fluorescence brightness was theresult of norepinephrine-stimulated calcium influxrather than secondary calcium influx from cellularinjury. The digital imaging studies, which were con-fined to single, viable rod-shaped cardiocytes (n=100cells/group), revealed two important findings. First,stimulation with norepinephrine (1 ,uM) for 60 min-utes led to a significant increase in intracellular fluo-rescence compared with control values (0.288+0.001versus 0.10+0.004, respectively; p<0.001). Further-more, this norepinephrine-induced increase in intra-cellular fluorescence brightness was significantly at-tenuated (p>0.30 for both) by pretreating the cellswith either 1 g.m propranolol (0.10±0.002, n=100cells) or 1 ,um verapamil (0.10±0.004, n=100 cells).An additional important finding of the present studywas that norepinephrine caused rhythmic "scintilla-tions" of fluorescence brightness within individualcells that were quite similar in appearance to therhythmic flashing of the firefly Photuris versicolor on asummer evening. This phenomenon, which is illus-trated in Figure 9, was seen in the majority of rod-shaped cardiocytes at various times after norepineph-rine stimulation. Furthermore, although not every cellshowing rhythmic scintillations developed spontane-ous beating, this phenomenon was always observed incells in which spontaneous beating developed. Al-though the present study was not designed to eluci-date the mechanism(s) for this interesting finding, therhythmic increase in fluorescence brightness probablyrepresents calcium-triggered calcium release from thesarcoplasmic reticulum.61Mechanical stimulator. Electrical stimulation of
cardiocytes at a frequency of 0.33 Hz resulted in an-2.5% decrease (p=0.82) in the percentage of rod-shaped cardiocytes in a given culture dish (n=8experiments) over time. Furthermore, compared withcontrol cultures that were not electrically stimulated,there was no significant increase in creatine kinaserelease (control, 951+22 IU; electrically stimulated,934 +49 IU; p =0.94).
200r
0.16
0.14
1
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

Mann et al Cardiocyte Adrenergic Regulation 801
FIGURE 9. Fluorescent "scintillation" in a norepinephrine-stimulated cardiocyte. Left panel: Level offluorescence brightness ina fluo-3-loaded cardiocyte treated with 1 pM norepinephrine for 30 minutes. Right panel: Same cell during the peak of afluorescent scintillation. Notice that an increase in fluorescence brightness occurs without a change in cell length, thus obviatingdepolarization as the mechanism. Also note that the fluorescence intensity for the ball-shaped cell in the left corner of each panelwas the same, indicating that the intensity of the light source was unchanged.
Adenosine triphosphate measurements. Table 5 is asummary of the results of the studies in which weexamined the effect of norepinephrine stimulation onintracellular ATP levels. As shown, there was nochange in the intracellular levels of ATP in either thecontrol or the norepinephrine-treated cultures. Two-way ANOVA showed that there were no significantdifferences between groups (p=0.99) or withingroups as a function of time of treatment (p=0.97).
DiscussionThe present study directly supports the hypothesis
that cAMP-mediated calcium overload is the primarymechanism responsible for catecholamine-inducedtoxicity in cultured adult mammalian cardiocytes.Two distinct lines of evidence support this statement.First, when the effects of adrenergic stimulation wereexamined in virtually pure populations of cardiocytesusing concentrations of norepinephrine that are nor-mally attainable at the neural cleft32 or available asactual circulating levels in certain pathological con-ditions,6,33,34 there was both a concentration-depen-dent decrease in cardiocyte viability, as shown by astriking decrease in viable rod-shaped cells, and asignificant release of creatine kinase. The view thatthese effects were mediated directly by the f3-adreno-
TABLE 5. ATP Levels in Control and Norepinephrine-Treated Cardiocytes
Control Norepinephrine (1 gM)(n=5) (n=5)
Baseline 12.9±1.1 13.6 1.215 Min 12.0+2.1 12.6±1.960 Min 13.1±1.8 12.7±2.224 Hr 13.3±+3.3 12.4±2.3
Each value is expressed as mean ±SEM of nM ATP/mg cardio-cyte protein. Intracellular levels of ATP were measured at thetimes indicated above using the luciferase assay. Two-wayANOVA indicated that there was no significant difference be-tween groups (p=0.99) or within groups (p=0.97) as a function oftime.
ceptor is supported by the finding that the toxiceffects of norepinephrine were attenuated signifi-cantly by f-adrenoceptor blockade and mimicked byselective stimulation of the P-adrenoceptor. In con-trast, a-adrenoceptor effects were relatively smalland evident only when very large concentrations ofa-adrenergic agonists and antagonists were used. It isof some interest that the toxic response to norepi-nephrine was not confined to a single mammalianspecies; toxicity was elicited in rat, cat, and -caninecardiocytes. Of note, toxicity was evident for ratcardiocytes only when very large concentrations ofnorepinephrine were used, probably reflecting therelatively smaller number of /-adrenoceptors in thisspecies compared with cat, dog, and humans.62-64
Second, continuous adrenergic stimulation led tocAMP-mediated calcium overload of the cardiocyte,as shown indirectly by pharmacological strategies inwhich increased intracellular cAMP was shown tocause spontaneous beating and cell hypercontracture,as well by data showing that calcium influx through theverapamil-sensitive calcium channel was necessary forthis effect. The role of cAMP-mediated calcium influxis supported more directly by the microspectrofluoro-metric studies, as well as by the time course studieswhere norepinephrine exposure led first to a rapidfourfold increase in intracellular cAMP and then to a3.2-fold increase in [Ca2"],. Furthermore, the norepi-nephrine effects on cAMP and [Ca2+]i were signifi-cantly attenuated by P-adrenoceptor blockade, asmight be expected from the relation betweenf,-adrenoceptor stimulation and activation of the ver-apamil-sensitive calcium channel.46w47 To be certainthat cardiocyte hypercontracture was the result ofcalcium overload of the cell rather than excessivemechanical activity, an additional control experimentwas performed in which the cells were electricallystimulated to contract. When the cells were stimulatedat a frequency similar to that seen with norepineph-rine exposure, there was no significant decrease in the
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

802 Circulation Vol 85, No 2 February 1992
number of viable rod-shaped cells or significant in-crease in creatine kinase release from the paced cells.Finally, to exclude the possibility that calcium influxinto the cell was secondary to depletion of high-energyphosphates rather than a direct effect of norepineph-rine, we measured intracellular ATP levels in vitro.These results showed that intracellular ATP levelswere unchanged when norepinephrine stimulationresulted in cAMP-mediated calcium overload of thecell. Parenthetically, it should be noted that the ex-perimental protocols detailed were designed to mini-mize the effects of free radicals in culture; therefore, itis not possible to comment on any potential effectsthat free radicals might have played in the observedcatecholamine-mediated toxic effects in our in vitromodel.Another major finding of the present study was
that continuous stimulation with norepinephrinecaused a concentration-dependent decrease in['H]phenylalanine incorporation in cultured adultcardiocytes. Thus, adrenergic stimulation not onlyresulted in diminished cell viability but also led to adecrease in protein synthetic activity in the remainingviable cardiocytes. The decrease in cytoplasmic label-ing was greatly attenuated by /8-adrenoceptor block-ade and mimicked by selective stimulation of the,3-adrenoceptor. In contrast, a-adrenoceptor stimu-lation led to a very small but significant decrease incardiocyte synthetic activity, albeit only with verylarge concentrations of agonist. Although the exactmechanisms for this decrease in ['H]phenylalanineincorporation are not known, the concentration-de-pendent decrease in ['H]uridine incorporation intonuclear RNA after norepinephrine exposure suggeststhat the decrease in cardiocyte synthetic activity maybe in part mediated at the transcriptional level.Nevertheless, on the basis of the present study, itwould be premature to comment on rates of proteinor RNA synthesis or degradation, given that size ofthe phenylalanine and uridine pools were not known.
Experimental Catecholamine CardiotoxicityIn 1959, Rona et a17 made the important observa-
tion that injection of isoproterenol into rats produces"infarctlike" myocardial necrosis in the absence ofsignificant coronary artery lesions. This observationled to the suggestion that "relative hypoxia" wasresponsible for the observed cardiac necrosis.7-9,65That is, increased cardiac inotropy and chronotropyafter adrenergic stimulation caused a relative imbal-ance between myocardial oxygen demand and bloodflow, such that demand exceeded supply. In support ofthis view is the observation that isoproterenol de-creases coronary blood flow in the early phase ofisoproterenol cardiotoxicity.10 In addition to this rela-tive hypoxia theory, a number of alternative hypothe-ses have been proposed to explain catecholamine-induced myocardial injury. Rona and coworkersl1-'4also suggested that catecholamine-mediated increasesin sarcolemmal permeability contributed to the patho-genesis of myocardial injury. Although the concept of
calcium-induced cardiac necrosis had been introducedpreviously,66 Fleckenstein'5 was the first to proposethe radically different concept that calcium overloadof the cell was the result of catecholamine-mediatedcell injury. According to this theory, the importantevent in the development of the catechol-amine-mediated lesion was a high-energy phosphatedeficiency that resulted from excessive activation ofcalcium-dependent ATPases and calcium-induced im-pairment of mitochondrial function. Critical supportfor the calcium overload hypothesis followed in animportant study by Bloom and Davis17 that showedthat myocardial calcium increased 10 minutes afterinjection of isoproterenol into rats, suggesting thatcalcium influx was the cause rather than the conse-quence of cardiac injury.'6 Although Bloom andSweat67 subsequently showed that increased levels ofmyocardial calcium were coupled to elevations inmyocardial cAMP, the view that cellular calciumoverload was consequent to /8-adrenoceptor-medi-ated elevations ofcAMP was first suggested by Bhagatet al.18 This hypothesis was subsequently confirmed ina series of studies by Opie and colleagues,19,20,24 whodemonstrated in Langendorff rat hearts that catechol-amine injury was mediated by the /-adrenoceptor.However, the importance of the ,B-adrenoceptor wasnot confirmed by an in vivo study in rabbits, whichsuggested instead that catecholamine cardiotoxicity islargely mediated by the a-adrenoceptor.21,22 Finally,others have suggested that oxidative catecholaminemetabolites and/or the formation of oxygen or oxygen-derived free radicals causes cardiac damage.25-28However, as noted in a recent review,29 the biologicalsignificance of these latter studies is uncertain giventhe large concentrations of adrenochrome (2 10- M)needed to cause cardiac injury. Thus, a number ofhypotheses have been proposed, but there is no con-sensus regarding the basic mechanism(s) responsiblefor catecholamine cardiotoxicity.
ConclusionsThe toxic cardiac effects of catecholamines have
been recognized at least since 1907, when Josue68 firstreported catecholamine-induced cardiac necrosis.Thus, we were not surprised to find that norepineph-rine caused toxic effects in isolated adult cardiocytes.This statement notwithstanding, the importance of thepresent study is twofold. First, this simple experimen-tal study provides straightforward and compellingevidence in support of the viewpoint that cAMP-mediated calcium overload of the cell is a fundamen-tally important early event in the genesis of catechol-amine-induced cardiac injury. Second, the presentstudy constitutes the initial demonstration that so-called "pathological" elevations of norepinephrinelead to a concentration-dependent decrease in cardi-ocyte RNA and protein synthetic activity, as well ascell viability.Although direct correlations between short-term
effects in isolated cells and long-term effects in theheart in vivo are not appropriate, these data do
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

Mann et al Cardiocyte Adrenergic Regulation 803
provide several potential clinical insights. For exam-ple, the prognosis of patients with congestive heartfailure is inversely related to the level of circulatingplasma norepinephrine.56 Although this catechol-amine response may well be an effect of diseaseseverity, it may also have a deleterious contributoryrole. Furthermore, our finding that catecholamine-induced calcium overload occurs predominately viathe f3-adrenoceptor suggests a mechanism for thesalutary clinical effect of (8-blockade in dilated car-diomyopathy.69-71 Finally, our finding that adrenergicstimulation causes decreased cardiocyte syntheticactivity suggests a potential mechanism, albeit spec-ulative, for the progressive pump dysfunction inpatients with dilated cardiomyopathy. That is, thenorepinephrine-induced decrease in cardiocyte RNAand protein synthesis may compromise the develop-ment of fully compensatory hypertrophy in responseto some forms of chronic cardiac stress. In summary,catecholamines have a major, and beneficial, role inthe short-term cardiovascular response to physiolog-ical stress. Unfortunately, during the long-term car-diovascular response to pathological stress, the ben-eficial role of catecholamines may occur at the priceof superimposed cardiac toxicity.
AcknowledgmentsThe authors thank Stephen Vinciguerra, Valarie
Young, and Mary Barnes for their technical assist-ance; Tommy Williams for the performance of thehigh-performance liquid chromatography assay; JonBenthal for the photography of the figures; and BettyOwens for secretarial assistance.
References1. Cannon WB: Methods of demonstrating adrenal secretion and
its nervous control, in Cannon WB (ed): Bodily Changes InPain, Hunger, Fear and Rage. New York, D Appleton and Co,1923, pp 40-51
2. Szakacs JE, Dimmette RM, Coward EC: Pathologic implica-tions of the catecholamines, epinephrine, and norepinephrine.US Arned Forces Med J 1959;10:908-925
3. Goldstein S, Killip T: Catecholamine depletion in thyrotoxi-cosis: Effect of guanethidine on cardiovascular dynamics.Circulation 1965;31:219-227
4. Raab W: The sympathogenic biochemical trigger mechanismof angina pectoris. Am J Cardiol 1962;9:576-584
5. Raab W, Van Lith P, Lopeschkin B, Herrlich HC: Catechola-mine-induced myocardial hypoxia in the presence of impairedcoronary dilatability independent of external cardiac work.AmJ Cardiol 1962;9:455-470
6. Cohn JN, Levine TB, Olivare MT: Plasma norepinephrine asa guide to prognosis in patients with chronic congestive heartfailure. N Engl J Med 1984;311:819-823
7. Rona G, Chappel CI, Balazs T, Gaudry R: An infarct-likemyocardial lesion and other toxic manifestations produced byisoproterenol in the rat. AMA Arch Pathol 1959;67:443-455
8. Reichenbach DD, Benditt EP: Catecholamines and cardiomy-opathy: The pathogenesis and potential importance of myo-fibriallar degeneration. Hum Pathol 1970;1:125-150
9. Ferrans VJ, Hibbs RG, Black WC, Weilbaecher DG: Isopro-terenol-induced myocardial necrosis: A histochemical andelectron microscopic study. Am Heart J 1964;68:71-90
10. Somani P, Laddu AR, Hardman HF: Nutritional circulation inthe heart: III. Effects of isoproterenol and beta adrenergicblockage on myocardial hemodynamics and rubidium- 86
extraction in the isolated supported heart preparation.J Pharmacol Exp Ther 1970;175:577-592
11. Boutet M, Huttner I, Rona G: Aspect microcirculatoire deslesions myocardiques provoquees par l'infusion de catechol-amines: Etude ultrastructurale a l'aide de traceurs de diffu-sion: 1. Isoproterenol. Path Biol 1973;21:811-825
12. Boutet M, Huttner I, Rona G: Aspect microcirculatoire deslesions myocardiques provoquees par l'infusion de catechol-amines: Etude ultrastructurale a l'aide de traceurs de diffu-sion: Norepinephrine. Path Biol 1974;22:377-387
13. Rona G, Bouter M, Huttner I: Membrane permeability alter-ations as manifestation of early cardiac muscle cell injury, inFleckenstein A, Rona G (eds): Recent Advances in Studies onCardiac Structure and Metabolism, Pathophysiology and Mor-phology ofMyocardial Cell Alterations. Baltimore, Md, Univer-sity Park Press, 1975, vol 6, pp 439-451
14. Rona G, Huttner I, Boutet M: Microcirculatory changes inmyocardium with particular reference to catecholamine-inducedcardiac muscle cell injury, in Meesen H (ed): Handbuch derallgemeinen Pathologie III7: MikrozirkulationlMicrocirculation.Heidelberg/New York, Springer, 1977, pp 791-888
15. Fleckenstein A: Specific inhibitors and promoters of calciumaction in the excitation-contraction coupling of heart muscleand their role in the prevention or production of myocardiallesions, in Harris P, Opie LH (eds): Calcium and the Heart.London, Academic Press, 1971, pp 135-188
16. Lehr D: Tissue electrolyte alterations in disseminated myocar-dial necrosis. Ann NYAcad Sci 1969;156:344-378
17. Bloom S, Davis DL: Calcium as mediator of isoproterenol-induced myocardial necrosis. Am J Pathol 1972;69:459-470
18. Bhagat B, Sullivan JM, Fischer VW, Nadel EM, Dhalla NS:cAMP activity and isoproterenol-induced myocardial injury inrats, in Kobayashi Y, Ito Y, Rona G (eds): Recent Advances inStudies on Cardiac Structure and Metabolism. Baltimore, Md,University Park Press, 1978, pp 465-470
19. Opie LH, Walpoth B, Barsacchi R: Calcium and catecholamines:Relevance to cardiomyopathies and significance in therapeuticstrategies. J Mol Cell Cardiol 1985;17(suppl 2):21-34
20. Wheatley AM, Thandroyen FT, Opie LH: Catecholamine-induced myocardial cell damage: Catecholamines or adreno-chrome. J Mol Cell Cardiol 1985;17:349-359
21. Downing SE, Lee JC: Contribution of a-adrenoceptor activa-tion to the pathogenesis of norepinephrine cardiomyopathy.Circ Res 1983;52:471-478
22. Downing SE, Chen V: Myocardial injury following endoge-nous catecholamine release in rabbits. J Mol Cell Cardiol1985;17:377-387
23. Persoon-Rothert M, van der Valk-Kokshoorn EJM, Egas-Kenniphaas JM, Mauve I, van der Laarse A: Isoproterenol-induced cytotoxicity in neonatal rat heart cell cultures ismediated by free radical formation. J Mol Cell Cardiol 1989;21:1285-1291
24. Horak AR, Podzuweit T, Opie LH: Cyclic AMP as mediator ofcatecholamine-induced enzyme release from isolated perfusedworking rat heart, in Tajuddin M, Das PK, Tariq M, Dhalla NS(eds): Advances in Myocardiology. Baltimore, Md, UniversityPark Press, 1980, vol 1, pp 367-373
25. Dhalla NS, Yates JC, Lee SL, Singh A: Functional andsubcellular changes in the isolated rat heart perfused withoxidized isoproterenol. J Mol Cell Cardiol 1978;10:31-41
26. Ferrans VJ, Hibbs RG, Black WC, Weilbaecher DG: Isopro-terenol-induced myocardial necrosis: A histochemical andelectron microscopic study. Am Heart J 1964;68:71-96
27. Singal PK, Kapur N, Dhillon KS, Beamish RE, Dhalla NS:Role of free radicals in catecholamine-induced cardiomyopa-thy. Can J Physiol Pharmacol 1982;60:1390-1397
28. Singal PK, Beamish RE, Dhalla NS: Potential oxidative path-ways of catecholamines in the formation of lipid peroxides andgenesis of heart disease. Adv Exp Med Biol 1983;161:391-401
29. Rona G: Catecholamine cardiotoxicity. J Mol Cell Cardiol1985;17:291-306
30. Mann DL, Kent RL, Cooper G IV: Load regulation of theproperties of adult feline cardiocytes: Growth induction bycellular deformation. Circ Res 1989;64:1079-1090
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

804 Circulation Vol 85, No 2 February 1992
31. Jacobson SL, Piper HM: Cell cultures of adult cardiomyocytesas models of the myocardium. J Mol Cell Cardiol 1986;18:661-678
32. Bevan JA: Norepinephrine and the presynaptic control ofadrenergic transmitter release. Fed Proc 1978;39:187-190
33. Waldenstrom AP, Hjalmarson AC, Thornell L: A possible roleof noradrenaline in the development of myocardial infarction.Am Heart J 1978;95:43-51
34. Dietz R, Schomig A, Strasser R, Kubler W: Catecholamines inmyocardial hypoxia and ischemia, in Delius W, Gerlach E,Grobecker H, Kubler W (eds): Catecholamines and the Heart.Berlin/Heidelberg/New York, Springer-Verlag, 1981, pp201-209
35. Schumann HJ, Endoh M, Wagner J: Positive inotropic effectsof phenylephrine in the isolated rabbit papillary muscle medi-ated both by a- and p-adrenoceptors. Naunyn SchmiedebergsArch Pharmacol 1974;284:133-148
36. Kimura S, Cameron JS, Kozlovskis PL, Basset AL, MyerburgRJ: Delayed afterdepolarizations and triggered activityinduced in feline Purkinje fibers by a-adrenergic stimulation inthe presence of elevated calcium levels. Circulation 1984;70:1074-1082
37. Szasz G, Gruber W, Bernt E: Creatine kinase in serum: 1.Determination of optimum reaction conditions. Clin Chem1976;22:650-656
38. Claycomb WC, Palazzo MC: Culture of the terminally differ-entiated adult cardiac muscle cell: A light and scanningelectron microscope study. Dev Biol 1980;80:466-482
39. Hewett K, Legato MJ, Danilo P, Robinson RB: Isolatedmyocytes from adult canine left ventricle: Ca2' tolerance,electrophysiology, and ultrastructure. Am J Physiol 1983;245:H830-H839
40. Cooper G IV, Mercer WE, Hoober JK, Gordon PR, Kent RL,Lauva IK, Marino TA: Load regulation of the properties ofadult feline cardiocytes. Circ Res 1986;58:692-705
41. Florio VA, Ross EM: Regulation of the catalytic componentof adenylate cyclase: Potentiative interaction of stimulatoryligands and 2',5'-dideoxyadenosine. Mol Pharmacol 1983;24:195-202
42. Newman WH, Becker BF, Heier M, Nees S, Gerlach E:Endothelium-mediated coronary dilatation by adenosine doesnot depend on endothelial adenylate cyclase activation: Stud-ies in isolated guinea pig hearts. Pflugers Arch 1988;413:1-7
43. Seamon KB, Daly JW: Forskolin: Its biological and chemicalproperties, in Greengard P, Robison GA (eds): Advances inCyclic Nucleotide and Protein Phosphorylation Research. NewYork, Raven Press, 1986, p 3
44. Cooper G IV, Kent RL, Uboh CE, Thompson EW, MarinoTA: Hemodynamic versus adrenergic control of cat rightventricular hypertrophy. J Clin Invest 1985;75:1403-1414
45. Smith PK, Krohn RI, Hermansen GT, Mallia AK, GartnerFH, Provenzano MD, Fujimoto EK, Goeke NM, Olsen BJ,Klenk DC: Measurement of protein using bicinchoninic acid.Anal Chem 1985;150:76-85
46. Osterrieder W, Brum G, Hescheler J, Trautwein W: Injectionof subunits of cyclic AMP-dependent protein kinase intocardiac myocytes modulates Ca2' current. Nature 1982;298:576-578
47. Rinaldi ML, Capony JP, Demaille JG: The cyclic AMP-dependent modulation of cardiac sarcolemmal slow calciumchannels. J Mol Cell Cardiol 1982;14:279-289
48. Tsien RW, Hess P, McCleskey EW, Rosenberg RL: Calciumchannels: Mechanisms of selectivity, permeation, and block.Ann Rev Biophys Chem 1987;16:265-290
49. Carafoli E: How calcium crosses plasma membranes includingthe sarcolemma, in Opie LH (ed): Calcium Antagonists andCardiovascularDisease. New York, Raven Press, 1984, pp 29-41
50. Dudel J, Peper K, Rudel R, Trautwein W: The effect oftetrodotoxin on the membrane current in cardiac muscle(Purkinje fibers). Pfiugers Arch 1967;295:213-226
51. Hess P, Lansman JB, Tsien RW: A novel type of cardiaccalcium channel in ventricular cells. Nature 1985;316:443-446
52. Arnsdorf MF, Bigger-JT: Effect of lidocaine hydrochloride onmembrane conductance in mammalian Purkinje fibers. J ClinInvest 1972;51:2252-2263
53. Bruschi G, Bruschi ME, Regolisti G, Borghetti A: MyoplasmicCa21-force relationship studied with fura-2 during stimulationof rat aortic smooth muscle.Am J Physiol 1988;254:H840-H854
54. Grynkiewicz G, Poenie M, Tsien RY: A new generation ofCa21 indicators with greatly improved fluorescence properties.J Biol Chem 1985;260:3440-3450
55. Kao JPY, Harootunian AT, Tsien RY: Photochemically gen-erated cytosolic calcium pulses and their detection by fluo-3.J Biol Chem 1989;264:8179-8184
56. Lundin A, Hasenson M, Persson J, Pousette A: Estimation ofbiomass in growing cell lines by adenosine triphosphate assay.Meth Enzymol 1986;133:27-42
57. Lundin A: Measurement of ATP, in Kricka LJ, Carter TJN(eds): Clinical and Biochemical Luminescence. New York,Dekker, 1982, p 43
58. Smith PK, Krohn RI, Hermansen GT, Mallia AK, GartnerFH, Provenzano MD, Fujimoto EK, Goeke NM, Olsen J,Klenk DC: Measurement of protein using bicinchonic acid.Anal Chem 1985;150:76-85
59. Winer BJ: Decision and analysis of single factor experiments,in Winer BJ (ed): Statistical Principles in Experimental Design.New York, McGraw-Hill Book Co, 1962, pp 201-205
60. Katz AM, Pappano AJ, Messineo FC, Smilowitz H, Nash-Adler P: Calcium-channel-blocking drugs, in Fozzard HA,Jennings RB, Haber E, Katz AM, Morgan HE (eds): The Heartand Cardiovascular System. New York, Raven Press, 1986, pp1597-1609
61. Fabiato A, Fabiato F: Excitation-contraction coupling of iso-lated cardiac fibers with disrupted or closed sarcolemmas:Calcium-dependent cyclic and tonic contractions. Circ Res1972;31:293-307
62. Corr PB, Shayman JA, Kramer JB, Kipnis RJ: Increaseda-adrenergic receptors in ischemic cat myocardium. J ClinInvest 1981;67:1232-1236
63. Mukherjee AZ, Haghani Z, Brady J, Bush L, McBride W, BujaLM, Willerson JT: Differences in myocardial a- and 8-adren-ergic receptor numbers in different species. Am J Physiol1983;245:H957-H961
64. Bristow MR, Minobe W, Rasmussen R, Hershberger RE,Hoffman BB: Alpha-1 adrenergic receptors in the non-failingand failing human heart. J Pharmacol Exp Ther 1988;247:1039-1045
65. Baroldi G: Human myocardial infarction: Coronarogenic andnoncoronarogenic coagulation necrosis, in Bajusz E, Rona G(eds): Recent Advances in Studies on Cardiac Structure andMetabolism: Myocardiology. Baltimore, Md, University ParkPress, 1972, vol 1, pp 399-413
66. D'Agostino AN: An electron microscopic study of cardiacnecrosis produced by 9 a-fluorocortisol and sodium phos-phate. Am J Pathol 1964;45:633-644
67. Bloom S, Sweat FW: Covariance of myocardial cyclic AMPand calcium during ,B-adrenergic stimulation in vivo. ResComm Chem Path Pharm 1974;8:505-514
68. Josue 0: Hypertrophie cardiaque causee par l'adrenaline et latoxine typhique. C R Soc Biol (Paris) 1907;63:285-286
69. Swedberg K, Waagstein F, Hjalmarson A, Wallentin I: Pro-longation of survival in congestive cardiomyopathy by beta-receptor blockade. Lancet 1979;1:1374
70. Engelmeier RS, O'Connel JB, Walsh R, Rad N, Scanlon PJ,Gunnar RM: Improvement in symptoms and exercise toleranceby metoprolol in patients with dilated cardiomyopathy: Adouble-blind, randomized, placebo-controlled trial. Circulation1985;72:536-546
71. Waagstein F, Caidahl K, Wallentin I, Bergh CH, Kjalmarson A:Long-term a-blockade in dilated cardiomyopathy. Circulation1989;80:551-563
KEY WORDS * cardiocyte * catecholamine * norepinephrine* -adrenoceptors
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from

D L Mann, R L Kent, B Parsons and G Cooper, 4thAdrenergic effects on the biology of the adult mammalian cardiocyte.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1992 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.85.2.790
1992;85:790-804Circulation.
http://circ.ahajournals.org/content/85/2/790the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 5, 2018http://circ.ahajournals.org/
Dow
nloaded from