Embed Size (px)
Citation preview

Adrenal Insufficiency

zona glomerulosa (aldosterone)
zonae fasciculata and reticularis (cortisol and adrenal androgens)
fetal zone (dehydroepiandrosterone)
androgens and estrogens.
adrenal cortex

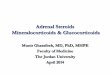
Adrenal cortex
Cortisol (glucocorticoid hormone)
Aldosterone (mineralocorticoid hormone)
Metabolism(carbohydratesproteinsfats)anti-inflammationreact to stress
Balance of Na+
K+
Adrenal Insufficiency
PrimaryAddison’s Disease Secondary

Adrenal cortex
Cortisol (glucocorticoid hormone)
Aldosterone (mineralocorticoid hormone)
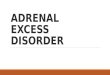
Primary Adrenal Insufficiency(Addison’s Disease)
damaged CRH(hypothalamus)
ACTH(Pituitary)
Renin-angiotensin II(Kidneys)

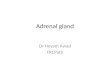
Secondary Adrenal Insufficiency
Adrenal cortex
Cortisol (glucocorticoid hormone)
CRH(hypothalamus)
ACTH(Pituitary)

Prevalence:
1-4 people per 100,000 in the US
in all ages
affects both males and females equally

Etiologyprimary adrenal insufficiency
adrenal damage
70% : autoimmune process.
30%: tuberculosis (a common cause where tuberculosis is more prevalent)
other bacterial, viral and fungal infections
adrenal hemorrhage
the spread of cancer into the adrenal glands.
genetic abnormality of the adrenal glands(rarely)

EtiologySecondary adrenal insufficiency
hypothalamus diesease
pituitary disease
Lack of ACTH receptors on adrenal cortex

Signs and Symptoms:
Abdominal pain
Decreased body hair
Dehydration (only in Addison’s disease)
Diarrhea or Constipation
Dizziness and Fainting
Fatigue
Hyperpigmentation (only in Addison’s disease - dark patches of skin, especially in the folds of the skin. Sometime black freckles on the forehead, and face and/or discoloration around areas such as the nipples, lips, and rectum)
Joint and muscle aches
Low blood pressure
Low blood sugar (hypoglycemia)
Muscle weakness
Salt craving (only in Addison’s disease)
Vomiting
Weight loss

TestsDiagnosis
Primary Secondary
(Addison’s disease) (Hypopituitarism)
Cortisol Low Low
Cortisol Low High
(ACTH stimulation test)
Aldosterone Low Normal
ACTH High Low
Renin High Normal

TestsDetermine Severity and monitor the treatment
Electrolytes (Sodium, Potassium, Chloride and Carbon dioxide) With Addison’s disease the sodium, chloride, and carbon dioxide levels are
often low, while the potassium level may be very high.
BUN and Creatinine: to monitor kidney function.
Glucose: may be very low during an addisonian crisis.

TestsOccasionally used tests
Insulin-induced hypoglycemia test. Glucose and cortisol levels are measured at predetermined intervals after an injection of insulin is used to stress the pituitary glands. In healthy people, blood glucose levels fall and cortisol concentrations increase. In those with adrenal insufficiency cortisol levels will remain low and glucose levels will fall then recover slowly.
21-hydroxylase autoantibodies. ordered when autoimmune Addison’s disease is suspected. They are considered a good marker of autoimmune Addison's disease but are not widely used at this time.

TestsNon-laboratory
X-rays: calcification on the adrenal cortex that may be due to a tuberculosis infection.
CT or MRI: size and shape of the adrenal glands and the pituitary. (The adrenal glands can be enlarged with infections and cancers. With autoimmune diseases and secondary adrenal insufficiency the adrenal glands are often normal or small in size.)

Treatment
There is usually no cure for primary adrenal insufficiency, unless the cause is an infection, in which case, patients may regain some adrenal function. However, even when damage to the adrenal cortex is extensive and permanent, persons with Addison’s disease should be able to live healthy, relatively normal lives by replacing the missing hormones and observing a few precautions.
In the case of secondary adrenal insufficiency, it is very rare for a patient to respond to treatment if the cause is pituitary damage or disease. However, if the underlying condition can be resolved, such as if the insufficiency is due to corticosteroid therapy, cortisol production may eventually resume.