Embed Size (px)
Citation preview

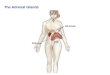
Adrenal Cortex• Divided into three zones • Zona glomerulosa (outer layer) produces
mineralocorticoids, mostly aldosterone.– Aldosterone causes kidneys to reabsorb (keep) sodium
and water, and lose potassium and H+. – Control is by K+ levels in blood (only mildly by Na+) and
by renin-angiotensin- aldosterone pathway.


• Zona Fasciculata (middle layer) produces glucocorticoids, mostly cortisol (hydrocortisone)– Regulate metabolism, esp. of glucose, and resistance
to stress.– Increase protein breakdown and decrease synthesis,
raising blood amino acid levels.– Lipolysis – promotes breakdown of adipose tissue,
increasing use of fatty acids for energy and decreasing use of glucose
– Gluconeogenesis – production of new glucose from other substances, increasing blood glucose

• Resistance to stress – increased glucose is available to tissues, and makes blood vessels more sensitive to agents that cause vasoconstriction
• Anti-inflammatory effects – inhibits cells that participate in inflammatory response – slower wound healing
• Depression of the immune response – prevents rejection of transplanted organs, but decreases resistance to infection.

• Control : through blood levels of cortisol and ACTH which is controlled by hypothalamus through corticotropin releasing hormone.
• Hyposecretion leads to Addison’s disease• Hypersecretion leads to Cushing’s syndrome

• Zona Reticularis (inner layer) – produces androgens (male sex hormones).
• These are overwhelmed by testosterone in males and so are insignificant.
• In females, they contribute to the female sex drive, and may be converted into estrogen in other tissues, which is especially important after menopause.

Adrenal gland:A. Adrenal cortex:
I. Hyper-corticism (Cushing’s syndrome):It is clinical picture produced by prolonged
increases in plasma glucocoricoids. The caused of increase of glucocorticoids
(which either exogenous or endogenous) or due to excess ACTH (which is also
either exogenous or endogenous).

The clinical characteristics of the disease will depend on the physiological functions of glucocorticoid:
•Protein depletion: it will cause protein catabolism and will end to cause the skin and subcutaneous tissues are thinmuscles are poorly developed wounds heals poorlyminor injures causes bruises and ecchymosed hair is thin and scraggly (atrophied),
facial hair, and acne.•Fat distribution: the extremities are thin, but fat collected in
abdominal wall, face, and upper back, where it produces a “buffalo hump”. As the thin skin of abdomen is stretched by the increased
subcutaneous fat depots, the sub-dermal tissue rupture to form prominent reddish-purple striae.
•Many amino acids liberated from catabolized protein are converted into glucose in the liver, and the result is hyperglycemia.

•The excess gluco-corticoid may exert a significant mineralo-corticoid action.
•About 85% of patients are hypertensive.•Bone dissolution: this is due to decrease bone
formation and increase bone resorption (osteoporosis)
•Mental effects: mental aberration ranging from increase appetite, insomnia, and euphoria to
psychosis.

CUSHING’S Syndrome(TOO MUCH CORTISOL!)
• secretion of cortisol from adrenal cortex• 4X more frequent in females• Usually occurs at 35-50 years of age
*Cushing’s disease if due to inc ACTH secreting tumor from pituitary
HYPER AND HYPOFUNCTION ADRENAL CORTEX HORMONES: Too much: Too little

II. Hyper-aldosteronsim: 1.It cause by primary (Conn’s syndrome: adrenocortical
adenoma) or secondary: caused by edema (cirrhosis, nephritic syndrome, cardiac failure). It is characterized clinically by hypertension, Na and water retention, and
hypokalemia, often with hypokalemic alkalosis. III. Hypo-corticism (Addison’s disease):
1.It either caused by primary which is idiopathic adrenal atrophy or secondary which caused by infection most
tuberculosis. It is characterized by hypotension, increased pigmentation of skin; decrease serum Na, Cl, glucose, and
bicarbonate; and increased serum K.

Addison’s Disease: Etiology/Pathophysiology• Common cause-autoimmune response to adrenal tissue (esp. white
females)• Susceptibility genes; other endocrine conditions often found• Other causes of Addison’s disease
– Tuberculosis (rare in North America)– Infarction– Fungal infections– AIDS– Metastatic cancer– Most often occurs in adults <60 years old
• Affects both genders equally• Disease not evident until 90% of adrenal cortex destroyed- advanced
before diagnosis

Addison’s Disease: Clinical Manifestations
• Primary features – Progressive weakness– Fatigue– Weight loss– Anorexia – Skin hyperpigmentation
primarily in• Areas exposed to sun• Pressure points• Over joints

Addison’s Disease: Diagnostic Studies• Subnormal levels of serum cortisol • Levels fail to rise over basal levels with ACTH stimulation test– Latter indicates primary adrenal disease – Positive response to ACTH stimulation indicates functioning
adrenal gland• Abnormal laboratory findings– Hyperkalemia– Hypochloremia– Hyponatremia– Hypoglycemia

Addison’s Disease-Diagnostic Studies
• Abnormal laboratory findings – Anemia– Low urine cortisol levels– ECG• Low voltage, vertical QRS axis, peaked
T waves from hyperkalemia• CT and MRI used to– Localize tumors – Identify adrenal calcifications or enlargement

• Usually due to adrenal tumor
• Too much aldosterone secretion– Sodium retention
(hypernatremia)– Potassium excretion
(hypokalemia)• Muscle weakness• Fatigue• Cardiac dysrhythmias• Glucose intolerance• Metabolic alkalosis
– Hydrogen ion excretion
HYPERALDOSTERONISM (Conn’ Syndrome)
*Hallmark- hyperaldosteronism•Hypertension with hypokalemic alkalosis
•Usually no edema•Headache

Review renin/aldosterone effect!

Hyperaldosteronism Etiology and Pathophysiology
• Primary hyperaldosteronism – Usually caused by adrenocortical adenoma
• Secondary hyperaldosteronism – Due to renal artery stenosis,
renin-secreting tumors, and chronic kidney disease

DIAGNOSIS/INTERVENTIONS-Hyperaldosteronism
• Primary aldosteronism– ↑ Plasma aldosterone
levels– ↑ Sodium levels– ↓ Potassium levels– ↓ Renin activity
• Adenomas are localized by CT or MRI
Preferred treatment of primary hyperaldosteronism is surgical removal of the adenoma (ADRENALECTOMY)

Adrenal Medulla• Made up of hormone producing cells called
chromaffin cells, which surround large blood vessels.
• Sympathetic postganglionic cells that are specialized to secrete hormones which are sympathomimetic.
• Secretions are 80% epinephrine and 20 % norepinephrine

• Control through nervous impulses that originate in the hypothalamus
• Not essential for life• Tumors are called pheochromocytomas, and
produce extended “Fight or Flight” response. Treated by surgical removal of tumor.

PHEOCHROMOCYTOMA
• Rare, benign tumor of the adrenal medulla• Produces excessive _________• Mostly in young to middle-aged adults• Results in severe hypertension• If untreated, may lead to – Diabetes mellitus– Cardiomyopathy– Death
catecholamines

Clinical Manifestations
• Hallmark-hypertension-200/150 or greater• “Spells”-paroxymal attacks– bladder distension,emotional distress, exposure to cold.
• Norepinephrine and Epinepherine released sporadically• Clinical features include– Severe, episodic hypertension– Severe, headache– Tachycardia with palpitations– Profuse sweating– Abdominal or chest pain
• Diagnosis is often missed

DIAGNOSIS
• Best test- Urinary fractionated metanephrines (catecholamines metabolites)
• Plasma catecholamines (elevated during an attack)• 24 hour urine- (metabolite of Epinepherine)• CT/MRI to locate tumor

Pheochromocytoma Treatment
• Surgical removal of tumor• Medications
– Calcium channel blockers control BP• nicardipine (Cardene)
– Sympathetic blocking agents may ↓ BP ; ↓ Symptoms of catecholamine excess
– Beta blockers to ↓ dysrhythmias, BP• Inderal
• Diet– high in vitamin, mineral, calorie, no caffeine
• Sedatives