Embed Size (px)
Citation preview

AJR:201, November 2013 1009
to 5:1 in some studies [5–7], with exclusively female patients in one series [8].
Adrenal cysts are usually unilateral, with-out a predilection for the right or left side. Patients are usually asymptomatic. Howev-er, abdominal pain, abdominal mass, flank pain, spontaneous intracystic hemorrhage, and cyst rupture have been reported [1], as well as posttraumatic cyst rupture with mas-sive retroperitoneal hemorrhage [9]. Arteri-al hypertension has also been reported in as-sociation with adrenal cysts, as well as cases of resolution of hypertension after cyst re-moval [10–15].
Adrenal Cysts: Natural History by Long-Term Imaging Follow-Up
Zina Ricci1Victoria ChernyakKevin HsuFernanda S. MazzariolMilana FlusbergSarah OhMarjorie SteinAlla Rozenblit
Ricci Z, Chernyak V, Hsu K, et al.
1All authors: Department of Diagnostic Radiology, Montefiore Hospital, 111 E 210th St, Bronx, NY 10467. Address correspondence to Z. Ricci ([email protected]).
Genitour inar y Imaging • Or ig ina l Research
AJR 2013; 201:1009–1016
0361–803X/13/2015–1009
© American Roentgen Ray Society
Adrenal cysts are uncommon, with a reported combined autopsy in-cidence of 0.073% (14/19,096) [1]. They are discovered inciden-
tally on imaging examinations, with a preva-lence of 1% reported by Song et al. [2] in a large series of 1049 adrenal lesions. Earlier in-vestigators have reported a higher prevalence of adrenal cysts in much smaller series [3–5].
Adrenal cysts have been reported in pa-tients of all ages, with a peak incidence be-tween the third and sixth decades [6, 7]. They have a definite female predilection, with a female-to-male ratio ranging from 2:1
Keywords: adrenal cyst, adrenal gland, CT, MRI, ultrasound
DOI:10.2214/AJR.12.9202
Received May 3, 2012; accepted after revision January 7, 2013.
OBJECTIVE. The purpose of this article is to determine the natural history of adrenal cysts on the basis of long-term imaging follow-up.
MATERIALS AND METHODS. This retrospective study included patients with adrenal cysts who had at least 12 months of imaging follow-up (1993–2010). Medical records were re-viewed. Two radiologists reviewed imaging examinations in consensus and recorded wall thick-ness (thin, ≤ 3 mm; thick, > 3 mm), septations, and calcification. CT attenuation value, MRI signal intensity, the presence or absence of enhancement, and typical sonographic features were used to confirm fluid content of the lesions. Cyst wall enhancement was recorded (thin, ≤ 3 mm and smooth; thick, > 3 mm). Cyst diameter on the initial and most remote follow-up examina-tions was compared. The Wilcoxon matched-pairs signed rank test was applied to assess statis-tically significant differences in size and CT attenuation on follow-up examinations.
RESULTS. Twenty patients with unilateral adrenal cysts (seven male and 13 female pa-tients; mean age, 44 years; range, 10–75 years) had a mean imaging follow-up period of 64 months (range, 12–198 months). CT, MRI, and ultrasound examinations were obtained in 19, 11, and 13 patients, respectively. Cysts were diagnosed by lack of enhancement on CT or MRI in 12 patients, typical sonographic features in three patients, and combination of CT and sonographic or MRI features in five patients. Signal intensities typical for fluid were found on all MRI examinations, attenuations of less than 20 HU on 17 of 19 (89%) CT examina-tions, and features of either simple or mildly complicated cysts on all sonograms. Thin walls, wall calcifications, and thin septations were found in 20 (100%), 12 (60%), and four (20%) lesions, respectively. During the follow-up of 20 lesions, the median cyst diameter increased by 26.0% (interquartile range, 6.8–68.4%) in 12 (60%) patients, decreased by 32.9% (inter-quartile range, 7.1–42.8%) in six (30%) patients, and was unchanged in two (10%) patients. The median baseline CT attenuation values did not significantly change on follow-up CT ex-aminations (p = 0.72). No patient developed a complication of adrenal cyst. Four patients had histologically confirmed benign adrenal cysts.
CONCLUSION. Interval enlargement of an adrenal cyst is frequent and as an isolated finding does not indicate malignancy or presence of a complication. However, some adrenal cysts may decrease or remain stable in size over time.
Ricci et al.Long-Term Imaging Follow-Up of Adrenal Cysts
Genitourinary ImagingOriginal Research
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by N
atio
nwid
e C
hild
ren'
s H
ospi
tal o
n 10
/24/
13 f
rom
IP
addr
ess
164.
107.
116.
242.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

1010 AJR:201, November 2013
Ricci et al.
Adrenal cysts are categorized into four ma-jor histopathologic types: endothelial (45%), pseudocysts (39%), epithelial (9%), and par-asitic (7%) [6, 16]. Endothelial cysts are the most common and include two subtypes: lymphangiomatous (42%) and hemangioma-tous (3%) cysts [16]. Pseudocysts, the sec-ond most common pathologic type of adrenal cysts, have walls composed of fibrous tissue because they lack an epithelial or endothelial lining [17]. They are thought to be a result of a prior adrenal hemorrhage [18]. Other authors have proposed that, on the basis of immuno-histochemical studies, pseudocysts are close-ly related to endothelial cysts [19]. Epithelial cysts are rare and include congenital glan-dular (retention) cysts, cystic adenomas, and other unspecified cysts, including mesotheli-al cysts [1]. Parasitic cysts, the rarest cause of adrenal cysts, are due to disseminated infec-tion with Echinococcus granulosus, but rarely adrenal involvement can be isolated [15].
The imaging features of uncomplicated adrenal cysts are usually straightforward and similar to those of benign renal cysts [20, 21]. Because adrenal cysts are rare, their natural history is not well established, to our knowledge, in the imaging or clinical litera-ture. The purpose of our study was to evalu-ate the natural history of adrenal cysts.
Materials and MethodsPatients
Our retrospective study received institution-al review board approval and was HIPAA com-pliant. Informed consent was waived. The med-ical record discharge database system, radiology information system, and our institutional patient database were searched for key words “adrenal cyst,” “adrenal pseudocyst,” and “adrenal lymph-angioma.” The database was searched from 1992 to 2010 by one author, and the information was then reviewed by two abdominal radiologists. Pa-tients with adrenal cysts diagnosed by CT, MRI, or ultrasound who had at least 12 months imaging follow-up were included in the study.
Medical records of each patient were reviewed to determine any history of malignancy or hyper-tension or both. Laboratory data, including uri-nary vanillylmandelic acid, urine catecholamine, or serum aldosterone, were recorded, when avail-able. Radiology reports were reviewed to deter-mine the clinical indication for initial imaging in each patient, as well as to establish the length of imaging follow-up.
Exclusion criteria included less than 12 months of imaging follow-up and lack of imaging stud-ies for review.
Image AnalysisTwo board-certified fellowship-trained abdom-
inal radiologists with 27 and 11 years of experi-ence, respectively, reviewed all available imaging examinations (CT, MRI, and ultrasound) in con-sensus. The reviewers were blinded to the pathol-ogy findings at time of imaging review; they were aware of the imaging diagnosis of adrenal cyst. For each cyst, the following features were record-ed on both the initial and most recent examina-tion: laterality, size, wall thickness (thin or thick), presence or absence of wall calcification, presence or absence of septations, attenuation values on CT, signal intensity on both T1- and T2-weighted se-quences on MRI, presence or absence of T2-hy-pointense rim on MRI, presence or absence of en-hancement on MRI or CT, and echogenicity on ultrasound. Each cyst was measured in two or-thogonal planes on an axial image. Craniocau-dal dimensions were not recorded because many of the older CT scans did not have coronal recon-structions available. A thin wall was defined as an imperceptible wall or a wall measuring 3 mm or less. A thick wall was defined as a wall measuring greater than 3 mm. If the most recent examination was an MRI, the attenuation values of the cyst on the most recent prior CT were recorded. If a cyst
had interim modalities different from the initial or the most recent ones, imaging characteristics on the interim modalities were recorded as well.
The CT criteria for adrenal cysts included at-tenuation values less than 20 HU on contrast-enhanced CT or a lack of contrast enhancement between unenhanced and contrast-enhanced im-ages, defined as less than 10 HU difference [20]. For a cyst with attenuation value 20 HU or great-er on contrast-enhanced CT and for any cyst im-aged with unenhanced CT alone, confirmation of the cystic nature by another imaging modality was required. The MRI criteria for adrenal cysts included hypointensity on T1-weighted sequenc-es, hyperintensity on T2-weighted sequenc-es, and lack of contrast enhancement, defined as less than 15% increase in signal intensity on contrast-enhanced images compared with unen-hanced images [22], or absence of signal within the cyst on subtraction images. The presence of wall enhancement was recorded as thin (smooth and ≤ 3 mm) or thick (> 3 mm) on enhanced CT and MRI examinations. On ultrasound, an adre-nal cyst was diagnosed if it was anechoic or hy-poechoic with low-level internal echoes, exhib-ited posterior acoustic enhancement, and lacked internal flow on Doppler examination.
TABLE 1: Summary of Patients Presenting Clinical Features at Time of Initial Examination
Patient No. Age (y) Sex Clinical Indication Hypertension
1 46 Female Abdominal pain Yes
2 54 Male Abdominal pain Yes
3 49 Female Abdominal pain No
4 64 Male Suspected retroperitoneal bleed No
5 25 Male Chest pain No
6 44 Male Pain and vomiting No
7 64 Female Hematuria, known left adrenal mass Not available
8 12 Female Right abdominal pain, vomiting No
9 35 Male Abdominal pain Yes
10 41 Female Abdominal pain, pseudoobstruction Not available
11 75 Female Right upper quadrant pain, hypertension Yes
12 32 Female Abdominal pain Not available
13 41 Female Left flank pain, hematuria, constipation No
14 36 Female Back pain, rule out disk herniation No
15 55 Female Elevated liver function tests Yes
16 37 Female Right upper quadrant pain No
17 45 Female Diabetes and proteinuria, suspected hydronephrosis Yes
18 29 Male Left lower quadrant pain No
19 45 Female Follow-up of adrenal mass Not available
20 54 Male Suspected suprarenal mass on excretory urogram for renal colic
Not available
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by N
atio
nwid
e C
hild
ren'
s H
ospi
tal o
n 10
/24/
13 f
rom
IP
addr
ess
164.
107.
116.
242.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:201, November 2013 1011
Long-Term Imaging Follow-Up of Adrenal Cysts
Technical ParametersTwenty-nine (19 initial and 10 follow-up) CT
examinations were performed on various CT scanners: LightSpeed QX/I (n = 4), HiSpeed Advantage (n = 1), HiSpeed CT/I (n = 8), and LightSpeed 16 (n = 6) (all from GE Healthcare) and Brilliance CT 16 (n = 10) (Philips Health-care). Images were acquired with a variable col-limation and had a reconstructed thickness of 5, 7, or 10 mm. IV contrast agents included iohexol (Omnipaque 300, Nycomed) or diatrizoate sodi-um (Hypaque 60, Amersham Health). Of the ini-tial 19 CT examinations, two patients underwent CT before and after IV administration of contrast agent, 10 underwent contrast-enhanced CT only, and seven underwent unenhanced CT only. Of the 10 follow-up CT examinations, three patients un-derwent contrast-enhanced CT and 10 underwent unenhanced CT.
Eleven MRI examinations were performed be-fore and after IV administration of 15–20 mL of gadopentetate dimeglumine (Magnevist, Bayer Healthcare Pharmaceuticals). The studies were obtained using 1.5-T magnets, either Philips ACS-NT (Philips Healthcare) (n = 5) or Signa Excite HD12 (GE Healthcare) (n = 6).
Thirteen ultrasound examinations were per-formed using an Acuson 128 XP (Siemens Health-care) for seven patients, ATL HDI 5000 (Philips Healthcare) for three patients, and Acuson Se-quoia 512 (Siemens Healthcare) for three patients.
Statistical AnalysisThe statistical analysis was performed using
STATA software (version 12.2, StataCorp). The data are reported as median and interquartile range (IQR) because of nonnormal distribution. The difference between mean CT attenuation val-ues of the initial and follow-up examinations was assessed using Wilcoxon matched-pairs signed rank test. A statistically significant difference was considered at p values less than 0.05.
ResultsThe initial database search yielded 28
patients. Eight patients were excluded be-cause of insufficient follow-up (n = 4), lack of available imaging studies (n = 1), imaging with unenhanced CT only, which precluded differentiation of an adrenal cyst from a low-attenuation lipid-rich adenoma (n = 2), and an extraadrenal origin of the cyst in a pa-
tient with a pathologically proven left subdi-aphragmatic bronchogenic cyst that was mis-diagnosed as an adrenal cyst on CT (n = 1).
The final study population consisted of 20 patients, including seven (35%) male and 13 (65%) female patients (mean age, 44 years; range, 10–75 years). Indications for the ini-tial imaging studies are summarized in Ta-ble 1. The most common clinical indication for the initial imaging study was abdominal or flank pain, seen in 12 (60%) patients. Five (25%) patients were imaged for varying rea-sons (suspected retroperitoneal bleed, chest pain, suspected disk herniation, abnormal liver function tests, or suspected hydrone-phrosis). In three (15%) patients, adrenal le-sions were initially diagnosed or were sus-pected on outside imaging studies that were not available for our review: one of these pa-tients presented with hematuria, one had re-nal colic, and one was referred for follow-up of an asymptomatic adrenal cyst. Only one patient had a known history of malignancy (colon carcinoma). Six (30%) patients had a history of hypertension. Two patients had an available endocrine biochemical profile, ob-
A
D
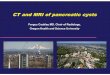
Fig. 1—41-year-old woman with incidental right adrenal cyst that decreased in size from 3.5 cm (not shown) to 2 cm at 16.5-year follow-up performed for nonspecific abdominal pain. A, Unenhanced CT scan with oral contrast agent only shows 2-cm hypoattenuated (17 HU) cyst (arrow) in right adrenal gland. B, Corresponding axial CT scan with IV and oral contrast agent shows no enhancement (17 HU) within cyst (arrow) and thin wall. C, Axial gradient-recalled echo in-phase sequence shows corresponding hypointense right adrenal cyst (arrow). D, Axial T2-weighted sequence shows hyperintense cyst (arrow) with thin dark wall. E, Axial enhanced gradient-recalled echo T1-weighted image shows thin rim enhancement of cyst (arrow). F, Corresponding subtraction image confirms only minimal wall enhancement (arrow).
C
F
B
E
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by N
atio
nwid
e C
hild
ren'
s H
ospi
tal o
n 10
/24/
13 f
rom
IP
addr
ess
164.
107.
116.
242.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

1012 AJR:201, November 2013
Ricci et al.
tained to exclude occult pheochromocytoma (n = 2). The median imaging follow-up peri-od was 45 months (IQR, 16.2–99.8 months). The indications for follow-up examinations in our series included follow-up of adrenal mass for 13 (65%) patients and abdominal or flank pain for seven (35%) patients.
The lesions were imaged by either a single imaging modality or a combination of two or three modalities (CT, ultrasound, or MRI),
as summarized in Table 2. The initial im-aging studies included 13 (65%) CT scans, five (25%) ultrasound examinations, and two (10%) MRI examinations. The final follow-up imaging studies included 13 (65%) CT scans, two (10%) ultrasound examinations, and five (25%) MRI examinations.
The imaging features of the lesions are summarized in Table 2. Of the 20 lesions, cystic nature was confirmed by a lack of en-
hancement on either CT or MRI in 12 (60%) cases, sonographic features of a simple cyst in three (15%) cases, and by pathologic anal-ysis in five (25%) cases. Of the 20 lesions, 11 (55%) were located on the right and nine (45%) were on the left. The median largest diameter of the lesions was 4.2 cm (IQR, 3.4–7.4 cm) on the initial study and 4.7 cm (IQR, 3.8–7.4 cm) on the latest follow-up study (p = 0.24). During the follow-up of 20
TABLE 2: Imaging Modalities Used and Features of the Adrenal Lesions
Patient No.
CT TechniqueCT Mean
Attenuation (HU)a
Ultrasound Echogenicity
MRI
SeptationsCT Wall
CalcificationsPathologic
FindingsInitial Follow-UpT1-
WeightedT2-
WeightedT2-
Hypointense Rim
1 No IV contrast agent
8.1 Hypoechoic Low High No None None
2 No IV contrast agent
No IV contrast agent
16.1 Anechoic None Rim, smooth
3 With IV contrast No IV contrast agent
14.8 Low High Yes Thin Rim, smooth
4 With and without IV contrast agent
No IV contrast agent
18.0 Anechoic None None
5 With IV contrast 19.9 None None Endothelial cyst
6 With IV contrast No IV contrast agent
16.5 Low High Yes None Nodular
7 With and without IV contrast agent
With IV contrast 15.0 None None
8 With IV contrast 15.5 Anechoic None None Aspiration: straw-colored clear fluid
9 With IV contrast 22.0 Low High Yes None Rim, smooth Pseudocyst within degenerated adenoma
10 With IV contrast No IV contrast agent
16.0 Anechoic Low High Yes None Rim, smooth
11 No IV contrast agent
20.0 Low High No Noneb None
12 With IV contrast 16 Anechoic Thin None Lymphangioma
13 With IV contrast No IV contrast agent
17.0 Hypoechoic Low High Yes Thin Rim, smooth
14 No IV contrast agent
With IV contrast 28 Hypoechoic Low High Yes None Rim, smooth
15 No IV contrast agent
21 Hypoechoic Low High No None Rim, smooth
16 Anechoic None Nodular
17 With IV contrast 17 Hypoechoic Low High Yes Thin Nodular
18 No IV contrast agent
No IV contrast agent
8.0 Anechoic None None Benign unspecified adrenal cyst
19 No IV contrast agent
19.0 Low High No None Nodular
20 With IV contrast With IV contrast 17.0 Hypoechoic None Rim, smoothaMean attenuation in Hounsfield units on initial CT performed.bCyst contained nonenhancing wall nodule.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by N
atio
nwid
e C
hild
ren'
s H
ospi
tal o
n 10
/24/
13 f
rom
IP
addr
ess
164.
107.
116.
242.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:201, November 2013 1013
Long-Term Imaging Follow-Up of Adrenal Cysts
lesions, the median cyst diameter increased by 26.0% (IQR, 6.8–68.4%) in 12 (60%) pa-tients, decreased by 32.9% (IQR, 7.1–42.8%) in six (30%) patients, and was unchanged in two (10%) patients. Table 3 summarizes the radiologic surveillance of the cyst sizes.
Of the nine patients who underwent two CT scans, the initial median attenuation was 16.1 HU (IQR, 15–17 HU), and the follow-up me-dian attenuation was 16 HU (IQR, 13–18 HU) (p = 0.72). Three (15%) lesions had attenua-tion values higher than that of simple fluid (> 20 HU). The cystic nature of these three mildly hyperdense lesions was confirmed by MRI. On MRI, all 11 lesions (100%) had signal intensity typical for simple fluid, showing high signal in-tensity on T2-weighted sequences and low sig-nal intensity on T1-weighted sequences. Of the 11 lesions imaged with MRI, seven (64%) ex-hibited a hypointense rim on T2-weighted se-quences (Figs. 1 and 2). Of 13 lesions that un-derwent at least one ultrasound, seven (54%) were anechoic and six (46%) were hypoecho-ic with low-level internal echoes. Of the six le-sions that were hypoechoic on ultrasound, five (83%) were confirmed to be cystic on MRI and one (17%) was confirmed to be cystic on con-trast-enhanced CT alone. One cyst contained a smoothly marginated wall nodule that lacked flow on color Doppler images and was non-enhancing on MRI (Fig. 3).
A thin wall was present in all 20 (100%) lesions on all modalities. On unenhanced CT, peripheral wall calcification was seen in eight of 13 (62%) lesions, whereas the wall was imperceptible in 10 (77%) lesions. On contrast-enhanced CT, discernible smooth wall enhancement was seen in four of thir-teen (31%) lesions. Of the nine lesions with no visible enhancing wall, continuous wall calcification precluded assessment of an en-hancing wall in three (33%) lesions, the wall was imperceptible in three (33%) lesions, and noncontiguous rim calcification was seen in three (33%) lesions. On contrast-en-hanced MRI, a discernible thin enhancing wall was seen in 10 of 11 (91%) lesions. Thin septations were found on at least one of the modalities in four of 20 (25%) lesions. Cal-cifications on CT or ultrasound were found in 12 of 20 (60%) lesions; all calcifications were peripheral, within the cyst wall. In eight of these 12 cases (67%), calcifications were smooth, and in four (33%) cases, calci-fications were nodular (Fig. 4). The presence or absence and imaging appearance of sep-tations or calcifications was stable over the follow-up period in 19 of 20 (95%) cases; in
one (5%) case, there was an increase in rim calcification on the follow-up examination. None of the 20 patients developed complica-tions related to the adrenal cyst, such as hem-orrhage or malignant transformation, during the follow-up period.
Four patients underwent adrenalectomy, with pathologic confirmation as follows: two endothelial adrenal cysts, one pseudocyst probably resulting from a degenerated adeno-ma, and one unspecified benign cyst. These patients were treated surgically because all were physically active young adults (25, 29, 32, and 35 years old, respectively), who were considered to be at increased risk for poten-tial cyst rupture or hemorrhage. Three of them had lesions that exhibited growth on follow-up examinations, and one had a stable large cyst measuring 8.5 cm. A fifth patient with right upper quadrant pain, a 12-year-old girl, underwent CT-guided cyst aspiration of a growing cyst that yielded straw-colored flu-id and no malignant cells. The parents of the child declined surgical treatment, which was suggested by the pediatrician, and chose a diagnostic aspiration.
DiscussionAdrenal cysts are rare benign lesions, with
the majority being either endothelial lym-phatic cysts or pseudocysts. These are occa-sionally detected by cross-sectional imaging studies that are performed for unrelated in-dications. Because of the rarity of these le-sions, their natural history is not well estab-lished in the imaging or clinical literature, to our knowledge, and patient management re-mains controversial.
Some older literature suggests an asso-ciation between adrenal cysts and other be-nign and malignant adrenal tumors. Abes-house et al. [6] reviewed the prior literature and reported a small number of pseudocysts to have a neoplastic origin, including ade-nomas, pheochromocytomas, and one ma-lignancy. In a review of 515 adrenal cysts, Neri and Nance [1] described 56% of the ad-renal pseudocysts in their series, with 37% being hemorrhagic, 1% associated with ade-nomas, 4% associated with pheochromocy-tomas, 2% associated with neuroblastomas, 1% associated with adrenocortical carci-nomas, less than 1% being metastatic, and
TABLE 3: Summary of Size and Follow-Up of Adrenal Lesions
Patient No.Duration of
Follow-Up (mos)Largest Initial
Size (cm)Largest Final
Size (cm) Change (%)Absolute Value of
Percentage Change
1 14.7 4.2 3.9 −7.14 7.14
2 28.8 10 11 10 10
3 47.5 3.3 3.4 3.03 3.03
4 111.9 5.8 6.3 8.62 8.62
5 54.5 6.3 8 26.98 26.98
6 42.6 8.9 6.1 −31.46 31.46
7 13.6 4.2 4.4 4.76 4.76
8 13.3 4.3 6.7 55.81 55.81
9 17.8 4 5 25 25
10 62.6 3.7 6.7 81.08 81.08
11 142.8 2.5 9.5 280 280
12 14.2 8.5 8.5 0 0
13 197.8 3.5 2 −42.86 42.86
14 75.2 8.3 3.6 −56.63 56.63
15 87.8 6.4 4.2 −34.38 34.38
16 11.6 3.3 3.3 0 0
17 113.2 4 4.2 5 5
18 27.6 2.8 4 42.86 42.86
19 35.9 3.2 3 −6.25 6.25
20 169.8 8.9 20 124.72 124.72
Median 45.0 4.2 4.7 4.9 26.0
Interquartile range 16.2–99.8 3.4–7.4 3.8–7.4 −6.7 to 34.9 5.6–49.3
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by N
atio
nwid
e C
hild
ren'
s H
ospi
tal o
n 10
/24/
13 f
rom
IP
addr
ess
164.
107.
116.
242.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

1014 AJR:201, November 2013
Ricci et al.
less than 1% as unspecified malignancies. In a series of 41 adrenal cysts, Erickson et al. [23] found six pseudocysts associated with adrenal neoplasms, including two adre-nal cortical carcinomas, two adenomas, and two pheochromocytomas. Chien et al. [24] in a histopathologic analysis found seven of 16 adrenal pseudocysts to be associated with tumors, including two pheochromocytomas, one neuroblastoma, one adrenal cortical car-cinoma, one adenoma, one myelolipoma, and one schwannoma. However, in none of these series were the radiologic features of
the lesions described, and it is unlikely that the included lesions (most of which were de-scribed as pseudocysts) would meet the im-aging criteria of an uncomplicated or mildly complicated cyst.
As shown by prior investigations and as confirmed by our series, the imaging features of a benign adrenal cyst are similar to those of a benign simple or mildly complicated re-nal cyst, except for slightly greater accept-able wall thickness and wall calcification for an adrenal cyst [21]. In our series, most adre-nal cysts were of fluid attenuation on CT, with
only 15% of lesions having an attenuation val-ue greater than 20 HU. They had the typical features of either simple or mildly compli-cated cysts on ultrasound, and typical signal intensity of a cyst on MRI. On MRI, a thin T2-hypointense rim was seen in 64% of our cases. All cases in our series exhibited a thin wall; smooth wall enhancement was more fre-quently seen on MRI than on CT. Some le-sions exhibited mildly complicated features, including calcifications visible on CT or ultra-sound or septations seen on all or some of the modalities. Thin septations and wall calcifi-
A
Fig. 2—55-year-old woman with history of hypertension with incidental left adrenal cysts that decreased in size on 7.3-year follow-up MRI examination (performed for follow-up of asymptomatic adrenal cyst). A, Axial CT scan with oral and IV contrast agent performed 1 year after initial examination shows 6.4-cm stable hypodense (21 HU) cyst (arrow) with thin wall and focal thin rim calcification. B, Follow-up axial T2-weighted MRI shows contracted 4.2-cm homogeneously hyperintense cyst (arrow).
B
A
D
Fig. 3—75-year-old woman with history of hypertension with incidental left adrenal cyst that increased in size from 2.5 cm (not shown) to 9.5 cm on follow-up sonogram and MRI (performed 11.9 years later for follow-up of adrenal cyst). A, Sagittal gray-scale sonogram shows 9.5-cm anechoic cyst with heterogeneously echogenic nodule (arrow) adjacent to wall. B, Corresponding color Doppler image shows lack of flow (arrow). C, Axial gradient-recalled echo T1-weighted sequence shows hypointense cyst (arrow) with hyperintense smoothly marginated wall nodule (arrowhead). D, Axial T2-weighted sequence shows T2-hyperintense cyst (arrow) containing T2-hypointense nodule (arrowhead). E, Axial contrast-enhanced gradient-recalled echo T1-weighted sequence shows thin wall enhancement (arrow) with hyperintense nodule (arrowhead). F, Corresponding subtraction image shows thin wall enhancement (arrow) and lack of enhancement within nodule (arrowhead), which is compatible with adherent loculated debris within cyst.
C
F
B
E
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by N
atio
nwid
e C
hild
ren'
s H
ospi
tal o
n 10
/24/
13 f
rom
IP
addr
ess
164.
107.
116.
242.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:201, November 2013 1015
Long-Term Imaging Follow-Up of Adrenal Cysts
cations were commonly seen in our series (in 25% and 60% of cases, respectively).
Thirty percent of patients in our series had hypertension. However, because of the over-all high incidence of benign essential hyper-tension, we cannot draw any conclusions about whether the adrenal cysts are precipitating fac-tors in hypertensive disease in these patients.
Management of adrenal cysts is controver-sial and is based on clinical and pathologic data. Traditionally, surgical treatment is in-dicated for lesions that are functional, ma-lignant, or parasitic in origin [8, 15]. Previ-ous literature states that hormonal workup is necessary to identify hormonally active le-sions, including those that are subclinical [8, 25–27]. Also, biochemical screening for pheochromocytoma is reported to be manda-tory because of its high rate of morbidity and mortality and its unpredictable course.
The differential diagnosis of adrenal cyst includes several entities. On unenhanced CT, a lipid-rich adenoma can superficially re-semble a nontumoral adrenal cyst on imag-ing, because both can have a similar fluid at-tenuation. On contrast-enhanced CT, adrenal adenomas typically have strong enhancement during a standard CT acquisition (70–80 sec-onds after injection) [28]. Therefore, a mor-phologically benign adrenal cyst with an at-tenuation value less than 20 HU on such a study likely represents a cyst. Although a de-layed washout is characteristic for an adeno-ma, it typically occurs at 10 minutes after the injection, and even then, it rarely drops below 30 HU [29]. For lesions with attenuation of 20 HU or greater, confirmation of their cystic nature can be obtained with ultrasound or un-enhanced and contrast-enhanced CT or MRI. A degenerated adenoma may not have typical enhancement or attenuation and may appear as an indeterminate cyst on CT or MRI [30]. Peripheral calcification or visible walls are not typical for an uncomplicated adenoma. Thus, a low-attenuation cyst with an apparent wall
or wall calcification on CT favors a cystic cyst rather than adenoma.
A cystic pheochromocytoma is uncommon and can resemble an adrenal cyst on imaging. These tumors are usually large and outgrow their blood supply with secondary central de-generation and cystic change. They typically have a more complex appearance than a be-nign adrenal cyst, with a thick enhancing wall that contains viable tumor, and may or may not have septa. Many of these patients are symptomatic; however, because of the lesser tumor burden in these lesions, some patients may be normotensive and have negative bio-chemical assay findings [31].
Necrotic adrenal metastases are rarely con-fused with adrenal cysts. They can be unilat-eral or bilateral, small or large, and variable in appearance, but typically are heterogeneous be-cause of necrosis or hemorrhage [32]. A prima-ry adrenal cortical carcinoma is typically large, has central necrosis with a solid component, and often has calcification or venous extension into the left renal vein or inferior vena cava [32].
An additional rare mimicker of an adrenal cyst is a subdiaphragmatic bronchogenic cyst. These congenital foregut cysts descend below the diaphragm in embryologic life and may ob-scure a normal adrenal, thus mimicking a pri-mary adrenal cyst [33, 34]. Limited reports de-scribe these cysts on CT to be homogeneously hyperdense with calcification [33–36]. We en-countered such a case but excluded it from our review, because it did not represent an adrenal cyst. Ectopic thyroid tissue can rarely occur in the adrenal glands and cause a cystic mass [37].
Our data correlate with the published litera-ture on adrenal cysts. They are often sizeable, with a mean baseline size of 5.3 cm in our se-ries. We found that many adrenal cysts do not exhibit size stability over time. In our series, 60% of adrenal cysts increased in size, 25% decreased in size, and only 15% remained un-changed during the follow-up period. Thus, ad-renal cysts often increase in size while remain-
ing asymptomatic benign lesions, necessitating surgical removal [25]. However, on the basis of this series, we cannot determine the neces-sity for such workup in patients with benign-appearing adrenal cysts by imaging criteria. In addition, it is doubtful that such a cyst can tru-ly masquerade as a cystic pheochromocytoma or necrotic neoplasm, which are well described as having a more complex appearance. Labo-ratory tests, aimed at evaluating for hypercor-tisolism, aldosterone-producing adenoma, and pheochromocytoma, may not be necessary for benign-appearing adrenal cysts.
There are no universal current recommen-dations for the workup of adrenal cysts, to our knowledge. Much of the older published litera-ture on this topic showed a role for cyst aspi-ration. Clear aspirate was a criterion to avoid surgery because it was thought to confirm be-nignity, and bloody aspirate was considered in-determinate and was an indication for surgery [1, 38–40]. However, given the present-day ad-vances in cross-sectional imaging, we think that these practices are obsolete. Clinical symp-toms, cyst size greater than or equal to 6 cm, and complex imaging appearance are factors reported to determine the management of non-functional cysts. An additional role for surgery has been purported to remove the potential risk of hemorrhage or local pressure effects of the tumor [8]. Serial imaging has been suggested for asymptomatic nonfunctional cysts by sever-al authors [1, 8, 10, 38], but specific recommen-dations for appropriate follow-up intervals or selection of the optimal imaging modality have not been clearly established, to our knowledge.
On the basis of a series of 13 cases of cystic adrenal lesions, Rozenblit et al. [21] suggest-ed that uncomplicated cysts up to 5–6 cm in size with wall thickness of less than 3 mm can be observed, whereas more complicated cysts should be surgically explored. Our series con-firms the safety of follow-up of adrenal cysts with benign imaging characteristics, regard-less of their size.
A
Fig. 4—44-year-old man with incidental left adrenal cyst that decreased in size on 3.6-year follow-up CT scan (performed for flank pain). A, Initial axial CT scan with oral and IV contrast agent shows 8.9-cm hypodense cyst (16.5 HU) with rim calcification (arrowhead). B, Follow-up axial unenhanced CT scan shows contracted 6.1-cm hypodense cyst (15 HU) with persistent rim calcification (arrowhead).
B
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by N
atio
nwid
e C
hild
ren'
s H
ospi
tal o
n 10
/24/
13 f
rom
IP
addr
ess
164.
107.
116.
242.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

1016 AJR:201, November 2013
Ricci et al.Limitations of this study include its retro-spective nature and small sample size. All le-sions in our series had benign imaging char-acteristics without suspicious features. In addition, not all lesions were imaged with all cross-sectional imaging modalities. We had pathologic confirmation of benign adrenal cysts in only a minority of patients. Howev-er, the follow-up interval of the remaining le-sions helps confirm their benign nature.
In conclusion, adrenal cysts often change in size, with a considerable proportion growing over time. Knowing that increase in size over time is a common occurrence in asymptom-atic adrenal cysts would allow clinicians and radiologists to comfortably opt for conserva-tive management when imaging features are benign. Analogous to finding growth in renal cysts, finding growth in adrenal cysts does not indicate malignancy. We surmise that, in pa-tients who are at low risk for potential traumat-ic rupture and hemorrhage of an adrenal cyst (as opposed to children and young athletic per-sons, or patients requiring long-term anticoag-ulation), conservative management of adrenal cysts is reasonable. Our study does not allow us to determine the necessity or intervals for imaging surveillance of these lesions, and it is uncertain whether these lesions mandate long-term surveillance imaging at all. We think that ultrasound, which is the modality of choice for the assessment of various cystic lesions, can be effective for surveillance of adrenal cysts, if further investigation is deemed necessary.
AcknowledgmentWe thank Jannette Diaz-Rodriguez for her
invaluable assistance in reference acquisition.
References 1. Neri LM, Nance FC. Management of adrenal
cysts. Am Surg 1999; 65:151–163
2. Song JH, Chaudhry FS, Mayo-Smith WW. The
incidental adrenal mass on CT: prevalence of ad-
renal disease in 1,049 consecutive adrenal masses
in patients with no known malignancy. AJR 2008;
190:1163–1168
3. Bhargav PR, Mishra A, Agarwal G, Agarwal A,
Verma AK, Mishra SK. Adrenal incidentalomas:
experience in a developing country. World J Surg
2008; 32:1802–1808
4. Vilar L, Freitas Mda C, Canadas V, et al. Adrenal
incidentalomas: diagnostic evaluation and long-
term follow-up. Endocr Pract 2008; 14:269–278
5. El-Hefnawy AS, El Garba M, Osman Y, Eraky I,
El Mekresh M, Ibrahim el H. Surgical manage-
ment of adrenal cysts: single-institution experi-
ence. BJU Int 2009; 104:847–850
6. Abeshouse GA, Goldstein RB, Abeshouse BS.
Adrenal cysts: review of the literature and report
of three cases. J Urol 1959; 81:711–719
7. Erbil Y, Salmaslioglu A, Barbaros U, et al. Clini-
cal and radiological features of adrenal cysts. Urol
Int 2008; 80:31–36
8. Pradeep PV, Mishra AK, Aggarwal V, Bhargav
PR, Gupta SK, Agarwal A. Adrenal cysts: an in-
stitutional experience. World J Surg 2006;
30:1817–1820
9. Favorito LA, Lott FM, Cavalcante AG. Traumatic
rupture of adrenal pseudocyst leading to massive
hemorrhage in retroperitoneum. Int Braz J Urol
2004; 30:35–36
10. Tanuma Y, Kimura M, Sakai S. Adrenal cyst: a
review of the Japanese literature and report of a
case. Int J Urol 2001; 8:500–503
11. Robledo-Ogazón F, Vargas-Rivas AE, Alvarado-
Aparicio A. Adrenal gland lymphangiomas: a case
report [in Spanish]. Cir Cir 2004; 72:213–216
12. Basiri A, Salim NS, Shadpour P. Hypertension
secondary to an adrenal pseudocyst cured by lap-
aroscopic partial adrenalectomy. J Endourol
2002; 16:689–691
13. Escudero MD, Sabater L, Calvete J, Camps B, Labi-
os M, Lledo S. Arterial hypertension due to primary
adrenal hydatid cyst. Surgery 2002; 132:894–895
14. Ozarmagan S, Erbil Y, Barbaros U, Salmaslioglu
A, Bozbora A. Primary hydatid disease in the ad-
renal gland: a case report. Braz J Infect Dis 2006;
10:362–363
15. Horchani A, Nouira Y, Nouira K, Bedioui H, Me-
nif E, Safta ZB. Hydatid cyst of the adrenal gland:
a clinical study of six cases. ScientificWorld-
Journal 2006; 6:2420–2425
16. Foster DG. Adrenal cysts: review of literature and
report of case. Arch Surg 1966; 92:131–143
17. Guo YK, Yang ZG, Li Y, et al. Uncommon adre-
nal masses: CT and MRI features with histopath-
ologic correlation. Eur J Radiol 2007; 62:359–370
18. Jennings TA, Ng B, Boguniewicz A, Khan M,
Rice D, Figge J. Adrenal pseudocysts: evidence of
their posthemorrhagic nature. Endocr Pathol
1998; 9:353–361
19. Carvounis E, Marinis A, Arkadopoulos N, Theo-
dosopoulos T, Smyrniotis V. Vascular adrenal
cysts: a brief review of the literature. Arch Pathol
Lab Med 2006; 130:1722–1724
20. Bosniak MA. The current radiological approach
to renal cysts. Radiology 1986; 158:1–10
21. Rozenblit A, Morehouse HT, Amis ES Jr. Cystic
adrenal lesions: CT features. Radiology 1996;
201:541–548
22. Ho VB, Allen ST, Hood MN, Choyke PL. Renal
masses: quantitative assessment of enhancement
with dynamic MR imaging. Radiology 2002;
224:695–700
23. Erickson LA, Lloyd RV, Hartman R, Thompson
G. Cystic adrenal neoplasms. Cancer 2004;
101:1537–1544
24. Chien HP, Chang YS, Hsu PS, et al. Adrenal cys-
tic lesions: a clinicopathological analysis of 25
cases with proposed histogenesis and review of
the literature. Endocr Pathol 2008; 19:274–281
25. Anagnostis P, Karagiannis A, Tziomalos K, Ka-
kafika AI, Athyros VG, Mikhailidis DP. Adrenal
incidentaloma: a diagnostic challenge. Hormones
(Athens) 2009; 8:163–184
26. Young WF Jr. Clinical practice: the incidentally
discovered adrenal mass. N Engl J Med 2007;
356:601–610
27. Wedmid A, Palese M. Diagnosis and treatment of
the adrenal cyst. Curr Urol Rep 2010; 11:44–50
28. Korobkin M, Brodeur FJ, Francis IR, et al. De-
layed enhanced CT for differentiation of benign
from malignant adrenal masses. Radiology 1996;
200:737–742
29. Korobkin M, Brodeur FJ, Francis IR, et al. CT
time-attenuation washout curves of adrenal ade-
nomas and nonadenomas. AJR 1998; 170:747–752
30. Newhouse JH, Heffess CS, Wagner BJ, et al. Large
degenerated adrenal adenomas: radiologic-patho-
logic correlation. Radiology 1999; 210:385–391
31. Andreoni C, Krebs RK, Bruna PC, et al. Cystic
pheochromocytoma is a distinctive subgroup with
special clinical, imaging and histological features
that might mislead the diagnosis. BJU Int 2008;
101:345–350
32. Dunnick NR, Korobkin M. Imaging of adrenal
incidentalomas: current status. AJR 2002;
179:559–568
33. Chung JM, Jung MJ, Lee W, Choi S. Retroperito-
neal bronchogenic cyst presenting as adrenal tumor
in adult successfully treated with retroperitoneal
laparoscopic surgery. Urology 2009; 73:e13–e15
34. Onol FF, Baytekin F, Dikbas O, Ergonen T, Tani-
dir Y. A retroperitoneal bronchogenic cyst mim-
icking adrenal tumor in an adult: is differential
diagnosis truly possible? J Clin Pathol 2009;
62:187–189
35. Terry NE, Senkowski CK, Check W, Brower ST.
Retroperitoneal foregut duplication cyst present-
ing as an adrenal mass. Am Surg 2007; 73:89–92
36. Hedayati N, Cai DX, McHenry CR. Subdiaphrag-
matic bronchogenic cyst masquerading as an “ad-
renal incidentaloma.” J Gastrointest Surg 2003;
7:802–804
37. Shuno Y, Kobayashi T, Mortia K, et al. Ectopic
thyroid in the adrenal gland presenting as cystic
cyst. Surgery 2006; 139:580–582
38. Orihuela E, Herbert FB, Goodacre BW. Per-
cutaneous management of benign adrenal cysts: a
treatment option in selected cases. J Endourol
1998; 12:251–253
39. Tung GA, Pfister RC, Papanicolaou N, Yoder IC.
Adrenal cysts: imaging and percutaneous aspira-
tion. Radiology 1989; 173:107–110
40. Copeland PM. The incidentally discovered adre-
nal mass. Ann Intern Med 1983; 98:940–945
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by N
atio
nwid
e C
hild
ren'
s H
ospi
tal o
n 10
/24/
13 f
rom
IP
addr
ess
164.
107.
116.
242.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved