Embed Size (px)
DESCRIPTION
Adrenal Cortical Hormones. ENDO 412. Objectives of the Lecture. 1- Identifying the general structure of the adrenal cortex. 2- Characterizing the chemical nature of the adrenal cortical hormones 3- Identifying the hypothalamic-pituitary-adrenal ( HPA ) axis. - PowerPoint PPT Presentation
Citation preview

Adrenal Cortical Hormones
ENDO 412

Objectives of the Lecture
1- Identifying the general structure of the adrenal cortex.2- Characterizing the chemical nature of the adrenal cortical hormones3- Identifying the hypothalamic-pituitary-adrenal (HPA) axis. 4- Describing in brief the actions of glucocorticoids & mineralocorticoids.5- Identifying and describing the regulation of actions of glucocorticoids &
mineralocorticoids.6- Listing causes of adrenocortical hyperfunction (Cushing`s syndrome).8- Describing the biochemical & clinical concepts of adrenocortical
hyperfunction.9- Identifying and describing laboratory investigations for detection of suspected
adrenocortical hyperfunction10- Identifying the causes of adrenocortical hypofunction11- Describing the biochemical & clinical concepts of Addison`s disease.12- Identifying and describing investigations of suspected cases of Addison’s
disease.

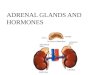
Structure of the adrenal cortex
• Outer: Zona Glomerulosa (produces mineralocorticoids: aldesterone)
• Middle: Zona Fasciculata (produces glucocorticoids : cortisol)
• Inner: Zona Reticularis (produces sex steroid hormones)

Synthesis of adrenal cortical hormones
Cholesterol is the precursor of all classes of steroid hormones

Mechanism of action of adrenal cortical (steroid) hormones
Cytosolic Receptors
Adrenal Cortical (Steroid) hormones belong to group I hormones
HRE of genes
Hormone Receptor Complex
Transcription of genes
is increased

Glucocorticoids (as Cortisol)
Action: on Metabolism
Carbohydrates: increase of gluconeogenesis (in liver).
Proteins: increase amino acids uptake by the liver for gluconeogenesis. So, increase proteolysis in skeletal muscles to give amino acids.
Lipids: increase ketogenesis in liver increase lipolysis in adipose tissue

Regulation
1- ACTH (adrenocorticotrophic hormone) of anterior pitutary:
by feedback control by corticitrophin releasing hormone (CRH): increased cortisol secretion (or synthetic glucocorticoids) suppresses secretion of CRH.
(HPA axis is the main regulation of cortisol secretion by adrenal cortex).
2- Stress induces sudden large increase in CRH that increases ACTH & cortisol.
3- Diurnal rhythm of plasma cortisol:
Levels of cortisol in blood is highest at the start of day & lowest at sleep.
Glucocorticoids (as Cortisol) cont.

Mineralocorticoids (as Aldesterone)
Action: Electrolyte balance (Na+ & K+) BY: Renin-Angiotensin System
Angiotensinogen (in liver, inactive)
Renin (synth. by kidney)
Angiotensin I
Angiotensin Converting Enzyme (ACE)
Angiotensin II
Aldesterone (from adrenal cortex)
In tubules of kidneyDecrease Na+ excretionIncrease K+ excretions
Hypernatremiahypokalemia
Increase BP

Regulation
1-Renin (of the kidney) increased in response to low blood volume or sodium loss.
2- Potassium (hyperkalemia) hyperkalemia (increase blood K+) stimulates release of aldesterone from adrenal cortex.
3- ACTH (ONLY IN STRESS)
Mineralocorticoids (as Aldesterone) cont.

Adrenal hyperfunction
• Hpercortisolism
Endogenous i.e. over secretion of CRH, ACTH or glucocorticoids (cortisol)Or: Exogenous intake of cortisol (or ACTH) (in all these cases, blood cortisol is elevated)
• Cushing`s Syndrome
describes a group of signs & symptoms resulting from excess glucocorticoids (cortisol) production or prolonged exogenous steroid use.

Causes of adrenal hyperfunction(Cushing`s syndrome)
1- ACTH dependent 1- ACTH secreting pituitary adenoma , 68% 2- Ectopic ACTH or ectopic CRH, 15% (usually malignant) 3- ACTH therapy (Iatrogenic Cushing`s Syndrome)
2- ACTH independent 1- Adrenal adenoma, 17% (ACTH is suppressed) 2- Glucocorticoids therapy

Biochemical & clinical concepts of Cushing`s syndrome
Clinical Effects Biochemical ChangesHyperglycemia (may be DM) Increased gluconeogenesis
Truncal obesity (Buffalo hump) Disturbed fat metabolism with redistribution
Thinning of skinWasting of musclesOsteoporosis of bones
Severe catabolic effects on proteins
Poor wound healingReduced resistance to infection (low immunity)
Suppressed immune response
Hpernatremia (increased Na+ in blood)Hypokalemia (decreased K+ in blood)AlkalosisHypertension
Mineralocorticoid effects of cortisol

Laboratory investigations of adrenal hyperfunction (Cushing`s syndrome)
Stage I: Diagnosis of Cushing`s syndromeSuspected cases by clinical examination are checked in Clinical Chemistry Laboratoryfor Cushing`s syndrome.
1 -Screening tests 1 -Cortisol excess
2 -Loss of diurnal rhythm determination 3 -Suppression resistance determination
2 -If screening tests are positive, diagnosis is confirmed by confirmatory tests Insulin hyperglycemic test
Stage II: If Cushing`s syndrome is confirmed, tests for determining the cause of Cushing`s syndrome (ACTH dependent or ACTH independent):
1 -Plasma ACTH 2 -CRH stimulation test (CRH-stimulated BIPSS & peripheral veins sampling)

Clinical manifestations (symptoms & signs)
Screening test
Positive Result
Confirmatory tests
Positive result
Plasma ACTH
Positive Negative
ACTH dependent ACTH independent
Laboratory investigations of adrenal hyperfunction (Cushing`s syndrome)

Screening test-1Cortisol excess
By: Urine free cortisol (and/or metaboites) Measurement
Free cortisol (& metabolites) is excreted in urine if blood cortisol exceeds capacity of its carrier protein.
Urine free cortisol (or metabolites) is a sensitive indicator of endogenous cortisolism.Advantage of urine free cortisol: It reflects free cortisol level during the period of urine collection.
17-hydroxycorticosteroid (metabolite of cortisol), is preferred as it is not affected by urine volume. (Other metabolites are secreted in higher amounts with increase urine volume).
Urine collection period: 24 hours (or only 10 hours from 10 PM till 8 AM)
NB: Random plasma cortisol measurement is of little value in diagnosis of Cushing`s syndrome as levels of normal people vary widely during the day & may overlap with levels found in patients of Cushing`s syndrome.
Laboratory investigations of adrenal hyperfunction (Cushing`s syndrome)

Screening tests-2By: Loss of diurnal rhythm determination
Principle of the test:Normally, blood cortisol is at its highest levels between 6 - 8 AM & at its lowest levels between 10 PM – 12 AM (midnight).
This variation is lost in Cushing`s syndrome (i.e. increased all over the day)Loss can be determined by measuring plasma cortisol 11 PM – 12 AM (midnight).
This test is more sensitive than urine cortisol in diagnosing Cushing` syndrome.
Or by: Saliva cortisol (instead of plasma cortisol)
- Cortisol is stable at room temperature in saliva (easy storing of samples)- Non-invasive (no sampling by puncture etc…)- Patient can collect the samples by himself - Many samples can be collected over a defined period.BUT: less sensitive than urine cortisol
Laboratory investigations of adrenal hyperfunction (Cushing`s syndrome)

Screening tests-3Loss of normal cortisol suppression by dexamethazone
By: Overnight dexamethazone suppression test
Principle of the testDexamethasone act as an exogenous cortisol substitute that suppresses endogenous cortisol secretion if adrenal cortex is normal (through suppressing ACTH if ant. pit. is normal)
ProcedureDexamethazone 1 mg is given at 11 PM (should suppress early morning cortisol high secretion).Then, 8-9 AM: serum free cortisol is measured.
Results:In normal individuals : cortisol is less than 3.6 mg/dl (cortisol is normally suppressed by dexameth.)
In Cushing`s syndrome: cortisol level in blood is higher than 3.6 mg/dl. (cortisol secretion is not suppressed by dexamethazone in these cases).
NB: Dexamethazone levels in blood is measured (for checking compliance of the patient).
Laboratory investigations of adrenal hyperfunction (Cushing`s syndrome)

Interpretation of Screening Tests
Positive results for screening test 1, 2 & 3
Cushing`s syndrome or Pseudo-Cushing`s syndrome
Depression Extremely anxious patients
Severe illness Alcoholism
So, confirmatory tests should be performed to rule out pseudo-Cushing`s syndrome
Laboratory investigations of adrenal hyperfunction (Cushing`s syndrome)

Confirmatory TestInsulin hypoglycemic test
Principle:Hypoglycemia induces CRH that induces ACTH that induces cortisol secretion. i.e. normal HPA axis)
In Cushing`s syndrome (for any cause), no response to hypoglycemia & accordingly no effect on CRH, ACTH or cortisol.
Procedure (IN HOSPITAL UNDER RECAUSIONS)Insulin IV (0.15 U/kg) will reduce blood glucose to 2.2 mmol/l or lessNormally, serum cortisol reaches its maximum 60-90 minutes after injectionBlood samples for cortisol is withdrawn before injection & then 60 and 90 minutes after injection (together with blood glucose measurement)
Results:Increase in blood cortisol in after-injection samples: Negative for Cushing`s syndrome.No difference between before & after samples: Positive for Cushing`s
( defect in HPA axis ----verify)??
Laboratory investigations of adrenal hyperfunction (Cushing`s syndrome)

Determining the Cause of Cushing`s SyndromeOnce Cushing`s syndrome is confirmed, cause is to be decided
(i.e. ACTH dependent or ACTH independent)
By:
Plasma ACTH (At 8 AM & 10 PM)
Undetectable Normal or Increased
ACTH independent ACTH dependent Adrenal Cause Pituitary cause Ectopic ACTH (e.g. Adrenal tumor)
to differentiate :
CRH stimulated BIPSS & peripheral vein sampling BIPSS ACTH / peripheral ACTH > 3 in pituitary causes BIPSS ACTH / peripheral ACTH < 2.5 in ectopic causes (BIPSS = bilateral inferior petrosal sampling)
Laboratory investigations of adrenal hyperfunction (Cushing`s syndrome)

Adrenal insufficiency (Addison`s disease)
Low cortisol result from:
1- Primary adrenal problem (destruction of 90% of adrenal cortex) mainly caused by autoimmune destruction of adrenal cortex (more than 70% of cases of adrenal insufficiency)
2- Secondary to ACTH deficiency (abnormal of HPA axis)
Main clinical manifestation:
1- Weakness, fatigue, anorexia, weight loss (failure to thrive)2- Hyponatremia, hyperkalemia & mild metabolic acidosis

Diagnosis Low Base-line Cortisol (at 8 AM)
Cosyntropin Test (Cortisol Stimulation Test)
Normal response to stimulation No response to stimulation
Secondary adrenal insufficiency ?? Primary adrenal insufficiency ??
LOW ACTH HIGH ACTH SECONDARY ADRENAL INSUFFICIENCY PRIMARY ADRENAL INSUFFICIENCY
Adrenal insufficiency (Addison`s disease)

Cosyntropin test:
Principle:
Cosyntropin is a synthetic stimulator of cortisol secretion by adrenal cortex. Cosyntrpoin test checks the capacity of adrenal gland to increase of hormone production in response to stimulation by cosyntropin
Procedure:
1- Base-line cortisol is measured 2- Then, cosyntropin is IV or IM administered3- Cortisol is measured 30 & 60 minutes after cosyntropin administration.
Results:
Normally, cortisol secretion is increased after stimulation of the adrenal gland by cosyntropin.
In primary adrenal insufficiency, cosyntropin fails to increase cortisol secretion by the adrenal cortex.
Adrenal insufficiency (Addison`s disease)