Embed Size (px)
Citation preview
Adrenal Adrenal CarcinomaCarcinoma
Dr. D.W. DaughertyDr. D.W. Daugherty
EpidemiologyEpidemiology
Estimated incidence of 0.5-2 per 10Estimated incidence of 0.5-2 per 1066 patients per yearpatients per year
Peaks of age distribution at age <5 Peaks of age distribution at age <5 and in the 4and in the 4thth and 5 and 5thth decades decades
Scattered reports of gene Scattered reports of gene associations, but rarity of lesion associations, but rarity of lesion limits studies – no clear associationslimits studies – no clear associations
Functioning LesionsFunctioning Lesions
60-65% of adrenocortical 60-65% of adrenocortical carcinomas are functioning lesionscarcinomas are functioning lesions CushingsCushings VirilizationVirilization FeminizationFeminization HyperaldosteronismHyperaldosteronism
DiagnosticsDiagnostics
Hormonal studies can be a first Hormonal studies can be a first diagnostic test which confirms diagnostic test which confirms ectopic steroid hormone secretion, ectopic steroid hormone secretion, leading to an imaging and tissue leading to an imaging and tissue diagnosis.diagnosis.
They also can be a “tumor marker” They also can be a “tumor marker” which can be useful for monitoring which can be useful for monitoring response to therapy and suspicion of response to therapy and suspicion of recurrence.recurrence.
HypercortisolismHypercortisolism
24 hour urinary cortisol exrection24 hour urinary cortisol exrection More than 90% of Cushinoid patients More than 90% of Cushinoid patients
have free cortisol levels greater than have free cortisol levels greater than 200mcg/ 24 hours. 97% of normals 200mcg/ 24 hours. 97% of normals have levels less than 100mcg/ 24 hourshave levels less than 100mcg/ 24 hours
ACTH measured with serum cortisol will ACTH measured with serum cortisol will demonstrate ACTH independent nature demonstrate ACTH independent nature of hypercortisolism. of hypercortisolism.
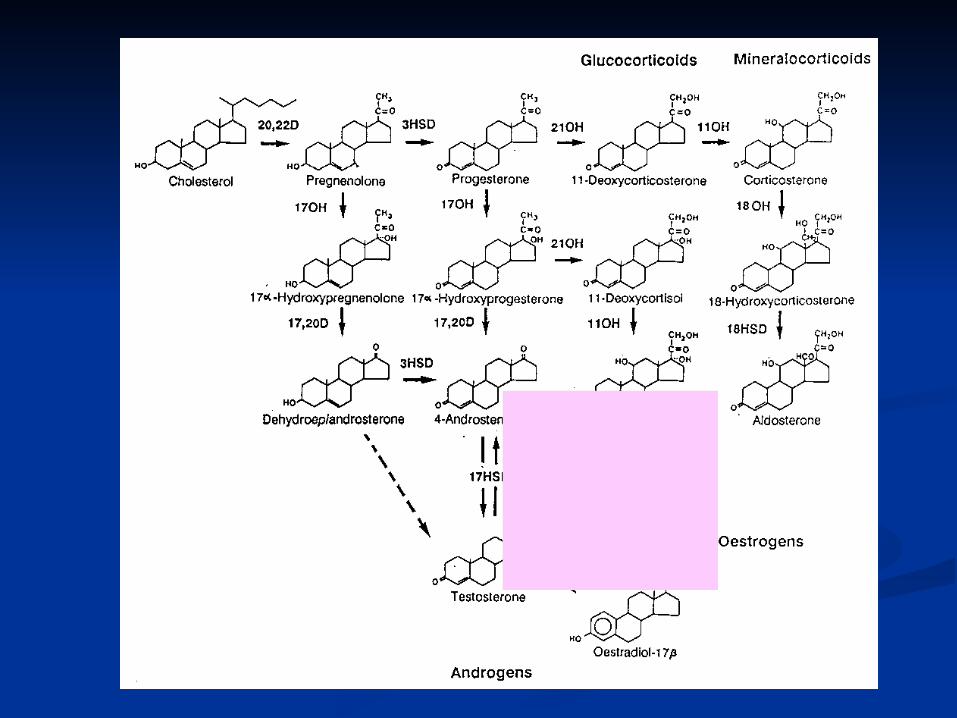
Other SteroidsOther Steroids Other steroids are elevated:Other steroids are elevated:
androstenediol and adrosetenedioneandrostenediol and adrosetenedione DHEA and DHEA-SDHEA and DHEA-S 11- deoxycortisol11- deoxycortisol urinary 17- ketosteroidsurinary 17- ketosteroids aldosteronealdosterone
Many intermediate enzymes are Many intermediate enzymes are defective or dysregulated, leading defective or dysregulated, leading to inefficient steroid production to inefficient steroid production and precursor accumulationand precursor accumulation
Potential Functional Potential Functional AssaysAssays
Serum TestosteroneSerum Testosterone Serum DHEA and DHEA-SSerum DHEA and DHEA-S 24 hour urinary ketosteroids24 hour urinary ketosteroids Plasma estradiol and/ or estronePlasma estradiol and/ or estrone Plasma aldosterone/ reninPlasma aldosterone/ renin Urinary catecholamines/ Urinary catecholamines/
metanephrines in all patientsmetanephrines in all patients
ImagingImaging
CT detects 98% of adrenal CT detects 98% of adrenal carcinomascarcinomas
MRI scanning can also provide MRI scanning can also provide vascular invasion/ tumor thrombosis vascular invasion/ tumor thrombosis information.information.
Many incidental findings?Many incidental findings? Malignant lesions tend to be > 5cm, Malignant lesions tend to be > 5cm,
have irregular shapes/ blurred margins, have irregular shapes/ blurred margins, and be heterogeneously enhancing.and be heterogeneously enhancing.
StagingStaging
Hormonal studies directed at Hormonal studies directed at symptomssymptoms
24h urine studies to r/o 24h urine studies to r/o pheochromocytomapheochromocytoma
CT scanning to determine extent and CT scanning to determine extent and resectability of lesionresectability of lesion
MRI may clarify vascular invasion; MRI may clarify vascular invasion; right sided lesions have a propensity right sided lesions have a propensity to form venous tumor embolito form venous tumor emboli
StagingStaging Stage I — Disease confined to the adrenal Stage I — Disease confined to the adrenal
gland and <5 cm in diameter (approx 20%) gland and <5 cm in diameter (approx 20%) Stage II — Disease confined to the adrenal Stage II — Disease confined to the adrenal
gland and >5 cm in diameter (approx 20%) gland and >5 cm in diameter (approx 20%) Stage III — Local invasion that does not Stage III — Local invasion that does not
involve adjacent organs or regional lymph involve adjacent organs or regional lymph nodes (approx 20%) nodes (approx 20%)
Stage IV — Distant metastases or invasion Stage IV — Distant metastases or invasion into adjacent organs plus regional lymph into adjacent organs plus regional lymph nodes (approx 40%)nodes (approx 40%)

SurgerySurgery
Complete surgical resection is the primary treatment modality
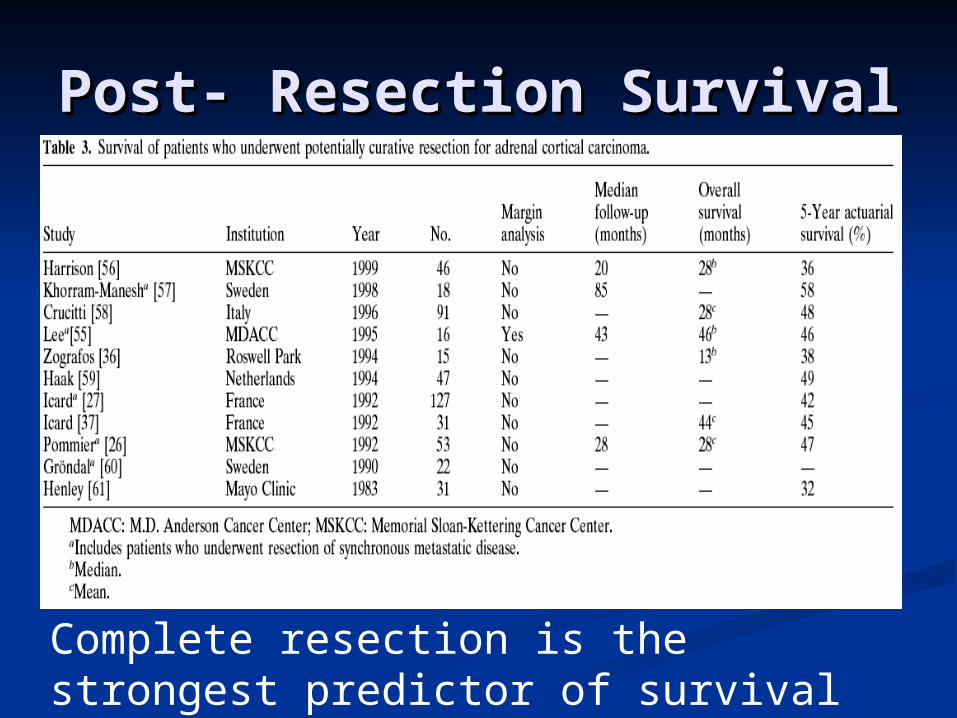
Post- Resection SurvivalPost- Resection Survival
Complete resection is the strongest predictor of survival
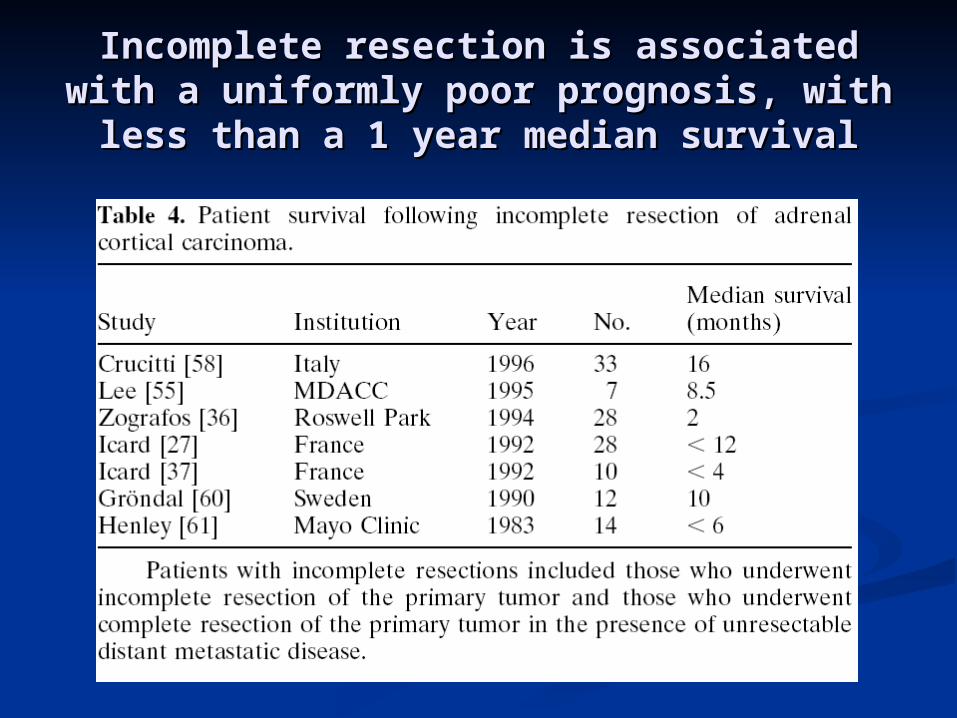
Incomplete resection is associated with Incomplete resection is associated with a uniformly poor prognosis, with less a uniformly poor prognosis, with less
than a 1 year median survivalthan a 1 year median survival
ResectabilityResectability
Unresectable tumors include those Unresectable tumors include those that invade the celiac plexus/ that invade the celiac plexus/ vascular structures/ SMA/ aortavascular structures/ SMA/ aorta
Prognostic factorsPrognostic factors In a case review of 46 patients at MSKCC, In a case review of 46 patients at MSKCC,
3 histologic factors correlated with 3 histologic factors correlated with survival:survival: Tumor > 12cmTumor > 12cm 6 or more mitotic figures/ 10hpf6 or more mitotic figures/ 10hpf presence of histologic evidence of intra-presence of histologic evidence of intra-
tumoral hemorrhagetumoral hemorrhage 5 year survivals:5 year survivals:
0 factors: 83%0 factors: 83% 1 factor: 42%1 factor: 42% 2 factors: 33%2 factors: 33%
TreatmentTreatment
AdrenalectomyAdrenalectomy Prednisone for steroid replacementPrednisone for steroid replacement Patients with glucocorticoid Patients with glucocorticoid
producing tumors postoperatively producing tumors postoperatively will need replacement due to will need replacement due to suppression of the remaining suppression of the remaining adrenaladrenal
Radiation ApproachRadiation Approach
There are emerging case reports There are emerging case reports demonstrating improved outcomes demonstrating improved outcomes when palliative XRT used for when palliative XRT used for localized lesionslocalized lesions
Chemotherapeutic Chemotherapeutic ApproachApproach
Emerging case reports, Emerging case reports, retrospective treatment data, and retrospective treatment data, and reviews are beginning to support reviews are beginning to support this approach.this approach.
MitotaneMitotane
1,1- dichloro-2-(o-chlorophenyl) 1,1- dichloro-2-(o-chlorophenyl) ethane (o,p-DDD).ethane (o,p-DDD).
Chemical relative to DDTChemical relative to DDT Found to have adrenolytic activity in Found to have adrenolytic activity in
dogs in vivo (selectively destroyed dogs in vivo (selectively destroyed the zonae reticularis and fasciculata)the zonae reticularis and fasciculata)
MitotaneMitotane
inhibits the mitochondrialinhibits the mitochondrial conversion conversion of cholesterol to pregnenolone and of cholesterol to pregnenolone and the conversionthe conversion of 11-deoxycortisol to of 11-deoxycortisol to cortisol (11B- hydroxylation). It cortisol (11B- hydroxylation). It produces selective adrenocorticalproduces selective adrenocortical
necrosis in both the adrenal tumor necrosis in both the adrenal tumor and metastases and metastases
MitotaneMitotane
Side effects are major and Side effects are major and frequent, including:frequent, including: CNS disturbance (vertigo, CNS disturbance (vertigo,
somnolence, ataxia)somnolence, ataxia) Liver ToxicityLiver Toxicity Renal ToxicityRenal Toxicity Nausea, VomitingNausea, Vomiting DiarrheaDiarrhea RashRash
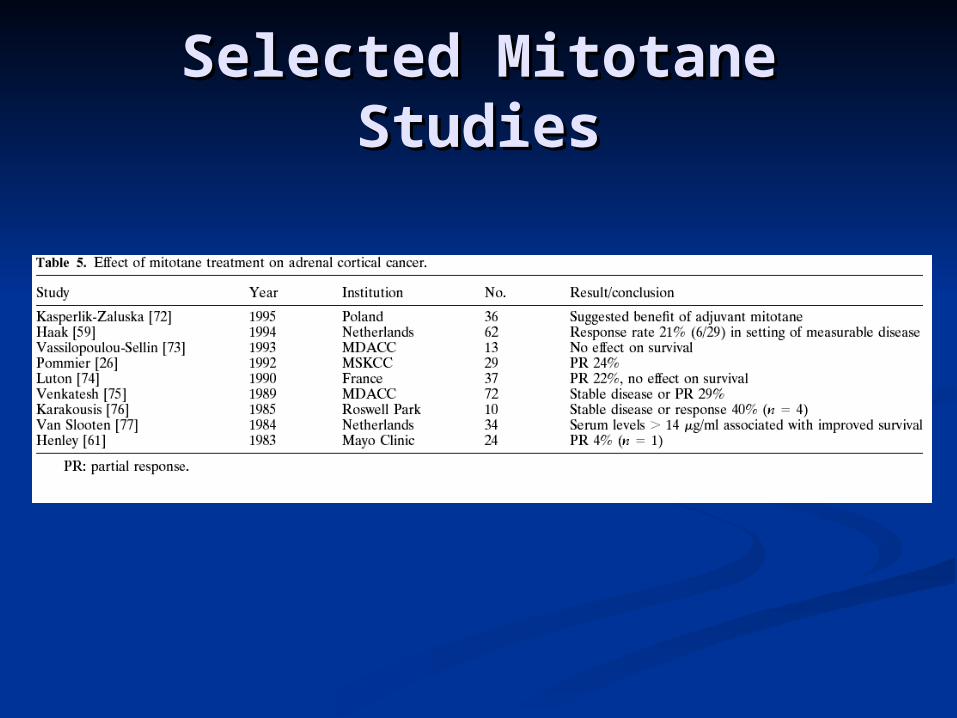
Selected Mitotane Selected Mitotane StudiesStudies
Other symptom- Other symptom- palliative Optionspalliative Options
Metyrapone (11B hydroxylase Metyrapone (11B hydroxylase inhibitor)inhibitor)
KetoconazoleKetoconazole AminoglutehamideAminoglutehamide
CytotoxicsCytotoxics
Various systemic cytotoxics have Various systemic cytotoxics have been used for advanced disease, been used for advanced disease, usually for those failing mitotane.usually for those failing mitotane.
Most studied have been Etoposide, Most studied have been Etoposide, cisplatin, and adriamycin. cisplatin, and adriamycin.
Paclitaxel and Temozolamide have Paclitaxel and Temozolamide have recently demonstrated antitumor recently demonstrated antitumor activity activity in vitroin vitro
CombosCombos
Original studies utilized Cisplatin Original studies utilized Cisplatin and Doxorubicin with and Doxorubicin with Cyclophosphamide or 5-FU. RR was Cyclophosphamide or 5-FU. RR was 20%20%
Cisplatin/ Etoposide reported to Cisplatin/ Etoposide reported to have an 11% response ratehave an 11% response rate
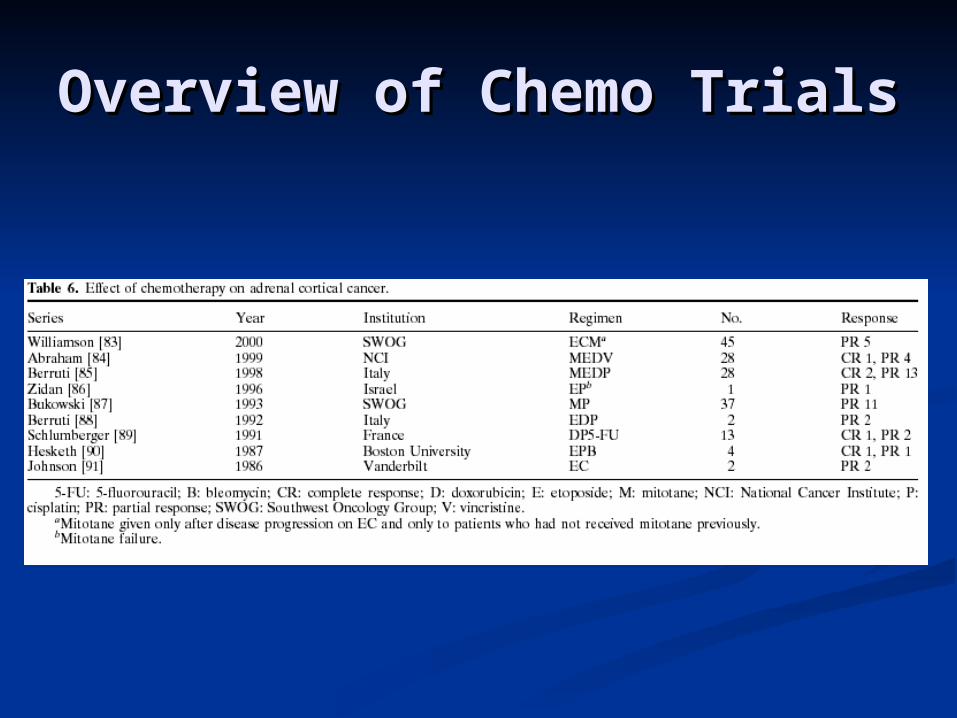
Overview of Chemo TrialsOverview of Chemo Trials

MDR issuesMDR issues
P-Glycoprotein (Pgp) is expressed P-Glycoprotein (Pgp) is expressed widely in normal adrenal and widely in normal adrenal and adrenocortical carcinoma cellsadrenocortical carcinoma cells
In vitroIn vitro, mitotane inhibits the Pgp , mitotane inhibits the Pgp efflux pump at concentrations efflux pump at concentrations achieved with mitotane therapyachieved with mitotane therapy
EDP-MEDP-M
Italian studyItalian study 28 patients enrolled28 patients enrolled Etoposide (100mg/ mEtoposide (100mg/ m22) d5-7; ) d5-7;
Doxorubicin (20mg/ mDoxorubicin (20mg/ m22) d1,8; ) d1,8; Cisplatin (40mg/ mCisplatin (40mg/ m22) d1,9 every 4 ) d1,9 every 4 weeksweeks
Concomitant mitotane up to 4g/ dayConcomitant mitotane up to 4g/ day
EDP-MEDP-M
CR in 2 patientsCR in 2 patients PR in 13 patientsPR in 13 patients Overall response of 54%Overall response of 54% Stable disease in 8, progessive in 5Stable disease in 8, progessive in 5 Median TTP of 24 months in Median TTP of 24 months in
respondersresponders
RecurrencesRecurrences
Recurrences that are amenable to Recurrences that are amenable to re- operation may be resected for re- operation may be resected for long term survivallong term survival
5 year survivals compare from 57% 5 year survivals compare from 57% in those amenable to resection to 0% in those amenable to resection to 0% for those who are notfor those who are not

RecurrencesRecurrences
Italian registry: 140 resectionsItalian registry: 140 resections Recurrences in 52 (37%)Recurrences in 52 (37%)
Locally in 13Locally in 13 Distant in 25Distant in 25 Local + Distant in 14Local + Distant in 14
20 patients underwent re- resection20 patients underwent re- resection 5 yr survival of 50% in those resected5 yr survival of 50% in those resected 5 yr survival of 8% in those not resected5 yr survival of 8% in those not resected
RecurrencesRecurrences
MSKCC: 47 patients with recurrent/ MSKCC: 47 patients with recurrent/ metastatic diseasemetastatic disease
Patients who had a complete second Patients who had a complete second resection had a median survival of 74 resection had a median survival of 74 months (5-year survival, 57%), whereas months (5-year survival, 57%), whereas those with incomplete second resection those with incomplete second resection had a median survival of 16 months (5-had a median survival of 16 months (5-year survival, 0%). year survival, 0%).
SummarySummary
Adrenocortical carcinoma is a rare Adrenocortical carcinoma is a rare disease that often presents latedisease that often presents late
Primary curative therapy is surgicalPrimary curative therapy is surgical No role for adjuvant chemotherapy No role for adjuvant chemotherapy
has been definitively demonstrated has been definitively demonstrated to dateto date
Palliative therapy with mitotane may Palliative therapy with mitotane may be useful; its palliative effect may be be useful; its palliative effect may be entirely due to adrenolytic effectentirely due to adrenolytic effect
SummarySummary
Re-operation appears to be the only Re-operation appears to be the only long term curative option in long term curative option in recurrent casesrecurrent cases
Cytotoxic chemotherapy in the Cytotoxic chemotherapy in the advanced/ metastatic setting has not advanced/ metastatic setting has not been definitively demonstrated to be been definitively demonstrated to be useful in controlled trialsuseful in controlled trials
EDP-M may be useful in metastatic EDP-M may be useful in metastatic settings; evaluation is ongoingsettings; evaluation is ongoing
Thank YouThank You