Embed Size (px)
Citation preview

Administration
Heather Patterson
PGY-2
March 15, 2007
Preceptor: Dr. Gavin Greenfield

Objectives
1. Role of the Administrator-Heirarchy in the CHR ED
2. Public Relations 3. Patient complaints and satisfaction4. Physician-physician complaints5. Staff- physician complaints6. Observation Units7. Determining schedules

Name that future administrator…
• Likes to wear pink shirts and/or tight shirts
• Will still respond to “chief”
• Likes to make sure we all feel part of the team….

Emergency Department Director
Qualifications
• Board certified emergency physician• Proven clinical and administrative skills• CME participation• Demonstrated knowledge and ability in
financial, managerial, and marketing aspects of EM
• Demonstrated ability to speak effectively on administrative and clinical matters related to EM

Emergency Department Director
Purpose of the Position (ACEP)
• Leadership & management in the ED• Work cooperatively with ED staff to provide
emergency services for patients. • Work cooperatively with diagnostic and
therapeutic services to ensure availability, quality, and effective use of services
• Provide input into preparation of departmental budget
• Monitor community needs and provide input into EMS and disaster planning

Emergency Department DirectorResponsibilities
• ED activities: leadership, organization, staffing, coordination, scheduling, and evaluation
• Ethical practice of EM within dept• Supervision of clinical and
administrative duties for EP’s • Hospital executive committee:
represent interests of EM– Liaison between hospital administration
and ED staff

Emergency Department DirectorSummary
• Department management
• Recruitment and orientation
• Education• Public relations • Liaison• Department meetings• Committees – hospital
and departmental
• Quality assurance• Peer review
– Physician evaluation
• Planning• Legal
– Risk management• Contracts and
finances

The Bottom Line:
The role of the administrator is to make the emergency
department a better place for patients and staff

Name that future administrator…..
• Likes to wear women’s clothes for special occasions
• Adults tend to be afraid of him so he works with kids now
• Owns a car but doesn’t use it often– runs, bikes, or swims instead….

Heirarchy ….
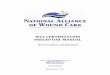
Executive Medical DirectorDr. Cam Waddell
Vice PresidentThelma Inkson
Regional Clinical Department HeadDr. Gil Curry
Director, Emergency, Urgent Care and Health Link
Caroline Hatcher
Acting DeputyRCDH
Dr. Lester Mercuur
Undergraduate CoordinatorL. Campfens
Division Chief, Education
FRCP: C. Hall
QI PhysicianT. Rich
Site ChiefsFMC: W. SefcikPLC: P. Davids
RGH: C. Godfrey
Patient Care ManagersFMC: B. KatholPLC: D. KellyRGH: T. Smith
Service Planning Coordinator
Maureen McNaul
Research CoordinatorR. Iwanow
Data SpecialistD. Wang
Regional Clinical Nurse Specialist
Vacant
REDIS CoordinatorsK. JessenS. LuznyH. BattleD. Hone
AssistantPatient Care Managers
FMC: T. DavidsonPLC: D. DooleyRGH: L. Walters
Division Chief, ResearchM. Yarema
Associate ResearchDirectorVacant
Resident Research Coordinator
C. Hall
Patient Care ManagerACH: K. Howe
Regional Department of Emergency Medicine / Emergency Services Organizational ChartJuly 2005
Director, Calgary Regional Sexual Assault Response Team
P. Head
Division Chief, Education
CCFP(EM): N. Collins
Assistant Division Chief, Education
CCFP(EM): I. Walker
Assistant Resident Research Coordinator’s
N. Collins & I. Walker

Bad publicity
• Recent cases:– July 2006
• “repeatedly asked for help for 3 hours, but were told they had to wait for a bed”. Miscarriage in waiting room.
– September 2006• “began miscarrying in the packed waiting room
and was denied a place to go despite asking for help. She had waited for 6 hours”.
– September 2006• “miscarried in waiting room after waiting more
than 6 hours”

Public Relations
• Gavin….

Patient Complaints:
• Why do we have a complaint system?• Identify systemic problems and create solutions (QI)• Identify personal deficiencies ie information delivery,
communication skills, bedside manner• Promote positive interactions with patients, public, and
staff• Reduce litigious dispute resolution • Create risk management strategies

Patient Complaints:
• Waiting time related– Waiting room time– Wait time for physician once in bed– Overall health care system and wait times
• Patient expectations– Meds not given ie: Narcotics refused for chronic pain
patient– Did not get tests they want ie: MRI, CT, Xray– Did not get admitted
• Personal interactions– MD, nurse, radiology

Patient Complaints:

Patient Complaints:
• Patients are encouraged to speak directly to those involved OR if uncomfortable, to speak with a supervisor, patient care manager or clinic manager
• Patient Care Representative Service:– “Point of entry into the regional health system for
patients or their advocates to express concerns, complaints or commendations regarding patient care”
– Can access this resource in person, by phone, fax, or email

Patient Complaints:
• Complaints are sent to the relevant department
• Non-MD related patient care managers• MD related site chiefs
• Chart reviewed• MD contacted for clarification and written comments• Patient is contacted in writing or by phone UNLESS
lawyer is involved. Then CMPA takes over.

Program/UnitAccess to Service
Clinical Support
Diagnostic Imaging
Financial
Medical Care (Physician)
Nursing Care
Other
Support Services
Grand Total
Emergency Services 13 1 1 4 19 36 2 3 79
PADIS 1 1
Urgent Care (8th & 8th Health Centre) 1 2 2 5
Grand Total 14 1 1 4 21 39 2 3 85
Program/UnitAccess to Service
Care Del. (Multi Disciplinary)
Clinical Support
Financial
Medical Care (Physician)
Nursing Care
Other
Support Services
Grand Total
Emergency Services 7 10 1 6 34 42 2 1 103
Security (8th & 8th Health Centre) 1 1
South Calgary Health Centre 2 1 2 2 7
Urgent Care (8th & 8th Health Centre) 2 1 2 5
Grand Total 11 10 1 7 37 46 2 2 116

Program/UnitAccess to Service
Care Del. (Multi Disciplinary)
Financial
Medical Care (Physician)
Nursing Care
Other
System
Grand Total
Emergency Services 71 23 7 37 37 4 1 180
Mental Health (8th & 8th Health Centre) 1 1
South Calgary Health Centre 1 2 5 2 10
Urgent Care (8th & 8th Health Centre) 1 1 2 2 6
Grand Total 72 24 8 42 44 6 1 197

Physician Complaints:
What do you do if you have a conflict with another physician?

Patient Satisfaction
• What factors influence patient satisfaction in emerg?

Patient Satisfaction
• Interpersonal skills:– Nursing and
physician– “expressive
quality”• Friendliness,
courtesy, respectfulness, compassion
• Mannerisms and perceived humanitarian concern

Patient Satisfaction
• Interpersonal skills:– Information delivery
• Amount, quality and understandability of information given
• Communication skills

Patient Satisfaction
• Wait times:– Perceived vs actual
• Actual wait time does not impact satisfaction rankings
• If patient feels that they have waited too long for their particular complaint, dissatisfaction is likely to arise!
– Studies show that neither patients nor providers are good at estimating times• Patients and physicians tend to overestimate

Patient Satisfaction
• Statistically not significant:• MD factors:
– Gender– Marital status– Technical skills
• ED factors:– Time/day– Busy dept/volume
• Patient factors – Acuity (1995) – debatable, nonreproducible results – Pain, chronic illness, medical vs surgical, insurance,
diagnosis– Tests done– Number of prior visits

Patient Satisfaction – how can we improve?
• Interpersonal interactions:– Things you learned in medical school
• Verbal and nonverbal communication is very important
• Be empathetic
– Information delivery• Explain everything that you do in an accessible
manner appropriate for the patient. • Use professional interpreters

Patient Satisfaction – how can we improve?
• Interventions:– Customer training. Improved pt impression
of nurse and MD skills and overall satisfaction (Mayer et al 1998)
– MD business cards given to pts. Improvement (schiermeyer et al 1994)
– Observation units in asthma and cardiac patients. Improvement. (Mowen et al 1993, Ryeman et al 1997, 1999)
– TV in rooms, standardized verbal estimates of wait time, and feedback forms available made no difference.
– Video in waiting room about ED. No impact (Krishal et al 1993, Corbet et al 2000 – poorly designed)

Observation Units
• The good, the bad, the ugly…..– What?– Why?– Who?– How?

Observation Units –What?
• Observation Units:– Area where patients can be observed or
have early investigation/management in ED
• Assessment Unit:– ED patients are assessed and initial
management is undertaken by inpatient hospital teams
• Admission Ward:– Admitted patient holding area

Observation Units – Older Stats
• US (1989)– 27% have obs units– 16% are in process of getting units
• UK (1998)– 57% have obs units
• AUS (1989)– 50%

Observation Units – Why?
• Patient Satisfaction:– Several non randomized trials say
increased pt satisfaction– 1999 Rydman et al (AEM) found increased
patient satisfaction with use of obs unit• Randomized 163 asthma pts to obs unit or usual
inpatient care• Patients reported fewer problems with care
received, communication, emotional support, physical comfort
• Fewer investigations in obs unit

Observation Units – Why?
• Emerg Impact:– Studies have suggested (1990s):
• Reduce ED workload• Improvement in ED flow• Faster referral to specialists
• LOS (1997)
– Decreased overall length of stay– Potential financial benefit for region
• If used appropriately for predetermined disease entities

Observation Units – Why not?
• Hospital impact– Study in the UK (1997) suggested if the ED
and hospital is functioning well and good clinical skills, no significant improvement is seen.
• Emerg Impact:– Staffing – “Dumping area”/ improper use
• Social vs medical pts
– Time limits exceeded– Inadequate/inefficient transfers to inpatient
units

Observation Units - Who?
• High risk discharge• Short term treatment• Short term observation

Observation Units - Who?
• Diagnostic evaluation• Abdominal pain • Chest pain (low probability of myocardial
infarction) • Flank pain (rule out renal colic) • Gastrointestinal bleeding with initial evaluation • Chest trauma (normal initial evaluation and chest
radiograph) • Abdominal trauma (normal initial evaluation and
lavage) • Drug overdose (clinically stable) • Syncope (negative initial evaluation) • Vaginal bleeding, threatened abortion
Management of observation units. Ann Emerg Med June 1995;25:823-830

Observation Units - Who?
• Short-term therapy • Allergic reactions • Asthma • Acute exacerbation of chronic congestive heart
failure • Dehydration • Hyperglycemia (mild to moderate)• Hypertensive urgencies • Selected infections (eg, pyelonephritis) • Seizure disorder requiring anticonvulsant
loading • Sickle cell pain crisis • Blood transfusion
Management of observation units. Ann Emerg Med June 1995;25:823-830

Observation Units - Who?
• Psychosocial needs • Alcohol intoxication • Adjustment reaction • Depression • Psychosis • Social disposition problems • Wrist laceration – psych related
Management of observation units. Ann Emerg Med June 1995;25:823-830

Observation Units – Admission Crit.
• Clearly identified patient care goals – Evaluation of high-risk chief complaints – Short-term therapy of an emergency condition – Meeting psychosocial needs
• Limited need for intense medical services
• Limited severity of illness; anticipation of discharge home within time limits
• Clinical condition appropriate for observation
Management of observation units. Ann Emerg Med June 1995;25:823-830

Observation Units - Who?
• How do we do?– 2 MDs retrospectively reviewed 1606 charts
of ED patients in the ED >4hrs – Asked to determine if they were
appropriate for Obs Unit, admission, or discharge.
– Compared to actual outcomes– We didn’t do a great job.
• 363 selected for OU. 181/363 discharged. • 1253 not appropriate for OU. 799/1253
admitted. 232/799 were appropriate for OU.

Observation Units - How?
• Clear admission criteria• Well planned policies and procedures• Know who’s the boss!• Proper staffing, location and
equipement• Quality assurance

Observation Units – Quality Assurance
• Utilization data:– Volume: %admit from ED and to inpatient
unit, timing, duration of stay, % exceeding time limit
– Care: morbidity, mortality, critical incidents, appropriateness of treatment, RTED
– Patient complaints
• Financial benefit?– Studies need to be done to assess actual
benefit vs theorized.– Strict inclusion criteria would be required

Observation Units – Benefit?

New Fellowship….. ACH - Career Opportunity in Emergency Medicine . . .
Waiting Room Medicine Fellowship
• Rotations include:– Unmonitored Cardiology — Make decisions about which of the 6 patients with
crushing chest pain should get the next available bed when it opens up in the morning.
– WR Surgery — You'd be surprised how many things you can sew, lance, drain and wrap in a simple WR chair.
– Communication Skills — Key objectives for the communication skills module include learning how to ask embarrassing questions in front of a crowd, learning to say "I'm sorry for the care you're receiving" in a manner that doesn't lead to your being assaulted by angry family members, and learning to say "these curtains are soundproof" with a straight face.
– EMS — Deal with ambulance diversion, critical care bypass; provide catering and nutritional requirements for waiting ambulance crews. Gain valuable skills in diverting ambulances with seriously ill patients from your ED to another equally overcrowded ED.

New Fellowship….. ACH - Career Opportunity in Emergency Medicine . . . Waiting
Room Medicine Fellowship
• Rotations include:– Lab & Radiology — Learn to make judicious use of investigations based on a
triage note and/or EMS report; no need to bother yourself with talking to or examining the patient until all the labs are back.
– Triage in the Real World — Practise reverse triage, where CTAS IVs and Vs are seen expeditiously, because they are "quick and easy," and CTAS IIs and IIIs are left to languish for hours.
– WR Ethics — Triage the conflicting values of good patient care and maintaining the flow.
– WR Admin Interactions — Dealing with disappointment; how to carry on after seeking help from the administrators on call.
– WR Patients as Monitors — Learning to use other WR patients for the reassessment of critically ill patients (with a focus on teaching lay people about the recognition of seizures, initial management of cardiac arrest, and guidelines for involving the triage nurse in WR care).

New Fellowship….. ACH - Career Opportunity in Emergency Medicine . . . Waiting
Room Medicine Fellowship
• Advanced Electives– Parking Lot Medicine – WR Intensive Care — Pocket Pressors are our friends
• Learning Materials– Standard EM texts, PLUS – All seasons of MASH on DVD
• Special Opportunity for ED Chiefs!

ACH - Career Opportunity in Emergency Medicine . . . Waiting Room Medicine Fellowship
• Applicants must have 1 yr of EM experience or be a final year resident.• CMPA coverage is essential – you are going to need it!• Pls send a letter detailing why you would like to specialize in WR medicine.
New Fellowship…..