Embed Size (px)
Citation preview
Adjunct Approaches to the Care of the PARDS
Patient
Doug Willson, MD Children’s Hospital of Richmond April 21, 2015
Disclosures
! I am a consultant for Discovery Laboratories
! No other conflicts to disclose
Adjunct Treatments The most important “adjunct
treatment” is more of a philosophy—we now understand that it is not necessary to destroy the lung to save the patient
--”baby lung” concept " low Vt ventilation --permissive hypercarbia --permissive hypoxia

SUPPORTIVE THERAPY
Adjunctive Therapy
Pop Quiz What is the most common avoidable cause of morbidity and mortality in PARDS? 1. Accidental extubation 2. Fluid overload 3. Pneumothorax 4. Nosocomial infection
Avoidance of Nosocomial Infection!
! Hospital-acquired infections have a higher mortality than any of the top 10 leading causes of death in the U.S. (and rank 8th as cause of death in U.S.)
! VAP, for example, increases mortality 4 fold in adult intensive care
! Bloodstream infections are equally frightening
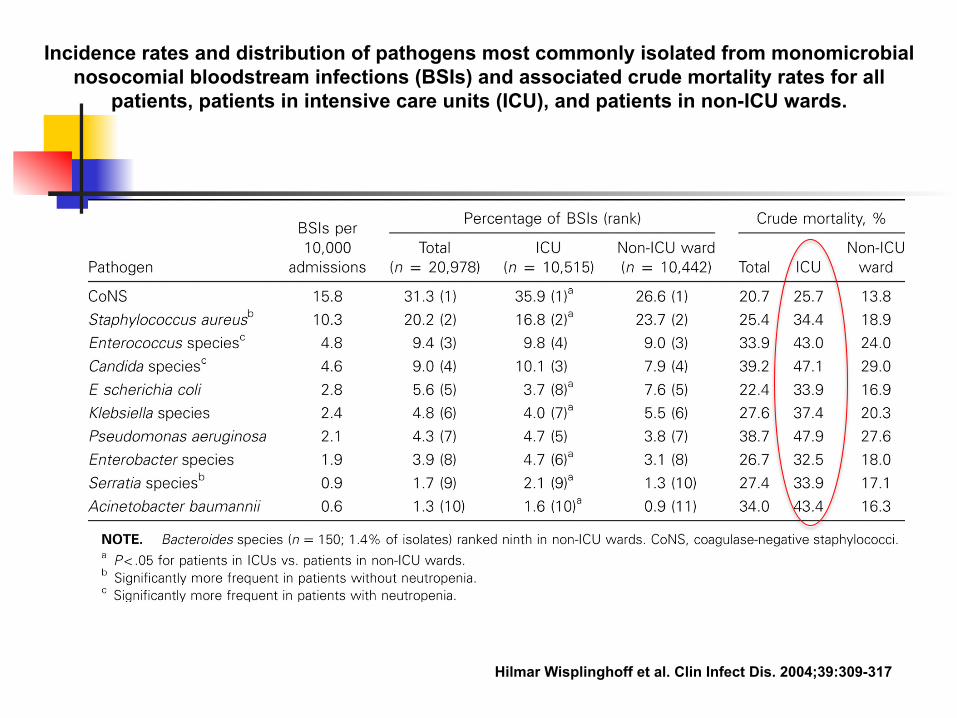
Incidence rates and distribution of pathogens most commonly isolated from monomicrobial nosocomial bloodstream infections (BSIs) and associated crude mortality rates for all
patients, patients in intensive care units (ICU), and patients in non-ICU wards.
Hilmar Wisplinghoff et al. Clin Infect Dis. 2004;39:309-317

Wash your hands!!!!!!!
Nutrition ! Inability to achieve 1/3 of energy needs in first 10
days clearly associated with mortality*
! A higher % of goal enteral nutrition intake associated with lower mortality*
! EDEN trial in adults, however, showed no benefit to “trophic” vs. “full” enteral feedings in first 6 days of ARDS (or to the specific supplementation with fish oil, etc.)**
*Mehta, CCM 2012 **Rice, JAMA 2012
2
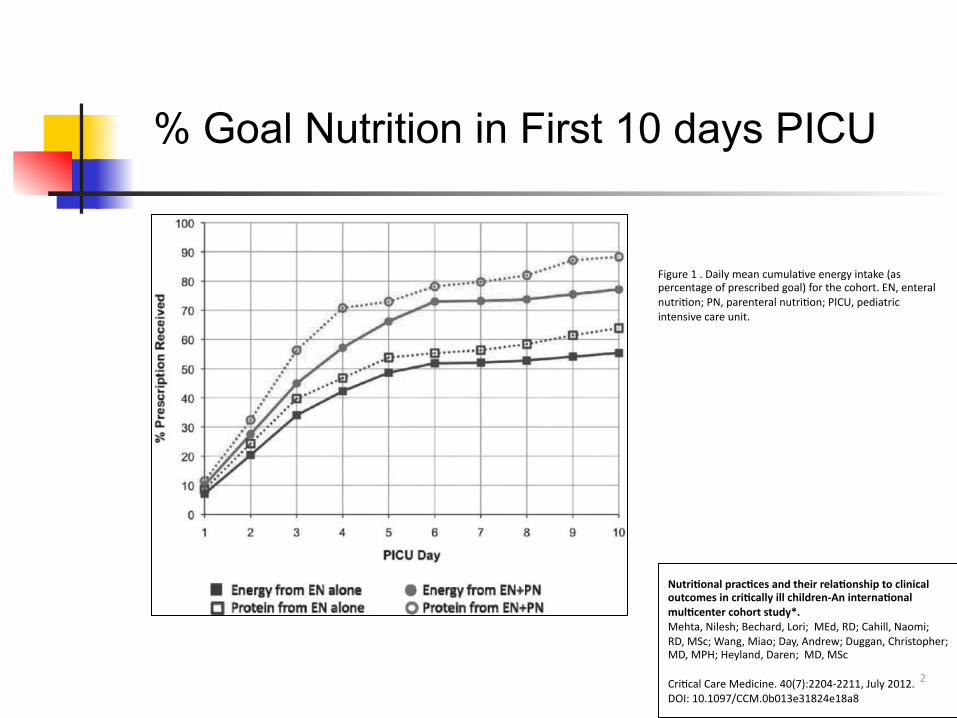
Nutri&onal prac&ces and their rela&onship to clinical outcomes in cri&cally ill children-‐An interna&onal mul¢er cohort study*. Mehta, Nilesh; Bechard, Lori; MEd, RD; Cahill, Naomi; RD, MSc; Wang, Miao; Day, Andrew; Duggan, Christopher; MD, MPH; Heyland, Daren; MD, MSc CriDcal Care Medicine. 40(7):2204-‐2211, July 2012. DOI: 10.1097/CCM.0b013e31824e18a8
Figure 1 . Daily mean cumulaDve energy intake (as percentage of prescribed goal) for the cohort. EN, enteral nutriDon; PN, parenteral nutriDon; PICU, pediatric intensive care unit.
% Goal Nutrition in First 10 days PICU
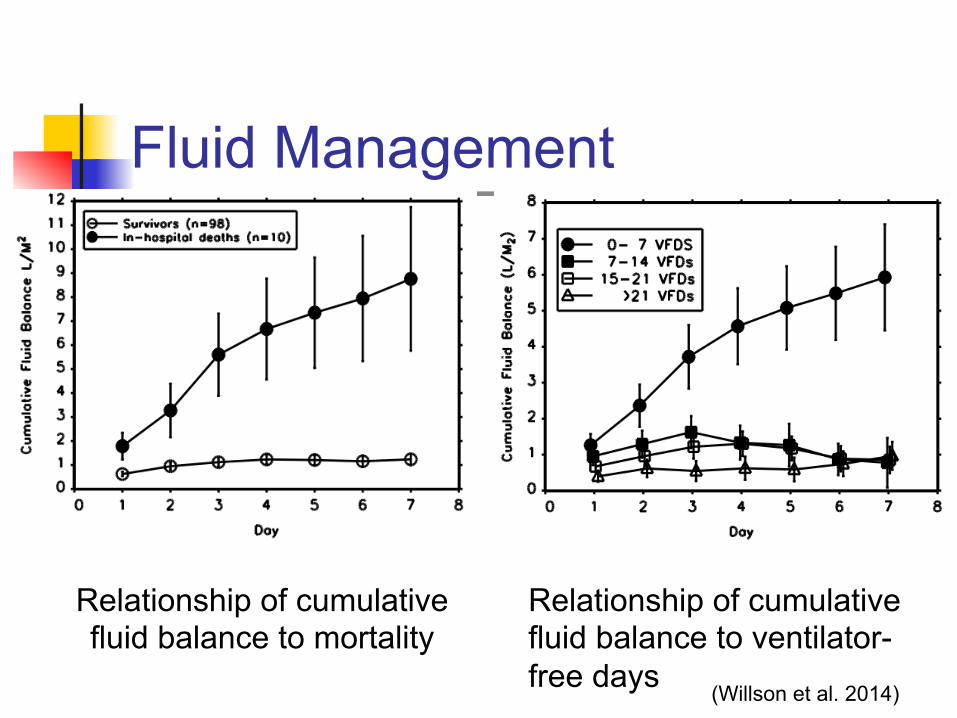
Fluid Management ! “The dry lung is the happy lung”! ! Initial resuscitation is vital (Rivers, et al),
but fluid restriction after resuscitation to avoid fluid overload shown by FACTT trial to decrease days on ventilator
! In my experience this is one of the most commonly overlooked aspects of management
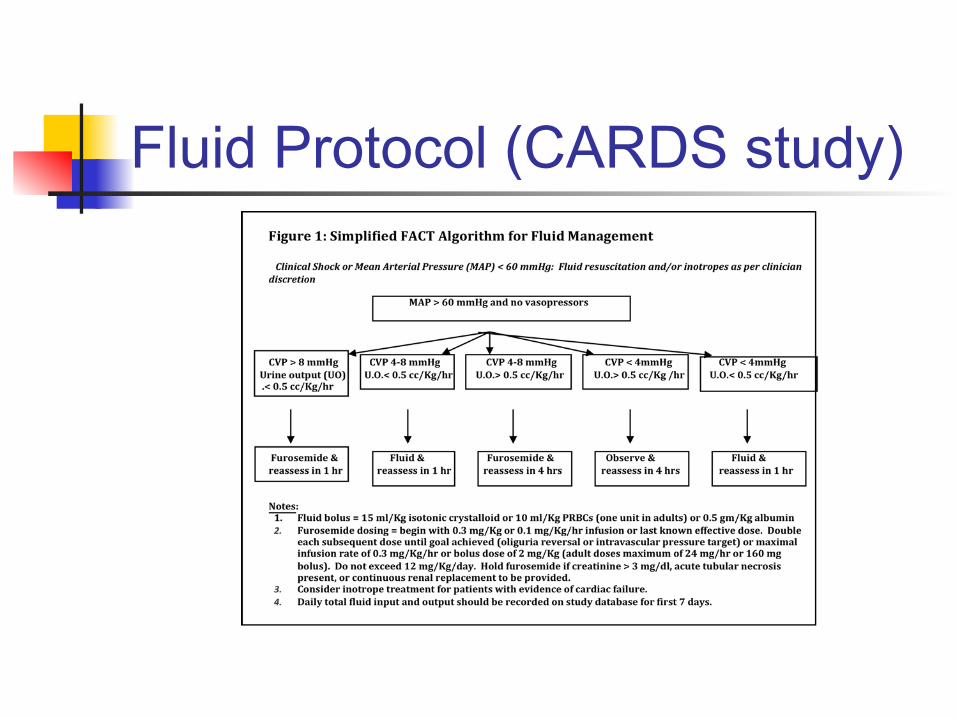
Fluid Protocol (CARDS study)
Fluid Management
Relationship of cumulative fluid balance to mortality
Relationship of cumulative fluid balance to ventilator-free days (Willson et al. 2014)
Fluid Management ! Fluid is a “drug” like any other and has a
therapeutic range and a toxicity ! Positive pressure ventilation leads to
fluid accumulation (decreased venous return)
! Should aim toward “even” or “negative” fluid balance after stabilization
Sedation: Pop Quiz #2 Which of the following medications have been associated with tolerance and withdrawal in children? 1. Midazolam (Versed) 2. Dexmedetomidine (Precedex) 3. Hydromorphone (Dilaudid) 4. Pentobarbital 5. Fentanyl 6. Lorazepam 7. All of the above
Sedation/Analgesia ! Adequate sedation/analgesia is necessary to
prevent adverse consequences in kids (i.e., accidental extubation)
! Over-sedation is the most common reason for failure to wean from mechanical ventilation
! Tolerance and it’s corollary, withdrawal, are common problems in the PICU—and prolong hospital stay.
! Unfortunately RESTORE study did not show shortened duration of mechanical ventilation with protocolized sedation
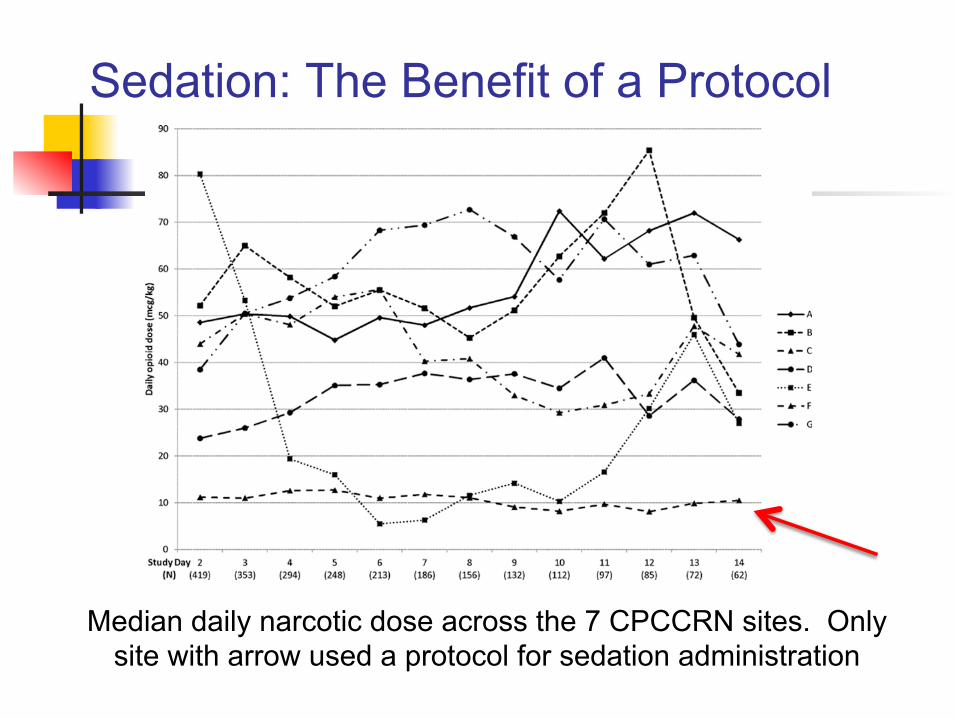
Sedation: The Benefit of a Protocol
Median daily narcotic dose across the 7 CPCCRN sites. Only site with arrow used a protocol for sedation administration
Supportive Care Avoidance of infection, appropriate fluid management, good nutrition, and judicious sedation are likely as important (if not more important) than any specific therapy for PARDS!
Adjunct Care ! Specific adjunctive therapy
! Nitric oxide ! Prone positioning ! Surfactant ! Steroids ! ECMO
Pop Quiz #3 Inhaled nitric oxide 1. Is expensive 2. Generally immediately improves oxygenation 3. Has been associated with renal dysfunction 4. Improves distribution of perfusion relative to
ventilation in the lung 5. All of the above 6. Only 1, 2, 4
Nitric oxide ! Vasodilates where the gas goes"improved
distribution of perfusion relative to ventilation ! Invariably initially improves PaO2 but not sustained ! Expensive ($140/hr) ! Oxygenation can worsen when discontinued because
of inhibition of endogenous NO ! No demonstrated improvement in duration of
ventilation, LOS, or mortality ! Effective treatment in pulmonary hypertension
(although pulmonary hypertension is part of PARDS)
Just say no!
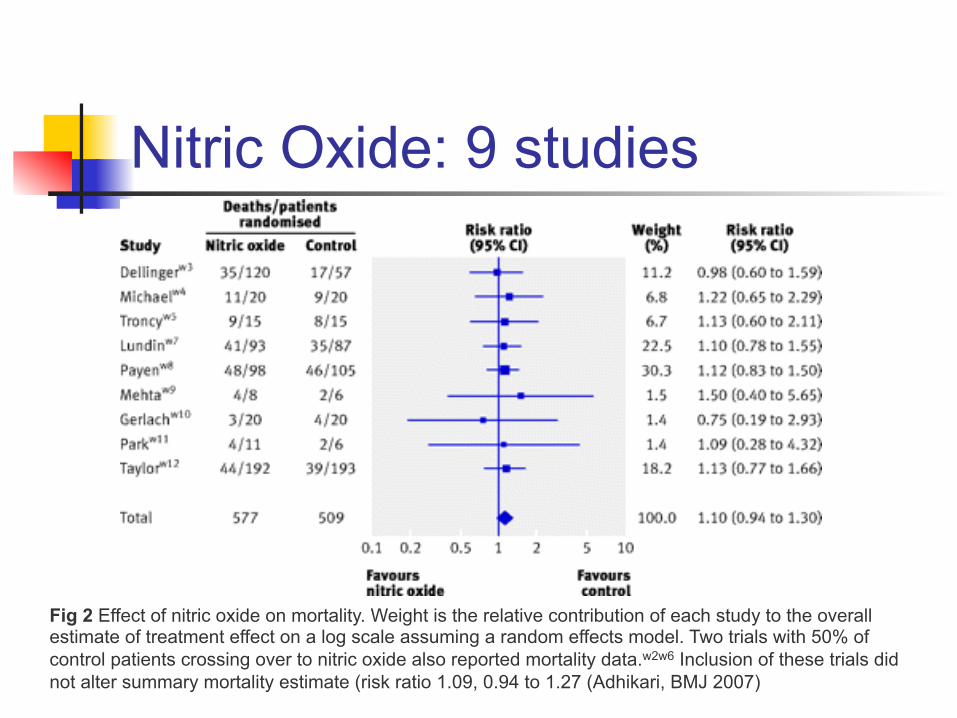
Nitric Oxide: 9 studies
Fig 2 Effect of nitric oxide on mortality. Weight is the relative contribution of each study to the overall estimate of treatment effect on a log scale assuming a random effects model. Two trials with 50% of control patients crossing over to nitric oxide also reported mortality data.w2w6 Inclusion of these trials did not alter summary mortality estimate (risk ratio 1.09, 0.94 to 1.27 (Adhikari, BMJ 2007)
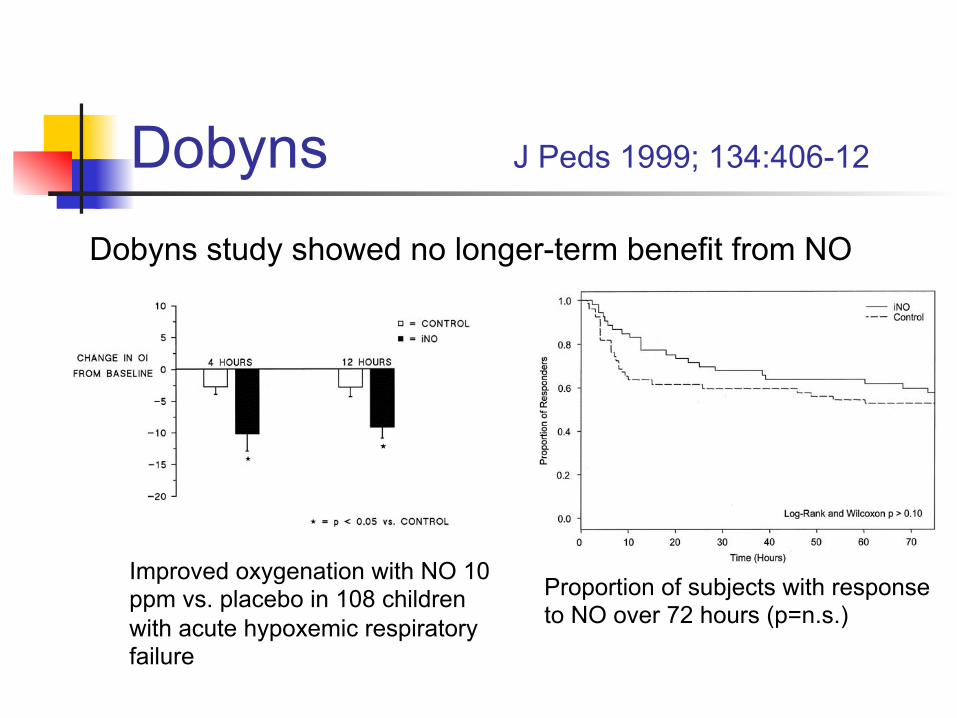
Dobyns J Peds 1999; 134:406-12
Improved oxygenation with NO 10 ppm vs. placebo in 108 children with acute hypoxemic respiratory failure
Proportion of subjects with response to NO over 72 hours (p=n.s.)
Dobyns study showed no longer-term benefit from NO

Nitric Oxide
Just say no!
Prone Positioning
Prone Positioning ! “Recruitment maneuver” ! Like NO, transiently improves PaO2 ! No longer-term benefit in initial studies
(Gattinoni, Curley) ! Few side effects, easily accomplished in
small children
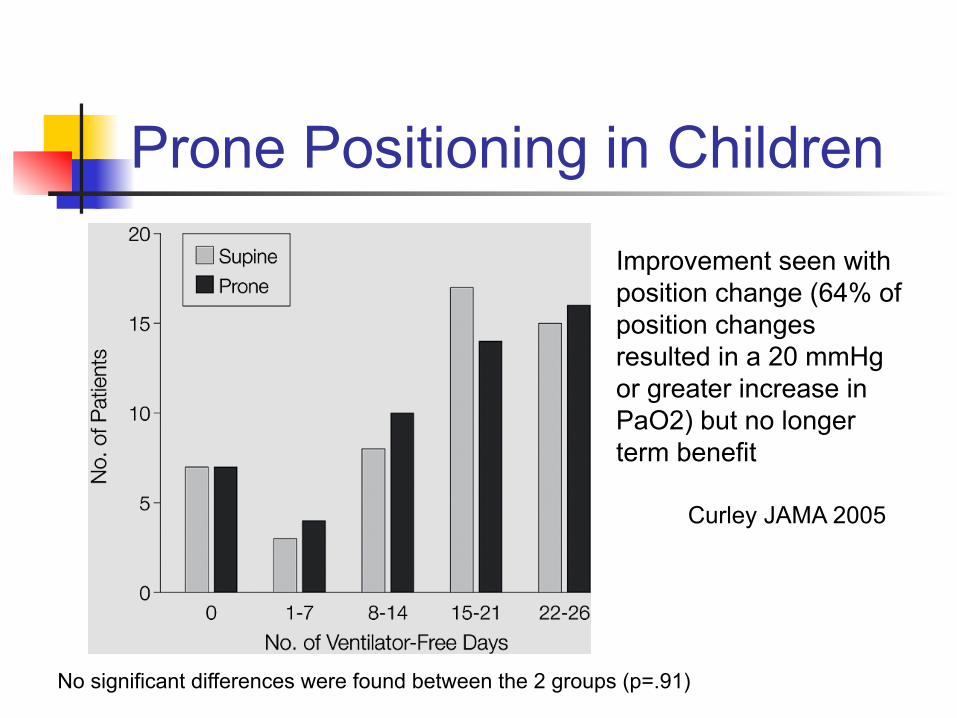
Prone Positioning in Children
Improvement seen with position change (64% of position changes resulted in a 20 mmHg or greater increase in PaO2) but no longer term benefit
No significant differences were found between the 2 groups (p=.91)
Curley JAMA 2005
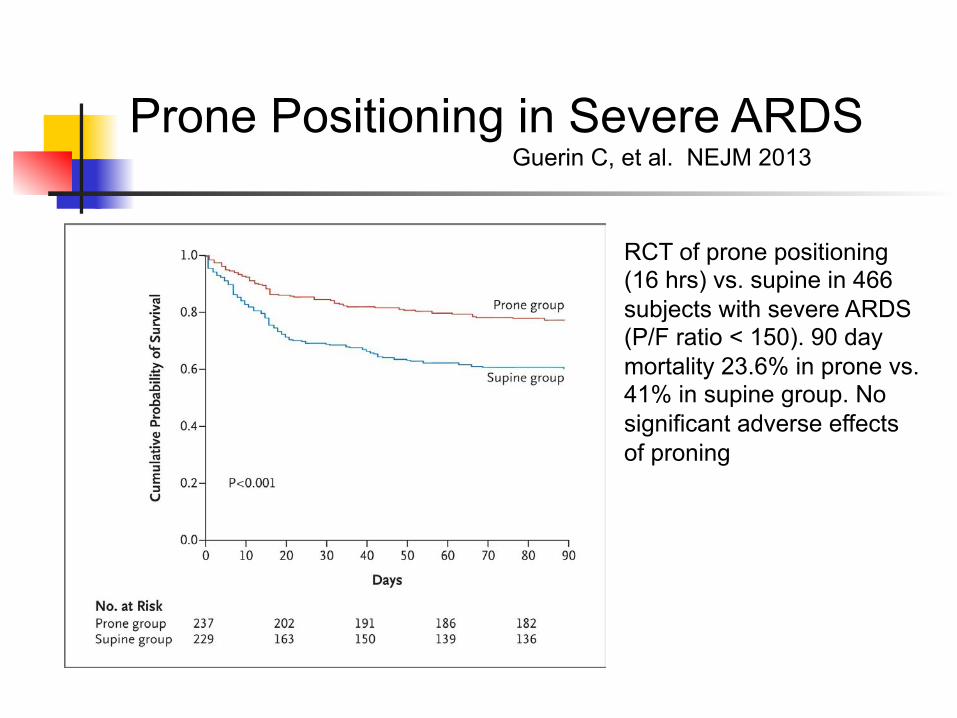
Kaplan–Meier Plot of the Probability of Survival fromRandomization to Day 90.
Guérin C et al. N Engl J Med 2013;368:2159-2168
Prone Positioning in Severe ARDS Guerin C, et al. NEJM 2013
RCT of prone positioning (16 hrs) vs. supine in 466 subjects with severe ARDS (P/F ratio < 150). 90 day mortality 23.6% in prone vs. 41% in supine group. No significant adverse effects of proning
Prone Positioning ! Dependent atelectasis is usual in ARDS ! “Proning” recruits these areas "
improved oxygenation ! Really no down side, particularly in kids ! Despite absence of evidence for longer-
term efficacy, would recommend
Steriods ! Older studies--no benefit in acute ARDS ! Newer study (Meduri)--benefit in “chronic”
stage of ARDS ! Concept of “CIRCI” (critical illness related
corticotropin insufficiency)
! Newer still study (ARDSnet)--not beneficial in “chronic” stage of ARDS
! Newest studies--may be beneficial in acute ARDS, chronic ARDS, or not!
Pop Quiz: Corticosteroids
1. Cataracts 2. Hypertension 3. Calcium wastage 4. Psychosis 5. Abdominal stria 6. Sleep disturbances 7. Weight gain
8. Osteoporosis 9. Avascular necrosis 10. Seizures 11. Depression 12. Suppression of the
HPA axis 13. Myopathy 14. Acne
Corticosteroids have been associated with all but one of the following side effects:
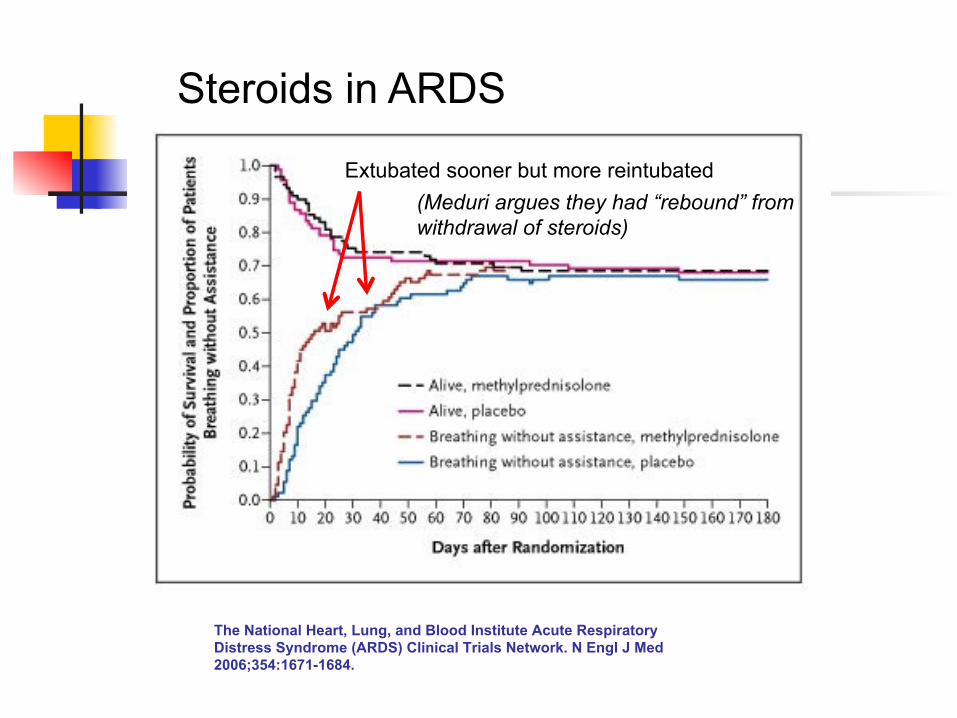
Probability of Survival and the Proportion of Patients with Persistent ARDS Who Became Able to Breathe without Assistance during the First 180 Days after Randomization.
The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. N Engl J Med 2006;354:1671-1684.
Steroids in ARDS
Extubated sooner but more reintubated (Meduri argues they had “rebound” from withdrawal of steroids)
Meduri, G. U. et al. Chest 2007;131:954-963
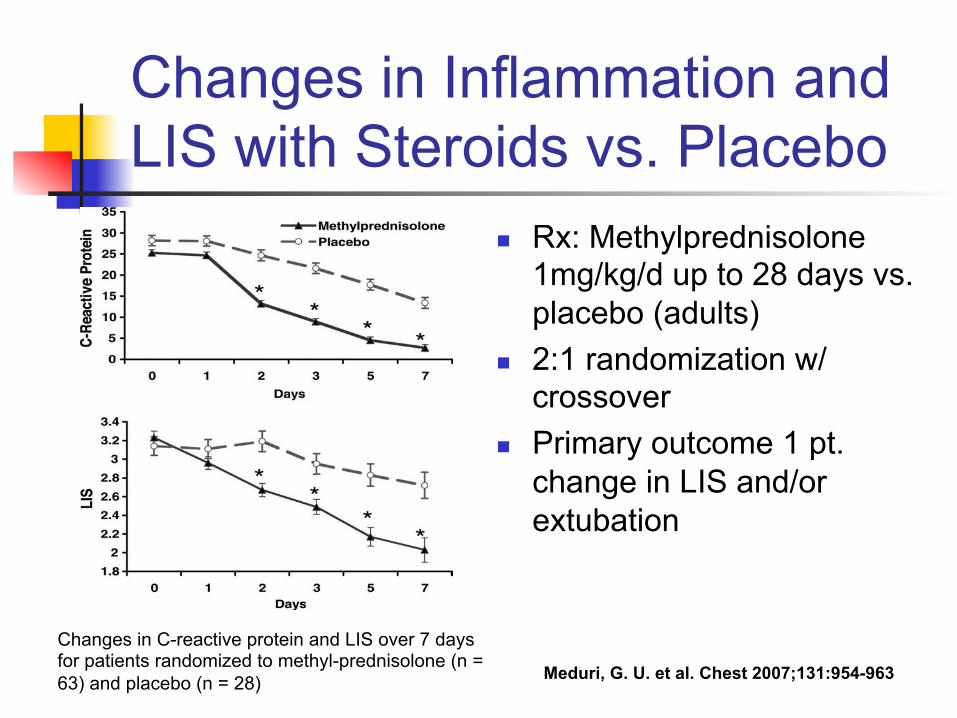
Changes in C-reactive protein and LIS over 7 days for patients randomized to methyl-prednisolone (n = 63) and placebo (n = 28)
Changes in Inflammation and LIS with Steroids vs. Placebo
! Rx: Methylprednisolone 1mg/kg/d up to 28 days vs. placebo (adults)
! 2:1 randomization w/ crossover
! Primary outcome 1 pt. change in LIS and/or extubation
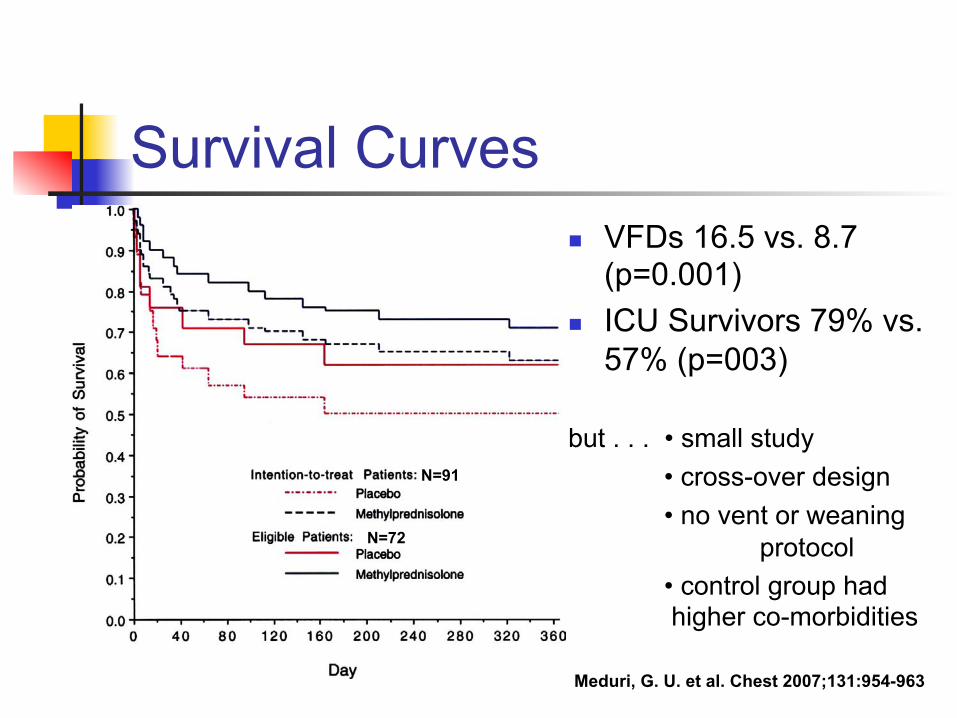
Meduri, G. U. et al. Chest 2007;131:954-963
Survival Curves ! VFDs 16.5 vs. 8.7
(p=0.001) ! ICU Survivors 79% vs.
57% (p=003) but . . . • small study
• cross-over design • no vent or weaning
protocol • control group had
higher co-morbidities
N=91
N=72
Steroids
No studies in kids . . .
. . . but steroids were used in 40% of patients in one Indian study and 60% in a German study
Surfactant ! RCTs in adults have been disappointing
(Anzueto, Gregory, Spragg) ! RCTs in children more hopeful (Willson,
Luchetti) ! No currently active studies in ARDS
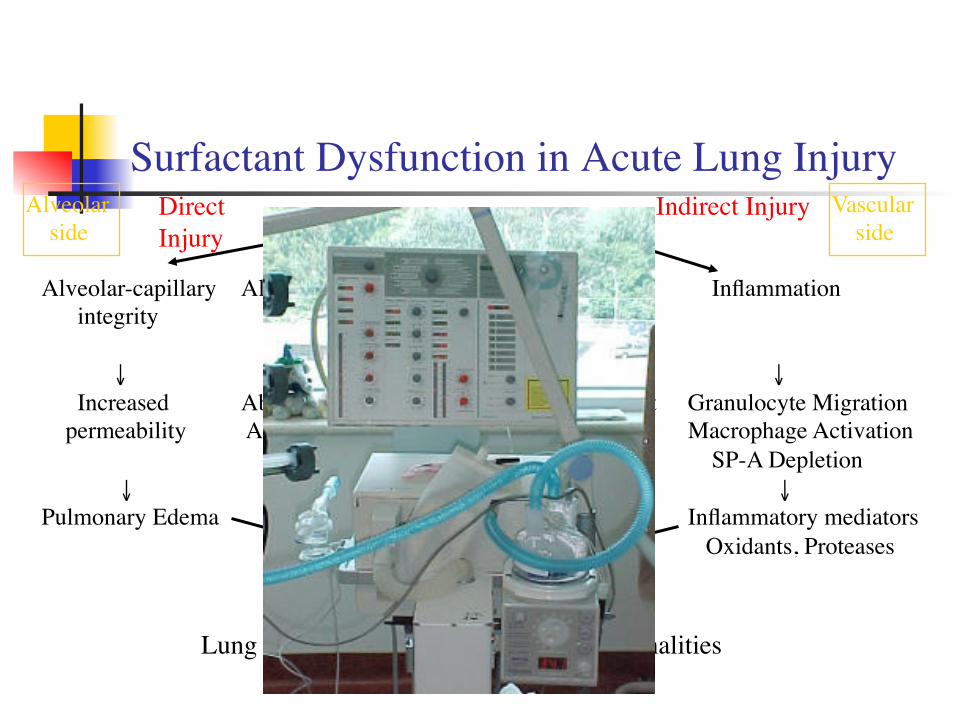
Surfactant Dysfunction in Acute Lung InjuryAcute Lung Injury
Alveolar-capillary integrity
↓ Increased permeability
↓Pulmonary Edema
Alveolar metabolism of surfactant
↓Abnormal Surfactant Aggregate Forms
Type IIPneumatocytes
↓Altered Surfactant • Synthesis • Secretion • Composition
Inflammation
↓Granulocyte MigrationMacrophage Activation SP-A Depletion ↓Inflammatory mediators Oxidants, ProteasesSurfactant Dysfunction
Lung mechanics and gas exchange abnormalities ↓FRC ↓Compliance ↑Shunt
Direct Injury
Indirect InjuryAlveolar side
Vascular side
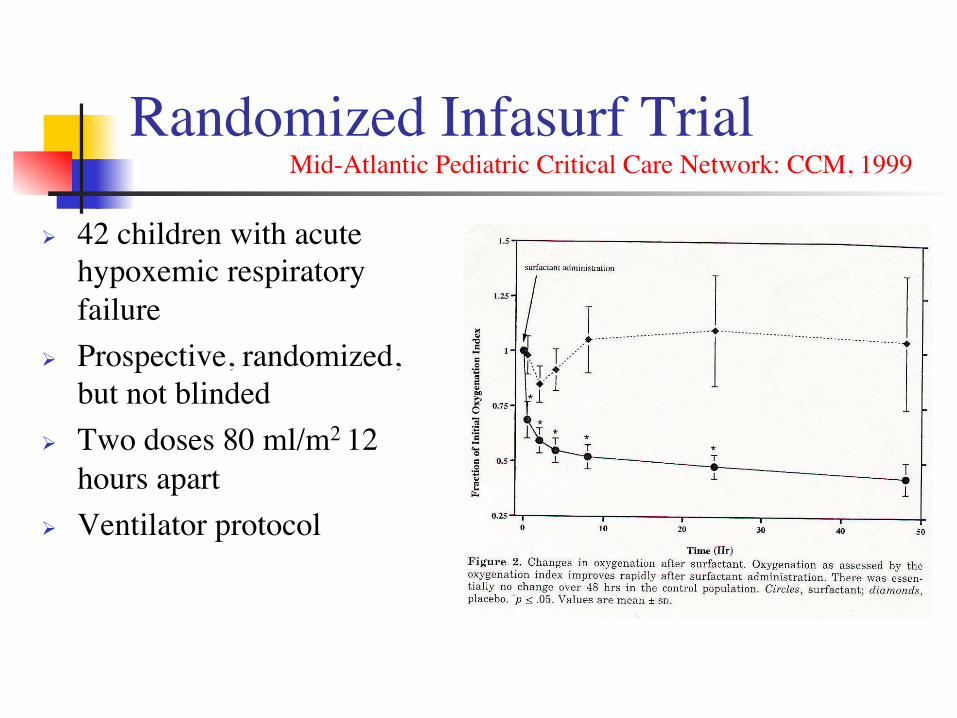
Randomized Infasurf Trial��� Mid-Atlantic Pediatric Critical Care Network: CCM, 1999
# 42 children with acute hypoxemic respiratory failure
# Prospective, randomized, but not blinded
# Two doses 80 ml/m2 12 hours apart
# Ventilator protocol
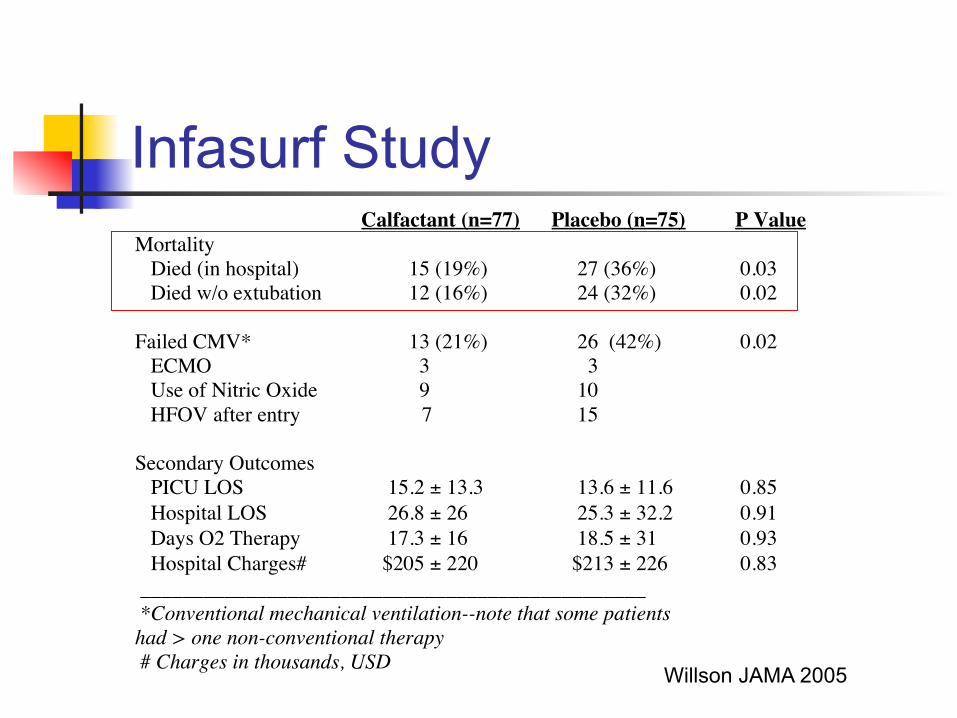
Infasurf Study
Calfactant (n=77) Placebo (n=75) P ValueMortality
Died (in hospital) 15 (19%) 27 (36%) 0.03 Died w/o extubation 12 (16%) 24 (32%) 0.02
Failed CMV* 13 (21%) 26 (42%) 0.02 ECMO 3 3 Use of Nitric Oxide 9 10 HFOV after entry 7 15
Secondary Outcomes PICU LOS 15.2 ± 13.3 13.6 ± 11.6 0.85 Hospital LOS 26.8 ± 26 25.3 ± 32.2 0.91 Days O2 Therapy 17.3 ± 16 18.5 ± 31 0.93 Hospital Charges# $205 ± 220 $213 ± 226 0.83
________________________________________________ *Conventional mechanical ventilation--note that some patients had > one non-conventional therapy # Charges in thousands, USD Willson JAMA 2005
CARDS Study ! No change in oxygenation with
surfactant ! No difference in VFDs, mortality, etc. in
either the adult or pediatric arm ! Differences in drug and recruitment may
account for lack of response
Exogenous surfactant
The jury is still out . . .
ECMO ! When all else fails . . . ! Use for respiratory failure has leveled
off in the U.S. (ELSO statistics), although increasingly used cardiac and for E-CPR
! New technology (smaller pumps, better cannula, more portable) is likely to lower the threshold for use.
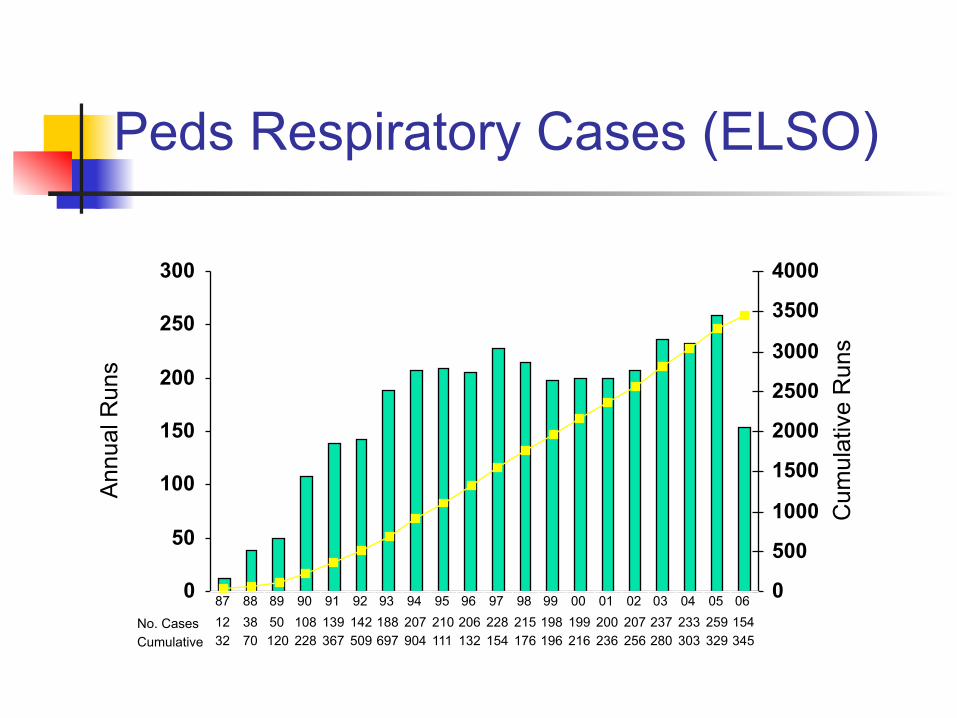
Peds Respiratory Cases (ELSO)
0
50
100
150
200
250
300
An
nu
al R
un
s
0
500
1000
1500
2000
2500
3000
3500
4000
Cu
mu
lative
Ru
ns
No. Cases 12 38 50 108 139 142 188 207 210 206 228 215 198 199 200 207 237 233 259 154
Cumulative 32 70 120 228 367 509 697 904 111 132 154 176 196 216 236 256 280 303 329 345
87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06
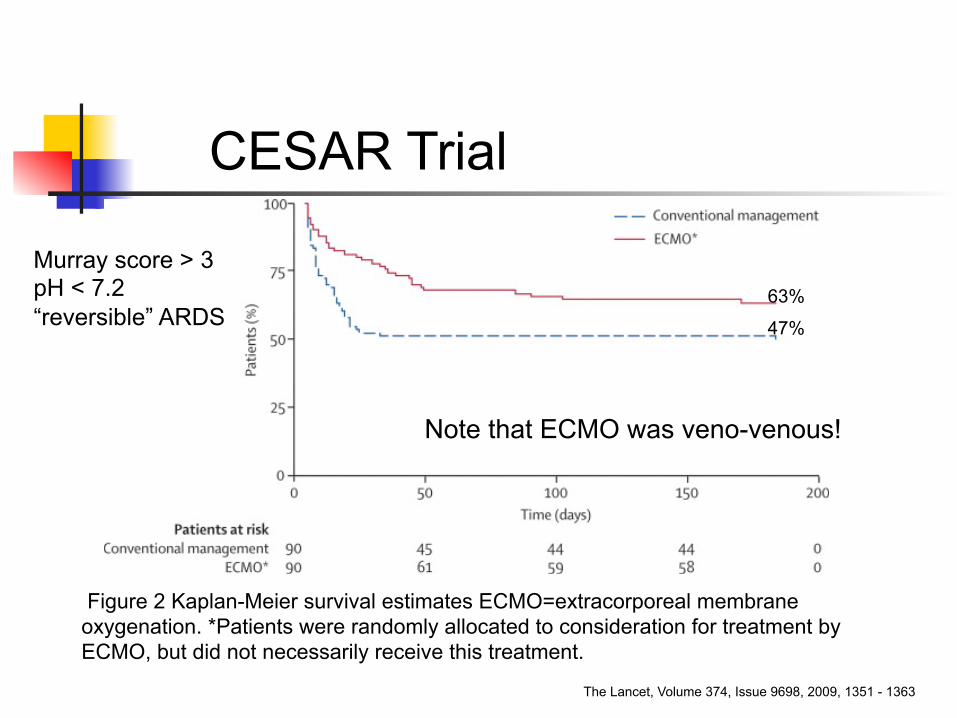
Figure 2 Kaplan-Meier survival estimates ECMO=extracorporeal membrane oxygenation. *Patients were randomly allocated to consideration for treatment by ECMO, but did not necessarily receive this treatment.
The Lancet, Volume 374, Issue 9698, 2009, 1351 - 1363
CESAR Trial
Note that ECMO was veno-venous!
63%
47%
Murray score > 3 pH < 7.2 “reversible” ARDS
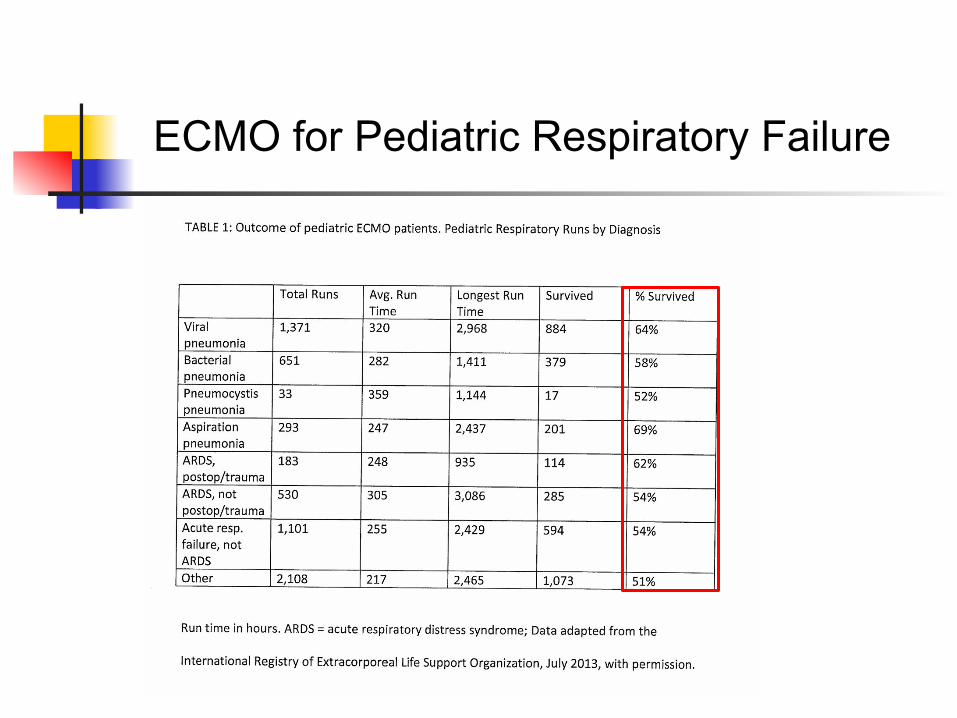
ECMO for Pediatric Respiratory Failure
ECMO Questions ! Should ECMO always be the “last
resort”? ! Should passive “ECCOR” be considered
like “lung dialysis” and used preventively? ! How (and in whom) are we to study these
issues?
Pop Quiz Mortality is decreasing in PARDS 1. True 2. False
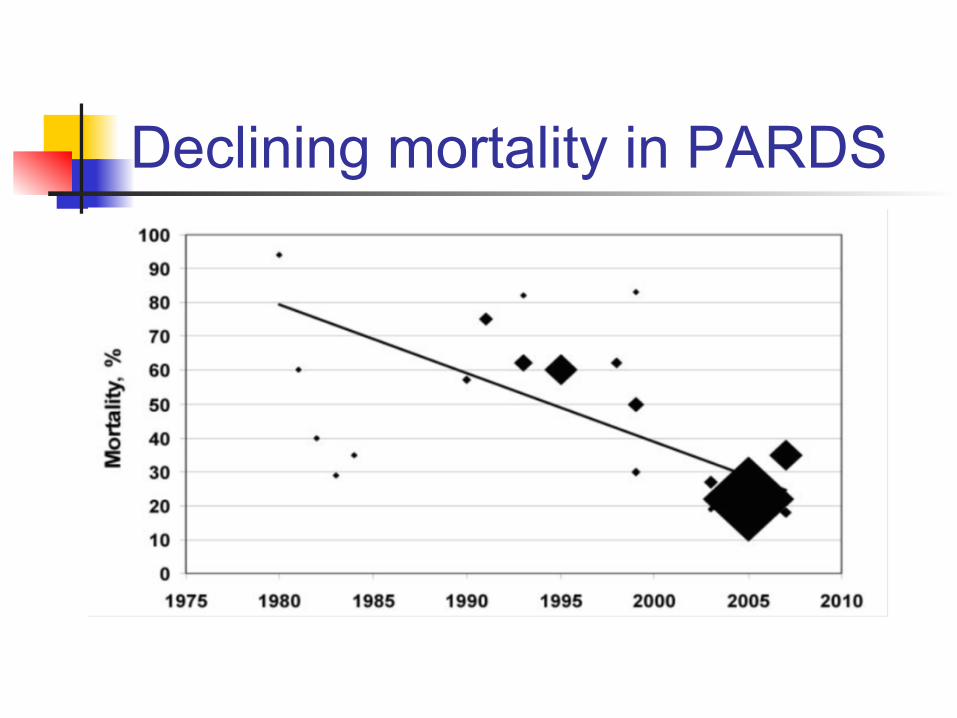
Declining mortality in PARDS
Adjunctive Rx for PARDS Conclusions ! Blood gases don’t have to be “normal” ! “Supportive care” is critical ! Surfactant and nitric oxide probably not
helpful and both are expensive ! Prone positioning is free, likely not harmful,
and worth trying ! ?Steroids for “chronic ARDS” ! To paraphrase Bogart “we’ll always have
ECMO”
Future Directions
It’s difficult to make predictions, particularly about the future . . .
Yogi Berra