Embed Size (px)
Citation preview

ADHD CNS stimulants overuse
Vita Chau TranDoctor of Pharmacy candidate 2016
APPE Transitional care studentPreceptor: Amy Lemieux

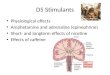
ObjectivesADHD definition, diagnosis, and treatmentCNS stimulants and its effects on body Management of ADHD CNS stimulant overdoseWhat can healthcare professionals do to
decrease number of CNS stimulant overuses

Background

Trend of US prescription on ADHD stimulants

What is ADHD? ADHD (Attention-deficit/hyperactivity disorder) is
neurodevelopmental disorder. It is described as a “persistent” or on-going pattern of
inattention and/or hyperactivity-impulsivity that gets in the way of daily life or typical development.
Patients with ADHD usually have difficulties with Maintaining attention Executive functioning (or the brain’s ability to begin an activity,
organize itself and manage tasks) Maintaining working memory
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5™ (5th ed.). Arlington, VA: American
Psychiatric Publishing, Inc.

CausesGenetics
Many studies have shown a link to biological relatives.
It is shown that both the genes that regulate Dopamine (DA) and Norepinephrine (NE) are involved.
The prevalence of getting ADHD in patients, who have siblings with an ADHD diagnosis is 20-50%.

Causes (continue)Neurobiology
Lack of NE and DA has shown to produce ADHD like symptoms
Dysfunction in prefrontal-striatal neural circuitsEnhancing the reuptake of DA and DA catabolism,
which causes DA removal in brain to occur fasterP50 suppression deficiency
Ability to suppress reaction to an auditory stimuli

A study compared 234 children with ADHD and 231 typically developing children, using 837 neuroanatomical magnetic resonance images acquired longitudinally.
Subjects with ADHD compared to controls have shown: The surface area developmental trajectory was delayed The cortical thickness was delayed Approximately a 2 to 3 year developmental delay in children
At 18 years of age, the differences were no longer significant (nearly 80% patients caught up and were fully developed at the age of 18 to 25)
Biol Psychiatry. 2012 Aug 1;72(3):191-7. doi: 10.1016/j.biopsych.2012.01.031. Epub 2012 Mar 13.
Delayed brain maturation

How does ADHD get diagnosed?
Symptom Criteria
At least six symptoms of inattention or at least six symptoms of hyperactivity or impulsivity have persisted for at least 6 months and occur often enough to be maladaptive and inconsistent with developmental level.
Inattention
Fails to pay close attention to details or makes careless mistakes in schoolwork, work, or other activities
Has difficulty sustaining attention in tasks or play activities Does not seem to listen when spoken to directly Does not follow through on instructions and fails to finish schoolwork, chores, or work duties
(not due to oppositional behavior or failure to understand) Has difficulty organizing tasks and activities Avoids, dislikes, or is reluctant to engage in tasks requiring mental effort (e.g., schoolwork,
homework) Loses things necessary for tasks or activities (e.g., written instructions, school assignments,
textbooks, pencils, tools, toys) Is easily distracted by extraneous stimuli Is forgetful in daily activities

ADHD diagnostic Hyperactivity
Fidgets with hands or feet and squirms in seat Leaves seat in classroom or other situations where remaining
seated is expected Runs about or climbs excessively in situations where these
activities are considered inappropriate; in adolescents or adults, this feature may be limited to subjective feelings of restlessness
Has difficulty in playing or engaging in leisure activities quietly
Is on the go or acts as if driven by a motor Talks excessively

How does ADHD get diagnosed?
Impulsivity
Blurts out answers before questions are completed Has difficulty awaiting turn (impatient) Interrupts or intrudes on others (e.g., butts in on conversations, games)
Exclusion Criteria
Symptoms do not occur exclusively during course of a pervasive developmental disorder, schizophrenia, or psychotic disorder.
Symptoms are not better accounted for by another mental disorder (e.g., mood disorder, anxiety disorder, dissociative disorder, personality disorder).

ADHD treatment optionsFirst line:
CNS stimulants (Methylphenidate, Amphetamines)
Second line:Atomoxetine
Third line Does not show as much improvement
BupropionModafinilDesipramine up to 200mg/day

What is AmphetamineBrand name: Adderall, Adderall XR Indications: ADHD, narcolepsyMechanism of action:
Stimulates the release of norepinephrine (NE) and other biologic amines from central adrenergic receptors.
On higher dosages, they cause the release of dopamine from mesocorticolimbic and nigrostrialtal dopamine system.
At still higher doses, amphetamine stimulates the release of 5-HT and acts as a direct agonist on central 5-HT receptors.
Acts as direct and indirect stimulant that is similar to cocaine to cause catecholamine release in central nervous system.

MethylphenidatesBrand name: Concerta®, Ritalin®,Methylin®,
Metadate®Mechanism of action:
Blocks the reuptake of norepinephrine and dopamine into presynaptic neurons; appears to stimulate the cerebral cortex and subcortical structures similar to amphetamines
Exerts effects similar to Amphetamines including adverse effects


Effects of CNS stimulant

Can you overdose on a CNS stimulant?

Patient caseCD,13 years old, 50-kg girl with a past medical
history significant for ADHD presented to ER 2 hours after ingesting approximately 20 Adderall 5-mg and 10-mg tablets of herself and her brother’s prescribed medications.
Patient reported ingesting medications to get high, an idea fostered by her friends, one of whom reportedly had previously ingested six Adderall tablets.
Patient denied suicidal ideation, intent or previous recreational drug use.

CD case (continue)Signs and symptoms presenting 2 hours after
ingestion:Dyspnea Increased work of breathingDenied chest pain, palpitations, or dizziness. She was alert and oriented to name, place, and
situation, but was intermittently combativeVital signs: BP: 218/128mmHG, HR 144/min, RR
20/min

CD (continue)Labs:
ECG demonstrated sinus tachycardia with ventricular bigeminy at 149/min
Native complexes demonstrated ST-segment depression, most pronounced in the inferior and lateral leads
CBC normalWBC: 13.8 x 109/L Toxicology screening was positive for
amphetamines onlyHCG was negative

Management overdoseSigns and symptoms 1st line treatment
First thing Supportive care and reassuranceWithin 1 hour of ingestion (if patient is cooperative)
Activated Charcoal 50 g orally as single dose, may repeat at 4 to 6
hour intervalsMild agitation (level 1)
(mildly aroused and cooperative, alert, may be irritable and pacing
around but still can talk or cooperate with exam, normal
vital signs)
Reassurance and oral sedation1. Diazepam: 10 mg PO as
single dose, may repeat if needed
2. Lorazepam: 0.5 mg orally as single dose, may repeat
3. Alternative: Olanzapine 10mg PO as single dose or
Haloperidol 5 mg as single dose (only in the absence of
QT prolongation)Moderate agitation (level 2)
( moderately aroused, restless, agiated, more vocal,
unreasonable, hostile, uncooperative, tachycardia,
hypertension
Treatment same as above butTertiary options: midazolam 5mg
IV or IM as a single dose

Signs and symptoms First line treatmentSevere agitation (level 3)
(Highly aroused, distressed, fearful, highly restless, and
agitated, noisy, abusive, uncooperative, possibly violent. Presence of security personnel
may be necessary until behavioral disturbance is under control
Parenteral sedation:1. Diazepam 10 mg IV as single
dose, repeat 5 mg dose if needed
2. Secondary options:a. Haloperidol 2.5 to 5 mg IV/IM
single doseb. Midazolam 5mg IV/IM as single
dose3. Tertiary options: Olanzapine 5-
10 mg IM single doseVolume depletion or
rhabdomyolysisHydration
Average patient may need 3-5 L of IV fluids in the first few hours of
admissionMetabolic acidosis Sodium bicarbonate
Electrolytes should be monitored regularly to avoid risk of
hypernatremia and hypokalemia.Dose adjusted based on serum
Bicarb level

Signs and symptoms TreatmentHyperthermia >100oF (>38oC)
but < 103oFDefervescence and muscle
relaxation Cooling blankets and ice packs
in the axillae, groin sponging, cooling fans might help
Diazepam 5-10mg IV/PO as single dose
Hyperthermia >103oF (>39.5oC) Defervescence and muscle paralysis
Indicates severe, potentially life-threatening toxicity and
mandates immediately cooling and muscle paralysis
Patient must be intubated before initiation of paralysis
PancuroniumSupraventricular tachycardia Supraventricular tachycardia
associated with hemodynamic compromised are best treated
with short acting beta blockage Esmolol 50-100
micrograms/kg/min IV

Amphetamine overdose management
Signs and symptoms TreatmentVentricular tachycardia Conventional therapy with anti-
arrhythmic medication or cardioversion
Amiodarone 300mg IV over a period of not less than 3 minutes initially, followed by 15-20mg/kg
IV over 24 hours.Seizure Diazepam IV 5-10mg q 10-20
min. Max 30mg/8-hour periodHypertension Vasodilator
Nitroglycerin: 5-200 micrograms/min IV
Labetalol 40-80 IV q 10 min. Max 300mg/ total dose

CD case (continue)Promethazine 12.5 mg IV and famotidine 20 mg IV
for nausea was givenGastrointestinal decontamination was performed
with 50 g activated charcoal via nasogastric tube1 L of NaCl containing 2 ampules of sodium
bicarbonate (88 mEq) was administered as IV bolus
Patient became increasingly agitated, was placed in soft restraints and was treated with total of 6 mg Lorazepam IV over a 105 minute period

Where is the gap for CNS stimulant overuse to occur?

Tools for assessment ADHD
Connors Parent and Teacher Rating Scale- ADHDConnors Parent and teacher Rating scale DSM-VSnap-IV rating scale


Real life how patient get prescribed CNS stimulants

Reason why students abuse ADHD medications

How to stop stimulants overuse?
Requires patience and empathy from teachers, prescribers, and family
Educate teachers and families about the danger of using stimulants on children Ask for collaborative efforts from families and schools to
treat kids using non-pharm behavioral methods. Prescribers need to have a clear eye and judgment on
prescribing and diagnosing the patients Weighing any risk factors
Disease states that mimic ADHD symptoms (ie: anxiety, depression, stress, sleep disorders)
Consider patient’s specific demographic information

Social and cultural factors that can influence ADHD over- or misdiagnosis
Cultural differences Western countries have been shown a higher number of ADHD
children compared to Asia The symptoms of ADHD is interpreted differently among
Western and Asian countries Parents interpret and observe their children’s behavior based
on sociocultural and ethnic experience School as a culture
Children’s development intersects with prevailing expectations and values in relation to their behavior, performance and achievement.
Children tend to follow and copy their friends’ behaviorsPrater, G., Minner, S., Islam, M., Hawthorne, D., & International Association of, S. E. (1997)
Prout, A. & James, A. (1997). Constructing and reconstructing childhood: Contemporary issues in the sociological study of childhood. London: Falmer press
Moon, Seokyoung. "Cultural Perspectives on Attention Deficit Hyperactivity Disorder:." AJP American Journal of Psychiatry 154.4 (1997): 532-35. Web. 12 June 2015.

What can Pharmacist do to help?
When filling prescription on any CNS stimulants, judgment should always be made to make sure the prescription is safe, reasonable, and accurate for the patient.
Being able to make interventions on any prescription’s problems, for example:High dosage Inadequate filling due dateDuplicate in therapyMultiple drugs filled for same ADHD management

Summary ADHD is one of the most common childhood brain disorders,
that can continue through adolescence and adulthood. ADHD can make it difficult for a child to succeed in school, get
along with others, and finish daily tasks. ADHD can be easily mistaken with other diseases or disorders
(depression, anxiety, sleep disorder, etc.). While CNS stimulants are the most effective way to control the
disorder, they can also exert unpredictable effects for patients (especially adolescents and children).
It is important for the healthcare professionals to be aware of the overuse and abuse of medication, particularly at a young age.

LET KIDS CAN BE KIDS!

References1. "ADHD Attention Deficit and Hyperactivity Disorders." (n.d.): n. pag. American Psychiatric Association. American Psychiatric Association, 2013. Web. 11 June 2015. <http://www.dsm5.org/documents/adhd%20fact%20sheet.pdf>.2. Jackson, Geissler, and Lesch KP. "Result Filters." National Center for Biotechnology Information. U.S. National Library of Medicine, Oct. 2011. Web. 11 June 2015. <http://www.ncbi.nlm.nih.gov/pubmed/21955202>.3 . Volkow ND, Swanson JM. Clinical practice: Adult attention deficit-hyperactivity disorder. N Engl J Med. 2013 Nov 14;369(20):1935-444. Paul, Shaw, Malik M, Watson B, and Sharp W. "Result Filters." National Center for Biotechnology Information. U.S. National Library of Medicine, 13 Mar. 2013. Web. 11 June 2015. http://www.ncbi.nlm.nih.gov/pubmed/224180145. Spencer T, Biederman J, Wilens T. Stimulant treatment of adult attention-deficit/hyperactivity disorder. Psychiatr Clin North Am. 2004 Jun;27(6. Sztajnkrycer, Matthew D., Selena Hariharan, and G. Randall Bond. "Cardiac Irritability and Myocardial Infarction in a 13-year-old Girl following Recreational Amphetamine Overdose." Pediatric Emergency Care 18.4 (2002): n. pag. Web.7. Prater, G., Minner, S., Islam, M., Hawthorne, D., & International Association of, S. E. (1997)8. Prout, A. & James, A. (1997). Constructing and reconstructing childhood: Contemporary issues in the sociological study of childhood. London: Falmer press9. Moon, Seokyoung. "Cultural Perspectives on Attention Deficit Hyperactivity Disorder:." AJP American Journal of Psychiatry 154.4 (1997): 532-35. Web. 12 June 2015























![Performance-enhancing Drugs and Issues of Health & Safety ... · Provigil, Nuvigil, Vigil, Modalert, Modasomil and Modiodal]. Amphetamines –stimulants used to treat ADHD. Adderall](https://img.pdfslide.us/doc/110x75/5fa6a4edb7144d66e25e65c9/performance-enhancing-drugs-and-issues-of-health-safety-provigil-nuvigil.jpg)