Embed Size (px)
DESCRIPTION
onkologi
Citation preview

REVIEW ARTICLE
Salivary Gland Pleomorphic Adenoma
William M. Mendenhall, MD,* Charles M. Mendenhall, MD,† John W. Werning, MD,‡Robert S. Malyapa, MD, PhD,* and Nancy P. Mendenhall, MD*
Abstract: We discuss the optimal treatment and outcomes forpleomorphic adenoma of the salivary glands by reviewing thepertinent literature.
Pleomorphic adenoma is the most common benign salivary glandneoplasm. It is found mostly in the parotid gland in middle-agedwomen. It progresses slowly and, left untreated, can produce sig-nificant morbidity and, rarely, death. The optimal treatment issuperficial or total parotidectomy with facial nerve preservation,which results in local control rates of 95% or higher. Radiotherapy(RT) is useful to obtain local control in patients with positivemargins, unresectable tumors, and multifocal recurrences after priorresection. Local control rates after RT for microscopic and grossresidual tumor are approximately 80% to 85% and 40% to 60%,respectively. The main complication is surgically induced 7th nerveinjury.
Surgery is the mainstay of treatment and results in a very highcure rate. RT increases the likelihood of local control in the smallsubset of patients with incompletely resectable tumors and/or mul-tifocal recurrences.
Key Words: pleomorphic adenoma, salivary gland, treatmentoutcomes
(Am J Clin Oncol 2008;31: 95–99)
Pleomorphic adenomas are the most common benign sali-vary gland neoplasm and, although usually found in the
parotid, may also arise in the submandibular, sublingual, andminor salivary glands.1–6 It occurs most often between theages of 30 and 60 years and is found more commonly infemales than in males.7 Laccourreye et al7 reported on 229patients treated at the University of Paris V (Paris, France)and observed a 1:1.4 male-to-female ratio. O’Brien1 reportedon 254 patients with parotid pleomorphic adenoma operatedat the Royal Prince Alfred Hospital (Sydney, Australia) and
observed a median age of 46 years and a 1:1.7 male-to-femaleratio. Patients usually present with a painless, slow-growingmass. The duration of symptoms is variable. Dawson andOrr8 reported a mean duration of symptoms of 5 years (range,1 month–34 years) in a series of 311 patients treated at theWestern General Hospital and Royal Infirmary (Edinburgh,Scotland). Although progression is slow, left untreated, thetumor can cause significant morbidity and, rarely, death.9,10
Although facial nerve dysfunction at initial presentation isalmost always an indication of a malignant lesion, it is rarelyobserved in patients with locally recurrent parotid pleomor-phic adenomas.10 Approximately 3% to 4% of pleomorphicadenomas may become carcinoma ex-pleomorphic adeno-mas, an aggressive malignancy that may metastasize andresult in death.4,11 The likelihood of malignant transformationincreases with the duration of the lesion.4 Rarely, benignpleomorphic adenoma may metastasize. Nouraei et al12 re-viewed the English literature published between 1953 and2005 and reported on 42 patients with pleomorphic ade-nomas with metastases that were biopsied and also provento be benign-appearing pleomorphic adenoma. The meaninterval between initial presentation and metastases was12.3 years for patients who had no prior local recurrenceand 16.9 years for those who had a previous local recur-rence. The most commonly involved metastatic sites werebone (45%), head and neck including cervical nodes(43%), lung (36%), and abdominal viscera (10%). The5-year cause-specific survival rate after diagnosis of me-tastases was 58%.
The etiology of pleomorphic adenoma is unknown.Alves et al5 reported on 60 patients treated for submandibulargland pleomorphic adenomas at the Cancer Hospital ACCamargo (Sao Paolo, Brazil); immunohistochemical stainsfor Ki-67 were performed to determine mitotic activity andfor mutation of the p53 tumor suppressor gene. All tumorsstained negatively for both Ki-67 and p53. Hamada et al13
analyzed mucins in 9 patients with recurrent pleomorphicadenomas and 40 patients with tumors that had been resectedand not recurred. The immunohistochemical expression ofmucins MUC1, MUC2, MUC4, MUC5AC, and MUC6 wasevaluated. They observed increased expression (defined asuptake in more than 30% of neoplastic cells) of MUC1/DF3in 4 of 9 (44%) recurrent tumors versus 3 of 40 (8%) locallycontrolled lesions (P � 0.011) suggesting that this may beuseful to identify pleomorphic adenomas that are more likelyto recur after surgery.
From the *Department of Radiation Oncology, University of FloridaCollege of Medicine, Gainesville, FL; †Department of Radiation On-cology, Phoebe Putney Memorial Hospital, Albany, GA; and ‡Depart-ment of Otolaryngology, University of Florida College of Medicine,Gainesville, FL.
Correspondence: William M. Mendenhall, MD, Department of RadiationOncology, University of Florida Health Science Center, 2000 SWArcher Road, PO Box 100385, Gainesville, FL 32610-0385. E-mail:[email protected].
Copyright © 2008 by Lippincott Williams & WilkinsISSN: 0277-3732/08/3101-0095DOI: 10.1097/COC.0b013e3181595ae0
American Journal of Clinical Oncology • Volume 31, Number 1, February 2008 95

DIAGNOSISA history is obtained and a physical examination is
performed, including a thorough head and neck evaluation.Magnetic resonance imaging is obtained to determine thelocation and extent of the lesion and its probable etiology.Fine needle aspiration biopsy is obtained; if negative and it isthought that the lesion is most likely pleomorphic adenomathen the patient undergoes resection with frozen sectionhistopathologic evaluation at the time of the operation.
PATHOLOGYPleomorphic adenomas are composed of neoplastic
myoepithelial cells intermingled with neoplastic ducts andstroma.3 A subset of tumors contain dyplastic cells and/orfoci of malignant cells. Ethunandan et al11 evaluated 100consecutive patients treated with surgery for pleomorphicadenomas at the Queen Alexandra Hospital (Portsmouth,UK) and found 96 to be benign, 1 apparently benign tumorcontained foci of vascular invasion, 1 lesion contained focaldysplasia, and the remaining 2 patients had tumors withintracapsular invasion. All 4 patients remained disease-free at15 months, 28 months, 32 months, and 36 months afterresection, respectively. Ohtake et al4 analyzed 101 patientswith pleomorphic adenoma for cellular atypia, p53 expres-sion, and proliferating cell nuclear antigen expression. His-tologically, 6% had focal cellular atypia and 45% had scat-tered atypical cells with no foci. Overall, cellular atypia wasidentified in 51% of patients with hematoxyllin and eosinstains, 56% of patients with p53 immunohistochemical stains,and 66% of patients with proliferating cell nuclear antigenstains. Cellular atypia identified via p53 positivity increasedwith tumor duration of more than 10 years (P � 0.005) andwas unrelated to tumor size.
Neural adhesion molecule (N-CAM) is a tumor sup-pressor molecule that has been shown to inhibit cell invasionin various malignancies.14 Saleh et al analyzed N-CAMexpression via immunohistochemistry in 4 patients with ple-omorphic adenoma and 4 patients with carcinoma ex-pleo-morphic adenoma and found that the luminal cells stainedstrongly positive for N-CAM in the former compared with thelatter.14 This suggests that downregulation of N-CAM occursas part of the process of malignant transformation that occursin a small subset of patients with pleomorphic adenomas.
�-catenin is a component of the wingless WNT signalingcascade and is associated with invasion and metastases in vari-ous neoplasms.15 It may also play a role in malignant transfor-mation. do Prado et al found �-catenin expression in 10 normalsalivary glands, 16 pleomorphic adenomas, and 3 carcinomasex-pleomorphic adenomas and found that in all cases there wasmembranous and cytoplasmic immunostaining for �-catenin.15
Further, there was loss of cytoplasmic �-catenin expression inpleomorphic adenomas and cytoplasmic accumulation in carci-nomas ex-pleomorphic adenomas. Thus, loss of the �-cateninadhesion molecule occurs during the development of pleomor-phic adenomas, and cytoplasmic accumulation of �-cateninoccurs with malignant transformation.
TREATMENTThe optimal treatment for pleomorphic adenomas is
wide excision with negative margins. The majority arise inthe parotid gland and, for these, the preferred treatment issuperficial parotidectomy or total parotidectomy with facialnerve dissection and preservation.1,2,6,16 Although wide mar-gins are preferred, the majority of parotid pleomorphic ade-nomas abut the main trunk and/or branches of the 7th nerveso that a limited enucleation or capsular dissection is neces-sary in most cases.6 Despite this being the case, local controlrates are normally 95% or higher after optimal surgery alone.The risk of major complications is relatively low after surgeryfor previously untreated pleomorphic adenomas. However,the risk of complications, particularly 7th nerve injury, isincreased after salvage surgery for locally recurrent tumors(Table 1).17
Postoperative radiotherapy (RT) is advised for thesmall subset of patients with positive margins and/or multi-focal recurrences. Although tumor spill and equivocal mar-gins were once indications for postoperative RT at our insti-tution, the likelihood of local control after surgery probablyexceeds 90% and we no longer advise adjuvant RT in thesesituations.6,9,16,18 The occasional patient presenting with aminor salivary pleomorphic adenoma not amenable to grosstotal resection may be treated with RT alone. The dose-fractionation schedules are similar to those used for malig-nancies. Patients with microscopic residual disease receiveeither 66 Gy in 33 once-daily fractions or 69.2 to 74.4 Gy at1.2 Gy per twice-daily fraction. Those with gross diseasereceive either 70 Gy in 35 once-daily fractions or 74.4 Gy in62 twice-daily fractions.
OUTCOMES
SurgeryAlves et al5 reported on 58 patients with submandibular
gland pleomorphic adenomas treated surgically and followedfrom 1 month to 464 months (median, 76 months). Fifty-fourpatients had previously untreated tumors and 4 patients wereoperated for local recurrences. Local control was achieved in57 of 58 patients (98%), including all 4 patients operated forrecurrent tumors. The patient who developed a recurrenceunderwent salvage surgery and was disease-free 8 years afterthe second procedure.
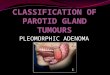
TABLE 1. Facial Nerve Injury After Surgery for ParotidPleomorphic Adenoma at Edinburgh University
7th Nerve InjuryPreviously Untreated
(N � 64 Patients)Locally Recurrent*(N � 19 Patients)
Total 0 (0%) 2 (11%)
Permanent partial 5 (8%) 1 (5%)
Temporary partial 6 (9%) 7 (37%)
None 53 (83%) 9 (47%)
Reprinted with permission from Arch Otolaryngol. 1984;110:167–171.*Includes 16 patients with pleomorphic adenomas and 3 patients with carcinoma
ex-pleomorphic adenoma. Four of 19 patients received postoperative RT.
Mendenhall et al American Journal of Clinical Oncology • Volume 31, Number 1, February 2008
© 2008 Lippincott Williams & Wilkins96

O’Brien1 reported on 355 patients with benign parotidtumors who were treated surgically between 1988 and 2002 atthe Royal Prince Alfred Hospital (Sydney, Australia). Fol-low-up ranged from 1 to 14 years (median, 6 years). Twohundred fifty-four patients (70%) had pleomorphic adeno-mas; surgery consisted of a limited superficial parotidectomyin all previously untreated patients. Local control wasachieved in 252 of 254 patients (99%). Both patients whodeveloped a local recurrence had been operated for a recur-rence after prior surgery and RT elsewhere.
Laccourreye et al7 reported on 229 patients who under-went total parotidectomy with 7th nerve preservation at theUniversity of Paris V between 1966 and 1991 for previouslyuntreated parotid pleomorphic adenomas. Minimum 2-yearfollow-up was available for 221 patients and 100 of 111eligible patients had follow-up at 10 years. No patient re-ceived postoperative RT. Complications included: hemor-rhage, 1.7%; hematoma, 6.1%; seroma, 4.8%; and skin ne-crosis, 0.9%. Temporary 7th nerve paresis and paralysisoccurred in 64.6% and 5.6% of patients, respectively. Per-manent 7th nerve paresis and paralysis occurred in 3.9% and0% of patients, respectively. Recovery of facial nerve func-tion was observed up to 18 months postoperatively. Frey’ssyndrome was observed in 65.9% of patients. The 10-yearlocal control rate was 99.6%.
Myssiorek et al19 reported on 139 patients treatedsurgically for de novo parotid pleomorphic adenomas at theLahey Clinic (Burlington, Massachusetts) and followed from6 to 39 years. Local control was achieved in 138 of 139patients (99%). Twenty-five additional patients were treatedwith surgery alone for locally recurrent pleomorphic adeno-mas and followed for an average of 12 years. Salvage pro-cedures included excision of the incisional scar, 12 patients;superficial parotidectomy, 8 patients; subtotal parotidectomy,3 patients; and total parotidectomy, 2 patients. Ten patients(40%) were locally controlled after the first salvage procedureand 8 additional patients were cured after 1 to 4 moreoperations for an ultimate local control rate of 72%.
Piekarski et al2 reported on 98 patients with parotidpleomorphic adenomas treated with extracapsular dissectionat the University of Lodz (Lodz, Poland) between 1979 and2002. Mean follow-up was 34 months. Seventeen patientsreceived postoperative RT (dose and fractionation unspeci-fied) for capsular rupture (7 patients), close margins (4patients), and capsular exposure (6 patients). Ten patients(10%) developed transient 7th nerve paresis and 8 patients(8%) had permanent facial nerve paresis. Although 90 of 98patients (92%) were locally controlled, the 10-year local
control rate was only 58%. The authors no longer recommendthis procedure for treatment of patients with pleomorphicadenomas. The outcomes of selected surgically treated pa-tients are outlined in Table 2.
RadiotherapyDawson and Orr8 reported on 311 parotid pleomorphic
adenomas treated at the Western General Hospital and RoyalInfirmary between 1950 and 1971 with surgery (usually localexcision) and postoperative RT. Two hundred seventy-ninepatients underwent a single plane radium needle implant andreceived 55 to 60 Gy over 6 days specified 5 mm from theplane of the needles. Twenty-eight patients received externalbeam RT (50–60 Gy in 20–25 fractions over 4–5 weeks) and4 patients received a combination of brachytherapy andexternal beam. Local control was achieved in 301 of 311patients (97%); the 20-year local control rate was 92%. Fourpatients (1%) developed a second malignancy including sar-coma at 14 years, 1 patient; adenocarcinoma at 18 and 30years, 2 patients; and carcinoma ex-pleomorphic adenoma at18 years, 1 patient.
Ravasz et al20 reported on 78 patients treated at theUniversity of Utrecht (Utrecht, The Netherlands) with sur-gery and postoperative RT for previously untreated (62 pa-tients) or locally recurrent (16 patients) parotid pleomorphicadenomas. Indications for postoperative RT in the 62 previ-ously untreated patients included enucleation, 36 patients;tumor spill, 7 patients; and positive margins after superficialor total parotidectomy, 19 patients. RT was administered withexternal beam to 50 Gy in 25 fractions followed by a 10 to 16Gy boost for nonradical excisions and 20 to 25 Gy boost forgross residual disease. Minimum follow-up was 6 years(median, 11 years). Local control rates were: previouslyuntreated, 62 of 62 patients (100%); locally recurrent, 15 of16 patients (94%); and overall, 77 of 78 patients (99%). Nopatient experienced a severe complication. Barton et al21
reported on 187 patients treated with surgery and postopera-tive RT for parotid pleomorphic adenoma at the ChristieHospital (Manchester, UK) and followed for a median of 14years. One hundred fifteen patients had previously untreatedtumors and 72 patients were treated for locally recurrentlesions. Indications for postoperative RT included incompleteexcision and tumor spill. RT was administered either withexternal beam (50 Gy in 15–16 fractions with a wedge pairtechnique) or interstitial brachytherapy (60 Gy at 5 mm froma single plane radium or cesium needle implant). Localcontrol rates were: previously untreated, 114 of 115 patients(99%); locally recurrent, 63 of 72 patients (88%); and overall,
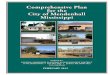
TABLE 2. Outcomes After Surgery Alone for Pleomorphic Adenoma
SeriesNo.
Patients SiteDe Novo/Locally
Recurrent Follow-up Local Control
Alves et al5 58 Submandibular gland 54/4 Median, 76 mo; range, 1–464 mo 57/58 (98%)
Laccourreye et al7 229 Parotid 229/0 — 99.6% at 10 yr
O’Brien et al1 254 Parotid — Median, 6 yr; range, 1–14 yr 252/254 (99%)
Myssiorek et al19 139 Parotid 139/0 6–39 yr 138/139 (99%)
25 Parotid 0/25 Mean, 12 yr 18/25 (72%)
American Journal of Clinical Oncology • Volume 31, Number 1, February 2008 Salivary Gland Pleomorphic Adenoma
© 2008 Lippincott Williams & Wilkins 97

177 of 187 patients (95%). Complications in patients treatedfor de novo tumors included 2 necroses (1 major; 1 minor), 1permanent 7th nerve injury, 1 salivary fistula, and 1 Frey’ssyndrome. Complications in patients treated for a local re-currence included 2 necroses (1 major; 1 minor), 4 facialnerve palsies, and 16 Frey’s syndrome. One patient devel-oped malignant transformation.
Liu et al22 reported on 55 patients with parotid pleo-morphic adenoma treated with surgery and postoperative RTbetween 1970 and 1987 at the Princess Margaret Hospital(Toronto, Canada). Indications for postoperative RT includedlocal recurrence, 29 patients; microscopic residual disease, 14patients; gross residual disease, 11 patients; nerve involve-ment, 11 patients; tumor spill, 8 patients; multifocality, 6patients; and/or miscellaneous, 5 patients. The median dose-fractionation schedule was 45 Gy in 20 fractions (range, 27.5Gy/11 fractions to 60 Gy/30 fractions). The median follow-upwas 12.5 years (range, 0.1–39.7 years). The 10-year localcontrol rates were 93% for previously untreated patients (N �31) compared with 82% for those treated for a local recur-rence (N � 24) with a significance level of P � 0.08. Patientstreated with RT for gross disease had a 62% 10-year localcontrol rate compared with 93% for those without grossresidual disease (P � 0.0005). One patient developed anosteoradionecrosis that healed spontaneously. No second ma-lignancies were observed.
Chen et al23 reported on 34 patients treated between1960 and 2004 at the University of California, San Franciscofor recurrent parotid pleomorphic adenoma. Thirty patientsunderwent a gross total resection and 4 patients underwent asubtotal excision. Tumor was multifocal in 16 of 34 patients(47%). The median RT dose was 50 Gy (range, 45–60 Gy).Follow-up ranged from 2.3 to 28.9 years (median, 17.4years). The 20-year local control rate was 94%. One patientdeveloped a second primary low-grade mucoepidermoid car-cinoma and underwent salvage surgery and is disease-free 3years postoperatively. Samson et al24 reported on 21 patientswith locally recurrent parotid pleomorphic adenoma treatedwith facial nerve preservation surgery and postoperative RTat the Massachusetts General Hospital (Boston, MA) between1979 and 1988. Eight patients were treated twice-daily and 13received once-daily fractionation. The mean dose was 50.5Gy (range, 50–67 Gy). Follow-up ranged from 2 to 11 years(mean, 5.9 years). No patient was lost to follow-up. Compli-
cations included 2 transient and 1 permanent 7th nerveinjuries. The local control rates were: microscopic residual,16 of 17 patients (94%); gross residual, 1 of 4 patients (25%);and overall, 17 of 21 patients (81%). Hodge et al9 reported on17 patients treated at the University of Florida with RT alone(2 patients) or combined with surgery (15 patients) between1970 and 2000. Fourteen patients were treated once-daily(median, 65 Gy; range, 56.6–70 Gy) and 3 patients weretreated twice-daily (median, 74.4 Gy; range, 62.9–74.4 Gy).Seven patients had previously untreated tumors and the re-mainder were locally recurrent after 1 or more prior opera-tions. Follow-up ranged from 1.8 to 27.1 year (median, 9.6years). Local control rates were: subclinical disease, 8 of 10patients (80%); gross residual disease, 3 of 7 patients (43%);and overall, 11 of 17 patients (65%). The 10-year localcontrol rate for all 17 patients was 61%. One patient died dueto locally recurrent pleomorphic adenoma and 1 patient dieddue to carcinoma ex-pleomorphic adenoma. No patient de-veloped a severe complication due to RT.
Douglas et al25 reported on 16 patients with recurrentand/or unresectable pleomorphic adenoma treated between1986 and 1993 with neutron RT at the University of Wash-ington (Seattle, WA). Indications for RT included grossresidual disease, 10 patients; indeterminate margins, 2 pa-tients; and/or multinodular recurrence, 9 patients. The mediandose was 18.9 neutron Gy (range, 17–22 neutron Gy). Fol-low-up ranged from 9 to 168 months (median, 83 months).Two patients were lost to follow-up at 30 and 97 months.Fourteen of 16 patients (88%) were locally controlled; the15-year local control rate was 85%. One patient died of askull base local recurrence. One patient developed mandibu-lar osteoradionecrosis. The outcomes of selected series ofpatients treated with surgery and RT are outlined in Table 3.
CONCLUSIONSThe optimal treatment for pleomorphic adenoma is
resection. The local control rate after optional surgery ex-ceeds 95%. Adjuvant RT improves the likelihood of localcontrol in the subset of patients with inadequate marginsand/or multinodular recurrence. Optimal dose-fractionationschedules are similar to those employed for salivary glandcarcinomas.
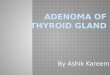
TABLE 3. Outcomes After Surgery and Radiotherapy for Pleomorphic Adenoma
Series No. PatientsDe Novo/Locally
Recurrent Follow-up Local Control
Dawson and Orr8 311 — Minimum, 10 yr 92% at 20 yr
Ravasz et al20 78 62/16 Median, 11 yr; minimum, 6 yr 77/78 (99%)
Barton et al21 187 115/72 Median, 14 yr 177/187 (95%)
Chen et al23 34 0/34 Median, 17.4 yr; range, 2.3–28.9 yr 94% at 20 yr
Samson et al24 21 0/21 Mean, 5.9 yr; range, 2–11 yr 17/21 (81%)
Hodge et al9 17* 7/10 Median, 9.6 yr; range, 1.8–27.1 yr 61% at 10 yr
Douglas et al25† 16 — Median, 83 mo; range, 9–168 mo 85% at 15 yr
*Surgery and postoperative RT, 15 patients; RT alone, 2 patients.†Neutron radiotherapy.
Mendenhall et al American Journal of Clinical Oncology • Volume 31, Number 1, February 2008
© 2008 Lippincott Williams & Wilkins98

REFERENCES1. O’Brien CJ. Current management of benign parotid tumors—the role of
limited superficial parotidectomy. Head Neck. 2003;25:946–952.2. Piekarski J, Nejc D, Szymczak W, et al. Results of extracapsular
dissection of pleomorphic adenoma of parotid gland. J Oral MaxillofacSurg. 2004;62:1198–1202.
3. Lourenco SV, Kapas S, Williams DM, et al. Expression patterns ofintegrins on pleomorphic adenoma and adenoid cystic carcinoma: studyon specimens and in vitro investigation of the effects of extracellularmatrix on the expression of these adhesion molecules. J Oral PatholMed. 2004;33:574–580.
4. Ohtake S, Cheng J, Ida H, et al. Precancerous foci in pleomorphicadenoma of the salivary gland: recognition of focal carcinoma andatypical tumor cells by P53 immunohistochemistry. J Oral Pathol Med.2002;31:590–597.
5. Alves FA, Perez DE, Almeida OP, et al. Pleomorphic adenoma of thesubmandibular gland: clinicopathological and immunohistochemicalfeatures of 60 cases in Brazil. Arch Otolaryngol Head Neck Surg.2002;128:1400–1403.
6. Donovan DT, Conley JJ. Capsular significance in parotid tumor surgery:reality and myths of lateral lobectomy. Laryngoscope. 1984;94:324–329.
7. Laccourreye H, Laccourreye O, Cauchois R, et al. Total conservativeparotidectomy for primary benign pleomorphic adenoma of the parotidgland: a 25-year experience with 229 patients. Laryngoscope. 1994;104:1487–1494.
8. Dawson AK, Orr JA. Long-term results of local excision and radiother-apy in pleomorphic adenoma of the parotid. Int J Radiat Oncol BiolPhys. 1985;11:451–455.
9. Hodge CW, Morris CG, Werning JW, et al. Role of radiotherapy forpleomorphic adenoma. Am J Clin Oncol. 2005;28:148–151.
10. Blevins NH, Jackler RK, Kaplan MJ, et al. Facial paralysis due to benignparotid tumors. Arch Otolaryngol Head Neck Surg. 1992;118:427–430.
11. Ethunandan M, Witton R, Hoffman G, et al. Atypical features inpleomorphic adenoma—a clinicopathologic study and implications formanagement. Int J Oral Maxillofac Surg. 2006;35:608–612.
12. Nouraei SA, Ferguson MS, Clarke PM, et al. Metastasizing pleomorphicsalivary adenoma. Arch Otolaryngol Head Neck Surg. 2006;132:788–793.
13. Hamada T, Matsukita S, Goto M, et al. Mucin expression in pleomorphicadenoma of salivary gland: a potential role for MUC1 as a marker topredict recurrence. J Clin Pathol. 2004;57:813–821.
14. Saleh ER, Franca CM, Marques MM. Neural adhesion molecule(N-CAM) in pleomorphic adenoma and carcinoma ex-pleomorphicadenoma. J Oral Pathol Med. 2003;32:562–567.
15. do Prado RF, Consolaro A, Taveira LA. Expression of betacatenin incarcinoma in pleomorphic adenoma, pleomorphic adenoma and normalsalivary gland: an immunohistochemical study. Med Oral Patol Oral CirBucal. 2006;11:E247–E251.
16. Natvig K, Soberg R. Relationship of intraoperative rupture of pleomor-phic adenomas to recurrence: an 11–25 year follow-up study. HeadNeck. 1994;16:213–217.
17. Maran AG, Mackenzie IJ, Stanley RE. Recurrent pleomorphic adenomasof the parotid gland. Arch Otolaryngol. 1984;110:167–171.
18. Buchman C, Stringer SP, Mendenhall WM, et al. Pleomorphic adenoma:effect of tumor spill and inadequate resection on tumor recurrence.Laryngoscope. 1994;104:1231–1234.
19. Myssiorek D, Ruah CB, Hybels RL. Recurrent pleomorphic adenomasof the parotid gland. Head Neck. 1990;12:332–336.
20. Ravasz LA, Terhaard CH, Hordijk GJ. Radiotherapy in epithelial tumorsof the parotid gland: case presentation and literature review. Int J RadiatOncol Biol Phys. 1990;19:55–59.
21. Barton J, Slevin NJ, Gleave EN. Radiotherapy for pleomorphic adenomaof the parotid gland. Int J Radiat Oncol Biol Phys. 1992;22:925–928.
22. Liu FF, Rotstein L, Davison AJ, et al. Benign parotid adenomas: areview of the Princess Margaret Hospital experience. Head Neck. 1995;17:177–183.
23. Chen AM, Garcia J, Bucci MK, et al. Recurrent pleomorphic adenomaof the parotid gland: long-term outcome of patients treated with radiationtherapy. Int J Radiat Oncol Biol Phys. 2006;66:1031–1035.
24. Samson MJ, Metson R, Wang CC, et al. Preservation of the facial nervein the management of recurrent pleomorphic adenoma. Laryngoscope.1991;101:1060–1062.
25. Douglas JG, Einck J, Austin-Seymour M, et al. Neutron radiotherapy forrecurrent pleomorphic adenomas of major salivary glands. Head Neck.2001;23:1037–1042.
American Journal of Clinical Oncology • Volume 31, Number 1, February 2008 Salivary Gland Pleomorphic Adenoma
© 2008 Lippincott Williams & Wilkins 99