ADENOIDECTOMY AND TONSILLECTOMY Dr Joel G Mathew Slide 2
ADENOIDECTOMY Slide 3 ADENOIDECTOMY - INDICATIONS Adenoid
hypertrophy causing: Adenoid hypertrophy causing: Otitis media with
effusion (SOM) Otitis media with effusion (SOM) Upper airway
obstruction and obstructive sleep apnoea Upper airway obstruction
and obstructive sleep apnoea Recurrent acute otitis media Recurrent
acute otitis media Recurrent rhinosinusitis (Abolishing infective
episodes) Recurrent rhinosinusitis (Abolishing infective episodes)
Slide 4 ADENOIDECTOMY - CONTRAINDICATIONS Acute upper respiratory
infections Acute upper respiratory infections Acute epidemic of
Poliomyelitis- >Paralytic polio (Exposed nerves) Acute epidemic
of Poliomyelitis- >Paralytic polio (Exposed nerves) Bleeding
disorders and Anaemia Bleeding disorders and Anaemia Cleft Palate
Cleft Palate Overt cleft palate Overt cleft palate Slide 5
SUBMUCOUS CLEFT PALATE (COVERT) Abnormal nasal speech, Abnormal
nasal speech, Bifid uvula Bifid uvula Thin strip of mucosa in the
middle of roof of mouth Thin strip of mucosa in the middle of roof
of mouth Notch at the back of hard palate. Notch at the back of
hard palate. Slide 6 ADENOIDECTOMY - PROCEDURE Anaesthesia General
Anaesthesia Anaesthesia General Anaesthesia If combined,
Adenoidectomy before Tonsillectomy If combined, Adenoidectomy
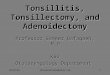
before Tonsillectomy Slide 7 POSITION ROSES POSITION Supine with
head extended by placing a pillow or sandbag beneath the shoulders.
Advantage Larynx lies at a higher level than oral cavity no risk of
aspiration. Excellent exposure Both hands of surgeon are free.
Hyperextension is avoided Makes cervical vertebral bodies
prominent-Damage to ligaments or cartilages of vertebral spine or
bodies -> Grisels syndrome Slide 8 GRISELS SYNDROME Non
traumatic subluxation of atlanto axial joint Non traumatic
subluxation of atlanto axial joint Results from any condition that
results in hyperaemia and pathological relaxation of the transverse
ligament of the atlanto-axial joint. Results from any condition
that results in hyperaemia and pathological relaxation of the
transverse ligament of the atlanto-axial joint. Due to infection in
the periodontoid vascular plexus that drains the
region->paraspinal ligament laxity. Due to infection in the
periodontoid vascular plexus that drains the region->paraspinal
ligament laxity. Presents with persistent neck pain and torticollis
1-2 weeks following surgery. Presents with persistent neck pain and
torticollis 1-2 weeks following surgery. More common in Downs
syndrome patients More common in Downs syndrome patients X-ray and
CT of Cervical spine confirms diagnosis. X-ray and CT of Cervical
spine confirms diagnosis. Treatment: Cervical immobilisation,
analgesics and antibiotics. Arthrodesis in intractable cases
Treatment: Cervical immobilisation, analgesics and antibiotics.
Arthrodesis in intractable cases Slide 9 TECHNIQUE OF ADENOIDECTOMY
The surgeon stands behind the patient. The surgeon stands behind
the patient. Boyle-Davis mouth gag is inserted, opened and held in
place by Draffins bipod stand Boyle-Davis mouth gag is inserted,
opened and held in place by Draffins bipod stand Palate is palpated
to exclude a submucous cleft palate. Palate is palpated to exclude
a submucous cleft palate. The soft palate is retracted by a suction
catheter introduced through the nose, and pulled out of the oral
cavity. The soft palate is retracted by a suction catheter
introduced through the nose, and pulled out of the oral cavity. The
adenoid is palpated with a finger. The adenoid is palpated with a
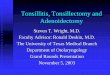
finger. Slide 10 St Clair Thomson adenoid curette with guard is
introduced into the nasopharynx above the upper end of adenoid
tissue, held like a dagger St Clair Thomson adenoid curette with
guard is introduced into the nasopharynx above the upper end of
adenoid tissue, held like a dagger With a downward and forward
sweeping movement, adenoids are shaved off. With a downward and
forward sweeping movement, adenoids are shaved off. A smaller sized
curette is used to curette the adenoids around the choana and the
Eustachian cushions A smaller sized curette is used to curette the
adenoids around the choana and the Eustachian cushions Nasopharynx
is packed with gauze packs for a few minutes for haemostasis.
Nasopharynx is packed with gauze packs for a few minutes for
haemostasis. Slide 11 OTHER TECHNIQUES OF ADENOIDECTOMY Suction
coagulator/diathermy Suction coagulator/diathermy Endoscopic
transnasal or transpalatal adenoidectomy with microdebrider
Endoscopic transnasal or transpalatal adenoidectomy with
microdebrider Coblator plasma field device Coblator plasma field
device Slide 12 POSTOPERATIVE CARE The patient is kept in lateral
position The patient is kept in lateral position Kept nil orally
until fully recovered from GA (4-6 hours). Kept nil orally until
fully recovered from GA (4-6 hours). Monitor vitals Monitor vitals
Watch for bleeding: Earliest sign-Frequent swallowing Watch for
bleeding: Earliest sign-Frequent swallowing Oral antibiotics and
analgesics Oral antibiotics and analgesics Slide 13 COMPLICATIONS
Haemorrhage ( < 0.7%) Managed by postnasal packing. Haemorrhage
( < 0.7%) Managed by postnasal packing. Surgical trauma:
Surgical trauma: Teeth Teeth Soft palate Soft palate Uvula Uvula
Eustachian cushions-stenosis, secretory otitis media Eustachian
cushions-stenosis, secretory otitis media Cervical
spine-atlantoaxial dislocation Cervical spine-atlantoaxial
dislocation Velopharyngeal insufficiency Velopharyngeal
insufficiency Hypernasal speech, swallowing difficulty and rarely
nasal regurgitation Hypernasal speech, swallowing difficulty and
rarely nasal regurgitation Adenoid remnant (Upto 29%) Adenoid
remnant (Upto 29%) Pulmonary complications-Aspiration, Coroners
clot Pulmonary complications-Aspiration, Coroners clot Infection of
Nasopharynx. Infection of Nasopharynx. Slide 14 TONSILLECTOMY Slide
15 TONSILLECTOMY-INDICATIONS Absolute Indications: Obstructive
symptoms and Obstructive sleep apnoea Malignancy or suspected
malignancy Recurrent peritonsillar abscess Tonsillitis causing
febrile seizures in children Relative Indications: Recurrent
tonsillitis: >= 7 episodes in 1 year >=4 episodes per year
for 2 consecutive years >= 3 episodes per year for 3 consecutive
years Halitosis due to chronic tonsillitis Tonsilloliths Tonsillar
cysts Dental and orofacial abnormalities Dipheria carriers
Rheumatic fever and Acute glomerulonephritis Slide 16 TONSILLECTOMY
AS PART OF ANOTHER PROCEDURE Excision of elongated styloid process
(Eagle syndrome) Nagging throat pain and a palpatory finding in the
tonsillar fossa. Confirmed by palpation and injection of
anaesthetic. Excision of elongated styloid process (Eagle syndrome)
Nagging throat pain and a palpatory finding in the tonsillar fossa.
Confirmed by palpation and injection of anaesthetic.
Glossopharyngeal neuralgia Glossopharyngeal neuralgia UPPP
(Uvulopalatopharyngoplasty)or LAUP (Laser-assisted
uvulopalatoplasty) or CAUP (Coblation assisted uvulopalatoplasty)
UPPP (Uvulopalatopharyngoplasty)or LAUP (Laser-assisted
uvulopalatoplasty) or CAUP (Coblation assisted uvulopalatoplasty)
Slide 17 CONTRAINDICATIONS Bleeding disorders Bleeding disorders
Cleft palate or submucous cleft palate Cleft palate or submucous
cleft palate Velopharyngeal insufficiency Velopharyngeal
insufficiency Acute infection Acute infection Uncontrolled systemic
disease Uncontrolled systemic disease Anaemia Anaemia Extremes of
age Extremes of age Slide 18 PROCEDURE Anaesthesia: General
anaesthesia Anaesthesia: General anaesthesia Position-Roses
position-supine with head extended by placing a pillow or sandbag
under the shoulder Position-Roses position-supine with head
extended by placing a pillow or sandbag under the shoulder
Operative techniques Operative techniques DISSECTION AND SNARING
-> Classical DISSECTION AND SNARING -> Classical Diathermy
Diathermy Coblation tonsillectomy Coblation tonsillectomy
Ultrasonic dissection Ultrasonic dissection Laser tonsillectomy
Laser tonsillectomy Capsulotomy techniques Capsulotomy techniques
Guillotine method (Ancient) Guillotine method (Ancient) Slide 19
DISSECTION AND SNARE METHOD Boyle Davis mouth gag is inserted,
opened and held in position with Draffins bipod stand Boyle Davis
mouth gag is inserted, opened and held in position with Draffins
bipod stand Upper pole of tonsil is held with tonsil holding
forceps and pulled medially Upper pole of tonsil is held with
tonsil holding forceps and pulled medially Mucosa is incised with
blunt scissors, knife, forceps or diathermy at the point where it
reflects from tonsil to anterior pillar. Incision is continued
inferiorly towards base of tongue. Mucosa is incised with blunt
scissors, knife, forceps or diathermy at the point where it
reflects from tonsil to anterior pillar. Incision is continued
inferiorly towards base of tongue. The tonsil is separated from its
bed by blunt dissection, upto the lower pole The tonsil is
separated from its bed by blunt dissection, upto the lower pole The
plane of dissection is the loose areolar tissue separating tonsil
from its bed. The plane of dissection is the loose areolar tissue
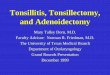
separating tonsil from its bed. Slide 20 Once lower pole is
reached, a tonsillar snare is passed over the tonsil holding
forceps, placed over the tonsil, threaded down to the lower pole,
tightened to crush the pedicle, and the tonsil is removed Once
lower pole is reached, a tonsillar snare is passed over the tonsil
holding forceps, placed over the tonsil, threaded down to the lower
pole, tightened to crush the pedicle, and the tonsil is removed
Gauze packs are kept in the tonsillar fossa Gauze packs are kept in
the tonsillar fossa Bleeding points are looked for, and bleeding
arrested with non absorbable sutures Bleeding points are looked
for, and bleeding arrested with non absorbable sutures Slide 21
Slide 22 POSTOPERATIVE CARE Patient is nursed in the lateral
position Patient is nursed in the lateral position Kept nil orally
until fully recovered from GA (4-6 hours). Kept nil orally until
fully recovered from GA (4-6 hours). Monitor vitals Monitor vitals
Watch for bleeding: Earliest sign-Frequent swallowing Watch for
bleeding: Earliest sign-Frequent swallowing Ice cold fluids and ice
cream given on the first day Ice cold fluids and ice cream given on
the first day Oral antibiotics and analgesics Oral antibiotics and
analgesics Slide 23 COMPLICATIONS OF TONSILLECTOMY HEMORRHAGE
HEMORRHAGE Primary Primary During the surgery During the surgery
Controlled by pressure packing, ligation, cauterisation Controlled
by pressure packing, ligation, cauterisation Slide 24 Reactionary
Reactionary Within 24 hours of surgery Within 24 hours of surgery
CAUSES OF REACTIONARY HEMORRHAGE (VIVA): CAUSES OF REACTIONARY
HEMORRHAGE (VIVA): 1.Formation of a blood clot or Dislodgement of
blood clot from lumen 2.Vasodilation of blood vessel
3.Postoperative rise in blood pressure 4.Increased venous pressure
by coughing or retching 5.Slipping of ligature Slide 25 Management
of Reactionary haemorrhage: Management of Reactionary haemorrhage:
Blood is cross matched Blood is cross matched Tonsillar fossa is
inspected and clot removed Tonsillar fossa is inspected and clot
removed Pressure with a swab soaked in 1:1000 Adrenaline Pressure
with a swab soaked in 1:1000 Adrenaline Administration of
hemostatic agents (Ethamsylate, Tranexamic acid) Administration of
hemostatic agents (Ethamsylate, Tranexamic acid) May require taking
to the operation theatre and ligation under General Anaesthesia.
May require taking to the operation theatre and ligation under
General Anaesthesia. Slide 26 Most dangerous form of haemorrhage
because: Most dangerous form of haemorrhage because: It may be
missed (Patient may still be under the effect of GA) It may be
missed (Patient may still be under the effect of GA) It may cause
fatal aspiration It may cause fatal aspiration Large hemorrhages
may require ligation or electrocoagulation under GA. Two GAs at a
short interval is dangerous. Large hemorrhages may require ligation
or electrocoagulation under GA. Two GAs at a short interval is
dangerous. Secondary haemorrhage (>24 hours 2 weeks) Secondary
haemorrhage (>24 hours 2 weeks) Cause: Infection of the
granulating tonsillar bed Cause: Infection of the granulating
tonsillar bed Treated with Antibiotics Treated with Antibiotics
Slide 27 OTHER COMPLICATIONS OF TONSILLECTOMY: OTHER COMPLICATIONS
OF TONSILLECTOMY: Injury to: Injury to: Temporo-mandibular joint
Temporo-mandibular joint Lips and commisures of mouth Lips and
commisures of mouth Tongue, uvula, soft palate Tongue, uvula, soft
palate Very rarely Glossopharyngeal nerve, pharyngeal venous
plexus, carotid sheath Very rarely Glossopharyngeal nerve,
pharyngeal venous plexus, carotid sheath Grisel syndrome (Non
traumatic atlanto axial dislocation) Grisel syndrome (Non traumatic
atlanto axial dislocation) Aspiration of blood-> Pneumonia,
collapse of lung, or lung abscess Aspiration of blood->
Pneumonia, collapse of lung, or lung abscess Slide 28 Hematoma and
oedema of uvula Hematoma and oedema of uvula Referred earache
Referred earache Velopharyngeal insufficiency Velopharyngeal
insufficiency Tonsillar remnants Tonsillar remnants