Embed Size (px)
Citation preview

CentralBringing Excellence in Open Access
JSM Surgical Oncology and Research
Cite this article: Senger JL, Kanthan R (2016) Adenoid Cystic Carcinoma of the Breast A Focused Review. JSM Surg Oncol Res 1(2): 1008.
*Corresponding authorJenna-Lynn Senger, 5005C Katz Group Centre University of Alberta Edmonton, Alberta, Canada T6G-2E1, Canada; Email:
Submitted: 31 August 2016
Accepted: 07 December 2016
Published: 07 December 2016
ISSN: 2578-3688
Copyright© 2016 Kanthan et al.
OPEN ACCESS
Keywords•Adenoid cystic carcinoma• Breast carcinoma•Malignant epithelial tumor
Review Article
Adenoid Cystic Carcinoma of the Breast A Focused ReviewJenna-Lynn Senger1 and Rani Kanthan2*1Division of Plastic Surgery, University of Alberta, Canada2Department of Pathology & Laboratory Medicine, University of Saskatchewan, Canada
Abstract
Adenoid cystic carcinoma is the most common epithelial malignancy of the minor salivary glands, where it follows an aggressive course with a strong predilection for metastases; by contrast, breast adenoid cystic carcinoma (bACC) represents only 0.1% of breast malignancies and has an indolent natural history with metastases occurring as an uncommon event. Identification of bACC is challenging, as patient risk factors, clinical presentation, and imaging features on ultrasound and MRI are similar to other breast malignancies. Histopathological evaluation is, therefore, critical to the accurate diagnosis of bACC. Additionally, despite being a triple negative hormonal breast cancer, bACC is relatively indolent with excellent overall survivorship; however, delayed metastases are reported up to ten years following initial diagnosis and therefore long-term surveillance is strongly recommended.
This manuscript provides an overall Focused Review on the epidemiology, clinical features, diagnostic workup, pathogenesis, treatment and prognostic/predictive factors of bACC as currently available in the published literature.
INTRODUCTIONAdenoid cystic carcinoma (ACC) is the most common
malignant epithelial tumor of the minor salivary glands and is characterized by the presence of a dual population of both epithelial/luminal and myoepithelial/basaloid (abluminal) cell proliferation [1]. ACC is infrequently detected outside of the salivary glands in locations including the uterine cervix, Bartholin’s glands, lacrimal glands, auditory canal, skin, upper respiratory tract and lung, kidney, esophagus, prostate, and breast [2,3].Within the breast ACC is rare, representing less than 0.1% of carcinoma[4]. Cleverly termed the “Dr Jekyll and Mr Hyde of exocrine gland carcinomas” [3], the same tumor that has an aggressive course when located in the salivary gland with a predilection for metastases behaves indolently in the breast, with rare involvement of the lymph node and infrequent metastases.
Epidemiology
Breast ACC (bACC) is rare, with an incidence of ~1/1 million female-years, a rate that has remained stable since the 1980s despite increases in mammogram screening [4]. Like other breast tumors, bACC occur in at any age; however, they have predominance in the fifth and sixth decades of life [4]. These tumors show a racial predilection towards Caucasians (82%) [5] and though they are most often seen in women, rarely this tumor has also been reported in the male breast [6].
Clinical Features
Patients with bACC typically present with a well-
circumscribed palpable breast mass, often associated with pain and nipple retraction [4]. Whereas pain in salivary gland ACC is due to perineural invasion, the latter is not typically a feature of bACC and thus the mechanism underlying this discomfort is not fully understood though it is often attributed to myoepithelial contraction [3]. These tumors display no preferential laterality or quadrantlocalization within the breast [7], rather, tumors are usually located periareolarly. Lesions normally measure 2-3cm and are unifocal in nature; however, tumors as large as 15cm are described, with others reporting multifocality [4,8]. These lesions are usually slow-growing, over the course of months to years without evidence of extra-mammary spread [9]. The majority of patients present with localized breast disease (~92%) [5].Compared to invasive ductal carcinoma, women with bACC tend to present with a larger tumor size, yet, have a lower incidence of axillary lymphadenopathy [10].
Diagnostic workup
Imaging Features: Imaging features are non-specific and bACC may be easily mistaken for other malignant or benign lesions.
Mammogram shows a lobulated mass that may or may not have sharp margins [8]. These circumscribed nodules are most commonly located in the outer quadrants of the breast of the periareolar region [10]. These lesions may appear benign, with a smooth surface and micro calcifications are rare [4,10]. Dense breast tissue may preclude accurate visualization of these tumors.

CentralBringing Excellence in Open Access
Kanthan et al. (2016)Email:
JSM Surg Oncol Res 1(2): 1008 (2016) 2/7
Ultrasound demonstrates a hypoechoic solid or heterogeneous mass with irregular margins that on Doppler examination displays minimal vascularity [4,8,11]. Posterior acoustic enhancement with shadowing has been described [8]. Magnetic Resonance Imaging (MRI) characteristics of bACC remain controversial in the literature; however, they can be useful when dense breast tissue precludes other imaging techniques [8]. Whereas some authors have described a round/oval lesion with rapid enhancement and no washout, others depict irregularly shaped masses with spiculated margins [11]. Tang et al showed a high T2WI signal with hypointense internal septations for large lesions and iso intense enhancement for smaller lesions [11].
The use of 18F FDG-PET scanning in bACC is similarly controversial, with some studies reporting no significant uptake, potentially as the tumor was only 8mm, whereas others have reported positive uptake [12].
Pathological Features: On gross exam, tumors measure a mean of 3.0cm (0.7-12.0cm) and appear as well-circumscribed pink/tan/gray lesions with microcysts [7]. Histopathological evaluation is central to the accurate diagnosis of bACC. As its definition suggests, bACC are characterized by a biphasic pattern of ‘luminal ’epithelial cells lining glands and ‘abluminal’ ‘basaloid’ myoepithelial cells around pseudocystic spaces [4].Epithelial cells have an eosinophilic cytoplasm with a round nucleus, whereas myoepithelial-like cells have a basophilic cytoplasm with an oval nucleus [13,7]. Myoepithelial cells form pseudolumina resulting from intraluminal stromal invagination [7]. On hematoxylin & eosin staining, tumor cells have a vesicular nucleus without prominent nucleoli, with low mitotic activity and no atypia [14,15]. These tumors show three prominent architectural patterns: cribriform, tubular/trabecular, and solid [4]. The cribriform pattern is composed of variably-sized islands of neoplastic cells forming true glandular spaces and pseudolumens that are filled with periodic acid Schiff (PAS)-positive mucins or acidic ‘stromal’ and ‘mucin’ respectively [3,16]. The tubular pattern is composed of elongated tubules lined by epithelial cells surrounded by a single layer of basaloid cells and the lumens may or may not contain secretions. The characteristics of the trabecular pattern are cells forming small nests, while the basaloid patterns are sheets of closely-packed basaloid cells with few true glandular spaces [3]. Based on these architectural patterns, grading of bACC is similar to ACC of the salivary gland, with tumors classified into three grades. Grade I tumors are those with a cribriform or tubular/trabecular architecture; Grade II tumors have < 30% solid growth, and Grade III have >30% solid growth [7]. Higher-grade tumors tend to be larger and behave more aggressively [7]. A‘solid basaloid pattern’confers the worse prognosis of bACCs [4]. In this context, therefore it has been suggested that solid basaloid-type bACC perhaps should be considered not as a variant but a separate entity from bACC [17]. Solid basaloid bACCs are composed almost entirely of large pleomorphic tumor cells in sheets and cordscontaining Hyperchromatic nuclei and scant cytoplasm, with moderate to marked atypia [14,16]. They can exist as an independent tumor phenotype, or in association with trabecular, tubular, and/or cribriform areas [17]. In contrast to salivary gland ACC, perineural invasion is very rare in most bACC [4]; however, it is more commonly found in the solid basaloid phenotype [16].
Additionally, unlike the other subtypes of bACC the tumor cells of this phenotype are non-reactive to smooth-muscle myosin and S-100 on immunohistochemistry [17].
Foschini recently (2016) proposed a three tier grading system for bACC based on histopathological features: Grade 1) typical ACC with tubular/cribriform features, good prognosis and rare post-management recurrences and/or metastases Grade 2) Basaloid bACC where recurrences and metastases can occur with a good long-term prognosis, and Grade 3) ACC with overtly malignant transformation that give rise to distant metastases and ultimately death [16]. On immunohistochemistry, the luminal epithelioid cells are positive for cytokeratin-7, epithelial membrane antigen (EMA), carcinoembryonic antigen (CEA) and c-kit (CD117) whereas the abluminal basaloid cells express vimentin, CD109, epidermal growth factor (EGFR), myoepithelial markers (p63, actin, calponin, S-100) and a variety of basal cytokeratins (CK5, CK6, CK14, CK17) [14]. CK-7 and EMA are the most specific markers for luminal cells and type IV collagen and vimentin are the most specific for abluminal cells [18]. Unlike the native breast where CD117 is specific for luminal epithelial cells, in bACC there is equal expression in the myoepithelial cells [18]. Similarly, myoepithelial markers CD10 and S100 are nonspecific in bACC. The paradoxical /reverse staining of CK5/6 in the inner epithelial cells rather than the myoepithelial cells, a feature also recognized in adenomyoepithelioma is a distinctive unique feature[18].Additionally, typically, bACC is a triple negative tumor with both cell types being negative for estrogen receptor, progesterone receptor and Her2-neuprotein. Based on this immunoprofile, bACC has often been accurately diagnosed by FNAC using immunohistochemical staining [9]. This immunohistochemical pattern may, however, not be strictly adhered in the solid basaloid variant of bACC. It has been suggested that the solid basaloid cells may be ‘primitive’ cells with the capacity for multidirectional differentiation [14].
Differential Diagnosis: The tubular-cribriform pattern of bACC is challenging to differentiate from the more common cribriform and tubular carcinomas based on histopathological architecture, particularly in small biopsy specimens. These lesions are composed of hyper-proliferation of a single type of neoplastic cells as opposed to the two cell types involved in bACC [7]. Extracellular meta chromatic globules and the presence of a myoepithelial population point towards bACC [9]. Immunohistochemistry may be required for distinction. Unlike bACC, cribriform carcinoma tumor cells are hormone receptor-positive and high molecular weight cytokeratin negative [18].cKit expression is suggested to be the most reliable diagnostic adjunct for making this differentiation, with ~95% of bACCs showing expression in the ductal luminal component but no expression in tubular/cribriform carcinoma [17]. Additionally, immunoreactivity for p63 is found in the majority of bACCs but is absent in tubular and cribriform carcinoma while E-cadherin is over expressed in all three breast pathologies [17]. While adenoepithelioma has a reverse staining pattern for CK5/6 as well as CK14, the latter does not hold true for bACC. It is suggested that this aberrant expression pattern may allow for heterogenous cell differentiation to not only glandular and myoepithelial lineages but also squamous and mesenchymal progenies as depicted in (Figure 1) [18].

CentralBringing Excellence in Open Access
Kanthan et al. (2016)Email:
JSM Surg Oncol Res 1(2): 1008 (2016) 3/7
Collagenous spherulosis (CS) is a benign myoepithelial lesion characterized by intraluminal eosinophilic, hyaline, acellular spherules rimmed by myoepithelial cells [18]. Both CS and bACC are composed of cribriform proliferation of epithelial and myoepithelial cells and can be therefore difficult to discriminate. Unlike bACC, CS typically does not form a mass and involves only a select few ducts, with cells of a lower nuclear-to-cytoplasmic ratio arranged in two-dimensional sheets [9]. An overlap in expression for myoepithelial markers p63 and SMA may confuse the two lesions; however, strong expression for ER, PR, CD10, and muscle-specific actin (HHF35) is identified in CS but not ACC whereas c-kit positivity is only associated with ACC [13].
Breast cylindroma is a very rare benign adnexal-type tumor that is easily confused with bACC as they are also composed of a dual proliferation of both basal and epithelial cells forming lobules surrounding PAS-positive basement material [19]. Unlike bACC, breast cylindromas are due to mutation of CYLD and lack the typical MYB-NFIB fusion gene or expression of c-kit as seen in bACC [19]. The differential diagnosis for the solid basaloid variant of bACC includes small cell carcinoma, solid papillary carcinoma,
metaplastic carcinoma, and malignant lymphoma [7]. Accurate differentiation of bACC from other breast tumorsis more zthan an exercise in academia, as despite its triple-negative phenotype bACC has a better prognosis compared with other forms of triple negative breast cancer and thus require appropriate therapeutic management. The correct diagnosis is often highly reliant on immunohistochemical staining and molecular analysis [19]. In keeping with triple-negative breast carcinomas, the majority (65%) of bACC expresses EGFR (Epidermal Growth Factor Receptor); however, there is no amplification of the EGFR gene [20]. Similarly, like triple-negative breast cancer, amplification of TOP2A is not a feature of bACC though unlike traditional triple-negative breast cancer AR (Androgen receptor) expression is not amplified in bACC [20].
PATHOGENESIS
Histopathogenesis
Though the exact origin of bACC is unknown, it has been postulated that it arises from a pluripotential progenitor cell
Figures
The spectrum of breast neoplasms with dual -luminal and abluminal cells
Figure
This flow diagram provides an overarching unified genesis of the genre of breast neoplasms with a dual component of luminal and
abluminal cells arising from the pluripotent parent host progenitor breast stem cells. Neoplasms with a benign outcome comprise the
breast adenomyoepithelioma, collagenous spherulosis and the cyclindroma, uncommon, but well documented lesions of the breast.
Alongside the malignant counterpart tumors of low grade with a good prognosis are the adenosquamous carcinoma [low grade] and
the adenoid cystic carcinoma. Amongst the high grade malignant neoplasms are depicted squamous and metaplastic carcinoma which
may represent progression of low grade tumors to a dedifferentiated phenotype.
Though traditionally adenoid cystic carcinoma of the breast is a neoplasm of good prognosis with over 90% survival over 15 years, the **solid basaloid variant of adenoid cystic carcinoma is an aggressive neoplasm. This variant may be an independent distinctive denovo
tumor type or may represent progression of bACC to a higher grade tumor. The mechanisms of the latter are unclear at the present
time.
Pluripotent Progenitor Stem Cells
Luminal & Abluminal cells
Benign
Breast Adenomyoepithelioma
Breast Cylindroma
Malignant
Low-grade
Low-Grade Adenosquamous
Carcinoma
Adenoid Cystic Carcinoma
High-grade
Squamous carcinoma
Metaplastic carcinoma
**Solid basaloid variant of Adenoid cystic carcinoma
Collagenous spherulosis
?progression
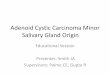
Figure 1 The spectrum of breast neoplasms with dual -luminal and abluminal cells.This flow diagram provides an overarching unified genesis of the genre of breast neoplasms with a dual component of luminal and abluminal cells arising from the pluripotent parent host progenitor breast stem cells. Neoplasms with a benign outcome comprise the breast adenomyoepithelioma, collagenous spherulosis and the cyclindroma, uncommon, but well documented lesions of the breast. Alongside the malignant counterpart tumors of low grade with a good prognosis are the adenosquamous carcinoma [low grade] and the avdenoid cystic carcinoma. Amongst the high grade malignant neoplasms are depicted squamous and metaplastic carcinoma which may represent progression of low grade tumors to a dedifferentiated phenotype.Though traditionally adenoid cystic carcinoma of the breast is a neoplasm of good prognosis with over 90% survival over 15 years, the **solid basaloid variant of adenoid cystic carcinoma is an aggressive neoplasm. This variant may be an independent distinctive �denovo tumor type or may represent progression of bACC to a higher grade tumor. The mechanisms of the latter are unclear at the present time.

CentralBringing Excellence in Open Access
Kanthan et al. (2016)Email:
JSM Surg Oncol Res 1(2): 1008 (2016) 4/7
capable of dual differentiation into the luminal and the basal ‘abluminal’ cell type. These dual proliferations of cells can result in the formation of benign lesions such as breast cyclindroma and breast adenomyoepithelioma. Their malignant counterpart includes lesions such as low grade adenosquamous carcinoma and adenoid cystic carcinoma. These malignant lesions are typically low grade indolent breast cancers yet, they can transform to higher grade aggressive lesions such as squamous carcinoma, solid basaloid variant bACC and metaplastic carcinoma as illustrated in (Figure 1).
Two case reports of bACC arising in adenomyoepitheliomas have been published [21, 22]. These are solitary tumors with myoepithelial proliferation admixed with epithelial elements that are typically classified as benign or low-grade malignant as local recurrence has been reported. Uncommonly, carcinomas arise in these lesions including biphasic tumors of both epithelial and myoepithelial origin such as bACC and it is suggested that these lesions may arise from the same pluripotent progenitor cells, creating a spectrum of adenomyoepithelioma-related epithelial/myoepithelial lesions ranging from low to high grade [21,22] (Figure 1). Some authors suggest that precursor lesions to bACC may include microglandular adenosis, tubular adenosis, adenomyoepithelioma, and fibroadenoma [14]. Microglandular adenosis is characterized by proliferation of small glands within the breast’s fibrous tissue [8]. It has been suggested that bACC may develop in continuity and in the background of this lesion; it is further suggested that there exists a morphological spectrum through which lesions progress that includes microglandular adenosis, atypical microglandular adenosis (“ACC in situ”) then invasive ACC [7]. No evidence exists to suggest tubular adenosis plays any similar role in this developmental pathway despite reports of its coexistence with bACC [3].
ACC of the breast has been reported to coexist with a number of other malignancies including micro-papillary invasive carcinoma, spindle-cell carcinoma, small-cell carcinoma, melanoma, invasive ductal carcinoma, and carcinoma in situ [23]. The “hypothesis of de-differentiation” proposes that these dual tumors are the result of a single tumor and at some point only part of the original tumor undergoes transformation that leads to the more aggressive pathology [23]. The two (immuno) histological patterns are due to multi-potential neoplastic progenitor stem cells committed to a myoepithelial phenotype undergoing de-differentiation along the neuro endocrine phenotype line which can progress as far as spindle-cell carcinoma or melanoma [23].
Molecular Mechanisms
The molecular mechanisms underlying bACC are more similar to ACC of the salivary gland than of other triple negative breast cancers. Gene fusion of the oncogene MYB to the transcription factor NFIB resulting from t (6;9)(q22-23;p23-24) translocation is an early event specific to ACC of the breast (28-100%) and is also seen in other breast cancers (23-100%). This results in over expression of MYB mRNA and protein [24, 25]. It is suggested that even in fusion-negative ACC, MYB activation remains an important molecular event and results from other mechanisms [24]. MYB is thereafter responsible for controlling cell proliferation, apoptosis, and differentiation [7]. Mutation rates of salivary gland and breast ACC are similar, at 0.31 vs 0.27
non-silent mutations/Mb [24]. Genetic changes of both types of ACC target chromatin remodeling, cell adhesion, RNA biology, ubiquitination, and signaling pathways including mutations of BRAF, FBXW7, SMARCA5, SF3B1 and FGFR2 [24]. While salivary gland ACC has mutations of NOTCH1, NOTCH2, and SPEN, this is not true for bACC [24]. Micro-RNA profiling of both salivary and breast ACC, however, showed different expression with salivary ACC over expressing, and bACC down-regulating seven miRNAs (let-7b, let-7c, miR-17, miR-20a, miR-24, miR-195, and miR-768-3) and salivary ACC down regulating and bACC over expressing nine others (et-7e, miR-23b, miR-27b, miR-193b, miR-320a, miR-320c, miR-768-5p, miR-1280 and miR-1826) [26]. Thus ACCs share a distinctive mutational profile due to inherent genomic structure irrespective of their site of origin.
ACC of the breast have a significantly lower frequency of genomic instability and copy-number alterations compared with invasive ductal carcinoma and basal-like carcinoma and many of the genomic changes associated with these more aggressive breast cancers are not common in bACC [7,25,27].In contrast to traditional triple negative cancers, bACC tumors have a low proliferation index with low Ki67 [7] and are characterized by a collection of genomic aberrations that are largely distinct from grade-matched triple-negative/basal-like invasive ductal carcinoma [27]. Breast ACC has a lack of 16q loss and 1q gain, hallmark features of invasive ductal carcinoma, or gains of 1q/6p/8q/10p and losses of 4p/5q/10q which are features of basal-like invasive ductal carcinoma [27]. Mutations typical of other triple-negative breast cancers such as TP53 and PIK3CA are absent in bACC [24,25] whereas the MYB-NFIB fusion is usually absent in other forms of breast cancer [27]. Similarly, though EGFR2(Her2 neu) is not overexpressed in bACC yet EGFR(Her-1) is commonly over expressed in the absence of any associated EGFR gene alterations[14]. The indolent nature of bACC “triple-negative” tumor is derived from its genetic stability when compared with the triple-negative IDC counterparts [27]. While bACCs are traditionally described as triple negative tumors [ER, PR and Her-2 neu negative], up to 26-61% are reported as ER-positive, and 23-36% as PR-positive [2]. It is suggested that hormone receptor positivity may indicate a non-pure bACC with elements of invasive cribriform carcinoma, and subsequently carry a worse prognosis than pure bACC [2]. Perhaps the estrogen-negative status of these tumors is not due to poor differentiation as is the case for typical triple-negative tumors, but rather due to preserved polarity and differentiation of the epithelial and myoepithelial cells [8]. Androgen receptor (AR) another important steroid receptor implicated in the pathogenesis of breast cancer is also absent in bACC unlike other triple negative tumors that often express AR. Proliferation rates also show marked contrast with bACC having extremely low rates while triple negative basal cancers are usually associated with high proliferation rates. TOP2A expression in bACC is low and is not associated with TOP2A gene amplification unlike triple negative breast cancers that often have high TOP2A expression with no associated gene amplification [14]. A characteristic stem cell marker CD44+/CD24- immunephenotype is observed in bACC and triple negative tumors. Though high cKIt protein expression is observed in bACC, this is not accompanied by underlying gene alterations [14]. Mutations in PIK3CA and PTEN are associated

CentralBringing Excellence in Open Access
Kanthan et al. (2016)Email:
JSM Surg Oncol Res 1(2): 1008 (2016) 5/7
with metastatic bACC and as such confer a poor prognosis, detected in both the primary tumor and the metastases to the kidney in one study [28]. Further large cohort studies are needed to confirm this hypothesis; however the rarity of these lesions and their indolent behavior precludes patient recruitment. High-grade transformation of bACC to triple-negative breast cancer of no special type involves clonal shifts and additional genetic effects, including mutation of EP300, NOTCH1, ERBB2, FGFR1, MYB, STAG2, KDM6A, and/or CDK12 [25]. The MYB-NFIB fusion gene is believed to play a central role in this transformation [25].
Treatment
The best practice management for bACC remains ill-defined and controversial [4]. It is suggested that treatment should be based on tumor grade, with grade I tumors undergoing simple lumpectomy, grade II simple mastectomy, and grade III mastectomy with axillary clearance; however, these guidelines are not universally accepted resulting in a high degree of variability in clinical practice [29].
Surgery
There remains no consensus whether bACC should be treated with a modified radical mastectomy or with breast conserving surgery, resulting in global variations. Modified radical mastectomy has fewer recurrences of bACC compared with local excision which can be as high as 6-37% [2,4]. Five-year postoperative rates of locoregional control are better with mastectomy (100%) compared with breast-conserving surgery (93%) [2]. This higher rate of local disease recurrence is postulated to be strongly correlated to the presence of positive margins. Some authors argue that the rate of local recurrence is unacceptably high when used in isolation [30]; however, when combined with radiotherapy breast conserving surgery has excellent outcomes, as discussed below [2]. Furthermore, success rates in the treatment of recurrent disease are extremely high so while a local recurrence creates added psychological stress to the patient and necessitates further surgical intervention, survival rates remain unchanged.
Axillary lymph node involvement is very rare at 0-2% and as such routine management of the axilla is controversial. A study by the Rare Cancer Network showed that among sixty-one patients with bACC, 68% had an axillary lymph node dissection and 16% had a sentinel node biopsy; all lymph nodes were negative with no axillary relapse by 79 months [2].The risk of lymph node involvement increases with larger tumors [5]. Therefore it is suggested that axillary dissection is indicated only in the presence of clinical palpable lymph node involvement, concomitant invasive carcinoma, and potentially for the ‘solid basaloid’ variant [15].Sentinel node biopsy is prudent for tumors larger than 3cm or in the event of a second dual invasive carcinoma [2,4]. An exception may be in the more aggressive solid basaloid-type bACCs who may merit sentinel node biopsy or complete axillary dissection even in the absence of positive clinical axillary findings [4,31]
Radiotherapy [RT]
Improved prognosis following radiotherapy management was reported by several authors for patients undergoing breast-
conserving surgery; RT improved the 5-year locoregional control rates by 12% but failed to influence survival as recurrences were successfully managed in one study [2]. Despite positive margins following breast conserving surgery, the addition of radiotherapy resulted in no local recurrences, with improvement in loco-regional control rates at 5- and 10-years from 83% and 42% among patients not treated with RT, to 95% and 88% among patients that did receive RT, respectively [2]. It is therefore inferred that breast conserving surgery with radiotherapy has equivocal outcomes to mastectomy [2]. Larger reviews of the SEER database revealed adjuvant RT improves overall and disease-specific survival [32].
Chemotherapy & Hormonal Therapy
The role of chemotherapy and hormonal therapy for bACC is not well described in the literature. Proposed indications for systemic chemotherapy may include a) metastatic disease, b) tumor size larger than 3cm, and/or c) high-grade lesions [4]. As these tumors are triple-negative, routine hormonal therapy is not indicated: however, targeted therapy such as anti-EGFR or c-kit may be a promising future treatment modality [15,20].
Prognosis and Predictive factors
ACC of the breast remains an indolent malignancy with high rates of local control, low rates of metastatic disease, and overall excellent survivorship. This may be partially due to detection at a low-grade stage, as bACC is more often identified as a well-differentiated tumor without lymph node involvement. A comparison between grade 1 bACC and grade 1 IDC showed no significant difference in overall survival [10].
Univariate analysis showed no relationship between disease-free survival and TNM staging, menopausal status, age, perineural invasion, type of surgery, margin status, or use of radiation therapy [2]. The presence of absence of a MYB-NFIB genetic fusion does not correlate with overall clinical outcome [33].
The prognosis of bACC is significantly better than other triple-negative breast cancers, or of ACC located elsewhere in the body. Ten-year survival rates are 85-100% compared with 30-54% for ACC of the head and neck [4].The prognosis of mixed/ dual tumors with bACC depends on the second component present: as the presence of this second component of higher malignancy dictates and trumps the overall prognosis [23]
The prevalence of axillary nodal disease is rare, reported at 0.8-2% and may be due to tumor extension rather than ‘true’ lymphatic spread [2]. A review of the National Cancer Database of 933 bACCs found that only 5% of women who underwent axillary node dissection were positive for disease [10]. Local recurrence at five years is reported at 6%, with a 31% rate at 10 years [4]. Distant metastases are rare, yet they have been reported in the lung most frequently followed by the liver, kidney, and bone. Unlike typical triple-negative breast cancer where metastatic disease occurs within the first three years, in bACC delayed metastases are reported up to ten years after initial diagnosis and these are not always preceded by axillary node involvement [15]. Yearly chest x-rays postoperatively are recommended for long-term follow-up as the lungs are the most frequent site of distant metastases [10] in this context, the solid

CentralBringing Excellence in Open Access
Kanthan et al. (2016)Email:
JSM Surg Oncol Res 1(2): 1008 (2016) 6/7
basaloid subtype is an exception of these observations as it has a more aggressive natural history with higher rates of local breast recurrences and delayed metastatic disease after many years [16]. One study found one-third of patients with grade 3 solid basaloid bACC had either nodal metastases or tumor recurrences [33]. Occasionally, late visceral metastases are not uncommon in bACC especially with the aggressive solid basaloid variant. Based on the Surveillance Epidemiology and End Results (SEER) Program data, a population based cohort study in the United States of 338 women with bACC the 5 year, 10year and 15 year survival was 98.1%, 94.9% and 91.4% respectively [34]. This reiterates the overall good prognosis of traditional bACC.
CONCLUSIONSIn summary, bACC is a unique clinic pathological breast
entity characterized by a heterogeneous histological appearance and relatively indolent course often attributed to a lower rate of tumor progression. It is an unusual type of breast cancer that occurs as a result of a dual proliferation of luminal and abluminal cells forming glands and pseudo lumens with a triple negative (ER-ve, PR -ve and Her2-ve) phenotype and basal-like features. It has a distinctive immune phenotype of being C-kit and p63 positive in addition to co-expression of other basal markers and its triple negativity. Despite the paucity of known molecular characteristics, all ACC including breast share a distinctive mutational fingerprint of MYB –NFIB fusion gene due to translocation of t(6:9). Surgery with breast conservation or mastectomy is the primary line of management with radiotherapy for positive margins to prevent local recurrences. As nodal metastasis is rare, a conservative approach towards routine axillary dissection is adopted. However, as basaloid solid variant of bACC and high grade tumors can show aggressive behavior, these can justify sentinel lymph node dissection for diagnostic staging. The role of chemotherapy is controversial except in a metastatic scenario. Though traditional bACC is associated with a low incidence of nodal and distant metastases late visceral metastases are not uncommon, thus long term surveillance is recommended with future prospects for continued development of novel molecular therapeutic targets in the current era of precision medicine.
REFERENCES1. Franzese C, Zei G, Masoni T, Cecchini S, Monteleone E, Livi L, et al.
Adenoid cystic carcinoma of the breast. The double face of an exocrine gland carcinoma. Strahlenther Onkol. 2013; 189: 1049-1050.
2. Khanfir K, Kallel A, Villette S, Belkacémi Y, Vautravers C, Nguyen T, et al. Management of adenoid cystic carcinoma of the breast: a Rare Cancer Network study. Int J Radiat Oncol Biol Phys. 2012; 82: 2118-2124.
3. Marchiò C, Weigelt B, Reis-Filho JS. Adenoid cystic carcinomas of the breast and salivary glands (or ‘The strange case of Dr Jekyll and Mr Hyde’ of exocrine gland carcinomas). J Clin Pathol. 2010; 63: 220-228.
4. Boujelbene N, Khabir A, Boujelbene N, Jeanneret Sozzi W, Mirimanoff RO, Khanfir K, et al. Clinical review--breast adenoid cystic carcinoma. Breast. 2012; 21: 124-127.
5. Thompson K, Grabowski J, Saltzstein SL, Sadler GR, Blair S. Adenoid cystic breast carcinoma: is axillary staging necessary in all cases? Results from the California Cancer Registry. Breast J. 2011; 17: 485-489.
6. Tang P, Yang S, Zhong X, Yao J, Zhang Y, Dong H, et al. Breast adenoid cystic carcinoma in a 19-year-old man: a case report and review of the literature. World J Surg Oncol. 2015; 13: 19.
7. Miyai K, Schwartz MR, Divatia MK, Anton RC, Park YW, Ayala AG, et al. Adenoid cystic carcinoma of breast: Recent advances. World J Clin Cases. 2014; 2: 732-741.
8. Glazebrook KN, Reynolds C, Smith RL, Gimenez EI, Boughey JC. Adenoid cystic carcinoma of the breast. AJR Am J Roentgenol. 2010; 194: 1391-1396.
9. Ilkay TM, Gozde K, Ozgur S, Dilaver D. Diagnosis of adenoid cystic carcinoma of the breast using fine-needle aspiration cytology: A case report and review of the literature. Diagn Cytopathol. 2015; 43: 722-726.
10. Kulkarni N, Pezzi CM, Greif JM, Suzanne Klimberg V, Bailey L, Korourian S, et al. Rare breast cancer: 933 adenoid cystic carcinomas from the National Cancer Data Base. Ann Surg Oncol. 2013; 20: 2236-2241.
11. Tang W, Peng WJ, Gu YJ, Zhu H, Jiang TT, Li C, et al. Imaging Manifestation of Adenoid Cystic Carcinoma of the Breast. J Comput Assist Tomogr. 2015; 39: 523-530.
12. Treglia G, Bertagna F, Ceriani L, Giovanella L. A rare case of adenoid cystic carcinoma of the breast detected by (18)F-FDG PET/CT. Rev Esp Med Nucl Imagen Mol. 2015; 34: 205-206.
13. Cabibi D, Giannone AG, Belmonte B, Aragona F, Aragona F. CD10 and HHF35 actin in the differential diagnosis between collagenous spherulosis and adenoid-cystic carcinoma of the breast. Pathol Res Pract. 2012; 208: 405-409.
14. Vranic S, Bender R, Palazzo J, Gatalica Z. A review of adenoid cystic carcinoma of the breast with emphasis on its molecular and genetic characteristics. Human Pathology. 2013; 44: 301-309.
15. Kumar BR, Padmanabhan N, Bose G, Paneer V. A case report of adenoid cystic carcinoma of breast - so close yet so far from triple negative breast cancer. Journal of clinical and diagnostic research. 2015; 9: 01-03.
16. Foschini MP, Rizzo A, De Leo A, Laurino L, Sironi M, Rucco V. Solid Variant of Adenoid Cystic Carcinoma of the Breast: A Case Series With Proposal of a New Grading System. Int J Surg Pathol. 2016; 24: 97-102.
17. Mastropasqua MG, Maiorano E, Pruneri G, Orvieto E, Mazzarol G, Vento AR , et al. Immunoreactivity for c-kit and p63 as an adjunct in the diagnosis of adenoid cystic carcinoma of the breast. Mod Pathol. 2005; 18: 1277-12s82.
18. Nakai T, Ichihara S, Kada A, Ito N, Moritani S, Kawasaki T, et al. The unique luminal staining pattern of cytokeratin 5/6 in adenoid cystic carcinoma of the breast may aid in differentiating it from its mimickers. Virchows Arch. 2016; 469: 213-222.
19. Fusco N, Colombo PE, Martelotto LG, De Filippo MR, Piscuoglio S, et al. Resolving quandaries: basaloid adenoid cystic carcinoma or breast cylindroma? The role of massively parallel sequencing. Histopathology. 2016; 68: 262-271.
20. Vranic S, Frkovic-Grazio S, Lamovec J, Serdarevic F, Gurjeva O, Palazzo J, et al. Adenoid cystic carcinomas of the breast have low Topo II? expression but frequently overexpress EGFR protein without EGFR gene amplification. Human Pathology. 2010; 41: 1617-1623.
21. Van Dorpe J, De Pauw A, Moerman P. Adenoid cystic carcinoma arising in an adenomyoepithelioma of the breast. Virchows Arch. 1998; 432: 119-122.
22. Yang Y, Wang Y, He J, Pan G, Tuo X, Jiang A, et al. Malignant adenomyoepithelioma combined with adenoid cystic carcinoma of the breast: a case report and literature review. Diagnostic Pathology. 2014; 9: 148.

CentralBringing Excellence in Open Access
Kanthan et al. (2016)Email:
JSM Surg Oncol Res 1(2): 1008 (2016) 7/7
Senger JL, Kanthan R (2016) Adenoid Cystic Carcinoma of the Breast A Focused Review. JSM Surg Oncol Res 1(2): 1008.
Cite this article
23. Kontos M, Karles D, Petrou A, Alexandrou PT. Adenoid cystic carcinoma intermingled with ductal carcinoma of the breast: a case report and review of the literature. J Med Case Rep. 2011; 5: 437.
24. Martelotto LG, De Filippo MR, Ng CK, Natrajan R, Fuhrmann L, Cyrta J, et al. Genomic landscape of adenoid cystic carcinoma of the breast. J Pathol. 2015; 237: 179-189.
25. Fusco N, Geyer FC, De Filippo MR, Martelotto LG, Ng CK, Piscuoglio S, et al. Genetic events in the progression of adenoid cystic carcinoma of the breast to high-grade triple-negative breast cancer. Mod Pathol. 2016; 29: 1292-1305.
26. Kiss O , Tőkés AM , Spisák S , Szilágyi A , Lippai N , Székely B, et al. Breast- and salivary gland-derived adenoid cystic carcinomas: potential post-transcriptional divergencies. A pilot study based on miRNA expression profiling of four cases and review of the potential relevance of the findings. Pathol Oncol Res. 2015; 21: 29-44.
27. Wetterskog D, Lopez-Garcia MA, Lambros MB, A’Hern R, Geyer FC, Milanezi F, et al. Adenoid cystic carcinomas constitute a genomically distinct subgroup of triple-negative and basal-like breast cancers. J Pathol. 2012; 226: 84-96.
28. Vranic S, Bilalovic N, Lee LMJ, Kruslin B, Lilleberg SL, Gatalica Z, et al. PIK3CA and PTEN mutations in adenoid cystic carcinoma of the breast metastatic to kidney. Human Pathology. 2007; 38: 1425-1431.
29. Spiliopoulos D, Mitsopoulos G, Kaptanis S, Halkias C. Axillary lymph node metastases in adenoid cystic carcinoma of the breast. A rare finding. G Chir. 2015; 36: 209-213.
30. Wang S, Ji X, Wei Y, Yu Z, Li N. Adenoid cystic carcinoma of the breast: Review of the literature and report of two cases. Oncol Lett. 2012; 4: 701-704.
31. Shin SJ, Rosen PP. Solid variant of mammary adenoid cystic carcinoma with basaloid features. A study of nine cases. The American Journal of Surgical Pathology. 2002; 26: 413-420.
32. Coates JM, Martinez SR, Bold RJ, Chen SL. Adjuvant radiation therapy is associated with improved survival for adenoid cystic carcinoma of the breast. J Surg Oncol. 2010; 102: 342-347.
33. D’Alfonso TM, Mosquera JM, MacDonald TY, Padilla J, Liu YF, Rubin MA, et al. MYB-NFIB gene fusion in adenoid cystic carcinoma of the breast with special focus paid to the solid variant with basaloid features. Human Pathology. 2014; 45: 2270-2280.
34. Ghabach B, Anderson WF, Curtis RE, Huycke MM, Lavigne JA, Dores GM, et al. Adenoid cystic carcinoma of the breast in the United States (1977 to 2006): a population-based cohort study. Breast Cancer Res. 2010; 12: 54.