Embed Size (px)
Citation preview

J. Neurol. Neurosurg. Psychiat., 1967, 30, 56
Addison's disease and diffuse cerebral sclerosis1D. HOEFNAGEL, A. BRUN, S. H. INGBAR, AND H. GOLDMAN
From the Departments of Medicine and Pathology, Dartmouth Medical School, Hanover, New Hampshire,the C. S. Kubik Laboratory for Neuropathology, Massachusetts General Hospital, and the Thorndike Memorial
Laboratory, Boston City Hospital, Boston, Massachusetts, U.S.A.
In an earlier paper (Hoefnagel, van den Noort, andIngbar, 1962), the association of diffuse cerebralsclerosis and adrenal cortical atrophy in a youngboy was described and reports in the literature offive similar cases were reviewed. Three more in-stances of this syndrome have been recorded since1962 (Fanconi, Prader, Isler, Luthy, and Sieben-mann, 1963; Blaw, Osterberg, Kosak, and Nelson,1964; Dubois, Loeb, Perier, Parmentier, andSzliwowski, 1964) and the present report describesthe clinical and pathological features of this entityin yet another young male.
CASE HISTORY
A Caucasian male was admitted to the hospital at theage of I0O years because of diffuse hyperpigmentation ofthe skin for three years and progressive neurologicaldisease of about six months' duration. He had been bornafter a normal, full-term pregnancy and a normal deliverywith a birth weight of 3 kg. (6 lb. 10 oz.). The neonatalperiod was uneventful, and physical growth, mental, andsocial development progressed normally. He had had un-complicated measles, chickenpox, and mumps; therewere no untoward reactions to a full complement ofimmunizations. The patient was the older of two children;a sister, seven years younger, was healthy. The father andmother were 21 and 20 years old respectively at the timeof the patient's birth; the mother denied having had mis-carriages. The parents were not consanguineous and therewas no knowledge of neurological disease, Addison'sdisease, or pigmentary disorders in the family. Betweenthe ages of 1 and 8 years the patient had mild chronicallergic rhinitis and an occasional attack of asthmaticbronchitis. At the age of 71 years he underwent a tonsil-lectomy; the procedure was uneventful, but about 12hours postoperatively there occurred intractable vomitingculminating in coma, shock, and hyperthermia. The childrecovered rapidly after treatment with intravenous fluidsand cortisone. The patient had always had a 'sensitive'skin; small wounds would take a long time to heal andthey often became infected. The skin tanned easily in thesummer with normal fading of the pigmentation in thewinter. At the age of 7 years, scars of the skin were noted
'Supported by grants (GM 10210, AM 00267 and 2B5393) from theUnited States Public Health Service and a grant from the Charles H.Hood Dairy Foundation.
to be unusually dark and at about that time there begana slowly progressive, diffuse hyperpigmentation of theskin, which did not fade during the winter. In all otherrespects the patient was in apparent good health until theage of 10 years when he developed a paralysis of the leftlateral rectus muscle and upon examination was alsofound to have poor vision, bilateral nerve deafness,dysarthria, and unsteadiness of gait. The cerebrospinalfluid pressure was 120; it showed no cells, the Pandy re-action was positive, sugar 90 mg. and total protein 147mg. per 100 ml. A pneumoencephalogram was normal.The child's general health remained excellent, but theneurological disorder worsened steadily with increasing
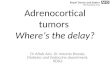
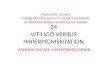
FIG. 1. The patient at 0JO years of age, showing diffusehyperpigmentation of the skin with accentuation in smallscars of the forehead.
56
Protected by copyright.
on March 25, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.1.56 on 1 February 1967. D
ownloaded from

Addison's disease and diffuse cerebral sclerosis
deafness, blindness, dysarthria, and ataxia; in the weeksbefore admission he became doubly incontinent. Therewere no headaches, vomiting or convulsions.Upon admission to the hospital the following were the
pertinent findings: height 145 cm. (57 in.), weight 42 kg.(93 lb.), blood pressure 115/85 mm. Hg, pulse 88/min.,and respiration 18/min. There was marked diffuse hyper-pigmentation of the skin (Fig. 1) accentuated in scars;the mucous membranes of the mouth were free of pig-mentation. Heart, lungs, abdomen, and genitalia werenormal. The sense of smell was intact. The patient walkedinto objects around him and there was no reaction tothreatening visual stimuli. The optic disks were flat,sharply outlined and pale; the retinae and maculae wereothervise normal. There were conjugate, roving move-ments of the eyes over a full range without a quick com-ponent. The pupils were equal in size and reacted slug-gishly to light directly and consensually; the comealreflexes were normal. There was no weakness of the facialmuscles. There was profound bilateral deafness. Thepatient walked with a stooped posture, slow, shufflingsteps, and marked ataxia. Involuntary movements wereabsent and resistance to passive manipulation of thelimbs was normal. The deep tendon reflexes were activeand symmetrical, the plantar responses were extensor, theabdominal reflexes absent and the cremasterics normal.The heel cords were tight and there was bilateral ankleclonus. Sensation to pinprick was intact.
Laboratory examinations showed the following:urine analysis was normal, haemoglobin 14-8 g. per 100ml.; normal total and differential white cell counts;serological test for syphilis and skin test for tuberculosiswere negative; blood urea nitrogen 9 mg. per 100 ml.,fasting blood sugars varied between 74 and 112 mg. per100 ml. The serum chloride levels varied between 96 and105, sodium between 133 and 146, potassium between4-6 and 5-4, and C02-combining power between 22 and23-2 mEq. per 1,000 ml. There were no calcifications on aradiograph of the abdomen and radiographs of the skulland chest were normal. Electrocardiography and electro-encephalography showed normal patterns. Examinationof the urine with cresyl violet and toluidine blue wasnegative for metachromatic mucolipids in the sedimentand metachromatic soluble lipids.
Urinary excretion of 1 7-hydroxycorticoids, duringfour days of control collections, ranged between 0-2 and0 4 mg. per 24 hours. In the same specimens, the level of17-ketosteroids was too low for accurate measurement,even though twice the usual volume of urine was ex-tracted; the results indicated that the excretion of 17-ketosteroids could not have exceeded 0-4 mg. per 24hours. Following the control collections, the patientreceived, over five consecutive days, a total of 240 unitsof A.C.T.H., either intravenously or as A.C.T.H. gelintramuscularly. Despite these large doses of A.C.T.H.,no increase in the urinary excretion of 17-hydroxycorti-coids or 17-ketosteroids was observed in 24-hour urinecollections during the five days.A diagnosis of Addison's disease associated with
diffuse cerebral sclerosis was made. After discharge fromthe hospital the neurological disorder worsened pro-gressively, not influenced by steroid therapy; the patient
developed a tetraplegia in flexion and died at the age of11 years and 3 months.
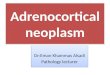
FINDINGS AT GENERAL NECROPSY On gross examination,congestion and oedema of the lungs with foci of atelec-tasis were noted. The pituitary, thyroid, pancreas, andtestes were normal, but careful dissection was necessaryto locate the markedly atrophied adrenal glands, each ofwhich weighed about I g. (normal for age 3 5-4 g.). Oncross section the corticomedullary junctions of theadrenals were distinct, but the cortex was less than 1 mm.thick. Pertinent microscopic findings were as follows: thelungs showed acute and chronic bronchopneumonia; inthe skin there was heavy melanin deposition in the basallayer of the epidermis with a small number of melanin-laden chromatophores in the upper dermis. The testiculartissue showed thickened basement membranes withabsence of Leydig cells, spermatogenesis, and mitoticactivity. The pituitary gland was normal. The peri-adrenal fat was atrophic. About two-thirds of the adrenalglands consisted of normal medulla; no defined zonaglomerulosa could be seen. There were several smalladrenocortical nodules formed by large eosinophiliccells with small eccentric nuclei and fine granular cyto-plasm (Fig. 2).
DESCRIPTION OF THE BRAIN (CASE x-379, MGH) The brainweighed 1,100 g. and had a normal shape and stirfacer~~~~~~~~~~~~~~~~~~~~~~~~~~ 2 "
FIG. 2. Cross section of adrenal, showing the atrophy ofthe cortex (haematoxylin and eosin, x 50).
57
Protected by copyright.
on March 25, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.1.56 on 1 February 1967. D
ownloaded from

D. Hoefnagel, A. Brun, S. H. Ingbar, and H. Goldman
A t -:l
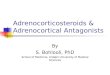
FIG. 3. Coronal sections through the frontal (A), parietal (B), and occipital (C) areas of the brain, showing the varyingdegrees of demyelination (myelin stain).
configuration. The optic nerves were slightly atrophicand of firm consistency. Coronal sections of the brainshowed widespread destruction of white matter bilater-ally in the occipital, temporal, and parietal lobes withless extensive changes in the frontal lobes (Fig. 3); theseareas looked grey and had a rubbery consistency. In thefrontal lobes there were several sharply delineated sub-cortical lesions of varying size. The thalamus, hypo-thalamus, pallidum, pituitary stalk, and mamillary bodieswere normal. The ventricular system was slightly widenedin its occipital portions. The cortex of the cerebral hemi-spheres was normal except where the white matter lesionshad extended to the pial membrane at the inferior-temporal and insular cortex bilaterally. The cerebellumwas normal. The mesencephalic peduncles were atrophicand gelatinous, particularly in their lateral halves. Allthrough the brain-stem the pyramidal tracts were greyand shrunken and the medulla and upper cervical cordwere reduced in width.The brain was extensively sampled, including the use of
whole hemisphere sections, and examined with thefollowing stains: haematoxylin and eosin, cresyl violet,Spielmeyer (for myelin), acid cresyl violet (for meta-chromatic substances), Sudan red (for fatty breakdownproducts), and silver stains (for axones and neurofibrils).
MICROSCOPIC INVESTIGATION The affected areas of whitematter showed extensive demyelination with completeloss of the basic structural pattern. In some areas therewas scar tissue formed by protoplasmic and fibrillaryastrocytes and a glial fibrillary meshwork containingmacrophages, which were often clustered perivascularlyin wide collars together with lymphocytes and plasmacells. The macrophages contained red sudanophilicmaterial, which did not react metachromatically. Axonswere present in reduced numbers. There also weredegenerative cell changes including pyknotic oligoden-droglial nuclei surrounded by swollen eosinophiliccytoplasm and larger cells showing karyorrhexis. In areaswith damaged U-fibres there were cortical changes, par-
ticularly in the deep layers, with loss of cortical myelinand degeneration of nerve cells which were encrustedwith a granular pigment. The hypothalamus showedmore discrete lesions than the brain paranchyma else-where; the paraventricular nuclei were normal. The optictracts showed symmetrical demyelination confined to thesuperior halves; demyelination was also noted in theoptic chiasm. The central portions of the optic nerveswere partly demyelinated; this change reached thesuperior surface only. The cellular response here was mildwith scattered astrocytes, but few lymphocytes and goodpreservation of the basic tissue pattern, whereas in theoptic tracts there was a marked lymphocytic and glialresponse and more complete loss of myelin with extensivescarring. The cerebellum showed only minimal changes.The mesen- and rhombencephalon showed demyelinatedlesions similar to those of the cerebral white matter,though much less extensive. The pyramidal tracts showedadvanced demyelination as far down as the cervical cord.
DISCUSSION
Adrenocortical hypofunction in the present patientevidently began at about 71 years of age, when in-creasing cutaneous pigmentation became apparentand when the child had an episode typical of post-operative adrenal crisis relieved by fluid replacementand cortisone. Nevertheless, despite the discontinua-tion of cortisone therapy, the patient was quite welluntil the age of 10 when the neurological disorderbecame manifest. At the time of admission to thehospital, evidence of adrenocortical failure, otherthan hyperpigmentation, was lacking. Presumably,an adequate level of basal corticosteroid secretionwas maintained; secretion was not increased, how-ever, in response to large doses of A.C.T.H. Thesefindings indicate a complete lack of adrenocorticalreserve. The intense cutaneous pigmentation in-
58
Protected by copyright.
on March 25, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.1.56 on 1 February 1967. D
ownloaded from

Addison's disease and diffuse cerebral sclerosis
dicated hypersecretion of A.C.T.H. In this respectthe present patient differs from one previouslyreported (Hoefnagel et al., 1962), who showedadrenocortical atrophy at necropsy, while duringlife there had not been cutaneous hyperpigmenta-tion; evidence of A.C.T.H. production in theanterior pituitary gland was lacking (absence ofbasophilic cells), although the patient had notreceived replacement therapy with steroids. In thepresent patient the clinical course of the neurologicaldisorder and the subsequent neuropathological find-ings were those of demyelinating diffuse cerebralsclerosis of the sudanophilic type.Some pertinent features of cases conforming to
this syndrome reported to date have been set out ina Table; only those with complete pathological de-scriptions have been included. In a similar tabula-tion, Dubois et al. (1964) excluded the case describedby Hoefnagel et al. (1962), because the authors con-sidered it to be a case of tuberous sclerosis associatedwith adrenocortical atrophy; however, after personalexamination of the histological material the authorsconfirmed the diagnosis of sudanophilic diffusecerebral sclerosis (Dr. 0. Perier, personal com-munication). In addition to the cases listed in theTable, several more are known to us to have beenobserved in other centres; all of these patients havebeen young males. In at least one instance, a boy
TABLESUMMARY OF CASES REPORTED IN THE LITERATURE
Reference
Age ofOnset ofAddison's Disease(yr.)
Siemerling andCreutzfeldt (1923)Pfister (1936)Gagnon and Leblanc,case 3 (1959)Lichtenstein andRosenbluth, case 3(1959)Brun and Voigt(1960)Hoefnagel et al.(1962)Fanconi et al. (1963)Blaw et al. (1964)Dubois et al. (1964)Present case
3-43
7
Unknown
9
Unknown14 yr. 3 mth.8U
Unknown71
Age ofOnset ofCerebralSclerosis(yr.)
Age atDeath (yr.)
6i 77 8i
14 yr
ance comes from earlier reports of affected malesiblings (Hoefnagel et al., 1962; Gagnon andLeblanc, 1959) and of maternal male relatives. Amaternal uncle of the patient of Blaw et al. (1964)had died at the age of 14 years of diffuse cerebralsclerosis, sudanophilic type; no information wasavailable on hyperpigmentation of the skin or thehistopathology of the adrenal glands. A maternalcousin of the case reported by Dubois et al. (1964)had died of a neurological disorder, clinically diag-nosed as diffuse cerebral sclerosis. Future work inthis syndrome should include studies to test theassumption that the gene for the trait is located onthe X chromosome; tests for colour vision, typingfor the Xg blood group, and endocrinological studiesin the female carriers are to be considered. Whileassuming that the cause of the syndrome is geneticin nature, any attempt to explain the pathogeneticrelationship of the neurological and endocrino-logical aspects has to be even more speculative. Inthe cases hitherto reported, evidence of adreno-cortical failure preceded or coincided with the onsetof manifestations of the disease of the nervous system(see Table). In those patients in whom the diagnosisof adrenocortical hypofunction was made duringlife with adequate response to treatment of theendocrinological features (Brun and Voigt, 1960;Fanconi et al., 1963; Dubois et al., 1964) the nervoussystem disease nevertheless pursued its courserelentlessly. It is possible that the adrenocorticalfailure occurs secondary to primary lesions of thenervous system; another possibility to be consideredis that a genetic defect acts through a metabolicpathway pertinent to the integrity of development ofthe adrenal cortex and maintenance of myelinationof the nervous system.
SUMMARY
9 10 Clinical, laboratory, and pathological observationsare described in a young boy affected by a syndrome
5 7 consisting of Addison's disease and diffuse cerebralsclerosis of the sudanophilic type. The findings are
9 101 compared with those of similar cases, previously5i 7 reported. It is likely that the syndrome is caused by
r 5 mth. 17i an X-chromosomal genetic defect.yr.- 0 ms.
7-810
9 yr. 9 mth.10
I I yr. 3 mth.
previously recorded in the literature as a case ofAddison's disease (Meakin, Nelson, and Thorn,1959), has since died of diffuse cerebral sclerosis(Mosier, quoted by Fanconi et al., 1963). An X-chromosomal recessive mode of inheritance has tobe considered with transmission of the trait to halfof the male offspring through unaffected carriermothers. Further support for this mode of inherit-
We wish to thank the following colleagues for help in thisstudy: Dr. Jack E. Hale, St. John's Hospital, Tulsa,Oklahoma; Dr. John F. Crigler Jr., Children's HospitalMedical Center, Boston, Massachusetts; Dr. N. S. Halmi,State University of Iowa, Iowa City, Iowa, and Dr. K.Benirschke, Dartmouth Medical School, Hanover, NewHampshire.
REFERENCES
Blaw, M. E., Osterberg, K., Kosak, P., and Nelson, E. (1964). Sudano-philic leukodystrophy and adrenal cortical atrophy. Arch.Neurol. (Chic.), 11, 626-631.
59
Protected by copyright.
on March 25, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.1.56 on 1 February 1967. D
ownloaded from

60 D. Hoefnagel, A. Brun, S. H. Ingbar, and H. GoldmanBrun, A., and Voigt, G. E. (1960). Entzundliche cerebrale Skierose Hoefnagel, D., van den Noort, S., and Ingbar, S. H. (1962). Diffusemit Nebenniereninsuffizienz. Dtsch. Z. Nervenheilk., 180, cerebral sclerosis with endocrine abnormalities in young males.654-664. Brain, 85, 553-568.Dubois, R., Loeb, H., P6rier, O., Parmentier, R., and Szliwowski, H. Lichtenstein, B. W., and Rosenbluth, P. F. (1959). Schilder's disease(1964). Maladie d'Addison et scl6rose diffuse de Schilder. with melanoderma. J. Neuropath. exp. Neurol., 18, 384-396.Helv. paediat. Acta, 19, 528-555. Meakin, J. W., Nelson, D. H., and Thorn, G. W. (199). Addison'sFanconi, A., Prader, A., Isler, W., Luithy, F., and Siebenmann, R. Meain,aseW.: NelonDrthr.H. alnd Thdocrn, .W1959)673.Adio'(1963). Morbus Addison mit Hirnskierose im Kindesalter. Ein disease in two brothers. J.cKin. Endocr., 19, 726-731.hereditAres Syndrom mit X-chromosomaler Vererbung? Ibid., Pfister, R. (1936). Beitrag zur Kenntnis der diffusen Hirnsklerose.18, 480-501. Arch. Psychiat. Nervenkr., 105, 1-16.Gagnon, J., and Leblanc, R. (1959). Sclerose cer6brale diffuse avec Siemerling, E., and Creutzfeldt, H. G. (1923). Bronzekrankheit undmelanodermie et atrophie surr6nale. Un. mdd. Can., 88, sklerosierende Encephalomyelitis (Diffuse Skierose). Ibid., 68,392-415. 217-244.
Protected by copyright.
on March 25, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.1.56 on 1 February 1967. D
ownloaded from