Embed Size (px)
Citation preview

Page 1 of 7 Addendum #1 RFP 2019-19
ADDENDUM NO. 1
ISSUE DATE: April 29, 2019
FSCJ RFP NUMBER: 2019-19 FSCJ SOLICITATION TITLE: Group Dental Indemnity & DHMO Insurance (“Group PPO & DHMO Dental Insurance”) The above numbered solicitation is amended as follows:
Exhibit “A”- Questions and Answers
Exhibit “B”- PPO Plan Cert.
Exhibit “C”- DHMO Plan Cert.
Exhibit “D”- PPO Dental Administrative Services Contract
Exhibit “E”- FSCJ 12.31.18 Actuarial Memo
Exhibit “F”- PPO Provider Utilization*
Exhibit “G”- DHMO Provider Utilization*
Exhibit “H”- PPO 2017-2018 Enrollment by Tier*
Exhibit “I”- DHMO 2017-2018 Enrollment by Tier*
Exhibit “J”- Updated Census Report*
Exhibit “K”- RFP-2019-19 Word Version* *these Exhibits are in Excel and Word formats therefore they need to be downloaded separately.
The hour and date specified for receipt of proposals: X is not extended, remains May 15, 2019 @ 2:00 p.m. _ is extended until: __________________________________________________________________ _ posting date is extended until: ________________________________________________________ Except as provided herein, all terms and conditions of the solicitation, including changes made by all prior addenda (if any), remain unchanged and in full force and effect.
Proposers must acknowledge receipt of this addendum prior to the time set for receipt and opening of proposals as specified in the solicitation, or as amended, by one of the following methods:
(a) By signing and returning one copy of this addendum. (b) By acknowledging receipt on the copy of the proposal submitted. (c) By separate letter or email referencing the solicitation and addendum numbers. Email [email protected] FAILURE TO ACKNOWLEDGE RECEIPT OF THIS ADDENDUM PRIOR TO THE HOUR AND DATE SPECIFIED MAY RESULT IN REJECTION OF YOUR OFFER. If, by virtue of this addendum, you desire to change an offer already submitted, such change may be made by letter that makes reference to the solicitation and this addendum and is received prior to the opening hour and date specified. _____________________________________
Randi Brokvist Executive Director of Purchasing
(Complete this portion)
TO BE RESPONSIVE ALL PROPOSERS MUST ACKNOWLEDGE RECEIPT OF ADDENDUM #1 COMPANY: __________________________________________
SIGNATURE: _________________________________________
TITLE: _______________________________________________ DATE: _______________________________________________
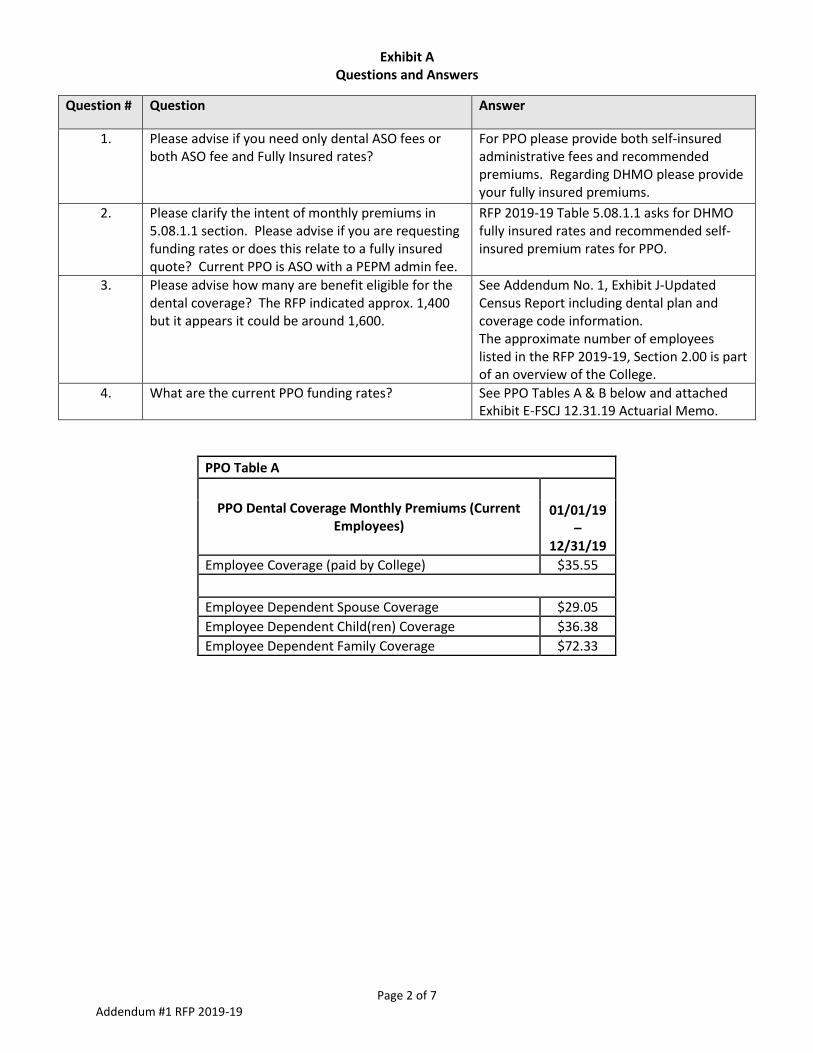
Exhibit A Questions and Answers
Page 2 of 7 Addendum #1 RFP 2019-19
Question # Question Answer
1. Please advise if you need only dental ASO fees or both ASO fee and Fully Insured rates?
For PPO please provide both self-insured administrative fees and recommended premiums. Regarding DHMO please provide your fully insured premiums.
2. Please clarify the intent of monthly premiums in 5.08.1.1 section. Please advise if you are requesting funding rates or does this relate to a fully insured quote? Current PPO is ASO with a PEPM admin fee.
RFP 2019-19 Table 5.08.1.1 asks for DHMO fully insured rates and recommended self-insured premium rates for PPO.
3. Please advise how many are benefit eligible for the dental coverage? The RFP indicated approx. 1,400 but it appears it could be around 1,600.
See Addendum No. 1, Exhibit J-Updated Census Report including dental plan and coverage code information. The approximate number of employees listed in the RFP 2019-19, Section 2.00 is part of an overview of the College.
4. What are the current PPO funding rates? See PPO Tables A & B below and attached Exhibit E-FSCJ 12.31.19 Actuarial Memo.
PPO Table A
PPO Dental Coverage Monthly Premiums (Current Employees)
01/01/19
–12/31/19
Employee Coverage (paid by College) $35.55
Employee Dependent Spouse Coverage $29.05
Employee Dependent Child(ren) Coverage $36.38
Employee Dependent Family Coverage $72.33

Exhibit A Questions and Answers
Page 3 of 7 Addendum #1 RFP 2019-19
Question #
Question Answer
5. What are the current DHMO rates? See DHMO Table A Below
DHMO Table A
DHMO Fully Insured Premium Rates
01/01/19-12/31/19
Employee Coverage (paid by College) $13.71
Retiree Coverage $13.71
COBRA Former Employee Coverage $14.01
Employee Family Coverage $15.86
Retiree Family Coverage $15.86
COBRA Family Coverage $16.21
Question #
Question Answer
6. Please provide a full census that includes the DOB, Gender, Zip Code, Plan of Coverage and Tier of coverage for all enrolled
See Addendum No. 1, Exhibit J-Updated Census Report.
7. Please clarify if you only need 2 tier (single and family) rates. If you require 4 tier, the census should indicate Employee, Employee and spouse, Employee and Child(ren) and Employee and Family.
The College requires all four tiers. See Addendum No. 1, Exhibit J-Updated Census Report.
PPO Table B
PPO Dental Coverage Monthly Premiums (Retirees & COBRA)
01/01/19
–12/31/19
Retiree Coverage $35.55
COBRA Former Employee Coverage $36.26
Retiree Spouse Coverage $29.05
Retiree Child(ren) Coverage $36.38
Retiree Family Coverage $72.33
COBRA Spouse Coverage $29.63
COBRA Child(ren) Coverage $37.11
COBRA Family Coverage $73.78

Exhibit A Questions and Answers
Page 4 of 7 Addendum #1 RFP 2019-19
Question #
Question Answer
8. Please provide a copy of the DHMO plan Cert that provides the current member copays along with all specialist services provided
See attached Exhibit C-DHMO Plan Cert.
9. Please provide a copy of the PPO plan Cert. See attached Exhibit B-PPO Plan Cert.
10. Please provide a copy of the PPO ASO Agreement with Delta Dental
See attached Exhibit D-PPO Dental Administrative Services Contract.
11. Please provide a PPO member report for the past 12-24 months that includes a count of subscriber and all dependents covered (including spouses and each dependent child)
See Addendum No. 1, Exhibit H-PPO Enrollment by Tier.
12. Please include an electronic PPO claims file for the past 12 months to include date of service, procedure code, provider information, provider location, network status (in vs out), submitted charge and allowed charge.
See Addendum No. 1, Exhibit F-PPO Provider Utilization. The College is unable to provide submitted charges and allowed charges.
13. Please provide a Provider Claims listing to include the Top 50 PPO providers by claims paid
See Addendum No. 1, Exhibit F-PPO Provider Utilization.
14. Please advise if we should include agent commission and if so, how much for the PPO and for the DHMO plans?
Yes. Please disclose any and all commissions and fees.
15. Please provide an updated census to also include Dental Tier (i.e. employee only, family, etc.), Dental Plan enrollment (which dental plan each participant is currently enrolled in), and indicate which subscribers are an Active employee, a Retiree or a Cobra subscriber.
See Addendum No. 1, Exhibit J-Updated Census Report.
16. If it is not possible to obtain an updated census, then please confirm the following: 1. Total # of Eligible Retirees and Total # of Enrolled Retirees. 2. Total # of Eligible Cobra and Total # of Enrolled Cobra. 3. Please confirm if provided census contains all eligible employees. If it doesn’t, please advise total eligible count.
See Answer #15.
17. Please provide the fully insured current monthly rates for the DHMO plan.
See Answer #5.
18. Please provide the detailed benefit Certificate of Coverage for both currently offered plans, if available.
See attached Exhibit B-PPO Plan Cert and Exhibit C-DHMO Plan Cert.
19. Could you please confirm whether FSCJ is accepting proposals from insurance carriers who are working directly with a broker/consultant such as myself?
Any proposers would need to disclose said arrangement and any fees associated with brokers.
20. Can you provide a full plan booklets for both PPO and DHMO?
See attached Exhibits B-PPO Plan Cert. and attached Exhibit C DHMO Plan Cert.
21. Can you provide rates for DMHO and premium equivalent rates for PPO?
See Addendum No. 1, Questions #4, PPO Tables A&B and Question #5, DHMO Table A.
22. What’s the employer contribution amount for DMHO and See Addendum No. 1, Question #5

Exhibit A Questions and Answers
Page 5 of 7 Addendum #1 RFP 2019-19
Question #
Question Answer
the retiree population? DHMO Table A.
23. Is the retiree group open or closed? Can you provide information has there been such a large increase in retirees?
Retiree group is open. Retiree enrollment remains flat.
24. Can you provide a census that list; elected plan, tier coverages, active vs retirees?
See Addendum No. 1, Exhibit J-Updated Census Report.
25. Can you provide updated claims data into 2019? See Addendum No. 1, Exhibit F-PPO Provider Utilization.
26. How long as the group been with Delta? Has there been any plan changes or rate changes over the last 3 years if so what?
See RFP Section, 2.03. An RFP was solicited in 2013 and Delta Dental was awarded for both PPO and DHMO Dental Insurance for the plan year starting January 2014. The PPO administrative fee was increased from 3.13% to 3.20% for the 2019 plan year.
27. Would you consider fully insured options for the PPO? No.
28. Can you provide a provider listing for the disruption which include zip codes and tax ID numbers for the providers?
See Exhibits F -PPO Provider Utilization and Exhibit G DHMO Provider Utilization. The College does not have access to provider tax ID numbers.
29. Regarding the reference letters/survey, page 33 states “number of pages: 3” but I only see pages 33 and 34 for the reference letter and survey. Is there a third page I’m missing or is it only 2 pages?
Page 33 of the RFP should Read “Number of pages including cover:2”
30. Can a certificate of insurance be provided for the PPO plan?
See attached Exhibit B PPO Plan Cert.
31. Can a full copayment schedule be provided for the DHMO plan?
See attached Exhibit C-DHMO Plan Cert.
32. In order to run a disruption report for the PPO and the DHMO, more information is needed. We will need TIN, provider number and full address at a minimum. A report simply comparing names is not reliable and will not serve the needs of FSCJ
See Exhibit F- PPO Provider Utilization. The College is unable to provide provider TIN numbers.
33. Do employees have to search Delta Dental’s website separately in order to determine if a provider is in the PPO network and/or the Premier network?
No.
34. PPO- Are all specialists paid at the Premier fee schedule even if they are contracted as participating in the PPO network?
Yes.
35. PPO-Are Premier dentists paid at the Premier fee schedule?
Yes.
36. PPO-Are non-Delta Dental dentists paid at the PPO fee schedule, the Premier fee schedule, 50th percentile, 80th
Dentists are paid at the PPO fee schedule.

Exhibit A Questions and Answers
Page 6 of 7 Addendum #1 RFP 2019-19
Question #
Question Answer
percentile, 90th percentile or some other methodology?
37. PPO- If non-Delta Dental dentists are paid at the MPA, what does that equate to when compared to percentiles? (40th, 50th, etc.)
Not applicable.
38. Can a census be provided that includes those covered by PPO, those covered by DHMO and by tier?
See Addendum No. 1, Exhibit J-Updated Census Report.
39. Are implants covered? If so, is surgical implantation covered or just the crown device?
See RFP Attachments B Summary of Current Delta Dental PPO Dental Plan and Attachment C Summary of Current Delta Dental DHMO Dental Plan.
40. Does FSCJ offer wellness programs for their employees? Yes, FSCJ offers a wellness program to its employees.
41. DHMO- Is this a capitated DHMO? Yes, it is capitated
42. DHMO-Are employees required to select a primary care dentist?
Yes.
43. DHMO- Can employees change dentists at any time or
must they contact Delta Dental to change their dentist if
they are required to select a primary care dentist?
Yes.
44. PPO-For Premier, do all dentists have the same fee schedule or are they able to submit their own fee schedule and have Delta Dental approve it?
The fees vary.
45. Can you please provide the RFP in Word format? See Addendum No. 1, Exhibit K-RFP 2019-19 Word Version.
46. Can you please provide current rates or rate relativities you wish for us to use?
See Addendum No. 1, Question #4 and Question #5 for the College’s current rates/premiums.
47. Does the College require plastic ID cards? No.
48. Does the College require an implementation credit? Yes. If there are costs related to implementation the College would require an implementation credit.
49. Can the PPO claim experience exhibit provide just the claims paid and enrollment by month for the past 12-24 months? The current exhibit is showing the # of single coverage but it appears to be a total and the actual single enrolled is not listed.
See Table Below
Month Total Claims Single plans Only (Active,Retired & COBRA)
TOTAL February 2017 84,807.25 846
TOTAL March 2017 62,709.70 844
TOTAL April 2017 64,878.00 838
TOTAL May 2017 60,986.50 835

Exhibit A Questions and Answers
Page 7 of 7 Addendum #1 RFP 2019-19
TOTAL June 2017 69,574.24 833
TOTAL July 2017 55,957.12 820
TOTAL August 2017 54,643.07 831
TOTAL September 2017 39,645.20 819
TOTAL October 2017 55,880.62 825
TOTAL November 2017 42,361.85 827
TOTAL December 2017 58,704.65 826
TOTAL January 2018 83,421.20 839
TOTAL February 2018 75,181.40 839
TOTAL March 2018 66,593.45 836
TOTAL April 2018 61,417.20 831
TOTAL May 2018 76,868.80 830
TOTAL June 2018 58,037.10 829
TOTAL July 2018 49,411.60 823
TOTAL August 2018 73,420.90 829
TOTAL September 2018 49,833.94 825
TOTAL October 2018 62,228.50 826
TOTAL November 2018 47,703.50 823
TOTAL December 2018 51,795.90 821
TOTAL January 2019 69,536.62 825
1,475,598.31

Exhibit B PPO Plan Cert.

FL-ASC-PPO-EOC(2006)
APPENDIX C
EMPLOYEE BENEFIT BOOKLET
FLORIDA STATE COLLEGE AT JACKSONVILLE
deltadentalins.com
Group No: 16724
Effective Date: January 1, 2014
Revised: January 1, 2015
Exhibit B

FL-ASC-PPO-EOC(2006) 16724
1
DENTAL PLAN COVERAGE FOR YOUR GROUP DENTAL PROGRAM
This plan is self-funded by your employer.
This booklet is a summary of your group dental program. Please read it carefully. It only summarizes the detailed provisions of the group dental contract issued by Delta Dental Insurance Company (“Delta Dental”) and cannot modify the Contract in any way. Claims Administered by:
Delta Dental Insurance Company 1130 Sanctuary Parkway
Suite 600 Alpharetta, Georgia 30009
(770) 641-5100 (800) 521-2651

FL-ASC-PPO-EOC(2006) 2 16724
TABLE OF CONTENTS
GROUP HIGHLIGHTS ................................................................................................................................................ 3
DEFINITIONS .............................................................................................................................................................. 3
CHOICE OF DENTIST ................................................................................................................................................ 5
WHO IS ELIGIBLE? .................................................................................................................................................... 5
DEDUCTIBLE .............................................................................................................................................................. 7
MAXIMUM AMOUNT ............................................................................................................................................... 7
BENEFITS, LIMITATIONS & EXCLUSIONS .......................................................................................................... 7
COORDINATION OF BENEFITS ............................................................................................................................ 10
AUTOMATED INFORMATION LINE .................................................................................................................... 11
CLAIMS ..................................................................................................................................................................... 11
PRE-TREATMENT ESTIMATES ............................................................................................................................. 12
CLAIMS APPEAL ..................................................................................................................................................... 12
PROVISIONS REQUIRED BY LAW ....................................................................................................................... 12
FL-ASC-PPO-EOC(2006) 3 16724
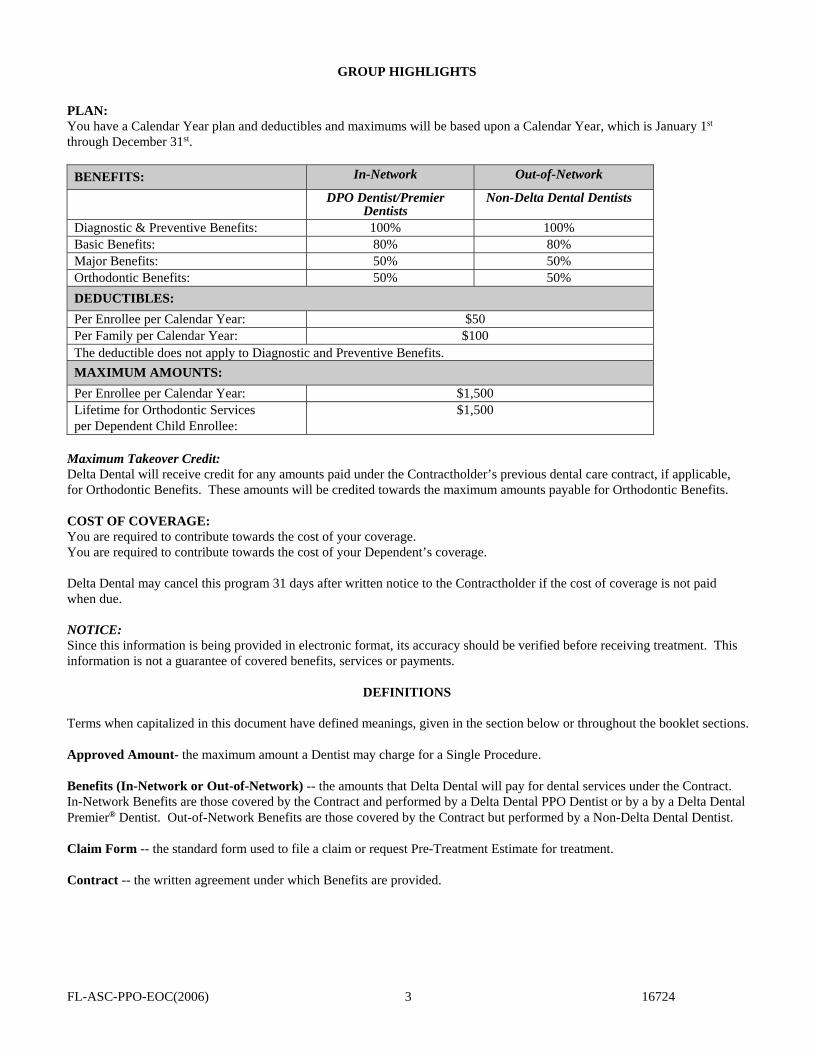
GROUP HIGHLIGHTS
PLAN: You have a Calendar Year plan and deductibles and maximums will be based upon a Calendar Year, which is January 1st through December 31st.
BENEFITS: In-Network Out-of-Network
DPO Dentist/Premier Dentists
Non-Delta Dental Dentists
Diagnostic & Preventive Benefits: 100% 100% Basic Benefits: 80% 80% Major Benefits: 50% 50% Orthodontic Benefits: 50% 50%
DEDUCTIBLES:
Per Enrollee per Calendar Year: $50 Per Family per Calendar Year: $100 The deductible does not apply to Diagnostic and Preventive Benefits.
MAXIMUM AMOUNTS:
Per Enrollee per Calendar Year: $1,500 Lifetime for Orthodontic Services per Dependent Child Enrollee:
$1,500
Maximum Takeover Credit: Delta Dental will receive credit for any amounts paid under the Contractholder’s previous dental care contract, if applicable, for Orthodontic Benefits. These amounts will be credited towards the maximum amounts payable for Orthodontic Benefits. COST OF COVERAGE: You are required to contribute towards the cost of your coverage. You are required to contribute towards the cost of your Dependent’s coverage. Delta Dental may cancel this program 31 days after written notice to the Contractholder if the cost of coverage is not paid when due. NOTICE: Since this information is being provided in electronic format, its accuracy should be verified before receiving treatment. This information is not a guarantee of covered benefits, services or payments.
DEFINITIONS
Terms when capitalized in this document have defined meanings, given in the section below or throughout the booklet sections. Approved Amount- the maximum amount a Dentist may charge for a Single Procedure. Benefits (In-Network or Out-of-Network) -- the amounts that Delta Dental will pay for dental services under the Contract. In-Network Benefits are those covered by the Contract and performed by a Delta Dental PPO Dentist or by a by a Delta Dental Premier® Dentist. Out-of-Network Benefits are those covered by the Contract but performed by a Non-Delta Dental Dentist. Claim Form -- the standard form used to file a claim or request Pre-Treatment Estimate for treatment. Contract -- the written agreement under which Benefits are provided.

FL-ASC-PPO-EOC(2006) 4 16724
Contract Allowance -- the maximum amount Delta Dental will use for calculating the Benefits for a Single Procedure. The Contract Allowance for services provided: by Delta Dental PPO Dentists and Delta Dental Premier Dentists is the lesser of the Dentist’s submitted fee, the Delta
Dental PPO Dentist’s Fee, the Dentist’s filed fee with Delta Dental in the Participating Dentist Agreement or Maximum Plan Allowance; or
by Non-Delta Dental Dentists is the lesser of the Dentist’s submitted fee or the Delta Dental PPO Dentist’s Fee. Contractholder -- the employer, union or other organization or group contracting to obtain Benefits. Delta Dental PPO Dentist (PPO Dentist) -- a participating Delta Dental Dentist who agrees to accept Delta Dental’s PPO Dentist’s Fees as payment in full and to comply with Delta Dental’s administrative guidelines. All PPO Dentists are also Delta Dental Premier Dentists. All PPO Dentists must be contracted in the Delta Dental Premier network. Delta Dental’s PPO Dentist’s Fee (PPO Dentist’s Fee) -- the fee outlined in the PPO Dentist Agreement. PPO Dentists agree to charge no more than this fee for treating PPO enrollees. Delta Dental Premier® Dentist (Premier Dentist) -- a Dentist who contracts with Delta Dental or any other member company of the Delta Dental Plans Association and who agrees to abide by certain administrative guidelines. Not all Premier Dentists are PPO Dentists; however, all Premier Dentists agree to accept Delta Dental’s Maximum Plan Allowance for each Single Procedure as payment in full. Dentist -- a person licensed to practice dentistry when and where services are performed. Dependent Enrollee -- a dependent of a Primary Enrollee or domestic partner who is eligible for Benefits under the Contract. Effective Date -- the date the program starts. This date is given on the booklet cover. Enrollee -- a Primary Enrollee or Dependent Enrollee enrolled to receive Benefits. Maximum Plan Allowance (MPA) -- the maximum amount Delta Dental will reimburse for a covered procedure. Delta Dental establishes the MPA for each procedure through a review of proprietary filed fee data and actual submitted claims. MPAs are set annually to reflect charges based on actual submitted claims from providers in the same geographical area with similar professional standing. The MPA may vary by the type of participating Dentist. Non-Delta Dental Dentist -- a Dentist who is neither a Premier nor a PPO Dentist and who is not contractually bound to abide by Delta Dental’s administrative guidelines. Open Enrollment Period -- the month of the year during which employees may change coverage for the next Contract Year. Participating PPO Dentist Agreement (PPO Dentist Agreement) -- an agreement between a member of the Delta Dental Plans Association and a Dentist which establishes the terms and conditions under which covered services are provided under a PPO program. Participating Dentist Agreement -- an agreement between a member of the Delta Dental Plans Association and a Dentist that establishes the terms and conditions under which services are provided. Pre-Treatment Estimate -- an estimation of the allowable Benefits under the Contract for the services proposed, assuming the patient is eligible. Primary Enrollee -- any employee or retiree eligible for Benefits under the Contract. Procedure Code -- the Current Dental Terminology (CDT) number assigned to a Single Procedure by the American Dental Association.

FL-ASC-PPO-EOC(2006) 5 16724
Qualifying Status Change -- a change in: legal marital status (marriage, divorce, legal separation, annulment or death); number of dependents (a child’s birth, adoption of a child, placement of child for adoption, addition of a step or foster
child or death of a child); employment status (change in employment status of Enrollee, spouse or dependent child); dependent child ceases to satisfy eligibility requirements (limiting age, student status or marital status); residence (Enrollee, dependent spouse or child moves); a court order requiring dependent coverage; or any other current or future election changes permitted by IRC Section 125.
Single Procedure -- a dental procedure that is assigned a separate CDT number.
CHOICE OF DENTIST
Delta Dental offers a choice of selecting a Dentist from our panel of PPO Dentists and Premier Dentists, or you may choose a Non-Delta Dental Dentist. A list of Delta Dental Dentists can be obtained by accessing the Delta Dental National Dentist Directory at deltadentalins.com. You are responsible for verifying whether the Dentist you select is a PPO Dentist or a Premier Dentist. Dentists are regularly added to the panel. Additionally, you should always confirm with the dentist’s office that a listed Dentist is still a contracted PPO Dentist or a Premier Dentist.
PPO Dentist The PPO program potentially allows you the greatest reduction in your out-of-pocket expenses, since this select group of Dentists in your area will provide dental Benefits at a charge which has been contractually agreed upon between Delta Dental and the PPO Dentist.
Premier Dentist The Premier Dentist, which include specialists (endodontists, periodontists or oral surgeons), has not agreed to the features of the PPO program; however, you may still receive dental care at a lower cost than if you use a Non-Delta Dental Dentist. A Premier Dentist can balance bill for the difference between the PPO Dentist’s Fee and the Premier Dentist’s Approved Amount. This amount may be more than the charge accepted by a PPO Dentist.
Non-Delta Dental Dentist If a Dentist is a Non-Delta Dental Dentist, the amount charged to you may be above that accepted by the PPO or Premier Dentists. Non-Delta Dental Dentists can balance bill for the difference between the PPO Dentist’s Fee and the Non-Delta Dental Dentist’s Approved Amount. For a Non-Delta Dental Dentist, the Approved Amount is the dentist’s submitted charge.
Additional advantages of using a PPO Dentist or Premier Dentist The PPO Dentist and Premier Dentist must accept assignment of Benefits, meaning PPO Dentists and Premier Dentists
will be paid directly by Delta Dental after satisfaction of the deductible and coinsurance, and the Enrollee does not have to pay all the dental charges while at the dental office and then submit the claim for reimbursement.
The PPO Dentist and Premier Dentist will complete the dental claim form and submit it to Delta Dental for reimbursement.
WHO IS ELIGIBLE?
Eligibility for Enrollment All present, permanent employees working 40 hours per week are eligible on the Effective Date.
All future permanent employees working 40 hours per week shall become eligible on the 1st day of the month following the date of hire.
If your dependents are covered, they will be eligible when you are or as soon as they become dependents. Dependents are your: a) Lawful spouse or domestic partner named in the Contratholder’s guidelines for domestic partnership;
b) Children from birth to the end of the year of their 26th birthday. Children include natural children, step-children,adopted children, children of the domestic partner and foster children. The child must be dependent on the EligiblePerson for support. Newborn infants are eligible from the moment of birth. Adopted children are eligible from themoment of placement in the physical custody of the Eligible Person, as certified by the agency making placement. Achild shall automatically be covered for 31 days after birth or adoption placement. To continue coverage after 31 days,notice of the birth or placement and additional fee, if any, must be received within the 31-day period.

FL-ASC-PPO-EOC(2006) 6 16724
A child 26 years or older may continue to be eligible as a dependent if the child is a) not self-supporting because of mental incapacity or physical handicap that began before age 26, and b) the child must be mostly dependent on the Eligible Person for support and maintenance. Proof of these facts must be given to Delta Dental or Contractholder within 31 days if it is requested. Proof will not be required more than once a year after the child is 28. Dependents in military service are not eligible. Enrollment Requirements If you are paying all or a portion of the cost of coverage for yourself or your dependents then: You must enroll within 31 days after the date you become eligible or during an Open Enrollment Period. All dependents must be enrolled within 31 days after they become eligible or during an Open Enrollment Period. If you elect dependent coverage, you must enroll all of your Dependent Enrollees for coverage. You must pay the cost of coverage in the manner elected by the Contractholder and approved by Delta Dental. Coverage
cannot be dropped or changed other than during an Open Enrollment Period or because of a Qualifying Status Change. If you pay the cost of coverage for Dependent Enrollees in the manner elected by the Contractholder and approved by
Delta Dental until your dependents are no longer eligible or until you choose to drop dependent coverage, coverage may not be changed at any time other than during an Open Enrollment Period or if there is a Qualifying Status Change.
A child who is eligible as a Primary Enrollee and a dependent can be insured under the Contract as a Primary Enrollee or as a Dependent Enrollee but not both at the same time.
Loss of Eligibility Your coverage ends on the last day of the month you stop working for the Contractholder or immediately when this program ends. Your dependents’ coverage ends when your coverage ends or on the date when dependent status is lost. Continuation of Benefits Delta Dental will not pay for Benefits for any services received after your coverage ends, but Delta Dental will pay for a Single Procedure incurred when the patient was covered if such procedure is completed within 31 days of the date coverage ends. A dental service is incurred as follows: for an appliance (or change to an appliance), at the time the impression is made; for a crown, bridge or cast restoration, at the time the tooth or teeth are prepared; for root canal therapy, at the time the pulp chamber is opened; and for all other dental services, at the time the service is performed or the supply furnished. Strike, Lay-off and Leave of Absence You and your dependents will not be covered for any dental services received while you are on strike, lay-off or leave of absence, other than as required under the Family & Medical Leave Act of 1993*. Benefits for you and your Dependent Enrollees will resume as follows: if coverage is reactivated in the same Calendar Year, deductibles and maximums will resume as if you were never gone; or if coverage is reactivated in a different Calendar Year, new deductibles and maximums will apply. Coverage will resume the first day of the month after you return to work, provided you submit to Delta Dental an enrollment card requesting that coverage be reactivated. *You and your dependents’ coverage is not affected if you take a leave of absence allowed under the Family & Medical Leave Act of 1993. If you are currently paying any part of your cost of coverage, you may choose to continue coverage. If you do not continue coverage during the leave, you can resume that coverage on your return to active work as if no interruption occurred. Important: The Family & Medical Leave Act does not apply to all companies, only those that meet certain size guidelines. See your Human Resources Department for complete information. If you are rehired within the same Calendar Year, deductibles and maximums will resume as if you were never gone.

FL-ASC-PPO-EOC(2006) 7 16724
Continued Coverage Under USERRA As required under the Uniformed Services Employment and Reemployment Rights Act of 1994 (USERRA), if you are covered by the Contract on the date your USERRA leave of absence begins, you may continue dental coverage for yourself and any covered dependents. Continuation of coverage under USERRA may not extend beyond the earlier of: 24 months beginning on the date the leave of absence begins or the date you fail to return to work within the time required by USERRA. For USERRA leave that extends beyond 31 days, the cost of coverage for continuation of coverage will be the same as for COBRA coverage. Continuation of Coverage Under COBRA COBRA (the Consolidated Omnibus Budget Reconciliation Act of 1985) provides a way for employees and their Dependent Enrollees who lose employer-sponsored group health plan coverage to continue coverage for a period of time. COBRA does not apply to all companies, only those that meet certain size guidelines. See your Human Resources Department for complete information.
DEDUCTIBLE
Your dental plan features a deductible. This is an amount you must pay out-of-pocket before Benefits are paid. The deductible amounts are listed on the Group Highlights page. Only the Dentist’s fees you pay for covered Benefits will count toward the deductible, but you do not have to pay a deductible for Diagnostic and Preventive Benefits.
MAXIMUM AMOUNT
The Maximum Amount payable is shown on the Group Highlights page. There may be maximums on a yearly basis, a per services basis, or a lifetime basis.
BENEFITS, LIMITATIONS & EXCLUSIONS Delta Dental will pay the Benefits for the types of dental services as described below. Delta Dental will pay Benefits only for covered services. These services must be provided by a Dentist and must be necessary and customary under generally accepted dental practice standards. Delta Dental may use dental consultants to review treatment plans, diagnostic materials and/or prescribed treatments to determine generally accepted dental practices. If you receive dental services from a Dentist outside the state of Florida, the Dentist will be reimbursed according to Delta Dental’s network payment provisions for said state according to the terms of the Contract. If a comprehensive dental procedure includes component or interim procedures that are performed at the same time as the comprehensive procedure, the component or interim procedures are considered to be part of the comprehensive procedure for purposes of determining the benefit payable under the Contract. If the Dentist bills separately for the comprehensive procedure and each of its component or interim parts, the total benefit payable for all related charges will be limited to the maximum benefit payable for the comprehensive procedure. Enrollee Coinsurance Delta Dental’s provision of Benefits is limited to the applicable percentage of Dentist’s fees shown on the Group Highlights page. You are responsible for paying the remaining applicable percentage of any such fees, known as the “Enrollee Coinsurance”. Your group has chosen to require Enrollee Coinsurances under this program as a method of sharing the costs of providing dental Benefits between Contractholder and Enrollees. If the Dentist discounts, waives or rebates any portion of the Enrollee Coinsurance to the Enrollee, Delta Dental will be obligated to provide as Benefits only the applicable percentages of the Dentist’s fees reduced by the amount of such fees that is discounted, waived or rebated.

FL-ASC-PPO-EOC(2006) 8 16724
BENEFITS Delta Dental will pay or otherwise discharge the percentage of Contract Allowance shown on the Group Highlights page for the following covered services. Diagnostic and Preventive Benefits: Diagnostic: procedures to assist the Dentist in choosing required dental treatment.
Preventive: prophylaxis cleaning, periodontal cleaning in the presence of gingival inflammation and topical application of fluoride solutions.
Basic Benefits: Oral Surgery: extractions and other surgical procedures (including pre-and post-operative care).
General Anesthesia or IV Sedation:
when administered by a Dentist for covered oral surgery or selected endodontic and periodontal surgical procedures.
Endodontics: treatment of the tooth pulp.
Periodontics: treatment of gums and bones supporting teeth.
Palliative: treatment to relieve pain.
Sealants: topically applied acrylic, plastic or composite materials used to seal developmental grooves and pits in permanent molars for the purpose of preventing decay.
Restorative: crown build-up, amalgam, synthetic porcelain, plastic restorations, composites (fillings) and prefabricated stainless steel restorations for treatment of carious lesions (visible destruction of hard tooth structure resulting from the process of decay).
Denture Repairs: adjustment, repair to partial or complete dentures including rebase procedures and relining.
Other Basic Services: cephalometric film, application of desensitizing medicament, space maintainers (including re-cementation), tissue conditioning, crown/inlay/onlay repair, bridge repair, gingival curettage, full-mouth debridement.
Major Benefits: Crowns, Inlays/Onlays
and Cast Restorations: treatment of carious lesions (visible decay of the hard tooth structure) when teeth cannot be restored with amalgam, synthetic porcelain, plastic restorations.
Prosthodontics: procedures for construction of fixed bridges, partial or completed dentures and the repair of fixed bridges; implant surgical placement and removal; and for implant supported prosthetics, including implant repair and recementation.
Other Major Services: crown lengthening, osseous surgery, free soft tissue graft, frenulectomy, mucogingival surgery, bone replacement grafts, pedicle soft tissue graft procedure, guided tissue regeneration and subepithelial connective tissue graft.
Orthodontic Benefits: Oral/facial photographic images, study models, procedures performed by a Dentist, involving the use of an active orthodontic appliance and post-treatment retentive appliances for treatment of malalignment of teeth and/or jaws which significantly interferes with their functions. LIMITATIONS Limitations on Diagnostic and Preventive Benefits: Delta Dental will pay for routine oral examinations and cleanings (including periodontal cleanings) no more than twice in
any 12 month period while the person is an Enrollee under any Delta Dental program or dental care program provided by the Contractholder.
Full-mouth x-rays or panoramic x-rays are limited to once every 36 months while the person is an Enrollee under any Delta Dental program.
Bitewing x-rays are provided once in a Calendar Year for each Enrollee. Topical application of fluoride solutions is limited to Enrollees under age 14.

FL-ASC-PPO-EOC(2006) 9 16724
Limitations on Basic Benefits: Cephalometric film is limited to once every 36 months. Space maintainers are limited to the initial appliance only and to Enrollees under age 14. Tissue conditioning is limited to twice in any Calendar Year. Denture adjustment is limited to twice in any Calendar Year. Re-cementation of a space maintainer is limited to once in any Calendar Year. Denture rebase and reline are limited to once in any 36 month period. Full-mouth debridement is limited to once in any 36 month period. Delta Dental limits Periodontics to Enrollees age 18 and older. Delta Dental will not pay to replace an amalgam, synthetic porcelain or plastic restorations, composites (fillings) within 12
months of treatment if the service is provided by the same Dentist. Delta Dental will not pay to replace prefabricated stainless steel restorations within 24 months of treatment if the service is
provided by the same Dentist. Delta Dental limits payment for stainless steel crowns under this section to services on baby teeth. However, after
consultant’s review, Delta Dental may allow stainless steel crowns on permanent teeth as a Major Benefit. Benefits for periodontal scaling and root planing in the same quadrant are limited to once in every 24-month period. Sealants are limited as follows:
(1) to 1st and 2nd molars on primary teeth, bicuspid and permanent molars of dependent children to age 17 if they are without cavities or restorations on the occlusal surface.
(2) Sealants do not include repair or replacement of a sealant on any tooth within two (2) years of its application. Limitations on Major Benefits: Delta Dental will not pay to replace any crowns, inlays/onlays or cast restorations which the Enrollee received in the
previous five (5) years under any Delta Dental program or any program of the Contractholder. Prosthodontic appliances and/or implants that were provided under any Delta Dental program will be replaced only after
five (5) years have passed, except when Delta Dental determines that there is such extensive loss of remaining teeth or change in supporting tissue that the existing fixed bridge or denture cannot be made satisfactory. Replacement of a prosthodontic appliance and/or implant supported prosthesis not provided under a Delta Dental program will be made if Delta Dental determines it is unsatisfactory and cannot be made satisfactory. Delta Dental will pay for the removal of an implant once for each tooth during the Enrollee’s lifetime.
Delta Dental limits payment for dentures to a standard partial or complete denture (coinsurances apply). A standard denture means a removable appliance to replace missing natural, permanent teeth that is made from acceptable materials by conventional means.
Limitations on Orthodontic Benefits: The maximum amount payable for each Enrollee during the Enrollee’s lifetime is shown on the Group Highlights page. Orthodontic Benefits will be provided in monthly payments, not to exceed 36 months. Benefits are not paid to repair or replace any orthodontic appliance received under this program. Benefits are not provided for orthodontic retreatment procedures. Orthodontic Benefits are limited to Dependent Child Enrollees to the end of the year of their 19th birthday. Non-orthodontic procedures performed for the purpose of orthodontic treatment are subject to the Orthodontic
coinsurance and lifetime maximum if covered as Benefits under Delta Dental’s standard processing policies. Limitations on All Benefits - Optional Services that are more expensive than the form of treatment customarily provided under accepted dental practice standards are called “Optional Services”. Optional Services also include the use of specialized techniques instead of standard procedures. For example: a crown where a filling would restore the tooth; a precision denture/partial where a standard denture/partial could be used; an inlay/onlay instead of an amalgam restoration; or a composite restoration instead of an amalgam restoration on posterior teeth. If you receive Optional Services, Benefits will be based on the lower cost of the customary service or standard practice instead of the higher cost of the Optional Service. You will be responsible for the difference between the higher cost of the Optional Service and the lower cost of the customary service or standard procedure.

FL-ASC-PPO-EOC(2006) 10 16724
EXCLUSIONS Delta Dental does not pay Benefits for: treatment of injuries or illness covered under workers’ compensation or employers’ liability laws; services received
without cost from any federal, state or local agency, unless this exclusion is prohibited by law.
cosmetic surgery or dentistry for purely cosmetic reasons.
services for congenital (hereditary) or developmental (following birth) malformations, including but not limited to cleftpalate, upper and lower jaw malformations, enamel hypoplasia (lack of development), fluorosis (a type of discoloration ofthe teeth) and anodontia (congenitally missing teeth), unless the service is provided to a newborn or adopted dependentchild for treatment of a medically diagnosed congenital defect.
treatment to restore tooth structure lost from wear, erosion or abrasion; treatment to rebuild or maintain chewing surfacesdue to teeth out of alignment or occlusion; or treatment to stabilize the teeth. For example: equilibration, periodontalsplinting, occlusal adjustment.
labial veneers.
any Single Procedure started prior to the date the person became covered for such services under this program.
prescribed drugs, medication, pain killers or experimental procedures.
charges by any hospital or other surgical or treatment facility and any additional fees charged by the Dentist for treatmentin any such facility.
charges for anesthesia, other than general anesthesia and IV sedation administered by a licensed Dentist in connection withcovered oral surgery or selected endodontic and periodontal surgical procedures.
extraoral grafts (grafting of tissues from outside the mouth to oral tissues).
treatment performed by someone other than a Dentist or a person who by law may work under a Dentist’s directsupervision.
charges incurred for oral hygiene instruction, a plaque control program, dietary instruction, x-ray duplications, cancerscreening or broken appointments.
services or supplies covered by any other health plan of the Contractholder.
services for Orthodontic treatment (treatment of malocclusion of teeth and/or jaws) except as provided under theOrthodontic Benefits section if applicable.
services for any disturbances of the temporomandibular (jaw) joints except as provided under the MPD-TMJ Benefitssection if applicable.
any tax imposed (or incurred) by a government, state or other entity, in connection with any fees charged for Benefitsprovided under the Contract, will be the responsibility of the Enrollee and not a covered Benefit.
COORDINATION OF BENEFITS
Delta Dental matches the Benefits under this program with your Benefits under any other group prepaid program or Benefit plan including another Delta Dental plan. (This does not apply to a blanket school accident policy). Benefits under one of the programs may be reduced so that your combined coverage does not exceed the Dentist’s fees for the covered services. If this is the “primary” program, Delta Dental will not reduce Benefits, but if the other program is the primary one, Delta Dental will reduce Benefits otherwise payable under this program. The reduction will be the amount paid for or provided under the terms of the primary program for services covered under the Contract (see Benefits and Limitations). How does Delta Dental determine which is the “primary” program?
(1) If the other Plan is not primarily a dental plan, this Plan is primary.

FL-ASC-PPO-EOC(2006) 11 16724
(2) If the other Plan is a dental program, the following rules are applied: a) the Plan covering the patient as an employee is primary over a Plan covering the patient as a dependent.b) the Plan covering the patient as an employee is primary over a Plan which covers the insured person as a
dependent; except that: if the insured person is also a Medicare beneficiary, and as a result of the rule establishedby Title XVIII of the Social Security Act and implementing regulations, Medicare is:i) secondary to the Plan covering the insured person as a dependent andii) primary to the Plan covering the insured person as other than a dependent (e.g. a retired employee),then the benefits of the Plan covering the insured person as a dependent are determined before those of the Plan covering that insured person as other than a dependent.
(3) Except as stated below, when this Plan and another Plan cover the same child as a dependent of different persons, called parents: a) The benefits of the Plan of the parent whose birthday falls earlier in a year are determined before those of the Plan
of the parent whose birthday falls later in that year, butb) If both parents have the same birthday, the benefits of the Plan which covered one parent longer are determined
before those of the Plan which covered the other parent for a shorter period of time.c) However, if the other Plan does not have the birthday rule described above, but instead has a rule based on the
gender of the parent, and if, as a result, the plans do not agree on the order of benefits, the rule in the other Planwill determine the order of benefits.
d) In the case of a dependent child of divorced parents, the Plan covering the patient as a dependent of the parentwith legal custody, or as a dependent of the custodial parent’s spouse (i.e. step-parent) will be primary over thePlan covering the patient as a dependent of the parent without legal custody. If there is a court decree whichwould otherwise establish financial responsibility for the health care expenses with respect to the child, thebenefits of a Plan which covers the child as a dependent of the parent with such financial responsibility will bedetermined before the benefits of any other policy which covers the child as a dependent child.
If the specific terms of a court decree state that the parents will share joint custody, without stating that one of the parents is responsible for the health care expenses of the child, the Plans covering the child will follow the order of benefit determination rules outlined in (3) a) through (3) c).
(4) The benefits of a Plan which covers an insured person as an employee who is neither laid off nor retired are determined before those of a Plan which covers that insured person as a laid off or retired employee. The same would hold true if an insured person is a dependent of a person covered as a retiree and an employee. If the other Plan does not have this rule, and if, as a result, the Plans do not agree on the order of benefits, this rule is ignored.
(5) If an insured person whose coverage is provided under a right of continuation pursuant to federal or state law also is covered under another Plan, the following will be the order of benefit determination: a) First, the benefits of a Plan covering the insured person as an employee, member or subscriber (or as that insured
person’s dependent);b) Second, the benefits under the continuation coverage.If the other Plan does not have the rule described above, and if, as a result, the Plans do not agree on the order of benefits, this rule is ignored.
(6) If none of the above rules determine the order of benefits, the benefits of the plan which covered an employee longer are determined before those of the Plan which covered that insured person for the shorter term.
AUTOMATED INFORMATION LINE
You may access Delta Dental’s automated information line on a regular business day to obtain information on Member Eligibility and Benefits; Group Benefit Information; Claim Status or to speak to a Customer Service Representative for assistance. AVA (800) 521-2651
CLAIMS
Claims for Benefits must be filed on a standard Claim Form which you or your Dentist may obtain from: Delta Dental Insurance Company
P.O. Box #1809 Alpharetta, Georgia 30023
(800) 521-2651 deltadentalins.com

FL-ASC-PPO-EOC(2006) 12 16724
PRE-TREATMENT ESTIMATES
A Dentist may file a Claim Form before treatment, showing the services to be provided to an Enrollee. Delta Dental will predetermine the amount of Benefits payable under the Contract for the listed services. Benefits will be processed according to the terms of the Contract when the treatment is performed. Pre-Treatment Estimates are valid for 60 days, or until an earlier occurrence of any one of the following events: the date the Contract terminates; the date the patient’s coverage ends; or the date the PPO Dentist’s or Premier Dentist’s Agreement with Delta Dental ends.
CLAIMS APPEAL Delta Dental will notify the Primary Enrollee if Benefits are denied for services submitted on a Claim Form, in whole or in part, stating the reason(s) for denial. The Enrollee has 180 days after receiving a notice of denial to appeal it by writing to Delta Dental giving reasons why the denial was wrong. The Enrollee may also ask Delta Dental to examine any additional information he/she includes that may support his/her appeal. Delta Dental will make a full and fair review within 60 days after Delta Dental receives the request for appeal. Delta Dental may ask for more documents if needed. In no event will the decision take longer than 60 days. The review will take into account all comments, documents, records or other information, regardless of whether such information was submitted or considered initially. If the review is of a denial based in whole or in part on lack of dental necessity, experimental treatment or clinical judgment in applying the terms of the Contract, Delta Dental shall consult with a Dentist who has appropriate training and experience. The review will be conducted for Delta Dental by a person who is neither the individual who made the claim denial that is subject to the review, nor the subordinate of such individual. The identity of such dental consultant is available upon request whether or not the advice was relied upon. If the Enrollee believes he/she needs further review of said claim, he/she may contact his/her state insurance regulatory agency if applicable or bring a civil action under section 502(a) of the Employee Retirement Income Security Act of 1974 (ERISA) if the Contract is subject to ERISA.
GENERAL PROVISIONS Clinical Examination Before approving a claim, Delta Dental will be entitled to receive, to such extent as may be lawful, from any attending or examining Dentist, or from hospitals in which a Dentist’s care is provided, such information and records relating to attendance to or examination of, or treatment provided to, an Enrollee as may be required to administer the claim, or that an Enrollee be examined by a dental consultant retained by Delta Dental, in or near his community or residence. Delta Dental will in every case hold such information and records confidential. Notice of Claim Forms Delta Dental will give any Dentist or Enrollee, on request, a standard Claim Form to make claim for Benefits. To make a claim, the form must be completed and signed by the Dentist who performed the services and by the Enrollee (or the parent or guardian if the patient is a minor) and submitted to Delta Dental. If the form is not furnished by Delta Dental within 15 days after requested by a Dentist or Enrollee, the requirements for proof of loss set forth in the next paragraph will be deemed to have been complied with upon the submission to Delta Dental, within the time established in said paragraph for filing proofs of loss, of written proof covering the occurrence, the character and the extent of the loss for which claim is made. Written Notice of Claim/Proof of Loss Delta Dental must be given written proof of loss within 12 months after the date of the loss. If it is not reasonably possible to give written proof in the time required, the claim will not be reduced or denied solely for this reason, provided proof is filed as soon as reasonably possible. In any event, proof of loss must be given no later than one year from such time (unless the claimant was legally incapacitated). All written proof of loss must be given to Delta Dental within 12 month of the termination of the Contract.

FL-ASC-PPO-EOC(2006) 13 16724
Time of Payment Claims payable under this Contract for any loss other than loss for which this Contract provides any periodic payment will be paid within 30 days after written proof loss is received. Delta Dental will notify the Primary Enrollee and his/her dentist of any additional information needed to process the claim within this 30 day period. Delta Dental will process the claim within 15 days of receipt of the additional information. If the requested information is not received within 45 days, the claim will be denied. Subject to due written proof of loss, all accrued indemnities for loss for which this Contract provides periodic payment will be paid monthly. To Whom Benefits are Paid PPO Dentists and Premier Dentists will be paid directly. Any other payments provided by the Contract will be made to the Primary Enrollee, unless the Enrollee requests when filing a proof of loss claim that the payment be made directly to the Dentist providing the services. All Benefits not paid to the Dentist will be payable to the Enrollee, or to his estate, except that if the person is a minor or otherwise not competent to give a valid release, Benefits may be payable to the parent, guardian or other person actually supporting him. Legal Actions No action at law or in equity will be brought to recover on the Contract prior to expiration of 60 days after proof of loss has been filed in accordance with requirements of the Contract, nor will an action be brought at all unless brought within three (3) years from expiration of the time within which proof of loss is required by the Contract. Cancellation of Program on an anniversary of the Effective Date upon 60 days written notice; or if your employer does not pay the monthly cost of coverage upon 31 days written notice; or if your employer does not provide a list of who is eligible upon 60 days written notice; or if less than the minimum number of Primary enrollees required under the Contract reported eligible for three (3) months or
more, upon 15 days written notice. THIS BOOKLET CONSTITUTES ONLY A SUMMARY OF THE DENTAL SERVICE CONTRACT. THE COMPLETE CONTRACT MUST BE CONSULTED TO DETERMINE THE EXACT TERMS AND CONDITIONS OF COVERAGE.

Exhibit C DHMO Plan Cert.

.................................................................................... ........................................................................................
......................... .................................................................
....................................................... .................................
......................................................................................... ........................................................
................................................................................................................ ..............................................................................................................
............................... ....................................................................................
...................................................................... ............................................................................................
............. ...................................................................................
.............................................................................................. .............................................................................................. ..............................................................................................
................................................. .................................................................................
...................................................................................................... .......................................................................
............................................................................................................ ....................................................................................................................... ........................................................................................................................
................................................................................
.......................................................
......................................................................................................................... ................................
......................... ...............................
...........
............................................. ..........................................................
............................................. ..........................................................
........................................................................
Exhibit C

............................................................................. ..........................................................
............................................................................................................. ..........................................................
................................................................................................................ ................................................... ...................................................
............................................................................................... .................................................................................................
........................................................................................ ......................................................................................... ..........................................................................................
................................................................................................ .............................................................
.................................................................................. ................................................................................
.............................................................................. .....................................................................
.................................................................................. .................................................................................
............................................................................... .....................................
........................................................................................... ................................................................................ ...............................................................................
............................................................................. ....................................................................
........................................................................................................ .......................................................................................................
.......................................................................................... ......................................................................................................
................................................................................................... .......................................................................................... .......................................................................................... .........................................................................................
............................................................................. ........................................................................................
...................................................................................... .............................................................................
..................................................................................... ....................................................................................
....................................................................... ...................................................................................
................................................................................. .......................................................................
......................................................................................... ......................................................................................
...................................................................................................................................................................................

..................................................................................................... ..............................................................................................
................................................................................... .........................................................................
........................................................................................... ...................................................................................................
....................................................................................... .........................................................................................................
....................................................................................................... .................................................................................................
...................................................................................... ........................................................................................................
........................................................................................................................ ................................................. ................................................
........................................................................................................ ............................................................. ............................................................
............................................................................. .........................................................................
.............................................................................. ...........................................
.................................................................................................................. ............................................................................... ...............................................................................
................................................................................. ..............................................................................
................................... .....................................
....................... ............................................................................................................................
.......................
................................................................................................................................
................................................................................................................................
....................................................................................................................... ...............................
...................................................................... ........................................................................ ...................................................................... .....................................................................
...................
.................................................................................... ..................................................................................
........................................................................................................... .............................................................................
.............................. .................................. ................................
............................................... ..............................................
........................................................

..................................................................... ...............................................
......................................................................................... .......................................................................... .........................................................................
............................................................................ ..........
..........................................................................................
.................................................................................................. ................................................................................................................
.................................................................................................. .....................................................................................................
................................................................................................ ........................................................................................
.......................................................................................................... ...........................................................................................................
...............................................
.............. ...............
......................................
..................................................................................................................................
.................................................................................................................................. ...............................................................................................................
..........................................................................................
......................................................................................................
...................................................................................................... .....................................................
....................................... ......................................................................
........................... .................................................................................................
...................................................................................................
...............................................................................................................
...................................................................................................
..................................................................................................................
.......................................................................
..................................................
.....................................
...................................................................................................................
...................................................................................................................

.....................................................................................
...................................................................................................................
..
..... ....................................................
............................................................. ...................................................................................................
........................................................................................................ .....................................................................................................
....................................................................................................... ....................................................................................................
............................. ..........................
.........................................................................................................................
......................................................................................................................... ................
.............
...............................................................................................................
.............................................................................................. ...........................................
........................................ ...............................
................................................................................................ .............................................................................................
................................................................................................... ................................................................................................
............................................................................................ ..........................................................
........................................................................................................... ................................................................................................................
....................................................................................... ...................................................................................................
............................................................................................... .................................................................................
.......................................................... ........................................................
................................................................................................ .............................................................................................
................................................................................................... .................................................................................................
................................................................................... ................................................................................
....................................................................................... ....................................................................................

.................................................................................. ...............................................................................
...................................................................................... ...................................................................................
............................................ .........................................
....................................................................................................... .....................................................................................................
........................................................................................... ......................................................................................................
........................................................................................... .............................................................................................................
........................................................................................................................ ....................................................................................
......................................................................... ...........................................................................................
........................................................................................................... ...............................................................................................
.................................................................................... ......................................................................................................
................................................................................ ...................................................................
........................................................................... ..............................................................
................................................................ ...................................................
................................................................................. .....................................................................
............................................................................... ...................................................................
.......................................................................... ..............................................................
............................................................... ..................................................
................................................................................ ....................................................................
................................................................................ ....................................................................................
......................................................................... ..........................................................................................
............................................................................................... .........................................................................
.............................................................. ................................................................................
........................................................................................ ............................................................................

.............................................................................................. ............................................................................................
...................................................................................... ...........................................................................
............................................................................................. ............................................................................................................
...................................................................................... ..........................................................................................................................
....................................................
................................................................................. .............................................
..................................................................................................... ..........................................................................................
....................................................................................... ...................................................................................
...................................... ............................................................................
................................................................................. ......................................
.................................................................................................... ................................................................
.................................................................. ..............................
...................... ......................
.................. ..................
........................................... ..................................
............................................................................. ..........................................................................................................
...................................................................................................... ........................................................................
.........................................................................................
......................................................................................................
...................................................
................................................................................

......................................................................... ...............................
........................................ ............
.................................................................... ................................................................
.................... ..............................
.. ...............................................
................................................. ..................
...................................................................................... .....................................................
....................................... ....................................
.......................................................... ...........................................................................................................
............................................................................................... .....................................................
............................................................................ ..............................................................
...................................... .......
............................................................................. ..........................
..................................................................................... ...............................................................
......................................................... ......................................................
............................................................. ..........................................................
.............................................................................. ........................................................................................................... .........................................................................................................
......................................................................................................
................................................................... .....................................
.................................. .................................................
...................................................................................



Useful information at your fingertips
Copyright © 2016 Delta Dental. All rights reserved.HL_DCU_SHELL_EN #92056M (rev. 7/16) E
Administered by:Delta Dental Insurance Company 1130 Sanctuary Parkway Alpharetta, GA 30009
Online: Visit deltadentalins.com/about/contact/contactUs_ddic.html and choose the “DeltaCare USA Customer Service” form.
Write to:Delta Dental Insurance Company 1130 Sanctuary Parkway Alpharetta, GA 30009
Call toll-free: 800-422-4234 Customer Service agents are available Monday through Friday, 8 a.m. to 9 p.m., Eastern time. Or, use our automated phone system, available 24/7.
NOTE: This is only a brief summary of your plan.This brochure is not intended to replace your legally required plan booklet. The Group Dental Service Contract determines the exact terms and conditions of your coverage. Please refer to the “Description of Benefits and Copayments” and “Limitations and Exclusions of Benefits” in this brochure for a complete list of covered procedures, copayments, plan limitations and exclusions. You may also consult your Evidence/Certificate of Coverage, which will be mailed to you upon enrollment. If you wish to review an Evidence/Certificate of Coverage prior to enrollment, you may request a copy by calling Customer Service at 800-422-4234.
Check out our SmileWay® Wellness programFind oral health resources, including a risk self-assessment tool, quizzes, articles, videos and a subscription to Grin!, our free dental wellness e-magazine, at mysmileway.com.
Find a network dentist near youUse our convenient “Find a Dentist” tool and select DeltaCare USA as your network.
• Find a dentist near your home or office
• Narrow your search by location, specialty,languages spoken — and more
Sign up for an online accountUse your mobile device or desktop to sign up for a free, secure Online Services account.
• Review your plan benefits
• Access your ID card
Contact usNeed help? Let us know.

Exhibit D PPO Dental Administrative Services Contract

Exhibit D











































Exhibit E FSCJ 12.31.18 Actuarial Memo

March 29, 2019
Mr. Daniel Keating, FSA, MAAA Life and Health Product Review Florida Office of Insurance Regulation 200 East Gaines Street Tallahassee, FL 32399-0328
Re: Florida State College at Jacksonville Dental Fund Section 112.08 Report for Plan Year 1/1/2018 to 12/31/2018
Dear Mr. Keating:
The purpose of this letter is to present the results of our review of the self-funded dental benefit plan of Florida State College at Jacksonville (FSCJ) in accordance with Section 112.08 F.S.
In the plan year 2015, FSCJ opted to fully insure their medical and prescription drug coverage. Since dental plan alone remains to be self-funded, this reporting contains only dental reserves and projections.
The plan had an actual operating gain of $67,806 (after considering IBNR liabilities) for FY 2018, and we project a slight operating loss of ($1,281) for FY 2019. As shown in Form OIR-B2-573, this results in a projected surplus of $436,765 as of the end of FY 2019.
The IBNR Claims Reserve was developed based on a claim lag study using the most recent 24 months of incurred and paid claim experience. For the months of November 2018 and December 2018, the level of incurred claims was developed using an estimate of PMPM claims as opposed to utilizing the calculated completion factors. See the following exhibits which have been attached to this report:
Exhibit 1: Claim triangle and enrollment by month Exhibit 1A: Exhibit that illustrates the development of the IBNR reserve by incurral month.
Based on the accumulated surplus, it is our opinion that the Fund is actuarially sound at this time. If you have any questions please do not hesitate to contact us.
Sincerely,
Kirk Braunius, ASA, MAAA Senior Consulting Actuary
cc: Debbie Monnseratt, FSCJ
Exhibit E

Florida State College At Jacksonville EXHIBIT 1A
Plan Year January 1, 2018 - December 31, 2018
Dental
Month Of Projected Incurred Calculated
Development Incurred and Paid Completion Factor Projected PEPM Claims 1 IBNR
(1) (2) (3) (3a) (4)=(2)/(3) (5)=(4)-(2)
11 $76,127 1.0000 N/A $76,127 $0
10 $78,762 1.0000 N/A $78,762 $0
9 $74,554 0.9998 N/A $74,566 $12
8 $61,451 0.9993 N/A $61,491 $41
7 $63,528 0.9983 N/A $63,633 $105
6 $55,314 0.9968 N/A $55,489 $175
5 $59,280 0.9934 N/A $59,672 $392
4 $62,108 0.9862 N/A $62,976 $868
3 $42,358 0.9778 N/A $43,320 $962
2 $58,252 0.9659 N/A $60,311 $2,059
1 $50,261 0.8111 $28.56 $61,965 $11,704
0 $28,222 0.4544 $28.67 $62,103 $33,882
TOTAL $710,216 0.9340 $760,415 $50,199
Margin (5%) $2,510
Total with margin $52,709
03/22/19
201812 FSCJ#3
1 For month 0 and month 1, the projected incurred claims was calculated by multiplying the projected PEPM claim amount by
the level of monthly enrollment.

Florida State College At Jacksonville EXHIBIT 1
Dental Claim Lag Report
Incurred
Month Total Paid
Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 (1) Enrollment
Jan-17 0 0 0 104 205 0 0 0 0 0 75 0 0 0 0 0 0 0 384 2,214
Feb-17 28 0 0 149 0 0 0 0 0 0 468 0 0 0 0 0 0 0 645 2,239
Mar-17 455 119 576 156 918 0 0 0 0 0 0 0 0 0 0 0 0 0 2,224 2,228
Apr-17 550 206 192 574 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1,522 2,229
May-17 2,094 1,278 269 318 0 55 0 0 0 0 0 0 0 0 0 0 0 0 4,014 2,221
Jun-17 26,325 1,258 287 770 352 192 418 12 0 0 0 0 0 0 0 0 0 0 29,613 2,215
Jul-17 26,451 21,063 3,429 491 (121) 0 214 162 918 80 0 0 540 0 0 0 0 0 53,228 2,189
Aug-17 0 30,790 16,832 5,717 915 395 770 739 111 0 1,190 58 0 0 0 0 0 0 57,516 2,192
Sep-17 0 0 17,179 14,238 2,233 388 1,321 684 0 0 60 0 0 0 575 0 0 0 36,677 2,167
Oct-17 0 0 0 26,178 18,137 3,412 855 124 146 114 0 882 0 0 0 0 0 0 49,847 2,166
Nov-17 0 0 0 0 26,579 21,159 2,207 1,176 487 0 0 55 0 0 543 0 0 0 52,207 2,171
Dec-17 0 0 0 0 0 33,105 27,450 864 222 642 1,500 0 0 0 0 37 0 0 63,819 2,173
Jan-18 0 0 0 0 0 0 50,186 20,201 2,911 1,480 578 32 238 0 275 0 0 227 76,127 2,228
Feb-18 0 0 0 0 0 0 0 51,221 24,324 1,939 1,223 0 0 55 0 0 0 0 78,762 2,234
Mar-18 0 0 0 0 0 0 0 0 37,474 28,644 5,179 618 371 1,544 369 0 355 0 74,554 2,222
Apr-18 0 0 0 0 0 0 0 0 0 28,519 27,073 2,869 2,328 58 255 349 0 0 61,451 2,219
May-18 0 0 0 0 0 0 0 0 0 0 39,523 18,229 2,040 649 1,904 0 1,183 0 63,528 2,215
Jun-18 0 0 0 0 0 0 0 0 0 0 0 35,295 17,479 2,216 251 73 0 0 55,314 2,218
Jul-18 0 0 0 0 0 0 0 0 0 0 0 0 26,416 29,437 992 817 991 627 59,280 2,202
Aug-18 0 0 0 0 0 0 0 0 0 0 0 0 0 39,515 21,222 1,134 238 0 62,108 2,189
Sep-18 0 0 0 0 0 0 0 0 0 0 0 0 0 0 23,450 18,419 501 (11) 42,358 2,163
Oct-18 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 41,347 14,018 2,888 58,252 2,165
Nov-18 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 30,418 19,843 50,261 2,170
Dec-18 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 28,222 28,222 2,166
TOTAL 55,903 54,714 38,763 48,696 49,217 58,705 83,421 75,181 66,593 61,417 76,869 58,037 49,412 73,474 49,834 62,175 47,704 51,796 1,061,911

March 29, 2019
Mr. Daniel Keating, FSA, MAAA Life and Health Product Review Florida Office of Insurance Regulation 200 East Gaines Street Tallahassee, FL 32399-0328
Re: Florida State College at Jacksonville Dental Fund Section 112.08 Report for Plan Year 1/1/2018 to 12/31/2018
Dear Mr. Keating:
Attached is our review of the self-funded dental benefit plan of Florida State College at Jacksonville (FSCJ) in accordance with Section 112.08 F.S.
In my opinion, the fund is actuarially sound based on the amount of surplus. In addition, the level of funding is generally consistent with actual expenses.
Please advise if you have any questions or want to discuss.
Sincerely,
Kirk Braunius, ASA, MAAA
Enclosures
cc: Debbie Monnseratt, FSCJ (with enclosure)

Florida State College At Jacksonville
General Information On Self-Funded Health Benefit Plans
Plan Fiscal Year 1/1/2018 - 12/31/2018
Plan Name Florida State College At Jacksonville
Individual Contact Ms. Debbie E. Monnseratt
Address 501 West State Street
Jacksonville, Florida 32202-4030
Fax Number (904) 632-3109
Phone Number (904) 632-3166
E-Mail Address [email protected]
Administrator Delta Dental Insurance Company
Individual Contact Angela Bevis, Account Manager, Sales & Marketing
Address 258 Southhall Lane, Suite 350
Maitland, FL 32751
Fax Number
Phone Number (904) 230-6944
E-Mail Address [email protected]
Actuarial Firm Merlinos & Associates, Inc.
Actuary Kirk Braunius, ASA, MAAA
Address 3274 Medlock Bridge Road
Peachtree Corners, Georgia 30092
Fax Number (770) 453-9776
Phone Number (678) 684-4855
E-Mail Address [email protected]
OIR-B2-570 03/22/19
Rev. 12 201812 FSCJ#3
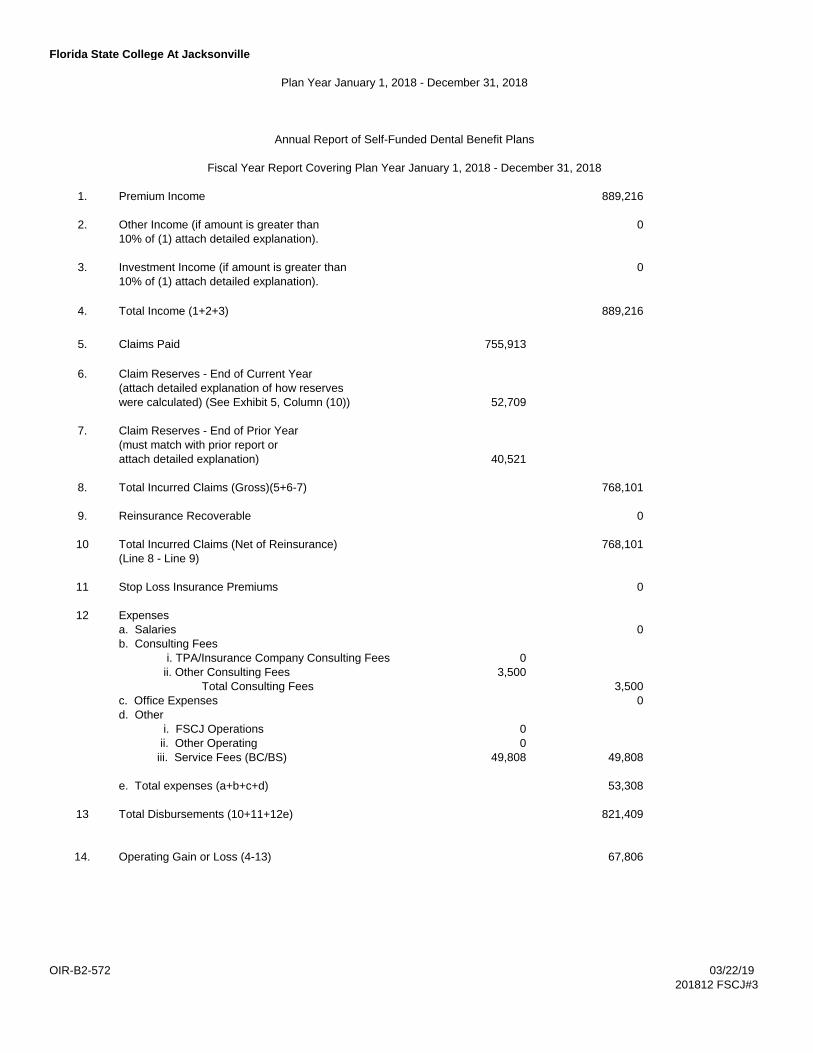
Florida State College At Jacksonville
Plan Year January 1, 2018 - December 31, 2018
Annual Report of Self-Funded Dental Benefit Plans
Fiscal Year Report Covering Plan Year January 1, 2018 - December 31, 2018
1. Premium Income 889,216
2. Other Income (if amount is greater than 0
10% of (1) attach detailed explanation).
3. Investment Income (if amount is greater than 0
10% of (1) attach detailed explanation).
4. Total Income (1+2+3) 889,216
5. Claims Paid 755,913
6. Claim Reserves - End of Current Year
(attach detailed explanation of how reserves
were calculated) (See Exhibit 5, Column (10)) 52,709
7. Claim Reserves - End of Prior Year
(must match with prior report or
attach detailed explanation) 40,521
8. Total Incurred Claims (Gross)(5+6-7) 768,101
9. Reinsurance Recoverable 0
10 Total Incurred Claims (Net of Reinsurance) 768,101
(Line 8 - Line 9)
11 Stop Loss Insurance Premiums 0
12 Expenses
a. Salaries 0
b. Consulting Fees
i. TPA/Insurance Company Consulting Fees 0
ii. Other Consulting Fees 3,500
Total Consulting Fees 3,500
c. Office Expenses 0
d. Other
i. FSCJ Operations 0
ii. Other Operating 0
iii. Service Fees (BC/BS) 49,808 49,808
e. Total expenses (a+b+c+d) 53,308
13 Total Disbursements (10+11+12e) 821,409
14. Operating Gain or Loss (4-13) 67,806
OIR-B2-572 03/22/19
201812 FSCJ#3

Florida State College At Jacksonville
Plan Year January 1, 2018 - December 31, 2018
Operating Projections For Self-Funded Dental Benefit Plans
Fiscal Year Report Covering January 1, 2019 Through December 31, 2021
Current Year Year 1 Year 2
1. Number of Employees 1,306 1,306 1,306
2. Premium Income 816,719 857,555 900,433
3. Other Income 0 0 0
(includes Investment Income)
4. Total Income (2+3) 816,719 857,555 900,433
5. Total Incurred Claims 764,350 802,568 842,696
(Net of Reinsurance)
6. Total Expenses 53,650 54,653 55,676
7. Total Disbursements (5+6) 818,000 857,221 898,372
8. Total Gain or Loss (4-7) (1,281) 334 2,061
9. Change in Surplus Due to Other 0 0 0
Factors (contribution,withdrawal)
10. Surplus beginning of year 438,046 436,765 437,100
11 Surplus end of year (8+9+10) 436,765 437,100 439,160
Assumptions Current Year Year 1 Year 2
1. Percent Premium Increase -6.7% 5.000% 5.000%
2 Trend - Dental 5.0% 5.0% 5.0%
Expense 2.0% 2.0% 2.0%
3 Premium Contribution (Monthly)
Single $35.55 $37.33 $39.20
Family $80.17 $84.18 $88.38
Local Governmental Unit $35.55 $37.33 $39.19
4 Stop Loss Minimum Attachment n/a n/a n/a
Point
OIR-B2-573 03/22/19
Rev. 12/03 201812 FSCJ#3

Florida State College At Jacksonville
Plan Year January 1, 2018 - December 31, 2018
General Information
Benefit Benefit Benefit
(a) (b) (c)
1. Type of benefit Dental
2. Number of covered employees 1,326
Single (Employee only) 830
Family (Employee and Dependents) 496
3 Claims Incurred 768,101
4 Annual Claim Cost per Employee (Line3/Line2) 579
Surplus Statement
1. Surplus from prior year 1 $354,552
(If a deficit, show as negative surplus)
2. Change in Surplus from Fund Operations $67,806
(Gain or Loss for Year From DI4-572, Line 14)
3. Change in Surplus Due to Other Factors 2 $15,688
(Contribution, Withdrawal)
4 Overall Change in Surplus, Present Year $83,494
(Sum of Line 2 and Line 3)
5 Surplus, End of Current Year $438,046
(Sum of Line 1 and Line 4)
NOTE
OIR-B2-574 03/22/19
201812 FSCJ#3
2 This is an adjustment to reconcile with the FSCJ financial statements.
3 If line 5 is negative, the plan is not in good standing with the Florida Office of Insurance Regulation. This deficit must be removed by
an infusion of an amount at least equal to the deficit. If the deficit is to be liquidated over a period of time, please provide the details of
this program for consideration, along with a supporting actuarial opinion. If the Plan's surplus is less than sixty days of anticipated
claims, other questions may be asked of the Plan as the Office sees fit.
1 This is the dental plan surplus in the beginning of the period, after removing the surplus amount associated with the FSCJ medical
plan.





























