Embed Size (px)
Citation preview

Adaptive Radiotherapy for HN Cancer: Technical Aspects
Di Yan, D.Sc, FAAPM
Beaumont Health System Michigan, USA
Status of ART in the Clinic

Clinical rationales of ART for HN caner
ART technologies & implementation in imaging, feedback & planning modification
Practical issues of ART in clinical operation
Learning Objectives

Significant normal tissue toxicities have been caused by the large treatment volume, and organ over dose during the treatment delivery due to
• Patient/organ position & volume variations
• Cavity shape variation (induced hot-spot on mucosa)
• Neck and shoulder flexing in treatment setup
• Shrinkage of large tumor & edema resolving
Can online anatomical image (CBCT, CT, MRI) guided ART reduce normal tissue toxicities?
HN Cancer ART: Clinical Rationales

Patie
nt/O
rgan P
ositio
n V
aria
tion

Org
an V
olu
me/D
ose V
aria
tions

Organ Dose Variations during the Treatment
Left Poratid: Cumulative Dose (Dmean) Variation
0
2
4
6
8
10
12
14
-15% -10% -5% 0% 5% 10% 15% 20% 25%
%Dose Variation (Delived - Planned)
No
of
Pa
tien
ts
Right Poratid: Cumulative Dose (Dmean) Variation
0
2
4
6
8
10
12
14
-5% 0% 5% 10% 15% 20%
%Dose Variation (Delived - Planned)
No
of
Pa
tie
nts
Cord: Cumulative Dose (Dmax) Variation
0
2
4
6
8
10
12
-6% -4% -2% 0% 2% 4% 6% 8% 10%
%Dose Variation (Delived - Planned)
No
of
Pa
tie
nts

Systematic approach to escalate or deescalate treatment dose based on spatial tumor cell bio-activities, such as
• Biological image markers to determine the most resistant tumor cells, which include
o PET; MRI: pre-treatment image, as well as the imaging of early treatment response
o spatial bio-parametric distribution in the planning objectives for dose painting
Can biological image guided (PET, MRI) ART be used to select patients, and improve their tumor control & long term survival?
HN Cancer ART: Clinical Rationales

Imaging (CBCT/CT-in-room), Feedback & Adaptation
1. Pre-treatment Simulation & Planning
Standard CT simulation & IMRT planning
0~5mm CTV-to-PTV margins & 5~7 beams
Planning CT image w/wo pre-selected bony
structures (adjacent to the target, C2-C5)
selected as the reference for daily treatment
localization & correction
Segmentation (commercial tools for auto-
segmentation), inverse planning, evaluation &
QA: 2~4 days
HN Cancer ART: Clinical Implementation

2. Daily CBCT/CT-in-room Localization & Correction
Pre-treatment CBCT/CT imaging for patient at the treatment position (~2 mins)
Bony (C2-C5) registration to the reference image by using the pre-selected bony structure (2~5 mins)
Couch translational correction (1~2 mins)
Imaging/registration/correction (commercial tools): 5~9 mins per treatment
Post-treatment image: once a week for QA purpose
HN Cancer ART: Clinical Implementation

Daily Treatment Localization

3. Daily/Weekly Treatment Evaluation and QA
Patient/organ position/volume/dose evaluation
(2~4hrs per week per patient)
Non or few commercial tools with very limited
functions at the present time can be applied for
this task
Technologies:
o CBCT-to-CT deformable image registration
o Organ position & volume variation quantification
o Daily CBCT density mapping & dose calculation
o Daily & cumulative treatment dose construction
HN Cancer ART: Clinical Implementation
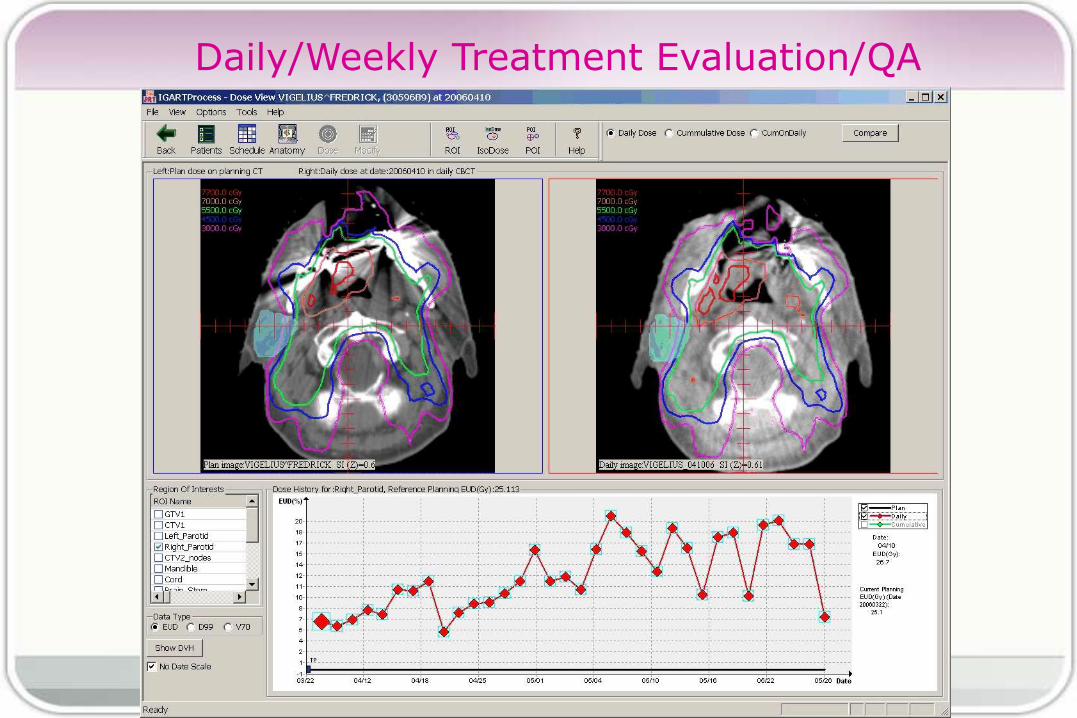
Daily/Weekly Treatment Evaluation/QA

4. New CT Simulation (after the first 10 and/or 20 treatment days)
New mask if necessary
Delineate targets and ROIs on the new CT image (auto propagation from the pre-treatment plan)
The new CT image will be used in the planning modification, and as the new reference image for the rest of daily image guidance
1~2 working days depending on the level of automation in segmentation & planning
This step could be replaced using the daily CBCT directly in future
HN Cancer ART: Clinical Implementation

5. IMRT Re-planning or Adaptive Inverse Planning
Re-planning on the new CT image (1~2 days)
o on a commercial planning system
o the initial planning objectives, constraints &
weights can be used as the guidelines
Adaptive inverse planning by including all daily
CBCT images obtained during the last week,
o organ variations in the objectives of inverse
planning optimization
o Auto-planning & evaluation (1~2 days)
HN Cancer ART: Clinical Implementation

Technical Issue: Deformable Image Registration
DVF
Mesh Structure

Technical Issue: Organ Variation Characterization
Patient 2 Patient 1
0
2
4
6
8
10
0 5 10 15 20 25 30 35Fraction #
Dis
pla
ce
me
nt (m
m)
Point 1
Point 2
Patient 3
L R

Technical Issue: Treatment Dose Construction
)ˆ),((|),ˆ),(()(|)( 11 jjKjjKKN vxvxdvDvD
Delivered dose Estimated dose
Expected Treatment Dose

Technical Issue: Adaptive Inverse Planning
kNkN
kN
k
DGDG
DFMax
ˆ||
|
1
1
1
“Expected Treatment Dose” in the objective & constraints
to determine the new or modified plan
* : Expected improvement from the previous treatment is used to
determine if “accepting the plan modification”

ART vs Conventional IMRT (5mm Target Margin)
0
10
20
30
40
50
60
70
80
CTV1
CTV2
Brain
_Stem
Cord
Man
dible
Left_
Parotid
Right
_Parotid
Org
an
Cu
mu
lati
ve
Do
se
(G
y)
PreTxPlan
FinalAdap
Improvement in Gy: 9.5+6 7.2+2 6.5+10 6.7+10 7.8+3
Dmax Dmax Dmax Dmean Dmean
Conventional IMRT
Weekly adaptation

Improvement of ART vs Clinical Efforts
0%
5%
10%
15%
20%
25%
30%
35%
40%
Brain_Stem Cord Mandible LP RP
% o
f re
du
cti
on
wrt
th
e P
re-T
x C
um
. Do
se
1 Adaptive Modification 2 Adaptive Modifications 3 Adaptive Modifications
4 Adaptive Modifications 5 Adaptive Modifications

‘Daily IGRT’ vs ‘Hybrid ART’
All treatment organ doses are normalized to the baseline IMRT plan with 0 target margin
T1: Daily IGRT with 0 target
margin
T2: Daily IGRT + two weekly replanning
T3: Daily IGRT + two adaptive planning
*Dose heterogeneity in targets could be a major concern

‘Daily IGRT’ vs ‘Hybrid ART’

Segmentation: 2~3 CTs and/or daily CBCTs
Manual: ~5 hrs per image
Auto + manual editing: 10 mins ~ 3 hrs per image
Planning: 2~3 times
Manual: 6 hrs per plan
Auto + manual modification: 30 mins ~ 4 hrs
Daily treatment position localization/correction
5~10 mins per fraction
Weekly volume/dose evaluation
2~5 hrs per week per patient
Who should do it in long term, Physicist or RTT?
Practical Issues (workload)

Decision of Modification: Cut-off value based on
Change of patient/organ volume?
Shrinkage of the target?
Patient weight loss?
Overdosing to a critical organ?
Hot-spots on oral mucosa?
Underdosing in targets?
OR
“Expected Improvement“ of organ dose-volume obtained from the adaptive plan candidate
Practical Issues

Treatment QA
Manual target delineated on the new CT could be quite different than the auto-one. How to add dose in the target?
Missing daily CBCT image
Increased clinical QA activity & error report
Workflow management: procedure tracking & notification
Proper documentation for billing
Practical Issues
Adaptive radiotherapy of HN cancer with daily image feedback & adaptive planning modification is feasible in the routine clinic
Significant improvement in normal tissue dose could be achieved by multiple weekly replanning, or optimized by adaptive inverse planning;
Average 10% ~ 18% improvement can be achieved for most of normal organs using a single adaptive modification
Average 15% ~ 29% improvement can be achieved using the weekly adaptive modifications
The main challenge in clinical implementation is now the lack of necessary software tools, and clinical workflow support
Summary

Acknowledgement
Technology R&D:
Jian Liang, PhD
Mattias Birkner, PhD
Yuwei Chi, PhD
An Qin, PhD
David Gerstein, MS
Tie Zhang, PhD
Clinical Development:
Shanna Martin, RTT
Jenni Wloch, RTT
Qian Liu, MS
Dan Krauss, M.D.
Peter Chen, M.D.
HN ART R&D has been supported by
Elekta; Philips