Embed Size (px)
Citation preview

ADAMS, CHAPTER 47
Drugs for Bone and Joint Disorders

ROLE OF CALCIUM IN ROLE OF CALCIUM IN MAINTAINING MAINTAINING HOMEOSTASISHOMEOSTASIS
Critical to proper functioning of the nervous, muscular, and cardiovascular systems
Adequate levels in body necessary to:
• Transmit nerve impulses• Prevent muscle spasms• Provide stability and movement

ROLE OF CALCIUM IN ROLE OF CALCIUM IN MAINTAINING MAINTAINING HOMEOSTASISHOMEOSTASIS
Also important for blood coagulation and myocardial activity
To maintain homeostasis:
• Calcium balance in the body is regulated by parathyroid hormone (PTH)

ROLE OF CALCIUM IN ROLE OF CALCIUM IN MAINTAINING MAINTAINING HOMEOSTASISHOMEOSTASIS
Parathyroid—Secretes PTH
• Stimulates osteoclasts• Accelerates bone resorption• Causes breakdown of bone• Consequently, calcium increases in blood• Calcium ion influences the excitability of all neurons

RECOMMENDED DIETARY RECOMMENDED DIETARY ALLOWANCE (RDA) OF ALLOWANCE (RDA) OF CALCIUMCALCIUM
For adults RDA is 800–1200 mg/day
Increased amounts of calcium required for:
• Pregnant women• Growing children • Menopausal women

RECOMMENDED DIETARY RECOMMENDED DIETARY ALLOWANCE (RDA) OF ALLOWANCE (RDA) OF CALCIUMCALCIUM
Normal serum calcium range is 4.5–5.5 mEqL or 8.5–10.mg/dl.
Serum calcium levels exceeding 5.5 mEq/L result in hypercalcemia.
Hypocalcemia results from serum calcium levels below 4.5 mEq/L

ROLE OF CALCIUM IN ROLE OF CALCIUM IN MAINTAINING MAINTAINING HOMEOSTASIS HOMEOSTASIS
Too high (hypercalcemia) calcium levels lead to:
• Decreased sodium permeability across cell membranes—a dangerous state
Too low (hypocalcemia) calcium levels cause:
• Cell membranes to become hyperexcitable• Convulsions or muscle spasms

ROLE OF PARATHYROID ROLE OF PARATHYROID HORMONE IN CALCIUM HORMONE IN CALCIUM BALANCEBALANCE
Control of calcium by the endocrine system begins in the parathyroid gland
The parathyroid secretes parathyroid hormone (PTH)
PTH stimulates osteoclasts and accelerates bone resorption
As a result, calcium increases in the blood

CALCITONINCALCITONIN
Increases bone density and reduces the risk of vertebral fractures

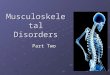
ROLES OF PARATHYROID HORMONE AND ROLES OF PARATHYROID HORMONE AND CALCITONIN IN CALCIUM BALANCECALCITONIN IN CALCIUM BALANCE
Calcitonin, secreted by the thyroid gland, stimulates bone deposition
This removes calcium from the blood
Together PTH and calcitonin control calcium homeostasis
PTH and calcitonin influence three targets: bones, kidneys, and gastrointestinal tract

FIGURE 47.1 (A) PARATHYROID HORMONE (PTH)
continued on next slide

FIGURE 47.1 (B) CALCITONIN ACTION

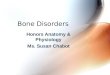
ROLE OF VITAMIN D IN ROLE OF VITAMIN D IN CALCIUM BALANCECALCIUM BALANCE
Vitamin D is necessary for effective absorption of calcium
Vitamin D is synthesized from precursor molecules
Cholecalciferol is converted to an intermediate form, calcifediol
Then it is metabolized to calcitriol (the active form of vitamin D)

FIGURE 47.2 PATHWAY FOR VITAMIN D ACTIVATION AND ACTION

OSTEOPOROSISOSTEOPOROSIS
Most common metabolic bone disease
Responsible for 1.5 million fractures per year
Related to bone deterioration—bone resorption outpaces bone deposition
• Lack of dietary calcium and vitamin D• Disrupted bone homeostasis

FIGURE 47.3 CALCIUM METABOLISM IN OSTEOPOROSIS

RISK FACTORS FOR RISK FACTORS FOR OSTEOPOROSISOSTEOPOROSIS
Onset of menopause: most common risk factor
High alcohol or caffeine consumption
Anorexia nervosa
Tobacco use
Physical inactivity
Testosterone deficiency
Lack of vitamin D or calcium
Drugs that lower calcium in blood
• Corticosteroids, anticonvulsants, immunosuppressants

PHARMACOTHERAPY OF PHARMACOTHERAPY OF OSTEOPOROSISOSTEOPOROSIS
Calcium supplements and vitamin D
Bisphosphonates
Estrogen receptor modulators
Calcitonin
Slow-release calcium fluoride
Statins
Hormone replacement therapy (HRT) no longer recommended

BISPHOSPHONATES FOR BISPHOSPHONATES FOR OSTEROPOROSISOSTEROPOROSIS
Most common treatment
Block bone resorption by inhibiting osteoclast activity, increase bone density

BISPHOSPHONATESBISPHOSPHONATES
Prototype drug: alendronate (Fosamax)
Mechanism of action: Lowers serum alkaline phosphate, an enzyme important to bone turnover
Primary use: for prevention and treatment of osteoporosis in postmenopausal women; for corticosteroid-induced osteoporosis; for osteoporosis in men; for Paget's disease
Adverse effects: diarrhea, nausea, vomiting, GI irritation, metallic- or altered-taste perception; pathologic fractures with long-term use

CALCIUM SALTSCALCIUM SALTS
Prototype drug: calcium salts
Mechanism of action: to return serum calcium levels to normal
Primary use: used to prevent and treat mild hypocalcemia; for osteoporosis; Paget's disease; chronic hypoparathyroidism, rickets, pregnancy, lactation, and rapid childhood growth
Adverse effects: hypercalcemia
• IV administration of calcium may cause hypotension, bradycardia, dysrhythmias, cardiac arrest

ROLE OF THE NURSE:ROLE OF THE NURSE:CALCIUM SUPPLEMENT CALCIUM SUPPLEMENT THERAPYTHERAPY
Assess for signs and symptoms of hypercalcemia such as:
• Drowsiness, lethargy, weakness, headache, • Anorexia, nausea, vomiting, thirst, and increased
urination

ROLE OF THE NURSE:ROLE OF THE NURSE:CALCIUM SUPPLEMENT CALCIUM SUPPLEMENT THERAPYTHERAPY
Obtain baseline and periodic vital signs, labs, and ECG
Assessment signs for hypocalcemia are facial twitching, muscle spasms, paresthesias, and seizures
Contraindicated in patients with a history of renal calculi, digoxin toxicity, dysrhythmias, or hypercalcemia
Investigate for history of fracture

VITAMIN D THERAPYVITAMIN D THERAPY
Primary use: for impaired kidney function or hypoparathyroidism
• Also useful in treating ricketsAdverse effects: hypercalcemia
• Headache, weakness, dry mouth, thirst• Increased urination, muscle or bone pain

VITAMIN D THERAPYVITAMIN D THERAPY
Prototype drug: calcitriol (Calcijex, Rocaltrol)
Mechanism of action: as active form of vitamin D
• Promotes intestinal absorption of calcium• Reduces bone resorption• Elevates serum levels of calcium

ROLE OF THE NURSE:ROLE OF THE NURSE:VITAMIN D THERAPYVITAMIN D THERAPY
Obtain a thorough history of current medications, vital signs
Complete a physical examination
Assess intake of fat-soluble vitamins, and current medications
Assess sclera, skin pigment, and bowel movements

ROLE OF THE NURSE:ROLE OF THE NURSE:VITAMIN D THERAPYVITAMIN D THERAPY
Provide education related to the prescribed drug treatment
Monitor lab studies:
• CBC, platelets, liver- and renal-function studies• Uric acid levels, and urinalysis• Magnesium and phosphate levels• Calcium and phosphate levels

SELECTIVE ESTROGEN RECEPTOR SELECTIVE ESTROGEN RECEPTOR MODULES (SERM) FOR OSTEOPOROSISMODULES (SERM) FOR OSTEOPOROSIS
Decrease bone resorption and increase bone density
May be either estrogen agonists or antagonists, depending on the drug or tissue involved

SELECTIVE ESTROGEN RECEPTOR SELECTIVE ESTROGEN RECEPTOR MODULATORS (SERMS)MODULATORS (SERMS)
Prototype drug: raloxifene (Evista)
Mechanism of action: Decreases bone resorption
• Increases bone mass and density by acting through estrogen receptor
Primary use: prevention of osteoporosis in postmenopausal women
Adverse effects: hot flashes, migraine headache, flu-like symptoms; endometrial disorder, breast pain, vaginal bleeding; may cause fetal harm when administered to pregnant women

OSTEOMALACIAOSTEOMALACIA
MBD characterized by softening of bones due to demineralization
Most frequent cause of osteomalacia is deficiency of vitamin D and calcium in the diet
Most prevalent in the elderly, in premature infants, and in individuals on strict vegetarian diets
If it occurs in children it is called rickets

OSTEOMALACIAOSTEOMALACIA
Signs and symptoms of osteomalacia include:
• Hypocalcemia, muscle weakness, muscle spasms• Diffuse bone pain, especially in the hip area
Classic signs of rickets in children include bowlegs and a pigeon breast.
• Children may also develop a slight fever and become restless at night.

PHARMACOTHERAPY OF PHARMACOTHERAPY OF OSTEOMALACIAOSTEOMALACIA
Calcium supplements and vitamin D
• Calcitriol is useful in treating rickets. • Calcitriol usually prescribed in combination with
calcium supplements.Recommendations
• Daily calcium and vitamin D• Adequate exposure to sunlight

OSTEOARTHRITISOSTEOARTHRITIS
Degenerative, age-onset disease
Characterized by wearing away of cartilage at articular joint surfaces
Symptoms
• Muscle spasms• Localized pain and stiffness• Joint and bone enlargement

OSTEOARTHRITISOSTEOARTHRITIS
Etiology poorly understood
• Thought to be due to excessive wear of weight-bearing joints
• Hip, knee, spine
Considered by some a normal part of aging

PHARMACOTHERAPY OF PHARMACOTHERAPY OF OSTEOARTHRITISOSTEOARTHRITIS
Goal is reduction of pain and inflammation
• Topical medications (capsaicin cream)• NSAIDs (including aspirin)• Acetaminophen

PHARMACOTHERAPY OF PHARMACOTHERAPY OF OSTEOARTHRITISOSTEOARTHRITIS
If OTC drugs don't succeed:
• Tramadol (Ultram)• Opiods with acetominophen• Sodium hyaluronate (Hyalgan) injections into joint

RHEUMATOID RHEUMATOID ARTHRITISARTHRITIS
Systemic autoimmune disorder
Characterized by inflammation of multiple joints
Autoantibodies (rheumatoid factors) activate inflammatory response in joints

RHEUMATOID RHEUMATOID ARTHRITISARTHRITIS
Other extra-articular systemic manifestations may develop: infections, pulmonary disease, pericarditis, blood abnormalities, metabolic dysfunction

PHARMACOTHERAPY FOR PHARMACOTHERAPY FOR RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
NSAIDs initially
Corticosteroids for severe inflammation
Disease-modifying antirheumatic drugs
Several months may be needed before therapeutic results are achieved

DISEASE-MODIFYING DISEASE-MODIFYING ANTIRHEUMATIC DRUGSANTIRHEUMATIC DRUGS
Prototype drug: hydroxychloroquine sulfate (Plaquenil)
Mechanism of action: Relieves severe inflammation of arthritis and lupus
• Mechanism of action not known

DISEASE-MODIFYING DISEASE-MODIFYING ANTIRHEUMATIC DRUGSANTIRHEUMATIC DRUGS
Primary use: for rheumatoid arthritis and lupus erythematosus
• For patients who have not responded well to other anti-inflammatory drugs
Adverse effects: anorexia, GI disturbances, loss of hair
• Possible ocular effects, headache• Mood and mental changes

GOUTGOUT
A form of acute arthritis characterized by buildup of uric acid in blood or joint cavities
Primary gout—hereditary defect in uric acid metabolism

GOUTGOUT
Secondary gout due to certain drugs or diseases that affect uric acid metabolism (diabetic ketoacidosis, kidney failure, leukemia, hemolytic anemia, others)

GOUTGOUT
Symptoms of acute attacks
• Red, swollen tissue• Often in big toes, ankles, fingers, wrists, knees,
elbowsTriggered by diet, injury, or other stress
Attacks often occur at night

PHARMACOTHERAPY OF PHARMACOTHERAPY OF GOUTGOUT
Goals: termination of acute attacks; prevention of future attacks
NSAIDs for pain and inflammation
Corticosteroids for more severe pain and inflammation
Uricosurics increase excretion of uric acid by blocking reabsorption in the kidney

PHARMACOTHERAPY OF PHARMACOTHERAPY OF GOUTGOUT
Prophylactic therapy:
• Drugs that inhibit formation of uric acid• Drugs that convert uric acid into a less toxic form

URIC ACID INHIBITORURIC ACID INHIBITOR
Prototype drug: alllpurinol
Mechanism of action: Inhibits synthesis of microtubules
• Subcellular structures responsible for helping white blood cells infiltrate area
Primary use: to reduce inflammation associated with acute gouty arthritis

URIC ACID INHIBITORURIC ACID INHIBITOR
Adverse effects: rashes, Stevens–Johnson syndrome, hypersensitivity syndrome, drowsiness, headache, vertigo, nausea, vomiting, abdominal discomfort, malaise, diarrhea, retinopathy, thrombocytopenia

ROLE OF THE NURSE: ROLE OF THE NURSE: DRUGS FOR GOUTDRUGS FOR GOUT
Obtain thorough history including current medications, vital signs
Complete a physical examination
Monitor lab studies
• CBC, platelets• Liver- and renal-function studies• Uric acid levels, urinalysis