Embed Size (px)
Citation preview

Acute AppendicitisAcute Appendicitis
Dr Moayad Ahmad LamberDr Moayad Ahmad Lamber
General surgeonGeneral surgeon
M.O.HM.O.H
3/6/20153/6/2015

AnatomyAnatomy
• It is a blind end muscular tube with mucosal , submucosal ,muscular and serosal layers.
• The lumen layered by colmnuar epithelium.
• Length 7.5- 10 cm
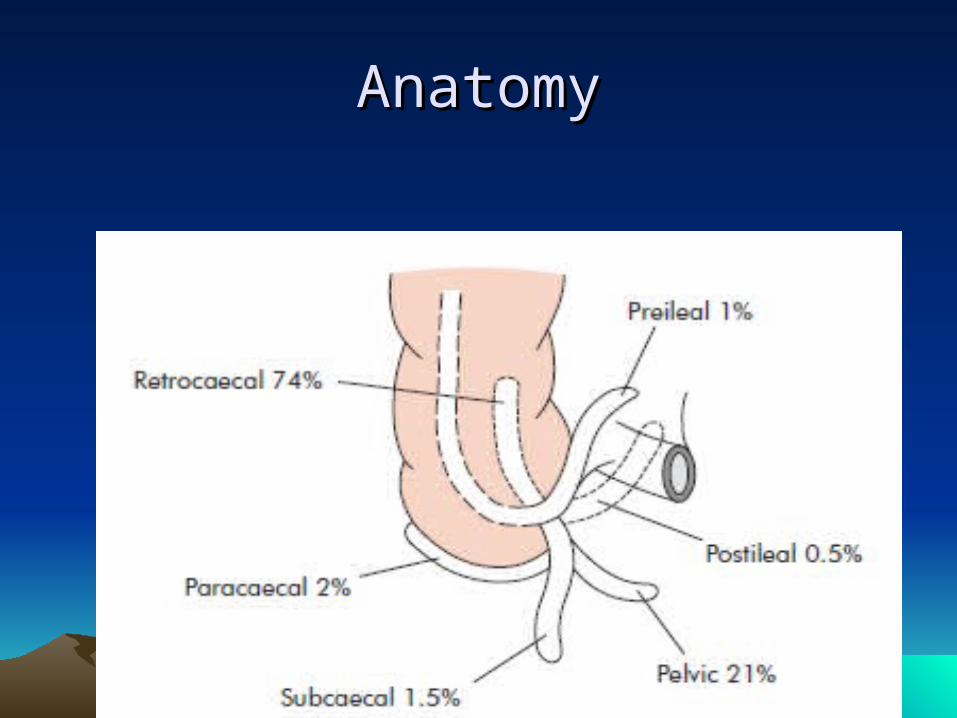
• Position most common retrocecal
• Base constant , confluence of the taenia coli
AnatomyAnatomy

AnatomyAnatomy
• Blood supply is by appendicular artery ,branch of the ilecolic artery , branch of SMA
• End artery
• Four , six or more lymphatic channels traverse the mesoappendics drain in the ilececal lymph nodes

AnatomyAnatomy

AetiologyAetiology
• Low fiber diet ? High sugar diet ?
• Luminal obstruction ( faecolith, sticture, lymphnode enlargment , tumor ,foreign body , pinwarms).
• Bacterial over growth within the lumen (mixed aerobic , anaerobic).

AetiologyAetiology
• Peak incidence in the teens and early 20S
• Rare in infants
• Male to female ratio 3:2 at age of 25 thereafter this declines
• Life time risk for appendectomy is 8.6 % for males and 6.7% for females .

pathologypathology
• Luminal obstruction with continues mucus secretion and inflammatory exudation increase intraluminal pressure , obstructing lymphatic drainage .
• Odema , mucosal ulceration , bacterial translocation to the submucosa.

pathologypathology
• Continues rise in pressure lead to venous obstruction and ischemia of the appendix wall .
• Ischaemic necrosis of the wall produce gangrene and peritonial contamination .
• Greater omentum and small bowel loops adhere to localize the inflammation .


Clinical diagnosisClinical diagnosis

Clinical diagnosisClinical diagnosis

Clinical diagnosisClinical diagnosis

Clinical diagnosisClinical diagnosis
• Special features according to position:
Retrocecal – rigidity is absent on deep pressure.
Pelvic – diarrhoea , tenderness may be absent , tendernesss on PR .
Postileal – pain may not shift , diarrhoea .

Clinical diagnosisClinical diagnosis
• Special features according to age
• Infants- rare , unable to give history , underdeveloped omentum.
• Children – vomiting , loss of appétit .
• Elderly – gangrene and perforation .
• Obese patient – obscure local signs , difficulty in operation.
• Pregnancy : most common surgical emergancy , fetal loss 3-5%, up to 20 %

Differential diagnosis Differential diagnosis




investigationinvestigation
DiagnosisDiagnosis
• CBC: the WBC is of limited value.
• C-Reactive Protien CRP and ESR have been studied with mixed results
DiagnosisDiagnosis
• UA: abnormal UA results are found in 19-40%
• Abnormalities include: pyuria, hematuria, bacteruria
• Presence of >20 wbc per field should increase consideration of Urinary tract pathology

TreatmentTreatment
• Appendectomy :- open
• - laprascopic
• Ivf
• Npo
• analgesia

Thank you





























