Embed Size (px)
Citation preview
Acute Versus Chronic DVT Imaging in the Vascular Lab
Heather Gornik, MD, RVT, RPVICleveland Clinic Heart and Vascular Institute
Heather L. Gornik, MD has the following relationships to disclose:
• CVR Global – Research support• FMD Society of America: Member, Medical Advisory
Board• IAC-Vascular testing: Member, Board of Directors

An Illustrative Case 46 year-old woman seen in consultation in vascular
medicine clinic for “coumadin failure”
1997: Right popliteal DVT while on OCPs treated with anticoagulation therapy x 6 months
1999: Right popliteal DVT + pulmonary embolism after minor GYN surgery. On warfarin x 12 months.
2010: History of recurrent Right popliteal DVT. On warfarin ever since with very good INR control
8/2011: Right leg aches after playing 18 holes of golf. Goes to local ER…
“Partially occlusive thrombus in the right popliteal vein”
What’s Going On Here?! Is this…..
A. Really a new popliteal DVT?
B. The same popliteal DVT reimaged by a different lab in a patient with the post-thrombotic syndrome (PTS)?
C. New thrombus on top of old thrombus?
D. Who knows!
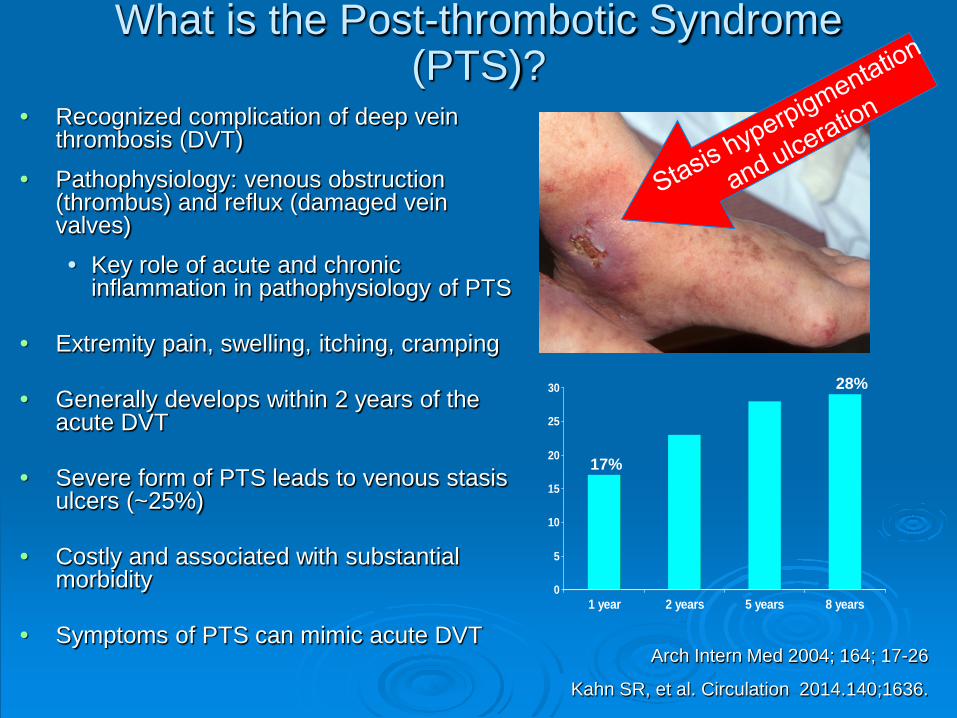
What is the Post-thrombotic Syndrome (PTS)?
• Recognized complication of deep vein thrombosis (DVT)
• Pathophysiology: venous obstruction (thrombus) and reflux (damaged vein valves)• Key role of acute and chronic
inflammation in pathophysiology of PTS
• Extremity pain, swelling, itching, cramping
• Generally develops within 2 years of the acute DVT
• Severe form of PTS leads to venous stasis ulcers (~25%)
• Costly and associated with substantial morbidity
• Symptoms of PTS can mimic acute DVTArch Intern Med 2004; 164; 17-26
Kahn SR, et al. Circulation 2014.140;1636.
0
5
10
15
20
25
30
1 year 2 years 5 years 8 years
17%
28%
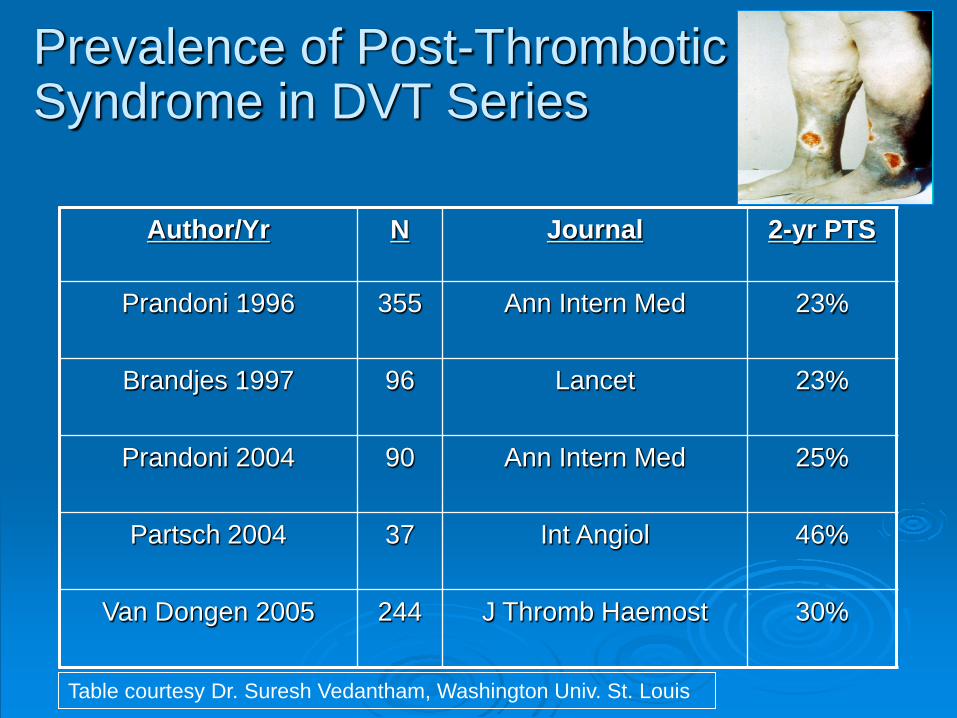
Prevalence of Post-Thrombotic Syndrome in DVT Series
Author/Yr N Journal 2-yr PTS
Prandoni 1996 355 Ann Intern Med 23%
Brandjes 1997 96 Lancet 23%
Prandoni 2004 90 Ann Intern Med 25%
Partsch 2004 37 Int Angiol 46%
Van Dongen 2005 244 J Thromb Haemost 30%
Table courtesy Dr. Suresh Vedantham, Washington Univ. St. Louis
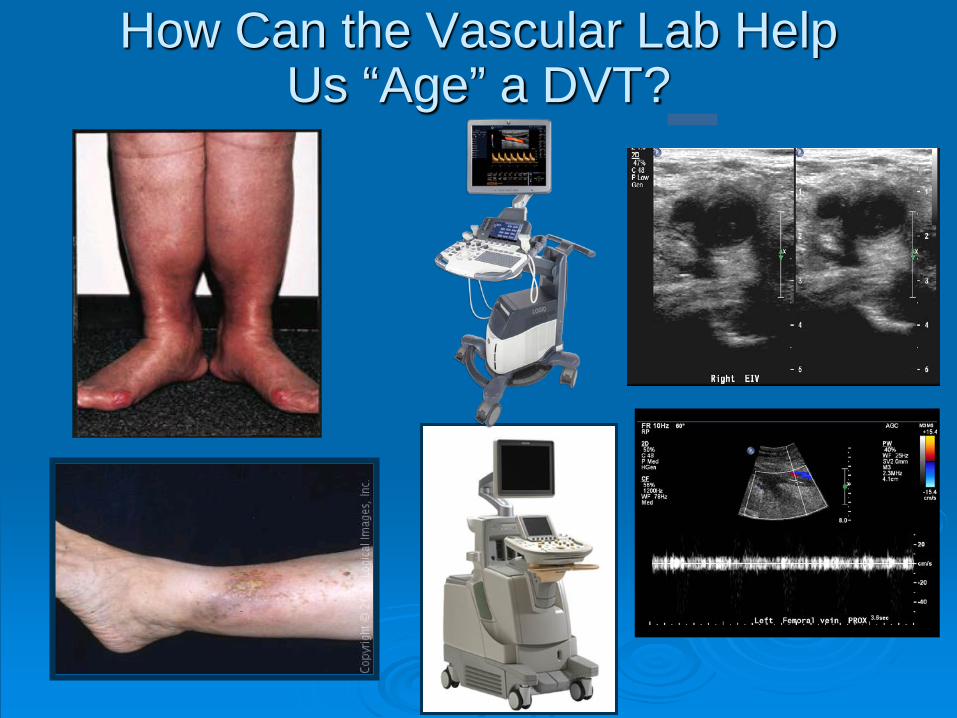
How Can the Vascular Lab Help Us “Age” a DVT?
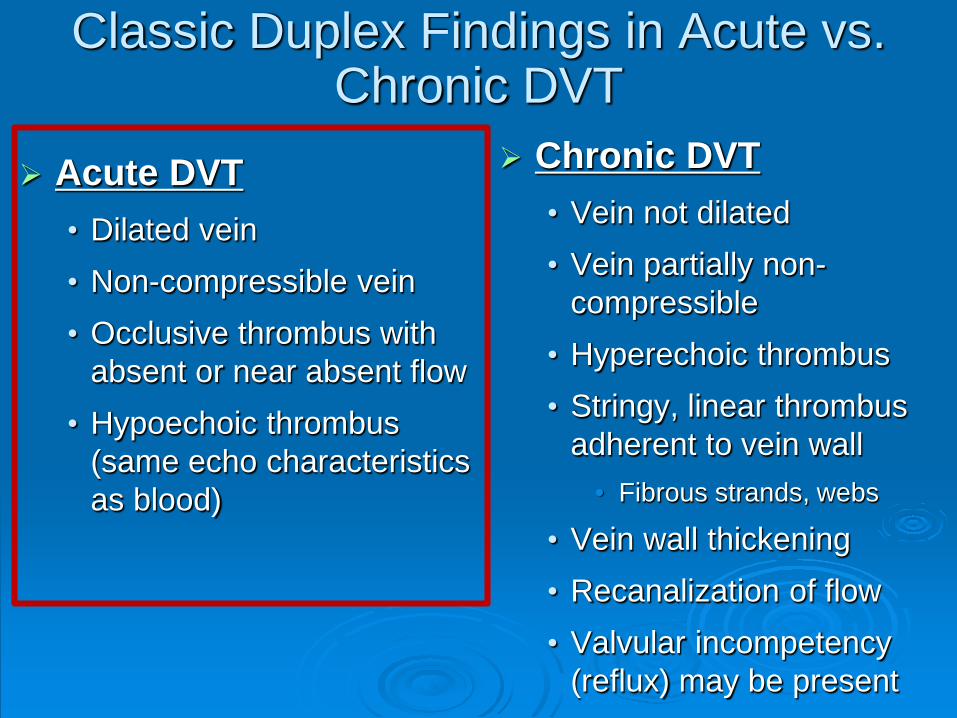
Classic Duplex Findings in Acute vs. Chronic DVT
Acute DVT• Dilated vein• Non-compressible vein• Occlusive thrombus with
absent or near absent flow• Hypoechoic thrombus
(same echo characteristics as blood)
Chronic DVT• Vein not dilated• Vein partially non-
compressible • Hyperechoic thrombus• Stringy, linear thrombus
adherent to vein wall • Fibrous strands, webs
• Vein wall thickening• Recanalization of flow• Valvular incompetency
(reflux) may be present
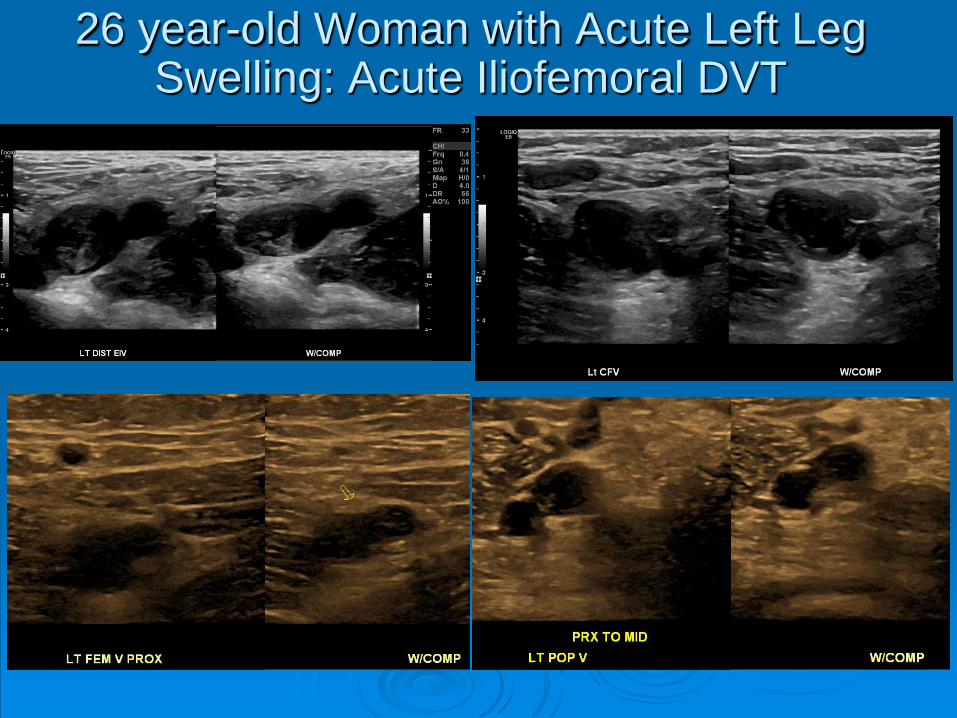
26 year-old Woman with Acute Left Leg Swelling: Acute Iliofemoral DVT
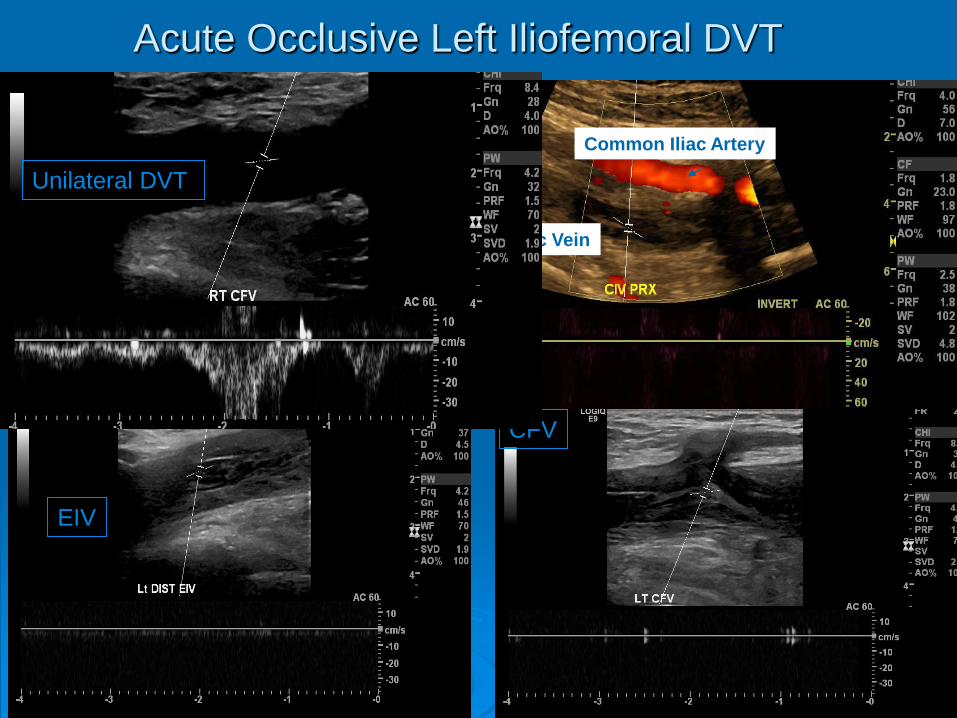
Acute Occlusive Left Iliofemoral DVT
CFV
EIV
Common Iliac Artery
Common Iliac Vein
CIV
Unilateral DVT
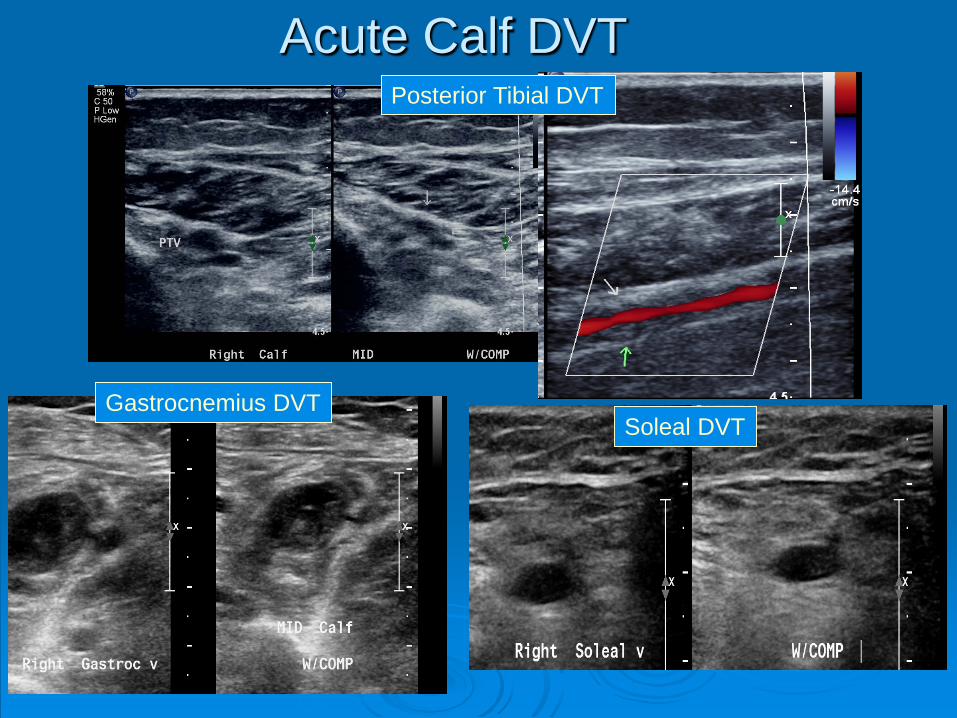
Acute Calf DVTPosterior Tibial DVT
Gastrocnemius DVTSoleal DVT
Classic Duplex Findings in Acute vs. Chronic DVT
Acute DVT• Dilated vein• Non-compressible vein• Occlusive thrombus with
absent or near absent flow• Hypoechoic thrombus
(same echo characteristics as blood)
Chronic DVT• Vein not dilated• Vein partially non-
compressible • Hyperechoic thrombus• Stringy, linear thrombus
adherent to vein wall • Fibrous strands, webs,
synechiae
• Vein wall thickening• Recanalization of flow• Valvular incompetency
(reflux) may be present
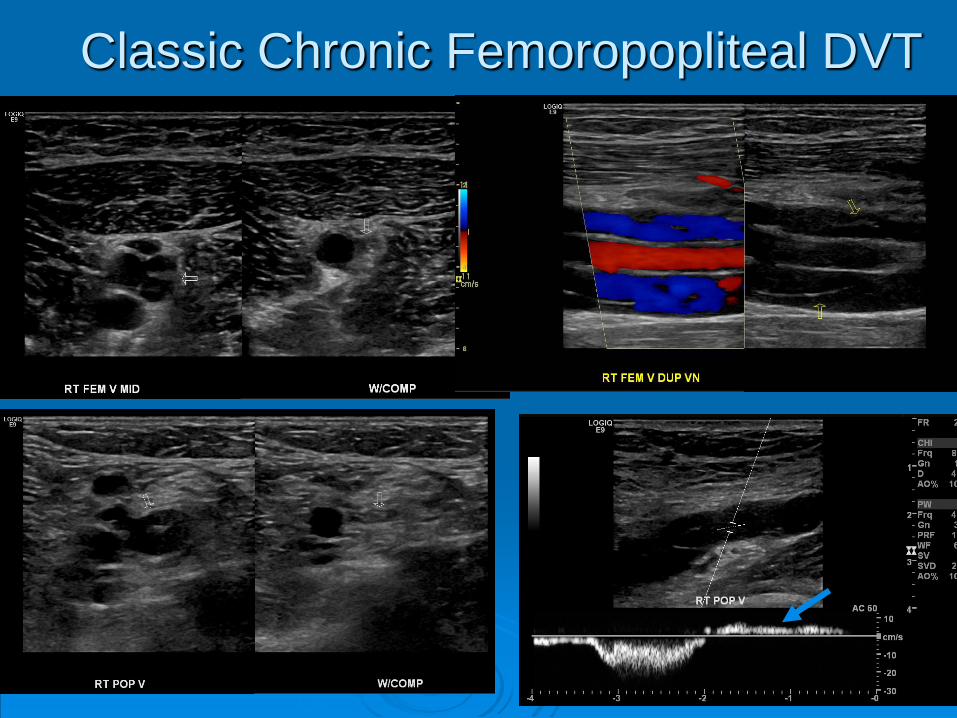
Classic Chronic Femoropopliteal DVT
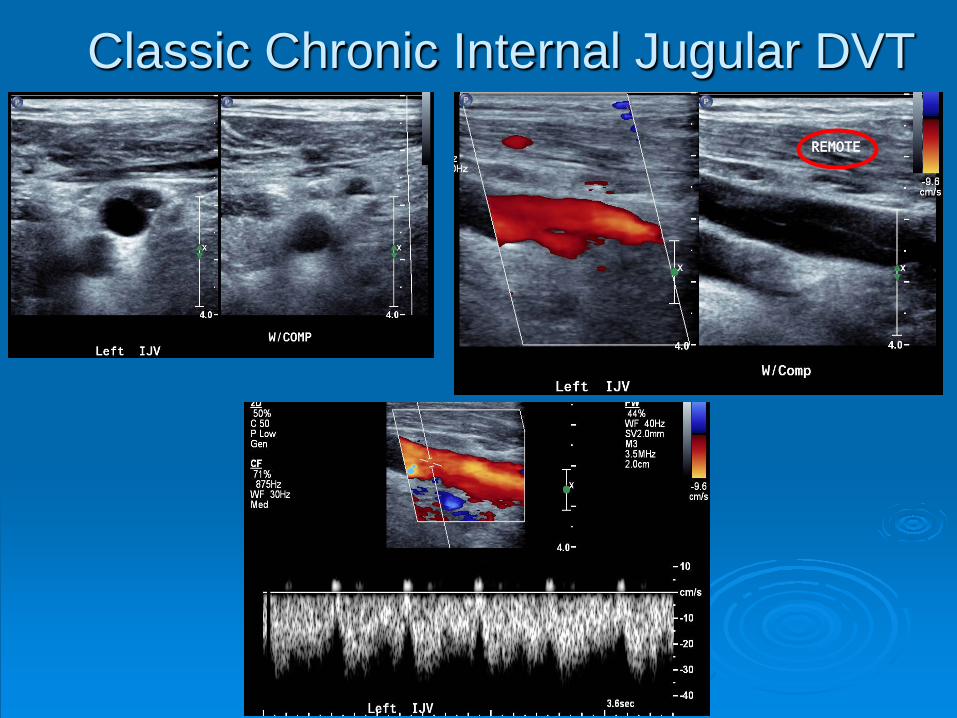
Classic Chronic Internal Jugular DVT
Pitfall: Determining Acute vs. Chronic DVT on a Duplex Examination is Not Always so Easy!
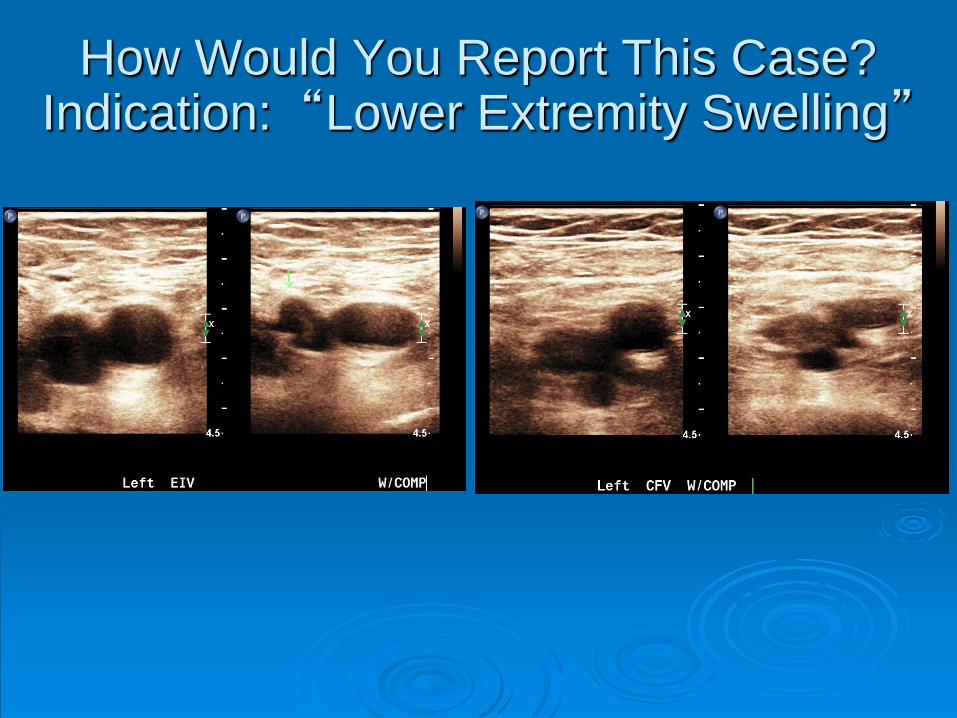
How Would You Report This Case?Indication: “Lower Extremity Swelling”
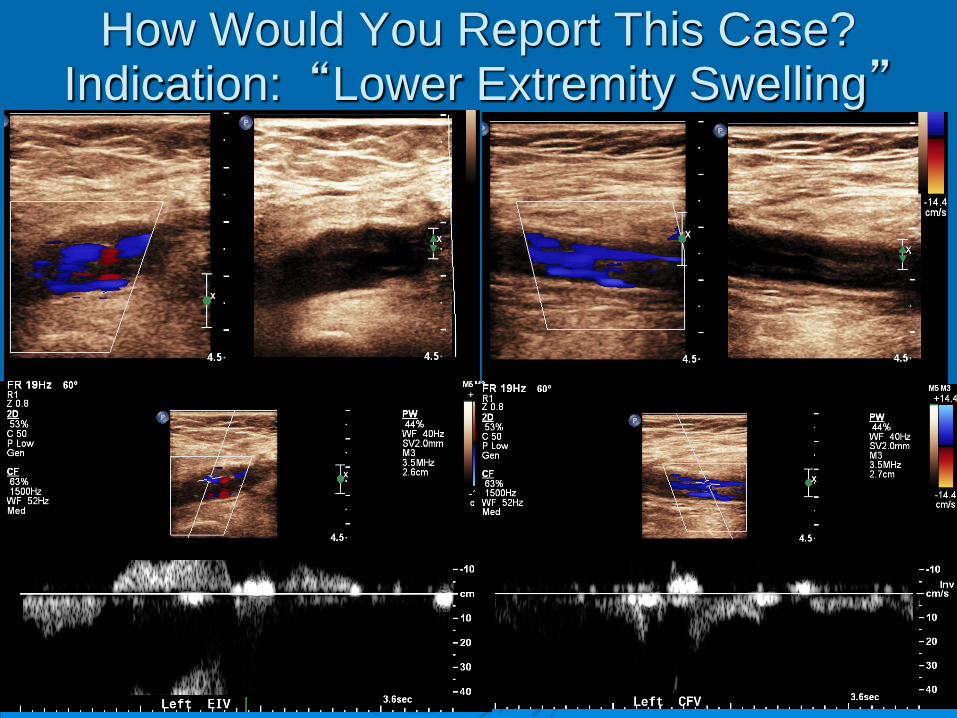
How Would You Report This Case?Indication: “Lower Extremity Swelling”
How would you report this case?
1. Acute DVT2. Subacute DVT3. Chronic DVT4. Age indeterminate DVT5. My lab does not even try to report DVT age
Can the ultrasound literature help us make this decision in any way?
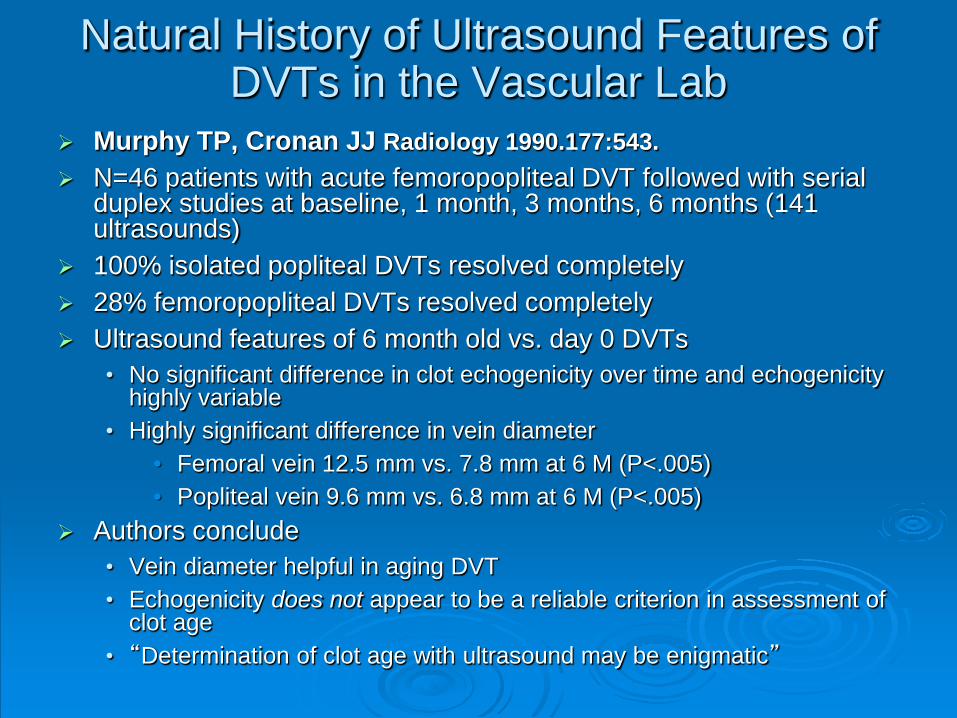
Natural History of Ultrasound Features of DVTs in the Vascular Lab
Murphy TP, Cronan JJ Radiology 1990.177:543. N=46 patients with acute femoropopliteal DVT followed with serial
duplex studies at baseline, 1 month, 3 months, 6 months (141 ultrasounds)
100% isolated popliteal DVTs resolved completely 28% femoropopliteal DVTs resolved completely Ultrasound features of 6 month old vs. day 0 DVTs
• No significant difference in clot echogenicity over time and echogenicity highly variable
• Highly significant difference in vein diameter• Femoral vein 12.5 mm vs. 7.8 mm at 6 M (P<.005) • Popliteal vein 9.6 mm vs. 6.8 mm at 6 M (P<.005)
Authors conclude • Vein diameter helpful in aging DVT • Echogenicity does not appear to be a reliable criterion in assessment of
clot age• “Determination of clot age with ultrasound may be enigmatic”
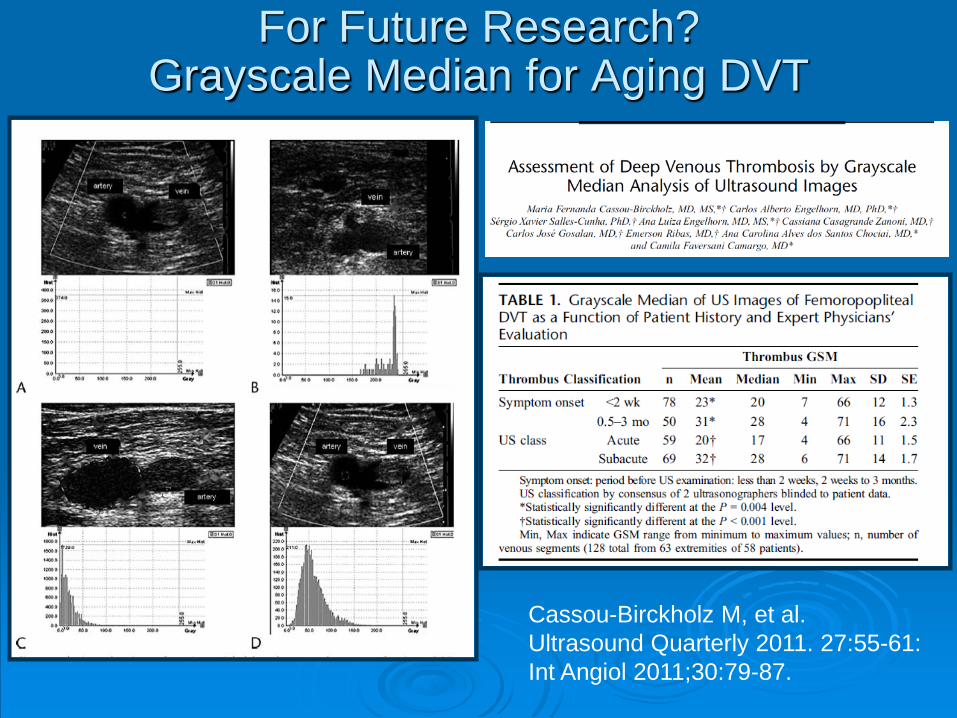
For Future Research? Grayscale Median for Aging DVT
Cassou-Birckholz M, et al.Ultrasound Quarterly 2011. 27:55-61:Int Angiol 2011;30:79-87.
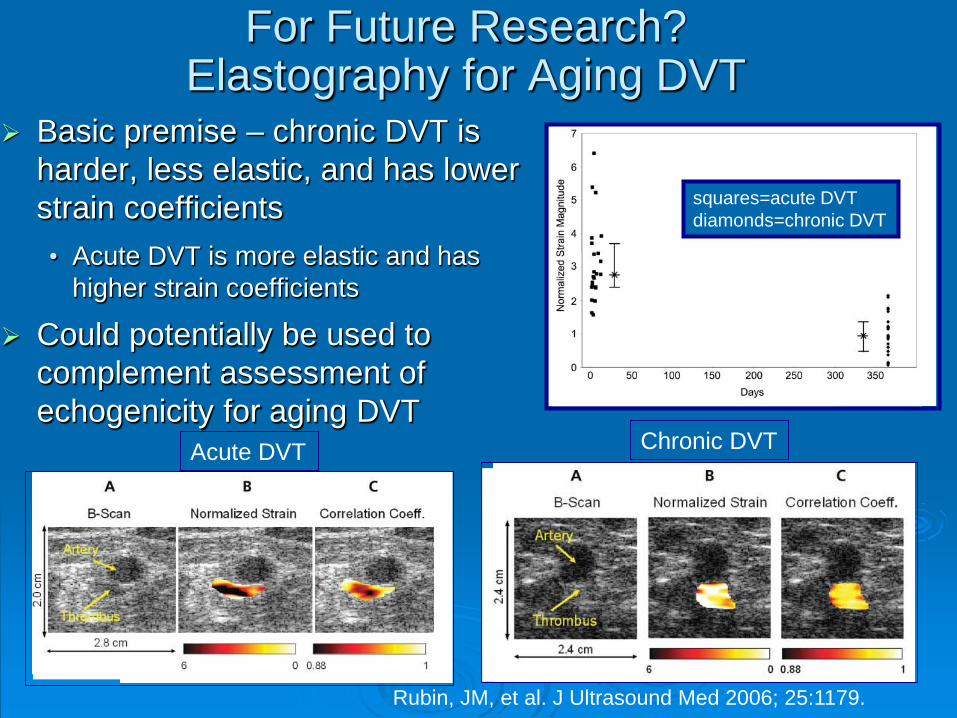
For Future Research?Elastography for Aging DVT
Basic premise – chronic DVT is harder, less elastic, and has lower strain coefficients• Acute DVT is more elastic and has
higher strain coefficients
Could potentially be used to complement assessment of echogenicity for aging DVT
squares=acute DVTdiamonds=chronic DVT
Acute DVT Chronic DVT
Rubin, JM, et al. J Ultrasound Med 2006; 25:1179.
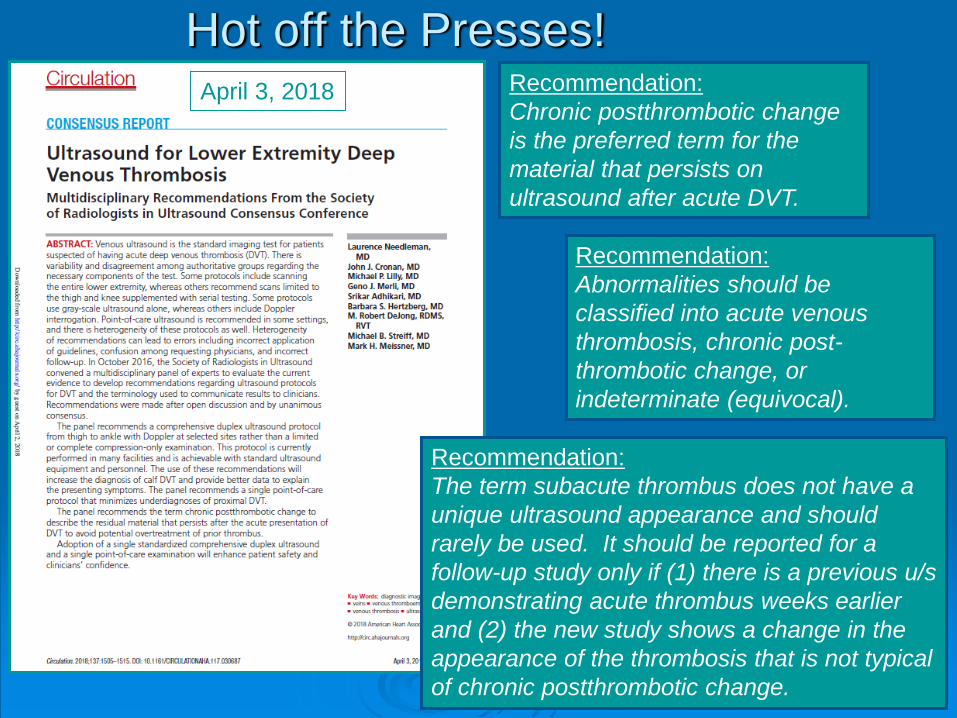
Hot off the Presses!
Recommendation:Abnormalities should be classified into acute venous thrombosis, chronic post-thrombotic change, or indeterminate (equivocal).
Recommendation:Chronic postthrombotic change is the preferred term for the material that persists on ultrasound after acute DVT.
Recommendation:The term subacute thrombus does not have a unique ultrasound appearance and should rarely be used. It should be reported for a follow-up study only if (1) there is a previous u/s demonstrating acute thrombus weeks earlier and (2) the new study shows a change in the appearance of the thrombosis that is not typical of chronic postthrombotic change.
April 3, 2018
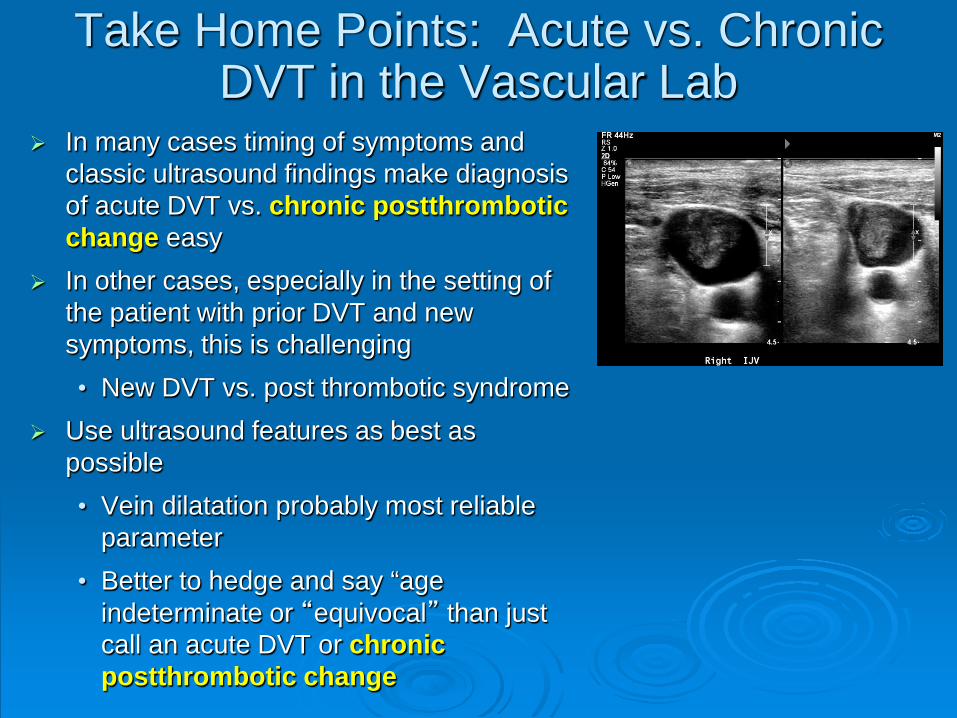
Take Home Points: Acute vs. Chronic DVT in the Vascular Lab
In many cases timing of symptoms and classic ultrasound findings make diagnosis of acute DVT vs. chronic postthromboticchange easy
In other cases, especially in the setting of the patient with prior DVT and new symptoms, this is challenging• New DVT vs. post thrombotic syndrome
Use ultrasound features as best as possible• Vein dilatation probably most reliable
parameter• Better to hedge and say “age
indeterminate or “equivocal” than just call an acute DVT or chronic postthrombotic change
Take Home Points: Acute vs. Chronic DVT in the Vascular Lab
“Aging” of DVT with ultrasound clearly an area in need of additional research
D-dimer may be helpful clinically in some cases to determine acute DVT reoccurrence (data free zone)• Very helpful but only if it is normal
Consider obtaining a post treatment baseline duplex ultrasound for select DVT patients:• Extensive proximal DVT
• Patients at high risk for recurrence (e.g., unprovoked DVT)
For new symptoms and suspected DVT recurrence, try to obtain the venous duplex in the same vascular laboratory
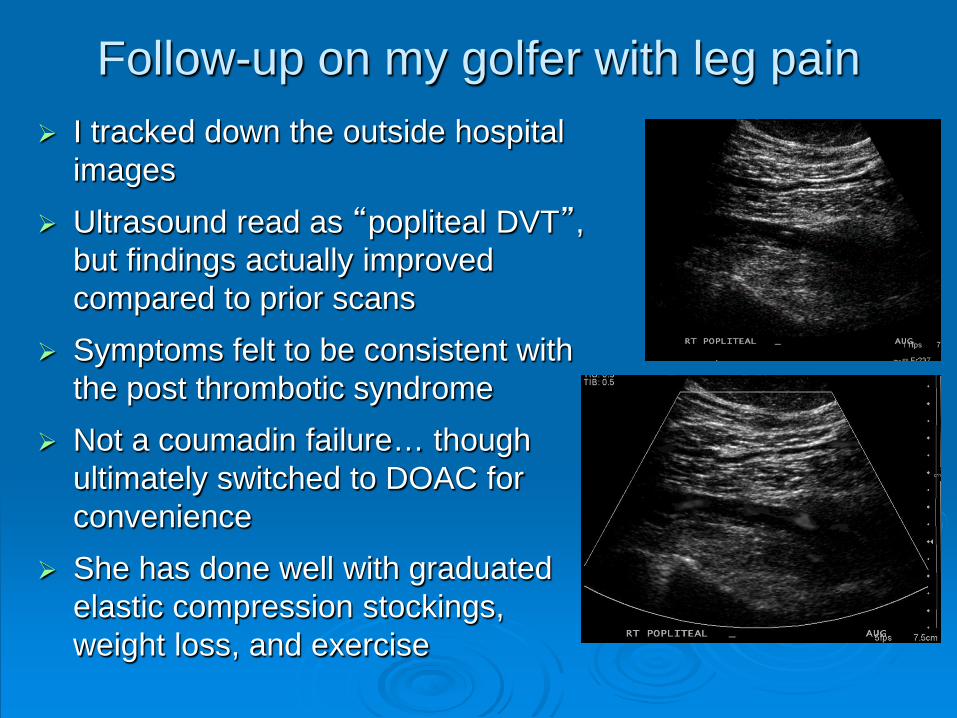
Follow-up on my golfer with leg pain I tracked down the outside hospital
images Ultrasound read as “popliteal DVT”,
but findings actually improved compared to prior scans
Symptoms felt to be consistent with the post thrombotic syndrome
Not a coumadin failure… though ultimately switched to DOAC for convenience
She has done well with graduated elastic compression stockings, weight loss, and exercise