Embed Size (px)
Citation preview

Washington University School of Medicine Washington University School of Medicine
Digital Commons@Becker Digital Commons@Becker
Open Access Publications
2021
Acute symptoms of mild to moderate COVID-19 are highly Acute symptoms of mild to moderate COVID-19 are highly
heterogeneous across individuals and over time heterogeneous across individuals and over time
Thomas L. Rodebaugh
Madelyn R. Frumkin
Angela M. Reiersen
Eric J. Lenze
Michael S. Avidan
See next page for additional authors
Follow this and additional works at: https://digitalcommons.wustl.edu/open_access_pubs

Authors Authors Thomas L. Rodebaugh, Madelyn R. Frumkin, Angela M. Reiersen, Eric J. Lenze, Michael S. Avidan, J. Philip Miller, Jay F. Piccirillo, Charles F. Zorumski, and Caline Mattar

M A J O R A R T I C L E
Heterogeneity in COVID-19 • ofid • 1
Open Forum Infectious Diseases
Received 19 November 2020; editorial decision 19 February 2021; accepted 23 February 2021.Correspondence: Thomas L. Rodebaugh, PhD, 1 Brookings Dr., CB#1125, Somers Family Hall,
Washington University in St Louis, St Louis, MO 63130 ([email protected]).
Open Forum Infectious Diseases®2021© The Author(s) 2021. Published by Oxford University Press on behalf of Infectious Diseases Society of America. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs licence (http://creativecommons.org/licenses/by-nc-nd/4.0/), which permits non-commercial reproduction and distribution of the work, in any medium, provided the original work is not altered or transformed in any way, and that the work is properly cited. For commercial re-use, please contact [email protected]: 10.1093/ofid/ofab090
Acute Symptoms of Mild to Moderate COVID-19 Are Highly Heterogeneous Across Individuals and Over TimeThomas L. Rodebaugh,1, Madelyn R. Frumkin,1 Angela M. Reiersen,2 Eric J. Lenze,2 Michael S. Avidan,3 J. Philip Miller,4 Jay F. Piccirillo,5 Charles F. Zorumski,2 and Caline Mattar6
1Department of Psychological and Brain Sciences, Washington University in St Louis, St Louis, Missouri, USA, 2Department of Psychiatry, Washington University School of Medicine (WUSM), St Louis, Missouri, USA, 3Department of Anesthesiology, WUSM, St Louis, Missouri, USA, 4Institute for Informatics, Division of Biostatistics, WUSM, St Louis, Missouri, USA, 5Department of Otolaryngology, WUSM, St Louis, Missouri, USA, and 6Department of Internal Medicine, Division of Infectious Diseases, WUSM, St Louis, Missouri, USA
Background. The symptoms of coronavirus disease 2019 (COVID-19) appear to be heterogenous, and the typical course of these symptoms is unknown. Our objectives were to characterize the common trajectories of COVID-19 symptoms and to assess how symptom course predicts other symptom changes as well as clinical deterioration.
Methods. One hundred sixty-two participants with acute COVID-19 responded to surveys up to 31 times for up to 17 days. Several statistical methods were used to characterize the temporal dynamics of these symptoms. Because 9 participants showed clin-ical deterioration, we explored whether these participants showed any differences in symptom profiles.
Results. Trajectories varied greatly between individuals, with many having persistently severe symptoms or developing new symptoms several days after being diagnosed. A typical trajectory was for a symptom to improve at a decremental rate, with most symptoms still persisting to some degree at the end of the reporting period. The pattern of symptoms over time suggested a fluctuating course for many patients. Participants who showed clinical deterioration were more likely to present with higher reports of severity of cough and diarrhea.
Conclusions. The course of symptoms during the initial weeks of COVID-19 is highly heterogeneous and is neither predict-able nor easily characterized using typical survey methods. This has implications for clinical care and early-treatment clinical trials. Additional research is needed to determine whether the decelerating improvement pattern seen in our data is related to the phenom-enon of patients reporting long-term symptoms and whether higher symptoms of diarrhea in early illness presages deterioration.
Keywords. cough; COVID-19; humans; severe acute respiratory syndrome coronavirus 2; smell; taste.
applyparastyle “fig//caption/p[1]” parastyle “FigCapt”
Dow
nloaded from https://academ
ic.oup.com/ofid/article/8/3/ofab090/6154666 by W
ashington University in St. Louis user on 06 M
ay 2021

2 • ofid • Rodebaugh et al
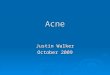
Graphical abstract
10.010.0
7.5
5.0
2.5
0.00 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
COVID-19 symptoms generally recede, but symptom courses arehighly heterogenous
Average symptom course (15–17 days) Highly varying individual courses
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
Symptom
Ache
Breath
Fatigue
Fever
Taste7.5
5.0
Sym
ptom
sev
erity
2.5
0.0
0 1 2
Time
3 4
INTRODUCTION
The World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) have described common symptoms of the coronavirus disease 2019 (COVID-19), including fever, dry cough, and difficulty breathing [1, 2]. They also report that many people may have few or no symp-toms despite infection. This characterization is based on studies that report cross-sectional or retrospective accounts of symp-toms from chart review or patient interviews [3–10].
Thus, the temporal dynamics of COVID-19 symptoms are unclear. For example, in a patient currently experiencing fever, should the patient be concerned about more severe illness if the fever seems to resolve but returns a day later? Notably, a recent review of long-term COVID-19 symptoms revealed that some patients expected a gradual, linear recovery and were troubled
by symptoms that instead waxed and waned [11]. Moreover, if COVID-19 symptoms have highly heterogeneous trajectories, this could be a barrier to measuring symptoms as a treatment outcome, in that reduction in symptoms on average could mask increases in specific symptoms, such that some patients could appear to improve (reduction in symptoms overall) while ac-tually deteriorating (eg, increase in shortness of breath alone).
The aim of the current study is to characterize the temporal dynamics of COVID-19 symptoms in a sample of participants in a randomized controlled trial testing the medication flu-voxamine (vs placebo) for early COVID-19 treatment [12]. Participants reported on their experience of common COVID-19 symptoms, as well as blood oxygen level and other clinical signs, twice daily for a maximum of 31 times over the course of a maximum of 17 days.
Dow
nloaded from https://academ
ic.oup.com/ofid/article/8/3/ofab090/6154666 by W
ashington University in St. Louis user on 06 M
ay 2021

Heterogeneity in COVID-19 • ofid • 3
We used these frequently sampled data to model trajectories of the self-reported symptoms. That is, we characterized the course of symptoms using latent trajectory models (also called latent growth curve models). These models test how to best characterize the changes in self-reported symptoms across the course of the study in those participants who ever reported that symptom. These models are commonly used to study the devel-opment of symptoms over time [13, 14].
To model trajectories meaningfully, it is essential to obtain se-quential data in real time, without reliance on retrospection. Asking people to recall events results in poor quality data even about events that seem highly memorable [15]. With frequently sampled data over time, a variety of statistical methods allows the researcher to characterize what is generally true in the sample over time, as well as to what extent participants vary from this average trajectory. Thus, we can determine the ways in which symptoms change over time, as well as whether changes in some symptoms tend to go together, as might be expected due to some symptoms being functionally related (eg, problems with smell and taste).
METHODS
Study Population
Participants were adults living in the community with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in-fection confirmed by polymerase chain reaction assay who were currently symptomatic with symptom onset <7 days be-fore beginning survey responses. Exclusion criteria included COVID-19 severe enough to require hospitalization or meeting the study’s primary end point for clinical deterioration at baseline (ie, oxygen saturation of <92% on room air), med-ical comorbidities including severe underlying lung disease (chronic obstructive pulmonary disease or home oxygen, in-terstitial lung disease, pulmonary hypertension), decompen-sated cirrhosis, congestive heart failure (stage 3 or 4), and being immunocompromised (solid organ transplant, bone marrow transplant recipient, AIDS, on biological immunologic medi-cations or high-dose steroids [>20 mg of prednisone per day]).
The clinical trial’s primary outcome measure was clinical deterioration, defined by meeting both of the following: (1) presence of dyspnea (ie, shortness of breath) and/or hospital-ization for shortness of breath or pneumonia plus (2) decrease in oxygen saturation (<92%) on room air and/or supple-mental oxygen requirement in order to keep oxygen saturation ≥92%. Participants typically stopped completing surveys on their symptoms once they met the primary outcome criteria. However, data are available from 1 participant who experienced moderate deterioration halfway through the trial and continued to provide data after deterioration. Notably, because we in-cluded all participants who provided any symptom survey data, we report on an additional 10 participants not included in the parent study [12]; these subjects were excluded from the parent
study because they either could not be confirmed to have taken the study drug (n = 7) or were deteriorated at baseline (n = 3).
Patient Consent Statement
The study was approved by Washington University’s Institutional Review Board before initiating any recruitment, and all partici-pants provided informed consent via an e-consent or written consent.
Survey
Data collection occurred via REDCap surveys sent to parti-cipants via email, with telephone-based data collection as a backup to ensure that individuals without internet access were able to participate. The data collection used an ecological mo-mentary assessment (EMA) framework. EMA (vs standard data collection methods) is thought to limit biased responding in participants due to retrospection because in EMA participants are asked about their current experience [16]. The surveys re-corded COVID-19 symptoms, oxygen saturation, vital signs, and medication adherence. Participants completed a baseline survey before starting the study medication, followed by surveys approximately twice a day for 15 days after starting the study drug; occasional delayed responding or technical errors led to a maximum of 17 days. At each survey, participants were asked whether they were experiencing a symptom at all. When they in-dicated “no,” this was coded as a value of 0. When they reported “yes,” they were then asked to rate the perceived severity of the symptom on a scale from 1 to 10. The symptoms rated included perceived fever, cough, shortness of breath, fatigue or weakness, chills, nausea, body aches, diarrhea, loss of appetite, difficulty with sense of smell, and difficulty with sense of taste.
Statistical Analysis
Analyses were conducted in Mplus [17], with visualizations produced in R. Because these analyses were not preregistered, we recommend considering them primarily descriptive and ex-ploratory. Results are reported for the entire group of partici-pants without reference to randomized controlled trial (RCT) group because there were no clear differences between groups on latent trajectory outcomes (the same 30 tests were conducted as reported below for demographic variables, yet the lowest P value was .015, whereas we considered .01 significant due to the large number of tests). Additional details on analyses and rele-vant statistical output are available in the Supplementary Data as well as at https://osf.io/t8frj/.
RESULTS
Participant Characteristics
In total 162 participants completed at least some EMA sur-veys (n = 162; median surveys answered, 23; median days cov-ered, 16); demographic data are missing for 10. Participants who
Dow
nloaded from https://academ
ic.oup.com/ofid/article/8/3/ofab090/6154666 by W
ashington University in St. Louis user on 06 M
ay 2021

4 • ofid • Rodebaugh et al
reported were mostly White (70%, n = 106), although many participants reported that they were Black (25%, n = 38), with an average age (SD) of 45.80 (13.04). The sample was primarily female, as judged by the number reporting being assigned fe-male sex at birth (69%, n = 109).
Symptom Frequency and Severity Across and Within Patients Over Time
The most common rating for all symptoms was 0, or not present (Supplementary Table 1; Supplementary Figure 1). Figure 1, which depicts raw data for all symptoms for a random set of participants, demonstrates that the frequent ratings of 0 oc-curred in a number of patterns, including symptoms never occurring, occurring and then resolving, starting in the middle of the reporting period, and fluctuating during some portion of the reporting period. The frequent “saw tooth” patterns seen in Figure 1 suggest symptoms waxing and waning. An expanded version of this figure is available in the Supplementary Figure 2.
Heterogeneity of Symptom Trajectories
To handle the frequent instance of 0s in the data, before pro-ceeding with further analysis we (1) restricted further analysis to participants who ever had that symptom and (2) consolidated symptom reports to 5 time points (Times 0 through 4). This procedure had the effect of “smoothing out” the sawtooth pat-tern present for many participants, allowing analysis of overall tendencies over time.
We examined typical trajectories using latent trajectory mod-eling. These models focus on slopes and intercepts as a way to characterize the course of symptoms across the whole sample. The intercept refers to the participant’s estimated level of the symptom at Time 0 (ie, during the first 3 days of the study). For participants with only random fluctuations or a stable level of a
symptom, the intercept would be enough to characterize their data, while the existence of a slope denotes that there are system-atic changes in the symptom. A linear slope indicates a tendency up or down. A quadratic slope indicates some curve to the line’s shape. A cubic slope indicates a second curvature of the line. The modeling allows us to determine whether the data are well char-acterized by the intercept and 1 or more slopes, as well as how many slopes are required to characterize the data of participants overall. The modeling also allows us to determine whether and how individual participants significantly vary from the average group trajectory. For example, the model might show that the mean slope is negative, indicating resolution of a symptom, but with significant variance, indicating that some participants are better characterized by an upward slope of symptoms.
Of the symptoms, only nausea was not reasonably well char-acterized by a latent trajectory model. As shown in Table 1, all other symptoms were best characterized by at least 1 curvilinear slope in addition to a linear slope, typically showing a decrease but with deceleration. Because we only analyzed those partici-pants who reported the symptom at some point, the number for each model (vs 162 who supplied any EMA) shows how com-monly the symptom was reported. The most common symp-toms were fatigue, fever, reduced appetite, and problems with sense of taste. The linear slopes all had negative means. Thus, participants on average tended to show reductions in symptoms over time, but the significant variance of most of the slopes indi-cates that many participants showed increases in symptoms. As a reminder, there was no indication that participants differed in these trajectories based on treatment group.
On the average, judging from the linear slope values, par-ticipants recovered the quickest from aches and low appetite and most slowly from cough and difficulty breathing. With the
Table 1. Summary of Latent Trajectory Models
SymptomParticipants in
AnalysisIntercept Mean
(Variance)Linear Slope Mean
(Variance)Quadratic Slope Mean
(Variance)Cubic Slope Mean
(Variance)
Ache2 120 3.80** (6.45**) –1.50** (2.10*) 0.20** (0.07*)
Appetite1 121 3.85** (4.45**) –1.54** (0.99*) 0.18** (0.04*)
Breath2 89 2.11** (2.86**) –0.37* (1.33*) 0.02 (0.06*)
Chill1 74 2.25** (3.63*) –1.13** (1.54*) 0.15** (0.04)
Cough3 129 2.86** (4.65**) –0.51** (0.94*) 0.01 (0.05*)
Diarrhea2 100 1.66** (1.68*) –0.66* (0.00a) 0.08* (0.01)
Fatigue3 144 4.26** (5.34**) –1.35** (1.61**) 0.15** (0.06**)
Fever3 72 2.26** (6.06**) –1.15** (2.84**) 0.16** (0.08*)
Smell1 112 5.80** (5.79**) –1.32** (4.20*) 0.10 (0.16*)
Taste3 119 5.06** (9.20**) –1.05* (10.67**) –0.07 (1.89**) 0.03 (0.04**)
Latent trajectory models were conducted on participants (n = 162) who ever reported the symptom. The intercept, linear, and quadratic slopes are then given. Intercepts indicate where participants start, on average, whereas linear slope indicates the general tendency up or down. Additional slopes indicate the extent to which symptom courses frequently reversed, slowed, or accelerated. Unstandardized estimates are given because these are directly relevant to the response scale of 0 (not at all) to 10 (most severe). Statistically significant slopes indicate that participants showed a group tendency overall. Significant variances indicate that participants meaningfully differed in this tendency. Thus, for example, despite the linear slopes being negative, at least 1 participant had a positive slope where the variance was statistically significant.
*P < .05; **P < .001.1,2,3Indicates number of fit indices showing good to excellent fit. When the number is higher, we can be more certain that the model describes the overall sample well. Further information on fit is available in individual outputs in the Supplementary Data.aVariance was fixed to 0 to permit estimation.
Dow
nloaded from https://academ
ic.oup.com/ofid/article/8/3/ofab090/6154666 by W
ashington University in St. Louis user on 06 M
ay 2021

Heterogeneity in COVID-19 • ofid • 5
exception of problems with sense of taste, all other symptoms had a second quadratic term that was positive, which indicates that although their symptoms went down, the rate at which they dropped began to slow. Thus, the most typical course was an ini-tially rapid recovery followed by some plateauing, or a pattern of decelerating improvement. Most symptoms had significant var-iance in both the linear and quadratic slope, which means that the curve could also move in a different direction for some par-ticipants. For example, some participants increased in symptoms and then decreased, whereas others had stable levels of symptoms or had increased symptoms that were maintained across the rest of the reporting period. The picture is even more complicated for taste, which had an additional cubic slope. This symptom thus showed at least 2 inflection points for many participants, as would be true if the symptom went up, down, and then up again.
Figure 2 displays illustrative curves for each symptom. These figures display the most typical (mean) course, alongside the typical course of (1) participants whose symptoms reduced rap-idly, as well as (2) those whose symptoms either reduced more
slowly or were exacerbated. In the latter 2 cases, the 10 parti-cipants with the most extreme linear slopes had their param-eters averaged to depict a typical rapidly improving and slowly improving course (with the exception of diarrhea, for which the most extreme quadratic courses were averaged because the linear slope had no variance). Finally, the single participant who deteriorated according to study criteria yet also provided a full set of EMA data is also presented. This participant ex-perienced moderate deterioration and visited the emergency room midway through the reporting period. Examining this participant’s raw data revealed no obvious signs of the deterio-ration aside from 3 elevated ratings of shortness of breath (a 5 or 6 out of 10) that occurred around this period, with these ratings surrounded by ratings of 0.
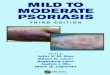
A further depiction of the wide variety of slopes is provided in Figure 3. Here we depict trajectories for the 5 symptoms with the best-fitting models. On the left, we see the average course of all of these symptoms is an improvement in mild symptoms that slows down. On the right, 9 randomly selected participants
Ache
Y-ax
is o
f ea
ch g
raph
sho
ws
sym
ptom
sev
erity
(0–1
0);
each
row
is d
ata
from
1 p
artic
ipan
t
Appetite Breath
Time points (0-30)
Chills Cough Diarrhea Fatigue Fever Nausea Smell Taste
Figure 1. Up to a 17-day course (median, 16) of symptoms for 10 randomly selected participants on a per-symptom basis. Each row includes data for 1 participant. Time points are ~12 hours apart on up to 17 days. Note the “saw tooth” pattern for many participants, indicating symptoms that wax and wane. An expanded version of this figure is available in Supplementary Data.
Dow
nloaded from https://academ
ic.oup.com/ofid/article/8/3/ofab090/6154666 by W
ashington University in St. Louis user on 06 M
ay 2021

6 • ofid • Rodebaugh et al
show us that these average trajectories vary significantly across individuals, with symptoms rising and falling at different rates across people. An expanded version of this figure is available in the Supplementary Data.
How Symptoms Change Together Over Time
Table 2 shows the correlations among linear slopes. Each person’s linear slope tells us to what extent their symptoms gen-erally tend to go up or down over time. The correlation between these slopes tells us whether we should expect that participants have symptoms that go together as they improve or worsen. Some pairs stood out with particularly strong correlations. These include problems with taste and smell, cough and trouble breathing, chills and fever, and, to a lesser extent, ache and fa-tigue. Thus, for example, we would expect that for a participant whose symptoms included both cough and trouble breathing these symptoms would tend to go up or down together over
time. In contrast, for a participant with fever and trouble breathing, we would have no reason to expect that a reduction in fever should necessarily go along with improved breathing, because the correlation is small and negative.
Symptom Dynamics, Demographics, and Clinical Deterioration
Most participants who deteriorated did so in the first several days and stopped providing EMA data. Thus, most of the 9 participants who deteriorated provided data only for Time 0 for the trajectories presented. Accordingly, we examined differences between the 9 participants who deteriorated (ie, developed dyspnea and hypoxia) and the rest of the sample only in the intercepts (the only meaningful trajectory in-formation for participants who only reported during Time 0). Given the small sample of participants who deterior-ated, Mann-Whitney U tests were conducted. Two effects retained statistical significance above a correction for the
10.0
7.5
5.0
2.5
0.0 Subgroup
Average
Rapid improvement
Slower improvement
Deteriorated10.0
Sym
ptom
sev
erity
7.5
5.0
2.5
0.0
0 1 2 3 4 0 1 2 3 4 0 1 2
Time
3 4 0 1 2 3 4 0 1 2 3 4
Ache Appetite Breath Chills Cough
Diarrhea Fatigue Fever Smell Taste
Figure 2. Representative courses of coronavirus disease 2019 symptoms across up to 17 days (median, 16 days). Each time point represents the average of 3 days, except that Time 4 included up to 5 days, but more typically 3 or 4. The Average line represents the average trajectory across the entire data set. The Rapid improvement and Slower improvement lines are the average for the 10 participants, with the strongest linear slope in the improving and worsening directions. For diarrhea, the quadratic slope was used as the linear slope had no variance. A worsening linear slope did not always translate to symptoms being aggravated overall because trajectories were curvilinear. Slower improvement lines are not depicted for appetite or chills because too few participants experienced worsening in this symptom as indexed by the linear slope. The Deteriorated lines provide the slope for the single participant who deteriorated midway through the trial yet provided a full set of data.
Dow
nloaded from https://academ
ic.oup.com/ofid/article/8/3/ofab090/6154666 by W
ashington University in St. Louis user on 06 M
ay 2021

Heterogeneity in COVID-19 • ofid • 7
number of tests conducted in this analysis: Participants who deteriorated were far more likely to have an elevated inter-cept (ie, higher initial levels) for both cough and diarrhea (all P = .002).
We also examined demographic variables to see if symptom dynamics differed, adopting a P of .01 to balance multiple testing against discovery of potentially important findings. Men and women showed no differences in any intercepts or slopes.
10.010.0
7.5
5.0
2.5
0.00 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
10.0
7.5
5.0
2.5
0.0
0 1 2 3 4
Symptom
Ache
Breath
Fatigue
Fever
Taste7.5
5.0
Sym
ptom
sev
erity
2.5
0.0
0 1 2
Time
3 4
Figure 3. On the left, the average course of 5 common symptoms across up to 17 days (median number of days, 16). On the right, 9 randomly selected participants (of those who had all 5 symptoms) and their individual trajectories. Note that because the model fits a curve to data points, the curve can transiently go above the response scale. An expanded version of this figure is available in the Supplementary Data.
Table 2. Partial Correlations Between Pairs of Linear Slopes Controlling for Intercepts With Number of Participants for Each Comparison
Ache Appetite Breath Chill Cough Fatigue Fever Smell Taste
Ache 97 75 68 100 114 63 90 93
Appetite 0.26* 73 65 100 115 61 89 97
Breath 0.39** 0.09 54 82 85 47 68 76
Chill 0.33** –0.01 0.38** 62 72 50 50 61
Cough 0.36** 0.13 0.68** 0.23 118 63 93 98
Fatigue 0.51** 0.44** 0.46** 0.31** 0.33** 69 104 111
Fever 0.06 0.10 –0.04 0.65** 0.09 0.15 52 58
Smell 0.23* 0.30** 0.04 0.00 0.18 0.32** –0.11 104
Taste 0.23* 0.35** 0.07 0.19 0.23* 0.31** 0.09 0.74**
No. for each comparison is on the top diagonal. Positive correlations indicate that symptoms tend to go either or up or down together. Negative correlations indicate that the symptoms diverge in trajectories (as 1 goes up, the other goes down). Thus, problems with smell are very likely to resolve along with problems with taste. Diarrhea is not included in these analyses because its linear slope had a variance of 0, which means it cannot correlate with other slopes.
*P < .05; **P < .01.
Dow
nloaded from https://academ
ic.oup.com/ofid/article/8/3/ofab090/6154666 by W
ashington University in St. Louis user on 06 M
ay 2021

8 • ofid • Rodebaugh et al
Black participants had a significantly higher intercept of chill and cough (all P < .007), suggesting more severe symptoms at the start of the study. No other slopes or intercepts showed clearly significant differences. Body mass index (BMI) did not correlate significantly with any intercepts or slopes. Thus, there were few signs that demographic variables were related to the course of COVID-19 symptoms.
DISCUSSION
Our study characterizes the course of COVID-19 among community-dwelling patients who are recovering at home. This information is important because it informs clinicians, patients, and researchers about the high degree of heteroge-neity, both between and within patients. We made the fol-lowing 4 major observations: First, the COVID-19 symptom course is highly heterogenous. Second, early symptoms re-lated to participant demographics and clinical deterioration. Third, symptoms often showed a pattern of decelerating im-provement. Fourth, some symptoms are likely to improve in tandem, whereas others are not. We discuss each of these points further below.
The overall picture is of symptoms reducing for most partici-pants, but often with a slowing of this reduction, often further complicated by waxing and waning of symptoms (eg, across 12-hour periods). Further, problems with the sense of taste were characterized by additional curvilinearity, reflecting increased volatility. As a notable example, the participant who clinically deteriorated (developed dyspnea and hypoxia) did this in spite of symptoms showing average or rapidly improving course in some respects. Although this is a report of only a single par-ticipant who experienced moderate deterioration, it stands as a warning that deterioration in COVID-19 can be rapid and unpredictable.
We found no evidence that symptom dynamics varied mean-ingfully across the treatment groups from the parent study, nor any association with BMI. However, participants who deteri-orated were more likely to have initially high levels of cough and diarrhea. This finding should be taken as exploratory and requiring confirmatory tests of whether higher levels of these symptoms in the initial days of illness might presage clinical de-terioration, especially because 3 of our deteriorated participants were deteriorated at baseline. Importantly, our more global findings indicate that the time frame of assessment might be crucial. Our finding is that participants with higher self-report of cough and diarrhea near the beginning of their illness were more likely to experience deterioration at some point. Because symptom courses often wax and wane, asking participants if they ever experienced that symptom or experienced it later in the illness would not necessarily yield the same result. However, at least 1 report has found that diarrhea presaged clinical de-terioration [18]. We expect that our finding regarding cough
might simply reflect the fact that most of those who deterior-ated did so early in the reporting period, but the possibility that severity of cough actually predicts deterioration seems worth investigating.
Our findings indicate that patients and health care providers can expect a variety of symptom courses, including the devel-opment of additional symptoms and a gradual and potentially stalling decline of some symptoms. The latter finding is con-sistent with another study showing that a minority of partici-pants continue to experience symptoms, particularly cough, fatigue, and shortness of breath [6]. In our results, cough and shortness of breath showed the smallest slope downward on average, suggesting, in combination with previous results, that these symptoms in particular are likely to be prolonged for many patients.
Whether the decelerating improvement pattern is unique to COVID-19 is difficult to determine because few studies have examined other common infectious diseases in regard to common trajectories of symptoms. However, a report focusing on the development of a symptom measure for influenza re-ported the average course of several symptoms [19]. Although challenging to compare directly due to differences in method-ology, our results seem to suggest (1) a longer course for sig-nificant symptoms of COVID-19 and (2) a greater deceleration in improvement across the second week. That is, for influenza symptoms, rapid recovery over the first 4 days (Time 0 to Time 1 in our analysis) was followed by a more gradual, approximately linear slope for the remainder of the days assessed. Our partici-pants experienced more gradual initial improvement, followed, most commonly, by a greater deceleration of improvement.
Judging from correlated slopes, some pairs of symptoms are likely to reduce in tandem. The strongest candidate for such a pairing is problems with smell and taste, which should be ex-pected given the functional connection between the 2 senses. Similarly, cough and shortness of breath, fever and chills, and, to a lesser extent, ache and fatigue are all pairs that show a ten-dency to decline over time together.
Limitations
The results of the study should be interpreted in light of its limi-tations. Patients were enrolled after diagnosis, which could have been up to 7 days after experiencing symptoms, and even longer after infection. This fact could explain some of the wide variety of trajectories, but not the observed waxing and waning or stalled improvement. Data were drawn from an RCT, with lim-ited diversity in patient population, conducted in 1 Midwestern metropolitan area, during the initial 7 months of the COVID-19 outbreak. It is unclear to what extent we should expect prev-alent symptoms of COVID-19 or their course to vary by virus variant, demographics, community, or even country. It is pos-sible that although asking participants first whether they had a symptom or not may have reduced patient burden, it may also
Dow
nloaded from https://academ
ic.oup.com/ofid/article/8/3/ofab090/6154666 by W
ashington University in St. Louis user on 06 M
ay 2021

Heterogeneity in COVID-19 • ofid • 9
have inclined participants to answer “no” even if a symptom was present in a mild form. Participants provided self-report of symptoms, which especially must be kept in mind when at-tempting to apply results to objective conditions. For example, 1 report found that a significant proportion of participants with COVID-19 reporting olfactory dysfunction did not meet cri-teria upon evaluation [20]. Nevertheless, self-reported symp-toms of problems with smell and taste have emerged as 2 of the best predictors of COVID-19 status [21, 22].
CONCLUSIONS
In conclusion, COVID-19 is a heterogeneous illness in terms of subjective symptoms and course. When patients experience a given symptom, it may fluctuate but will typically follow a gradual improvement over the course of 2 weeks or more. Many patients, however, will develop new symptoms during the same course, and many symptoms may take considerably beyond a 2-week window to resolve completely. This tendency toward slowly improving symptoms may be related to the increasing reports of a more chronic form of the disease in certain popu-lations [6, 8, 11]. It is important to warn patients, and clinicians caring for them, not to expect a linear decrease in all symptoms; some may be intermittent or get worse before they get better. Future studies following a cohort of patients with COVID-19 symptoms over a longer period of time could be useful in de-termining how, if at all, acute symptom presentation relates to chronic symptom experiences.
Supplementary DataSupplementary materials are available at Open Forum Infectious Diseases online as well as at https://osf.io/t8frj/. Consisting of data provided by the authors to benefit the reader, the posted materials are not copyedited and are the sole responsibility of the authors, so questions or comments should be addressed to the corresponding author.
AcknowledgmentsFinancial support. This study was supported by the Taylor Family
Institute for Innovative Psychiatric Treatment at Washington University and the COVID-19 Early Treatment Fund. Additional support came from the Center for Brain Research in Mood Disorders at Washington University, the Bantly Foundation, and National Institutes of Health grant UL1TR002345.
Role of the funder/sponsor. None of the funders were involved in the design or conduct of the study; collection, management, analysis, or inter-pretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Potential conflicts of interest. Dr. Lenze reports that he received grants from the COVID Early Treatment Fund, the Taylor Family Institute for Innovative Psychiatric Research, and the Center for Brain Research in Mood Disorders for this study. He also reports grant funding in the past 36 months from the Patient-Centered Outcomes Research Institute, Takeda, Alkermes, Janssen, Acadia, and the Barnes Jewish Foundation. He has received consulting fees in the past 36 months from Janssen and Jazz Pharmaceuticals. Dr. Zorumski reports that he is on the Scientific Advisory Board of Sage Therapeutics, reports personal fees from CME Outfitters, and also has stock and stock options with Sage Therapeutics. Dr. Miller reports that he has received research funding from the Patient-Centered Outcomes Research Institute. Dr. Rodebaugh, Ms. Frumkin, Dr. Reiersen,
Dr. Piccirillo, Dr. Avidan, and Dr. Mattar have nothing to disclose. All au-thors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Author contributions. T.L.R. and M.R.F. conducted data analysis. T.L.R. wrote the primary draft with substantive contributions from A.M.R., E.J.L., and C.M. M.R.F. provided data visualizations. All authors edited the manuscript and provided conceptual or statistical input. All authors con-tributed to interpretation of the data.
References1. Centers for Disease Control and Prevention. Symptoms of Coronavirus. https://
www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html. Accessed 16 March 2021.
2. World Health Organization. Coronavirus disease (COVID-19). https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-covid-19. Accessed 16 March 2021.
3. Lechien JR, Chiesa-Estomba CM, Place S, et al; COVID-19 Task Force of YO-IFOS. Clinical and epidemiological characteristics of 1420 European pa-tients with mild-to-moderate coronavirus disease 2019. J Intern Med 2020; 288:335–44.
4. Wiersinga WJ, Rhodes A, Cheng AC, et al. Pathophysiology, transmission, diag-nosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA 2020; 324:782–93.
5. Liu W, Liu Y, Xu Z, et al. Clinical characteristics and predictors of the duration of SARS-CoV-2 viral shedding in 140 healthcare workers. J Intern Med. in press.
6. Tenforde MW, Kim SS, Lindsell CJ, et al; IVY Network Investigators; CDC COVID-19 Response Team; IVY Network Investigators. Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a multistate health care systems network - United States, March-June 2020. MMWR Morb Mortal Wkly Rep 2020; 69:993–8.
7. Pullen MF, Skipper CP, Hullsiek KH, et al. Symptoms of COVID-19 outpatients in the United States. Open Forum Infect Dis 2020; 7:XXX–XX.
8. Cellai M, O’Keefe JB. Characterization of prolonged COVID-19 symptoms in an outpatient telemedicine clinic. Open Forum Infect Dis 2020; 7:XXX–XX.
9. Xia L, Chen J, Friedemann T, et al. The course of mild and moderate COVID-19 infections—the unexpected long-lasting challenge. Open Forum Infect Dis 2020; 7:XXX–XX.
10. Ng DHL, Choy CY, Chan YH, et al; National Centre for Infectious Diseases COVID-19 Outbreak Research Team. Fever patterns, cytokine profiles, and out-comes in COVID-19. Open Forum Infect Dis 2020; 7:XXX–XX.
11. Maxwell E. Living with COVID-19. 2020. Available from: https://evidence.nihr.ac.uk/themedreview/living-with-covid19/. Accessed 16 March 2021.
12. Lenze EJ, Mattar C, Zorumski CF, et al. Fluvoxamine vs placebo and clinical dete-rioration in outpatients with symptomatic COVID-19: a randomized clinical trial. JAMA 2020; 324:2292–300.
13. Curran PJ, Hussong AM. The use of latent trajectory models in psychopathology research. J Abnorm Psychol 2003; 112:526–44.
14. Duncan TE, Duncan SC. The ABC’s of LGM: an introductory guide to latent var-iable growth curve modeling. Soc Personal Psychol Compass 2009; 3:979–91.
15. Henry B, Moffitt TE, Caspi A, et al. On the “remembrance of things past”: a lon-gitudinal evaluation of the retrospective method. Psychological Assessment 1994; 6: 92–101.
16. Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annu Rev Clin Psychol 2008; 4:1–32.
17. Muthén LK, Muthén BO. Mplus User’s Guide. Los Angeles, CA: Muthén & Muthén; 1998.
18. Zheng T, Yang C, Wang HY, et al. Clinical characteristics and outcomes of COVID-19 patients with gastrointestinal symptoms admitted to Jianghan Fangcang Shelter Hospital in Wuhan, China. J Med Virol. in press.
19. Powers JH 3rd, Bacci ED, Guerrero ML, et al. Reliability, validity, and responsive-ness of InFLUenza Patient-Reported Outcome (FLU-PRO©) scores in influenza-positive patients. Value Health 2018; 21:210–8.
20. Lechien JR, Cabaraux P, Chiesa-Estomba CM, et al. Objective olfactory evalua-tion of self-reported loss of smell in a case series of 86 COVID-19 patients. Head Neck 2020; 42:1583–90.
21. Menni C, Valdes AM, Freidin MB, et al. Real-time tracking of self-reported symp-toms to predict potential COVID-19. Nat Med 2020; 26:1037–40.
22. Yan CH, Faraji F, Prajapati DP, et al. Association of chemosensory dysfunction and COVID-19 in patients presenting with influenza-like symptoms. Int Forum Allergy Rhinol 2020; 10:806–13.
Dow
nloaded from https://academ
ic.oup.com/ofid/article/8/3/ofab090/6154666 by W
ashington University in St. Louis user on 06 M
ay 2021