-
8/7/2019 Acute Respiratory Failure in the US - Incidence and 31
Day Survival
1/8
DOI 10.1378/chest.118.4.11002000;118;1100-1105Chest
Carolyn E. Behrendt
: Incidence and 31-Day Survival*StatesAcute Respiratory Failure
in the United
http://chestjournal.chestpubs.org/content/118/4/1100.full.html
services can be found online on the World Wide Web at:The online
version of this article, along with updated information and
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
written permission of the copyright holder.this article or PDF
may be reproduced or distributed without the priorDundee Road,
Northbrook, IL 60062. All rights reserved. No part of
Copyright2000by the American College of Chest Physicians,
3300Physicians. It has been published monthly since 1935.
is the official journal of the American College of
ChestChest
2000 American College of Chest Physiciansby guest on November
15, 2010chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/content/118/4/1100.full.htmlhttp://chestjournal.chestpubs.org/content/118/4/1100.full.htmlhttp://chestjournal.chestpubs.org/content/118/4/1100.full.htmlhttp://chestjournal.chestpubs.org/site/misc/reprints.xhtmlhttp://chestjournal.chestpubs.org/site/misc/reprints.xhtmlhttp://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/site/misc/reprints.xhtmlhttp://chestjournal.chestpubs.org/content/118/4/1100.full.html
-
8/7/2019 Acute Respiratory Failure in the US - Incidence and 31
Day Survival
2/8
Acute Respiratory Failure in the UnitedStates*
Incidence and 31-Day Survival
Carolyn E. Behrendt, PhD
Study objectives: To estimate the incidence of acute respiratory
failure (ARF) in the United Statesand to analyze 31-day hospital
mortality among a cohort of patients with ARF.Design and setting:
Retrospective cohort drawn from the Nationwide Inpatient Sample of
6.4million discharges from 904 representative nonfederal hospitals
during 1994.Patients: All 61,223 patients in the sample whose
discharge records indicated all of the following:acute respiratory
distress or failure, mechanical ventilation, > 24 h of
hospitalization, and age> 5 years.Results: An estimated 329,766
patients discharged from nonfederal hospitals nationwide in 1994met
study criteria for ARF. The incidence of ARF was 137.1
hospitalizations per 100,000 USresidents age > 5 years.
Incidence increased nearly exponentially each decade until age 85
years.Overall, 35.9% of patients with ARF did not survive to
hospital discharge. At 31 days, hospital
mortality was 31.4%. According to the proportional hazards
model, significant mortality hazardsincluded age (> 80 years and
> 30 years), multiorgan system failure (MOSF), HIV, chronic
liverdisease, and cancer. Hospital admission for coronary artery
bypass, drug overdose, or trauma otherthan head injury or burns was
associated with a reduced mortality hazard. Interaction was
presentbetween age and MOSF, trauma, and cancer. A point system
derived from the hazard model classifiedpatients into seven groups
with distinct 31-day survival probabilities ranging from 24 to
99%.Conclusions: The incidence of ARF increases markedly with age
and is especially high among persons> 65 years of age.
Nonpulmonary hazards explain short-term (31-day) survival.
(CHEST 2000; 118:11001105)
Key words: acute disease; adult; aged; child; hospital
mortality; incidence; respiratory insufficiency; survival analysis;
UnitedStates
Abbreviations: APACHE
acute physiology and chronic health evaluation; ARF
acute respiratory failure; BMT
bonemarrow transplant; CABG coronary artery bypass graft;
ICD-9-CM International Classification of Diseases, 9th
Revision,Clinical Modification; MOSFmultiorgan system failure
Apicture of the epidemiology of acute respiratory
failure (ARF) is emerging, but significant gapsremain. Surveys
of ICU patients have estimated theincidence of ARF to be 77.6 cases
per 100,000population age 15 years in Sweden, Denmark, andIceland
and 88.6 cases per 100,000 residents in
Berlin.1,2
The incidence of ARF in the United States,however, is unknown.
Rates of hospital mortalityamong ICU patients with a diagnosis of
ARF orrequiring mechanical ventilation range from 28 to58%.112
Higher mortality rates have been observed
among ARF patients with AIDS or hematologicmalignancy (65% and
83% mortality, respective-ly).13,14
Independent hazards for ARF mortality includeolder age,1,2,4
6,8,11,12,14 severe chronic comorbidities(HIV, active malignancy,
cirrhosis),1,5,6,810,12 certain
precipitating events (trauma,3,6,8,11
drug overdose,8,9
bone marrow transplant [BMT]13), and multipleorgan system
dysfunction or failure (MOSF).3,4,7,913
Mortality has also been associated with acute lunginjury9,12 or
bilateral infiltrates on chest radiograph,1
and with an elevated acute physiology score1,6,7 orAPACHE (acute
physiology and chronic health eval-uation) score.9,10
To my knowledge, no study to date has appliedsurvival analysis
to a representative cohort of USARF patients, surgical as well as
medical, children aswell as adults. Such a cohort can be extracted
from
*From Childrens Hospital, San Diego, CA.Manuscript received
November 16, 1999; revision acceptedMarch 28, 2000.Correspondence
to: Carolyn E. Behrendt, PhD, 4065 3413Pase o de l Campo, Palos V
erdes , CA 9 02 74 ; e -mail :[email protected]
1100 Clinical Investigations in Critical Care
2000 American College of Chest Physiciansby guest on November
15, 2010chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/
-
8/7/2019 Acute Respiratory Failure in the US - Incidence and 31
Day Survival
3/8
the Nationwide Inpatient Sample, a database of allpatients
discharged from a representative sample of904 nonfederal hospitals
throughout the UnitedStates during 1994.15 Using data on these
ARFpatients, the current study estimates age-specificincidences of
ARF and constructs a proportionalhazards model to explain the
associated hospitalmortality. These findings will enhance the
epidemi-
ologic picture of ARF, increasing the informationavailable to
support clinical decision making, coun-seling of ARF patients and
their families, and inves-tigation of new therapies.
Materials and Methods
Data Source
The 1994 Nationwide Inpatient Sample was designed toinclude
acute care discharges from representative hospitals acrossthe
United States during a 1-year period.15 A systematic random
sample of 904 hospitals was drawn from 2,135 nonfederal
generaland specialty hospitals stratified by geographic region,
urban orrural location, control (government nonfederal, private
not-for-profit, and private investor-owned), teaching status, and
bed size.All discharges from the selected hospitals were included,
for atotal of 6,385,011 inpatients. Available data included
patientdemographics, sampling weights, International Classification
ofDiseases, 9th Revision, Clinical Modification (ICD-9-CM)
dis-charge codes for diagnoses and procedures, duration of
hospital-ization, discharge disposition, and hospital
characteristics.
Definitions
Patients in the Nationwide Inpatient Sample were consideredto
have ARF if they had a diagnostic code for acute respiratory
distress or failure (ICD-9-CM 518.5, 518.81, or 518.82) together
with a procedure code for continuous mechanical
ventilation(ICD-9-CM 96.7). Such ventilation included positive
end-expi-ratory pressure but excluded continuous positive airway
pressure,intermittent positive-pressure breathing, and oxygen by
facemask or nasal cannula. Total hours of ventilation were
notrecorded in the database, so no minimum period of mechanical
ventilation was specified. Instead, ARF patients were limited
tothose who remained in the hospital at least 24 h. Infants
andchildren 5 years were excluded.
Additional clinical conditions were ascertained using ICD-9-CM
codes. MOSF was defined as one or more of the followingin addition
to respiratory failure: acute renal failure, cardiacarrest, shock,
acute cerebrovascular event, disseminated intravas-
cular coagulation, acute intestinal vascular insufficiency,
acutehepatic failure, head injury with loss of consciousness for 24
hor until death, and burns involving 20% of body surface.Trauma
refers to a primary diagnosis of crushing or internalinjury, open
wounds, superficial injury or contusion, sprains orstrains,
fractures other than isolated hip fracture, spinal cordinjury,
other injuries, or ARF with lung contusion. Head injury
with loss of consciousness for 24 h or until death and
burnsinvolving 20% of body surface were categorized as MOSFrather
than trauma.
Statistical Analysis
National sampling weights were used in all analyses (SUDAAN7.5.3
software; Research Triangle Institute; Research Triangle
Park, NC) except the generation of survival plots (SAS
6.12software; SAS Institute; Cary, NC). For the national estimates
ofARF incidence, US Census Bureau estimates of the
residentpopulation as of July 1, 1994, served as the population
denomi-nators.16
The SEs of proportions and 95% confidence intervals
aroundproportional hazard estimates were calculated using Taylor
serieslinearization.17,18 This method takes into account the
intraclustercorrelation that may result from the survey design,
which in-
cluded all patients at selected hospitals rather than
selectedpatients from all hospitals.The follow-up period began at
24 h after hospital admission
and continued through 31 days. After this time, the
acceleratednature of several hazards (age 80 years, MOSF, coronary
arterybypass graft [CABG], and drug overdose) undermined the
req-uisite assumption of proportional hazards.19 Survivors
includedpatients who were discharged alive at any time and also
those
who died in the hospital after the follow-up period; survival
timeswere censored at 31 days. Terms were retained in the
multivar-iate model if they were significant at p 0.0001 and
improvedthe 2 log-likelihood ratio.
Results
Patients
Among the Nationwide Inpatient Sample, 62,642patients with acute
respiratory distress or failurereceived mechanical ventilation and
were hospital-ized 24 h. After excluding the 2.3% of thesepatients
who were 5 years of age, a total of 61,223ARF patients remained.
Their median age was 69years (5th to 95th percentile range, 30 to
87 years).Children aged 5 to 17 years comprised 1.4% ofpatients.
Half (51.1%) of all patients were male.
The highest frequency of head injury, burns, andother trauma
combined (20.8%) was among patientsaged 30 years, whereas the
greatest prevalence ofcongestive heart failure (47.2%) and COPD
(39.0%)was among patients aged 50 years. The frequencyof asthma
decreased steadily with age, from 16.6%among children aged 5 to 17
years to 2.9% amongadults aged 80 years.
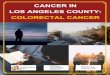
Incidence
The ARF patients in the sample corresponded to329,766 discharges
nationwide or 137.1 hospitaliza-
tions per 100,000 US residents aged 5 years. ARFincidence
increased markedly with age, resulting inan 88-fold difference in
risk between the youngestand oldest age groups (Fig 1).
Survival
Overall, 35.9 0.3% of ARF patients did notsurvive to hospital
discharge. Most (87.5%) deathsoccurred within the 31-day follow-up
period. Me-dian length of stay (5th to 95th percentile range) was13
days (3 to 55 days) among survivors and 10 days (1to 50 days) among
nonsurvivors.
CHEST / 118 / 4 / OCTOBER, 2000 1101
2000 American College of Chest Physiciansby guest on November
15, 2010chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/
-
8/7/2019 Acute Respiratory Failure in the US - Incidence and 31
Day Survival
4/8
A cohort of 61,113 ARF patients was appropriatefor survival
analysis. Patients admitted to the hospitalfor BMT (n 86 or 0.14%)
were excluded. Becauseof the variable lag time between admission
for BMTand onset of ARF, their survival curve could not bealigned
with that of the rest of the cohort. Another24 patients (0.04%) who
lacked data on survivalstatus at follow-up were also excluded.
At the end of 31 days, hospital mortality among thecohort was
31.4 0.2%. As shown in Table 1,hazards for 31-day mortality
included age, MOSF,
HIV, chronic liver disease, and cancer. Mortalityhazard was
significantly reduced among patientsadmitted for CABG, drug
overdose, or trauma otherthan head injury or burns (hereafter
referred tosimply as trauma).
Significant interaction was present between ageand MOSF, trauma,
and cancer. Mortality hazardincreased at age 30 years (but only
among patientswithout MOSF or trauma) and again at age 80
years.MOSF was a significant hazard among all age groupsbut had
proportionally greater impact among pa-tients aged 80 years,
especially those 30 years
and those admitted to the hospital for trauma.Cancer was a
significant hazard until age 80 years;thereafter, mortality among
patients with and with-out cancer did not differ.
Trauma patients aged 30 to 79 years who did notdevelop MOSF had
a mortality rate as low as thatamong uncomplicated patients aged 30
years; thesegroups were combined to serve as the models
referentcategory. The fit of the model was further improved
bycombining cancer and chronic liver disease into a singleterm
(severe chronic comorbidity) and by combining
drug overdose and CABG into another term (low-riskprecipitating
event). The model was not improved byincluding a term for
sepsis.
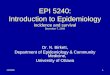
A point system, shown in the far right column ofTable 1,
converted the hazard profiles of individualpatients into scores
from 1 to 5 (Table 2). Theobserved survival curves associated with
these scores(Fig 2) were each significantly different from thenext
(log-rank test, p 0.001 for all pairs). Thesteepest curve was the
least smooth, owing to thesmall number of patients (n 101) with the
maxi-mum score.
Figure 1. Cases and incidence of ARF in the United States, 1994,
by age. Bars denote the numbersof ARF cases; diamonds indicate
incidence per 100,000 US residents. Age-specific incidence
estimatesare, from left to right, 9.7, 21.6, 32.3, 52.3, 99.9,
231.3, 493.5, 765.5, and 852.9 cases per 100,000.
1102 Clinical Investigations in Critical Care
2000 American College of Chest Physiciansby guest on November
15, 2010chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/
-
8/7/2019 Acute Respiratory Failure in the US - Incidence and 31
Day Survival
5/8
Discussion
As in previous studies of ARF incidence, thecurrent case
definition excluded persons who werenot admitted to a hospital as
well as inpatients who
did not receive mechanical ventilation or who weredischarged
within 24 h.1,2 Unlike earlier studies, thecurrent study did not
restrict ARF cases to ICUpatients and did not specify a minimum
period ofmechanical ventilation. These broader inclusion cri-teria
help to explain why the current study yielded ahigher incidence
estimate than previous studies. Thetrue incidence of ARF may have
been underesti-
mated, however, because the Nationwide InpatientSample did not
include patients admitted to federalhospitals and because some ARF
patients may nothave been coded as such at discharge.
The gap between the current estimate (137.1/100,000 residents
aged 5 years) and that previ-ously published from Berlin
(88.6/100,000 residents)narrows once the Berlin estimate has been
adjustedfor age.2 Adjustment is necessary because, whereasthe
entire population of Berlin served as the esti-mates denominator,
its numerator was restricted toARF cases 14 years. Assuming that
children 14
Table 2Survival Among ARF Patients (n 61,113)
by Hazard Score
Score nDeaths Through
31 Days, No.31-d Survival*
(SEM), %
1 267 2 99.3 (0.4)0 4,231 320 92.6 (0.3)1 25,344 4,794 81.2
(0.3)2 13,435 4,668 65.3 (0.4)3 11,274 5,389 52.4 (0.4)4 6,461
4,010 38.0 (0.5)5 101 78 24.0 (3.1)
Total 61,113 19,261 68.6 (0.2)
*Percent cumulative survival at 31 days, calculated using
nationalsampling weights.
Table 1Thirty-one-Day Hospital Mortality Among a Nationally
Representative Sample (n 61,113) of PatientsWith ARF*
Variables n
Observed31-d
Mortality, %
ProportionalHazard
(95% CI)HazardPoints
MOSFYes
Age 80 yr 3,879 59.9 8.55 (7.77, 9.41) 4
Age 3079 yr 13,773 50.5Age 1829 yr 503 44.3 5.86 (5.34, 6.43)
3Age 517 yr 179 32.4
NoAge 80 yr 8,228 32.3 3.69 (3.36, 4.05) 2Age 3079 yr without
trauma 31,024 21.3 2.07 (1.90, 2.27) 1Age 3079 yr with trauma 1,267
11.0Age 1829 yr 1,570 10.9 1.00 0Age 517 yr 690 6.5
HIV infectionYes 1,163 52.0 2.00 (1.86, 2.15) 1No 59,884 31.0
1.00
Severe chronic comorbidityCancer age 80 yr, no liver disease
4,990 45.2
Liver disease, no cancer age
80 yr 1,872 54.2 1.83 (1.77, 1.89)
1Both comorbidities 152 63.6Neither comorbidity 54,099 29.3
1.00
Low-risk precipitating eventDrug overdose or poisoning 1,280
17.9 0.39 (0.35, 0.43) 1CABG 1,140 7.8Neither event 58,693 32.2
1.00
*CI confidence interval.When these points are totaled according
to an individual patients characteristics, the resulting score
corresponds to one of seven 31-day survival
curves observed among ARF patients with the same score (see Fig
2).The frequency of MOSF (29.9% overall) was significantly higher
among those ARF patients who underwent CABG (51.9%) or who had
chronic
liver disease (48.2%) and significantly lower among trauma
patients (22.5%), children ages 5 to 17 years (20.7%), and patients
admitted for drugoverdose or poisoning (12.1%).
Trauma does not include head injury or burns; these conditions
are categorized instead as MOSF.
Mortality was not associated with sex, pneumonia, aspiration
pneumonitis, CHF, COPD, hypertension, diabetes mellitus,
interstitial lung disease,neuromuscular disease, GI hemorrhage,
pancreatitis, embolism, aneurysm, ketoacidosis, inhalational
injury, or near-drowning.
CHEST / 118 / 4 / OCTOBER, 2000 1103
2000 American College of Chest Physiciansby guest on November
15, 2010chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/
-
8/7/2019 Acute Respiratory Failure in the US - Incidence and 31
Day Survival
6/8
years comprised 20% of the Berlin population (as was the case in
the US population16), the age-
adjusted incidence of ARF in Berlin would beapproximately
110.8/100,000 residents aged 14years. It is unclear why another
European survey ofARF yielded a much lower estimate of 77.6
per100,000 population aged 15 years.1
The incidence of ARF was found to increasenearly exponentially
with each decade until age 85years. Comparable incidence estimates
by age havenot been published.
The current 36% rate of mortality before dis-charge was similar
to the 37% rate previouslyreported among ARF patients admitted to
40 US
hospitals6 and approached the 41% and 43% ratesreported among
ARF patients in two Europeansurveys.1,2 Whether ARF incidence or
mortalitydiffers significantly between the United States andEurope
cannot be determined at this time, be-cause of varying case
definitions among studies todate.
Because discharge data reflect the entire courseof
hospitalization rather than the initial day offollow-up, the
current survival analysis and thepoint system derived from it are
explanatory ratherthan prognostic. The current survival analysis
con-
firmed reports of associations between ARF mor-tality and older
age, MOSF, HIV, cancer, chronicliver disease, trauma, and drug
overdose.113 Theincrease in mortality at age 30 years and again
atage 80 years observed in the current study hasbeen noted in
previous studies of patients receiv-ing mechanical ventilation and
ARF patients.5,8,12
Also consistent with earlier studies was the currentlack of
association between ARF mortality and sex,pneumonia, COPD,
congestive heart failure, anddiabetes.15,9,10,14 The current data
did not confirman independent association between ARF mortal-ity
and sepsis.3,9
The current survival analysis reflects the limita-tions as well
as the strengths inherent in theNationwide Inpatient Sample
database. The lackof data on acute lung injury and acute
physiologicor APACHE score and the necessity of excludingBMT
patients precluded testing of these potentialhazards in the
multivariate model. However, thepresence of large numbers of
children, youngadults, and the elderly within the sample permit-ted
the significant interaction between age andother hazards for ARF
mortality to be detected forthe first time.
Figure 2. Plot of survival among ARF patients (n 61,113) by
hazard score.
1104 Clinical Investigations in Critical Care
2000 American College of Chest Physiciansby guest on November
15, 2010chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/
-
8/7/2019 Acute Respiratory Failure in the US - Incidence and 31
Day Survival
7/8
Conclusion
The incidence of ARF increases markedly with ageand is
especially high among persons 65 years ofage. Nonpulmonary hazards
explain short-term (31-day) survival.
ACKNOWLEDGMENT: The author thanks Alvaro Munoz,PhD, for valuable
advice on the survival analysis.
References
1 Luhr OR, Antonsen K, Karlsson M, et al. Incidence andmortality
after acute respiratory failure and acute respiratorydistress
syndrome in Sweden, Denmark, and Iceland. Am JRespir Crit Care Med
1999; 159:18491861
2 Lewandowski K, Metz J, Deutschmann H, et al.
Incidence,severity, and mortality of acute respiratory failure in
Berlin,Germany. Am J Respir Crit Care Med 1995; 151:11211125
3 Vasilyev S, Schaap RN, Mortensen JD. Hospital survival ratesof
patients with acute respiratory failure in modern respira-tory
intensive care units. Chest 1995; 107:10831088
4 Stauffer JL, Fayter NA, Graves B, et al. Survival
followingmechanical ventilation for acute respiratory failure in
adultmen. Chest 1993; 104:12221229
5 Swinburne AJ, Fedullo AJ, Bixby K, et al. Respiratory
failurein the elderly: analysis of outcome after treatment
withmechanical ventilation. Arch Intern Med 1993; 153:16571662
6 Knaus WA, Sun X, Hakim RB, et al. Evaluation of definitionsfor
adult respiratory distress syndrome. Am J Respir Crit CareMed 1994;
150:311317
7 Jimenez P, Torres A, Roca J, et al. Arterial oxygenation
doesnot predict outcome of patients with acute respiratory
failureneeding mechanical ventilation. Eur Respir J 1994;
7:730735
8 Cohen IL, Lambrinos JL. Investigating the impact of age
onoutcome of mechanical ventilation using a population of41,848
patients from a statewide database. Chest 1995;107:16731680
9 Epstein SK, Vuong V. Lack of influence of gender onoutcomes of
mechanically ventilated medical ICU patients.Chest 1999;
116:732739
10 Knaus WA. Prognosis with mechanical ventilation: the
influ-ence of disease, severity of disease, age, and chronic
health
status on survival from an acute illness. Am Rev Respir Dis1989;
140:S8S13
11 Gracey DR, Naessens JM, Krishan I, et al. Hospital
andposthospital survival in patients mechanically ventilated
formore than 29 days. Chest 1992; 101:211214
12 Pascual FE, Matthay MA, Bacchetti P, et al. Assessment
ofprognosis in patients with community-acquired pneumonia
who require mechanical ventilation. Chest 2000;117:50351213
Montaner JSG, Hawley PH, Ronco JJ, et al. Multisystem
organ failure predicts mortality of ICU patients with
acuterespiratory failure secondary to AIDS-related PCP. Chest1992;
102:18231828
14 Epner DE, White P, Krasnoff M, et al. Outcome of mechan-ical
ventilation for adults with hematologic malignancy. J In-
vest Med 1996; 44:25426015 Healthcare Cost, and Utilization
Project Nationwide Inpa-tient Sample, release 3, 1994, CD-ROM.
Rockville, MD: USDepartment of Health and Human Services, Agency
forHealthcare Research and Quality, 1996
16 Statistical abstract of the United States 1995: resident
popu-lation by age and state 1994. 115th ed. Washington, DC:
USBureau of the Census, 1995; 33
17 Binder D. On the variances of asymptotically normal
estima-tors from complex surveys. Int Stat Rev 1983; 51:279292
18 Binder D. Fitting Coxs proportional hazards models fromsurvey
data. Biometrika 1992; 79:139147
19 Lawless JF. Statistical models and methods for lifetime
data.New York, NY: John Wiley and Sons, 1982; 279
CHEST / 118 / 4 / OCTOBER, 2000 1105
2000 American College of Chest Physiciansby guest on November
15, 2010chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/
-
8/7/2019 Acute Respiratory Failure in the US - Incidence and 31
Day Survival
8/8
DOI 10.1378/chest.118.4.11002000;118; 1100-1105Chest
Carolyn E. BehrendtSurvival
: Incidence and 31-Day*Acute Respiratory Failure in the United
States
November 15, 2010This information is current as of
http://chestjournal.chestpubs.org/content/118/4/1100.full.htmlUpdated
Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/118/4/1100.full.html#ref-list-1This
article cites 16 articles, 13 of which can be accessed free at:
References
http://chestjournal.chestpubs.org/content/118/4/1100.full.html#related-urlsThis
article has been cited by 15 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlfound online
at:Information about reproducing this article in parts (figures,
tables) or in its entirety can bePermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation
about ordering reprints can be found online:
Reprints
"Services" link to the right of the online article.Receive free
e-mail alerts when new articles cite this article. To sign up,
select the
Citation Alerts
PowerPoint slide format. See any online figure for
directions.
articles can be downloaded for teaching purposes inCHESTFigures
that appear inImages in PowerPoint format
2000 A i C ll f Ch t Ph i iby guest on November 15,
2010chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/content/118/4/1100.full.htmlhttp://chestjournal.chestpubs.org/content/118/4/1100.full.htmlhttp://chestjournal.chestpubs.org/content/118/4/1100.full.htmlhttp://chestjournal.chestpubs.org/content/118/4/1100.full.html#ref-list-1http://chestjournal.chestpubs.org/content/118/4/1100.full.html#ref-list-1http://chestjournal.chestpubs.org/content/118/4/1100.full.html#related-urlshttp://chestjournal.chestpubs.org/content/118/4/1100.full.html#related-urlshttp://www.chestpubs.org/site/misc/reprints.xhtmlhttp://www.chestpubs.org/site/misc/reprints.xhtmlhttp://www.chestpubs.org/site/misc/reprints.xhtmlhttp://www.chestpubs.org/site/misc/reprints.xhtmlhttp://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://www.chestpubs.org/site/misc/reprints.xhtmlhttp://www.chestpubs.org/site/misc/reprints.xhtmlhttp://chestjournal.chestpubs.org/content/118/4/1100.full.html#related-urlshttp://chestjournal.chestpubs.org/content/118/4/1100.full.html#ref-list-1http://chestjournal.chestpubs.org/content/118/4/1100.full.html