Embed Size (px)
Citation preview
ACCMS
AohbBfe
Pw1lpgbao
CAaomiorbo4bMm
FRT
FHr
©A
Case Report
cute Renal Papillary Necrosis withomplete Bilateral Ureteral Obstruction in ahild
orris Gordon, Raimondo M. Cervellione, Robert Postlethwaite, Abdu Shabani, andupul Hennayake
9-year-old girl presented with apparent meningococcal septicemia and developed acute renal failure after 48 hoursf treatment with antibiotics and analgesics. Early ultrasound scanning demonstrated mild bilateral hydronephrosis andydroureter. Intravenous urography showed slow contrast uptake with delay nephrogram and no contrast entering theladder. Repeat ultrasonography revealed bilateral papillary irregularity and echogenic debris in the distal ureters.ilateral double-J stents were inserted cystoscopically, resulting in prompt polyuria and a return of normal renal
unction. Although rare, recognition of sloughed papilla in papillary necrosis causing ureteral obstruction can lead to
arly management with no long-term sequelae. UROLOGY 69: 575.e11–575.e12, 2007. © 2007 Elsevier Inc.1wbisArudiRs(csj
uebthtrirmAc
CFq
apillary necrosis is a rare condition characterizedby disruption of the renal papillae and, conse-quently, decreased renal function. The first case
as recognized and reported in adults by Freidreich in877,1 and very few reports are available in the pediatriciterature.2,3 It has also been recognized in adults thatapillary necrosis can cause ureteral obstruction by mi-ration of the sloughed papilla into the ureters.4–7 Weelieve this is the first report of a child who developedcute papillary necrosis and bilateral complete ureteralbstruction that required surgical intervention.
ASE REPORT9-year-old white girl presented to a local hospital with
2-day history of fever, vomiting, and erythematous rashn her chest and back. She was suspected of havingeningococcal septicemia and was started on ceftriaxone
ntravenously, as well as paracetamol and ibuprofenrally. Her pyrexia quickly settled, as did her rash. Sheemained well perfused, with normal blood pressure, andlood cultures showed no growth. However, poor urineutput was noted during her stay that had progressed at8 hours into the admission to complete anuria, withiochemical renal failure. She was transferred to Royalanchester Children’s Hospital. On arrival, she was re-arkably well, apart from abdominal pain. Her urea was
rom the Departments of Paediatric Urology, Paediatric Nephrology, and Paediatricadiology, Central Manchester and Manchester Children’s University Hospitals NHSrust, Manchester, United KingdomAddress for correspondence: Raimondo Maximilian Cervellione, M.B.Ch.B,
.R.C.S, Department of Paediatric Urology, Royal Manchester Children’s Hospital,ospital Road, Pendlebury, Manchester M27 4HA, United Kingdom. E-mail:
Submitted: July 28, 2006; accepted (with revisions): January 5, 2007
2007 Elsevier Inc.ll Rights Reserved
2.0 mmol/L (normal range 2.5 to 8.5), her creatinineas 570 �mol/L (normal range 30 to 140), and a fulllood count was normal. A urethral catheter was passedn the bladder, but no urine was obtained. Early ultra-onography showed mild bilateral hydroureteronephrosis.n abdominal x-ray showed no evidence of radiopaque
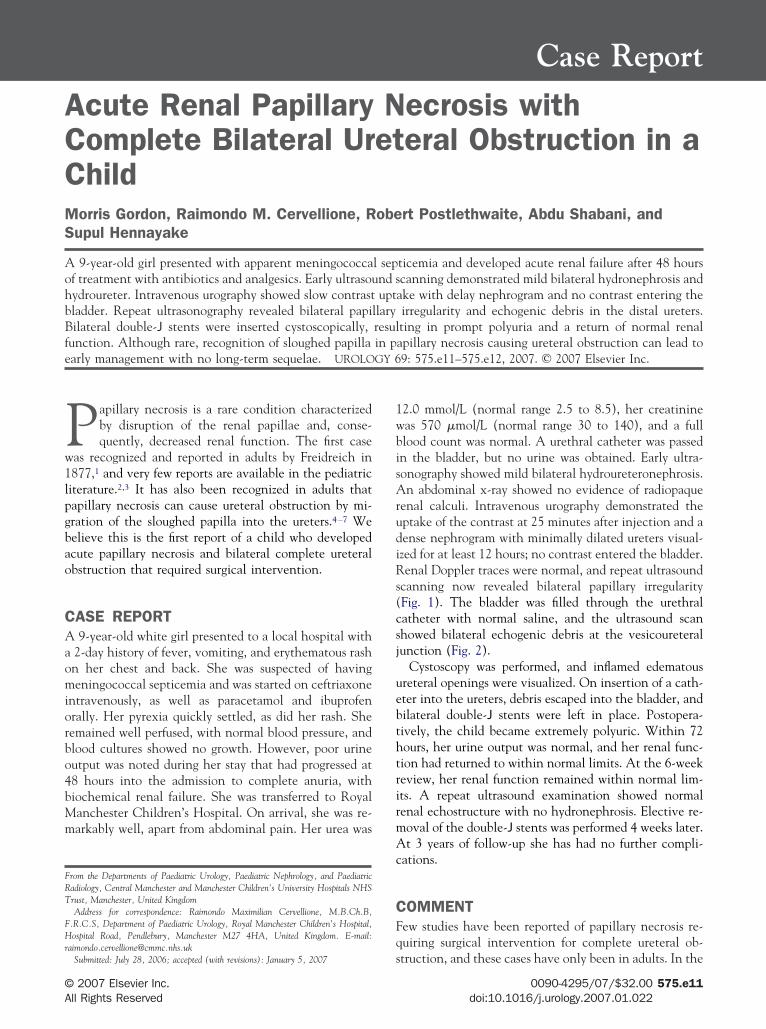
enal calculi. Intravenous urography demonstrated theptake of the contrast at 25 minutes after injection and aense nephrogram with minimally dilated ureters visual-zed for at least 12 hours; no contrast entered the bladder.enal Doppler traces were normal, and repeat ultrasound
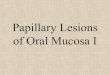
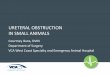
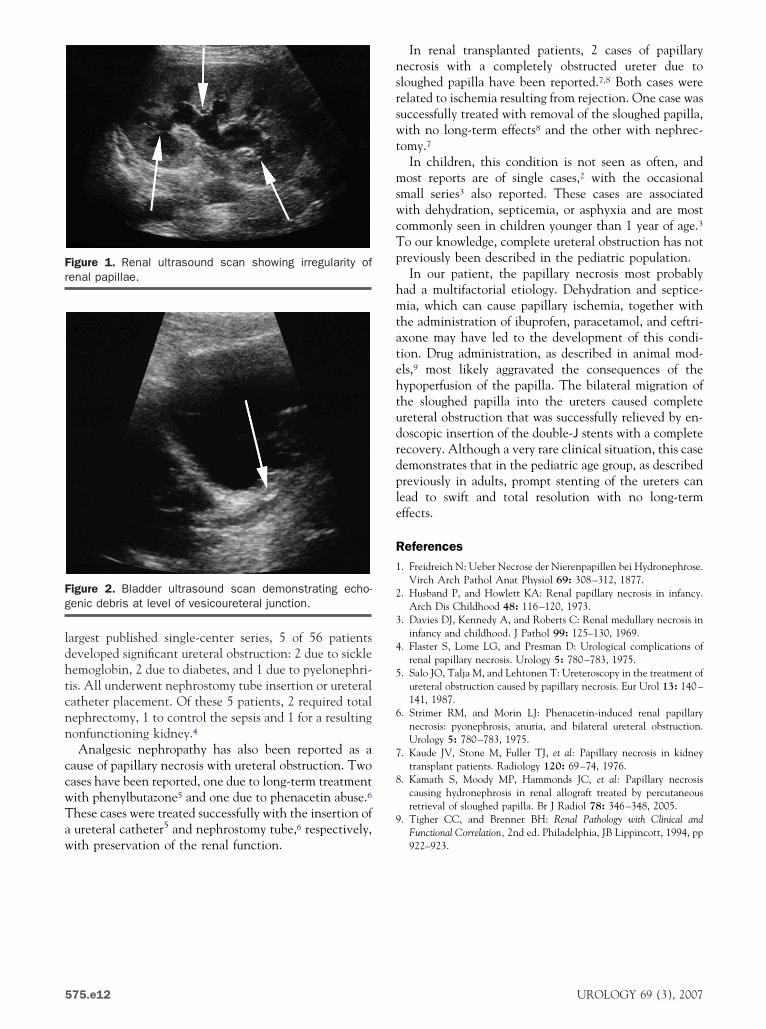
canning now revealed bilateral papillary irregularityFig. 1). The bladder was filled through the urethralatheter with normal saline, and the ultrasound scanhowed bilateral echogenic debris at the vesicoureteralunction (Fig. 2).
Cystoscopy was performed, and inflamed edematousreteral openings were visualized. On insertion of a cath-ter into the ureters, debris escaped into the bladder, andilateral double-J stents were left in place. Postopera-ively, the child became extremely polyuric. Within 72ours, her urine output was normal, and her renal func-ion had returned to within normal limits. At the 6-weekeview, her renal function remained within normal lim-ts. A repeat ultrasound examination showed normalenal echostructure with no hydronephrosis. Elective re-oval of the double-J stents was performed 4 weeks later.t 3 years of follow-up she has had no further compli-
ations.
OMMENTew studies have been reported of papillary necrosis re-uiring surgical intervention for complete ureteral ob-
truction, and these cases have only been in adults. In the0090-4295/07/$32.00 575.e11doi:10.1016/j.urology.2007.01.022
ldhtcnn
ccwTaw
nsrswt
mswcTp
hmtatehtudrdple
R1
2
3
4
5
6
7
8
9
Fr
Fg
5
argest published single-center series, 5 of 56 patientseveloped significant ureteral obstruction: 2 due to sickleemoglobin, 2 due to diabetes, and 1 due to pyelonephri-is. All underwent nephrostomy tube insertion or ureteralatheter placement. Of these 5 patients, 2 required totalephrectomy, 1 to control the sepsis and 1 for a resultingonfunctioning kidney.4Analgesic nephropathy has also been reported as a
ause of papillary necrosis with ureteral obstruction. Twoases have been reported, one due to long-term treatmentith phenylbutazone5 and one due to phenacetin abuse.6hese cases were treated successfully with the insertion ofureteral catheter5 and nephrostomy tube,6 respectively,
igure 1. Renal ultrasound scan showing irregularity ofenal papillae.
igure 2. Bladder ultrasound scan demonstrating echo-enic debris at level of vesicoureteral junction.
ith preservation of the renal function.
75.e12
In renal transplanted patients, 2 cases of papillaryecrosis with a completely obstructed ureter due toloughed papilla have been reported.7,8 Both cases wereelated to ischemia resulting from rejection. One case wasuccessfully treated with removal of the sloughed papilla,ith no long-term effects8 and the other with nephrec-
omy.7In children, this condition is not seen as often, andost reports are of single cases,2 with the occasional
mall series3 also reported. These cases are associatedith dehydration, septicemia, or asphyxia and are mostommonly seen in children younger than 1 year of age.3o our knowledge, complete ureteral obstruction has notreviously been described in the pediatric population.In our patient, the papillary necrosis most probably
ad a multifactorial etiology. Dehydration and septice-ia, which can cause papillary ischemia, together with
he administration of ibuprofen, paracetamol, and ceftri-xone may have led to the development of this condi-ion. Drug administration, as described in animal mod-ls,9 most likely aggravated the consequences of theypoperfusion of the papilla. The bilateral migration ofhe sloughed papilla into the ureters caused completereteral obstruction that was successfully relieved by en-oscopic insertion of the double-J stents with a completeecovery. Although a very rare clinical situation, this caseemonstrates that in the pediatric age group, as describedreviously in adults, prompt stenting of the ureters canead to swift and total resolution with no long-termffects.
eferences. Freidreich N: Ueber Necrose der Nierenpapillen bei Hydronephrose.
Virch Arch Pathol Anat Physiol 69: 308–312, 1877.. Husband P, and Howlett KA: Renal papillary necrosis in infancy.
Arch Dis Childhood 48: 116–120, 1973.. Davies DJ, Kennedy A, and Roberts C: Renal medullary necrosis in
infancy and childhood. J Pathol 99: 125–130, 1969.. Flaster S, Lome LG, and Presman D: Urological complications of
renal papillary necrosis. Urology 5: 780–783, 1975.. Salo JO, Talja M, and Lehtonen T: Ureteroscopy in the treatment of
ureteral obstruction caused by papillary necrosis. Eur Urol 13: 140–141, 1987.
. Strimer RM, and Morin LJ: Phenacetin-induced renal papillarynecrosis: pyonephrosis, anuria, and bilateral ureteral obstruction.Urology 5: 780–783, 1975.
. Kaude JV, Stone M, Fuller TJ, et al: Papillary necrosis in kidneytransplant patients. Radiology 120: 69–74, 1976.
. Kamath S, Moody MP, Hammonds JC, et al: Papillary necrosiscausing hydronephrosis in renal allograft treated by percutaneousretrieval of sloughed papilla. Br J Radiol 78: 346–348, 2005.
. Tigher CC, and Brenner BH: Renal Pathology with Clinical andFunctional Correlation, 2nd ed. Philadelphia, JB Lippincott, 1994, pp
922–923.UROLOGY 69 (3), 2007