Embed Size (px)
Citation preview
Acute PancreatitisDoes Gender Matter?
PAUL GEORG LANKISCH, MD,* CHRISTINE ASSMUS, MD,* DIRK LEHNICK, DSc,†PATRICK MAISONNEUVE, MD,‡ and ALBERT B. LOWENFELS, MD§
In a number of gastrointestinal and nongastrointestinal diseases, gender has been proven tobe an independent risk factor for severity. To determine whether this holds true for severityin acute pancreatitis is the aim of our study. This paper derives from a prospective study onthe epidemiology of acute pancreatitis, which included 274 patients (172 male and 102female) with a first attack of the disease. Severity parameters were: Atlanta criteria (arterialPO2 � 60 mm Hg, and serum creatinine on admission �2 mg/dl after rehydration); Ranson’sand Imrie’s prognostic factors; APACHE II score; Balthazar-scored contrast-enhancedcomputed tomography (CT) results obtained within 72 hr of admission; days spent in theintensive care unit and total hospital stay; the necessity for artificial ventilation, dialysis, orsurgery; and mortality. As already known, there is a significant association between genderand etiology of pancreatitis in general. Not surprisingly, the men in our study had alcohol-induced acute pancreatitis more frequently than women, whereas biliary pancreatitis pre-dominated among the women. As for severity, there was no significant association betweengender and any of the severity parameters with a few minor exceptions: longer hospital stays,higher Imrie scores and more pseudocysts for women, and more necroses in women withidiopathic pancreatitis. Thus, gender is no independent risk factor for the severity andoutcome of acute pancreatitis.
KEY WORDS: acute pancreatitis; gender; etiology; prognostic scores; severity; mortality.
According to reports over the years, many diseasesshow a gender bias. The insights from these reportsinto the pathophysiology of these illnesses are impor-tant for diagnosis and assessment of severity andtreatment. They can also help set policies for medicalresource utilization (1, 2). Whether the severity of
acute pancreatitis also shows a gender bias is thequestion addressed by this study.
MATERIALS AND METHODS
This study is one of the outcomes of a prospective inves-tigation on the epidemiology of acute pancreatitis under-taken in the Municipal Clinic of Luneburg, which serves asthe only hospital for a community of 150,000 inhabitants.Patients totaled 274, and included those admitted with afirst attack of acute pancreatitis from 1988 to 1999. Thediagnosis was based on characteristic signs and symptoms,enzyme elevation (amylase and/or lipase), and the Baltha-zar-scored results of a contrast-enhanced computed tomog-raphy (CT) within 72 hr of admission (3, 4). In addition tothe Balthazar scores, other parameters of severity were theAtlanta definitions of initial organ failure (5): shock (sys-tolic blood pressure �90 mm Hg); respiratory insufficiency(arterial PO2 � 60 mm Hg, N � 154); renal insufficiency(serum creatinine �2 mg/dl after rehydration); gastrointes-tinal bleeding (�500 cc/24 hr). Since none of our patients
Manuscript received December 17, 2000; revised manuscriptreceived May 25, 2001; accepted May 28, 2001.
From the *Department of Internal Medicine, Municipal Clinicof Luneburg, Luneburg; †Institute for Statistics and Econometrics,University of Gottingen, Gottingen, Germany; ‡European Instituteof Oncology, Milano, Italy, and §New York Medical College,Valhalla, New York.
P. Maisonneuve received support from the Italian Associationfor Cancer Research [Associazione Italiana per la Ricerca sulCancro (AIRC)], and A.B. Lowenfels was supported by the C.D.Smithers Foundation and Solvay Pharmaceuticals, which is grate-fully acknowledged.
Address for reprint requests: Prof. Dr. P.G. Lankisch, Medi-zinische Klinik, Staedtisches Klinikum Lueneburg, Boegelstrasse 1,D-21339 Lueneburg, Germany.
Digestive Diseases and Sciences, Vol. 46, No. 11 (November 2001), pp. 2470–2474 (© 2001)
2470 Digestive Diseases and Sciences, Vol. 46, No. 11 (November 2001)0163-2116/01/1100-2470$19.50/0 © 2001 Plenum Publishing Corporation
had an initial shock or gastrointestinal bleeding, initialorgan failure or organ failure on admission in our studycomprise only respiratory and/or renal insufficiency. Fur-ther severity parameters were days spent in the intensivecare unit and total hospital stay; the Ranson score adjustedfor etiology (6, 7); the Imrie score (8); the APACHE IIscore (9); the need for artificial ventilation, dialysis, orsurgery (necrosectomy); and mortality.
Etiological classifications were standard. Biliary diseasewas deemed present when gallstones were found in thegallbladder or in the common bile duct by ultrasound, CT,or endoscopic retrograde cholangiopancreatography(ERCP). Alcohol abuse was taken as the etiology when thepatient or relatives reported regular alcohol consumption ofmore than 3 liters/day of beer, or more than 120 g/day ofpure alcohol in the form of wine or schnapps, or an alcoholexcess immediately preceding the attack of acute pancre-atitis. Other etiologies were attributed to endoscopic pro-cedures (ERCP), hyperlipidemia, trauma, Salmonella infec-tion, or drugs. In the remaining idiopathic cases, etiologywas classified as unknown.
For statistical analysis, rate ratios, �2 test of indepen-dence, and the Wilcoxon rank sum test were used.
RESULTS
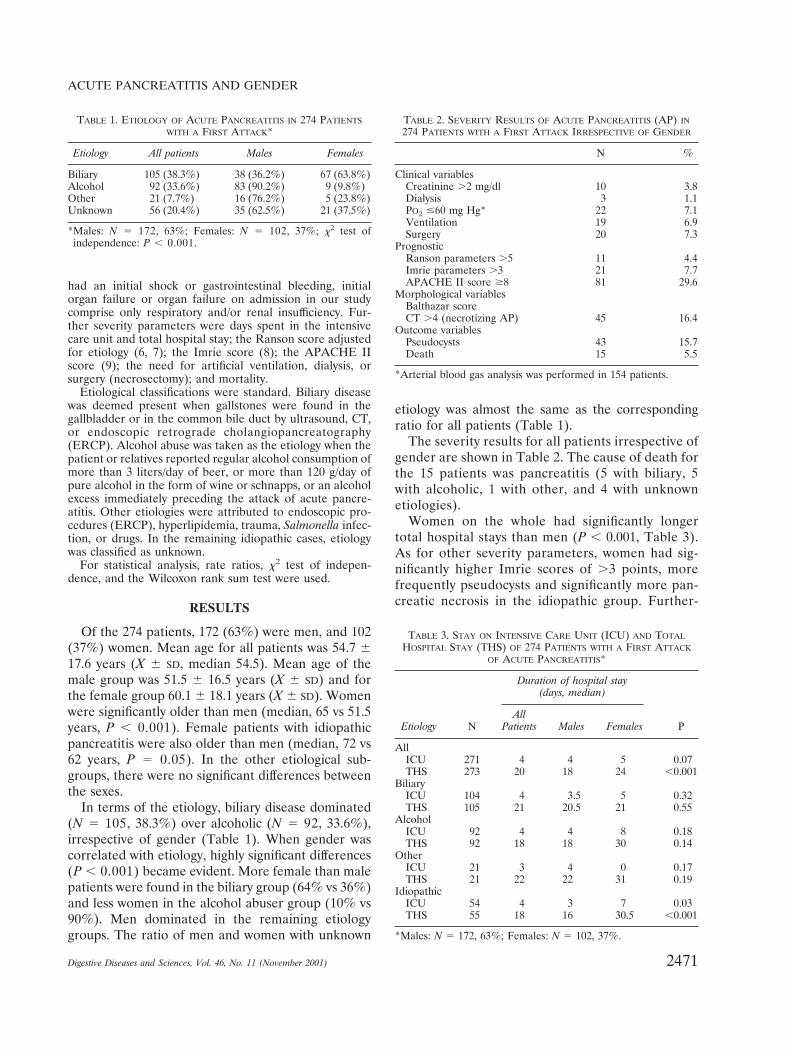
Of the 274 patients, 172 (63%) were men, and 102(37%) women. Mean age for all patients was 54.7 �17.6 years (X � SD, median 54.5). Mean age of themale group was 51.5 � 16.5 years (X � SD) and forthe female group 60.1 � 18.1 years (X � SD). Womenwere significantly older than men (median, 65 vs 51.5years, P � 0.001). Female patients with idiopathicpancreatitis were also older than men (median, 72 vs62 years, P � 0.05). In the other etiological sub-groups, there were no significant differences betweenthe sexes.
In terms of the etiology, biliary disease dominated(N � 105, 38.3%) over alcoholic (N � 92, 33.6%),irrespective of gender (Table 1). When gender wascorrelated with etiology, highly significant differences(P � 0.001) became evident. More female than malepatients were found in the biliary group (64% vs 36%)and less women in the alcohol abuser group (10% vs90%). Men dominated in the remaining etiologygroups. The ratio of men and women with unknown
etiology was almost the same as the correspondingratio for all patients (Table 1).
The severity results for all patients irrespective ofgender are shown in Table 2. The cause of death forthe 15 patients was pancreatitis (5 with biliary, 5with alcoholic, 1 with other, and 4 with unknownetiologies).
Women on the whole had significantly longertotal hospital stays than men (P � 0.001, Table 3).As for other severity parameters, women had sig-nificantly higher Imrie scores of �3 points, morefrequently pseudocysts and significantly more pan-creatic necrosis in the idiopathic group. Further-
TABLE 1. ETIOLOGY OF ACUTE PANCREATITIS IN 274 PATIENTSWITH A FIRST ATTACK*
Etiology All patients Males Females
Biliary 105 (38.3%) 38 (36.2%) 67 (63.8%)Alcohol 92 (33.6%) 83 (90.2%) 9 (9.8%)Other 21 (7.7%) 16 (76.2%) 5 (23.8%)Unknown 56 (20.4%) 35 (62.5%) 21 (37.5%)
*Males: N � 172, 63%; Females: N � 102, 37%; �2 test ofindependence: P � 0.001.
TABLE 2. SEVERITY RESULTS OF ACUTE PANCREATITIS (AP) IN274 PATIENTS WITH A FIRST ATTACK IRRESPECTIVE OF GENDER
N %
Clinical variablesCreatinine �2 mg/dl 10 3.8Dialysis 3 1.1PO2 �60 mg Hg* 22 7.1Ventilation 19 6.9Surgery 20 7.3
PrognosticRanson parameters �5 11 4.4Imrie parameters �3 21 7.7APACHE II score �8 81 29.6
Morphological variablesBalthazar scoreCT �4 (necrotizing AP) 45 16.4
Outcome variablesPseudocysts 43 15.7Death 15 5.5
*Arterial blood gas analysis was performed in 154 patients.
TABLE 3. STAY ON INTENSIVE CARE UNIT (ICU) AND TOTALHOSPITAL STAY (THS) OF 274 PATIENTS WITH A FIRST ATTACK
OF ACUTE PANCREATITIS*
Etiology N
Duration of hospital stay(days, median)
PAll
Patients Males Females
AllICU 271 4 4 5 0.07THS 273 20 18 24 �0.001
BiliaryICU 104 4 3.5 5 0.32THS 105 21 20.5 21 0.55
AlcoholICU 92 4 4 8 0.18THS 92 18 18 30 0.14
OtherICU 21 3 4 0 0.17THS 21 22 22 31 0.19
IdiopathicICU 54 4 3 7 0.03THS 55 18 16 30.5 �0.001
*Males: N � 172, 63%; Females: N � 102, 37%.
ACUTE PANCREATITIS AND GENDER
2471Digestive Diseases and Sciences, Vol. 46, No. 11 (November 2001)
TA
BL
E4.
RA
TE
RA
TIO
SV
SC
HA
RA
CT
ER
IST
ICS
OF
274
PAT
IEN
TS
WIT
HA
FIR
STA
TT
AC
KO
FA
CU
TE
PAN
CR
EA
TIT
IS*
All
Bili
ary
Alc
ohol
Oth
erId
iopa
thic
NR
R(a
dj)
95%
CI
NR
R95
%C
IN
RR
95%
CI
NR
R95
%C
IN
RR
95%
-CI
Clin
ical
vari
able
sC
reat
inin
e�
2m
g/dl
265
0.47
[0.1
3;1.
70]
105
0.35
[0.0
2;7.
12]
890.
38[0
.07;
2.01
]19
0.13
[0.0
1;2.
66]
521.
89[0
.08;
44.2
7]D
ialy
sis
274
0.45
[0.0
6;3.
23]
105
1.75
[0.0
4;86
.61]
920.
11[0
.00;
5.41
]21
0.33
[0.0
1;14
.89]
560.
36[0
.05;
2.56
]PO
2�
60m
mH
g*†
154
0.59
[0.2
2;1.
57]
561.
25[0
.18;
8.75
]63
0.29
[0.0
4;1.
95]
100.
79[0
.06;
9.63
]25
0.41
[0.0
6;2.
63]
Ven
tilat
ion
274
1.24
[0.3
5;4.
35]
105
1.75
[0.1
9;16
.28]
922.
62[0
.17;
40.9
7]21
1.00
[0.0
5;21
.15]
560.
20[0
.03;
1.18
]Su
rger
y27
41.
63[0
.49;
5.38
]10
52.
92[0
.40;
21.2
7]92
2.84
[0.1
8;44
.31]
211.
00[0
.05;
21.1
5]56
0.26
[0.0
4;1.
63]
Prog
nost
icpa
ram
eter
sR
anso
n�
527
30.
62[0
.24;
1.61
]10
51.
05[0
.14;
7.66
]92
0.42
[0.0
8;2.
23]
210.
33[0
.01;
14.8
9]55
0.58
[0.0
6;5.
20]
Imri
e�
327
30.
34[0
.16;
0.75
]10
50.
35[0
.06;
1.93
]92
0.30
[0.0
8;1.
08]
210.
33[0
.01;
14.8
9]55
0.41
[0.0
9;1.
90]
Apa
che
�7
274
0.99
[0.5
7;1.
71]
105
0.89
[0.5
6;1.
42]
921.
10[0
.24;
5.14
]21
1.67
[0.0
9;29
.66]
560.
82[0
.40;
1.66
]M
orph
olog
ical
vari
able
sB
alth
azar
scor
eC
T�
4(n
ecro
tizin
gA
P)27
40.
79[0
.43;
1.45
]10
50.
94[0
.27;
3.25
]92
1.07
[0.3
5;3.
27]
212.
33[0
.14;
38.4
4]56
0.23
[0.0
6;0.
90]
Out
com
eva
riab
les
Pseu
docy
sts
274
0.57
[0.3
5;0.
92]
105
0.93
[0.3
2;2.
71]
920.
52[0
.24;
1.12
]21
0.56
[0.0
9;3.
29]
560.
26[0
.04;
1.63
]D
eath
274
1.37
[0.4
5;4.
22]
105
2.45
[0.5
1;11
.85]
921.
25[0
.07;
20.9
2]21
1.00
[0.0
5;21
.15]
560.
61[0
.11;
3.21
]
*Mal
es:N
�17
2,63
%;F
emal
es:N
�10
2,37
%;a
confi
denc
ein
terv
al�
1(b
oth
low
eran
dup
per
boun
d)in
dica
tes
ahi
ghri
skfo
rfe
mal
epa
tient
s.R
R,r
ate
ratio
;RR
(adj
),ra
tera
tio(a
djus
ted
for
etio
logy
);C
I,co
nfide
nce
inte
rval
;AP,
acut
epa
ncre
atiti
s.†A
rter
ialb
lood
gas
anal
ysis
was
perf
orm
edin
154
patie
nts.
LANKISCH ET AL
2472 Digestive Diseases and Sciences, Vol. 46, No. 11 (November 2001)

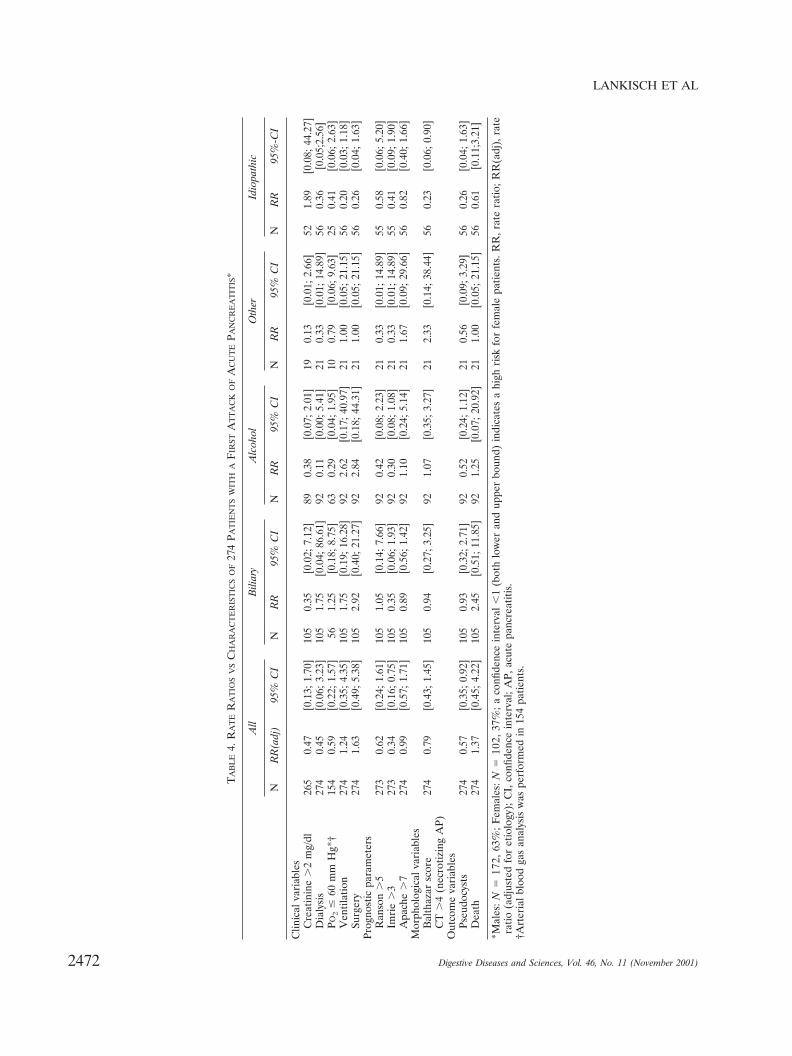
more, women had higher, although not significantlyso, values for all other severity parameters only inthe idiopathic group with the exception of serumcreatinine (Table 3). Apart from these exceptions,there were no significant associations between gen-der and severity (Table 4).
DISCUSSION
Gender-based differences in diagnosis, treatment,and outcome of diseases have been reported in thelast decades in connection with numerous disorders.For example, in the United States, it was found thatphysicians seem to pursue a less aggressive manage-ment course for coronary disease in women than inmen (10), with the result that women who are hospi-talized for that disease undergo fewer major diagnos-tic and therapeutic procedures than men (11). Arecent large study from Spain (12) has shown theneed for overcoming the gender bias in coronarymanagement since women were found to have morelethal and severe first acute myocardial infarctionthan men, irrespective of comorbidity, age, or previ-ous angina.
In comparison to the number of studies on otherdiseases, the number on gender bias in gastrointesti-nal disorders is lower, as a literature search that weundertook revealed (Medline and HealthStar data-base, 1965–1998).
Most of these gastrointestinal studies deal only withgender distribution and not with differences concern-ing severity. Zarling and Bernsen (1) showed in anIllinois-wide study 20 conditions that predominateamong women, eight that predominate among men,and 20 showing no significant female–male differ-ences, including ulcerative colitis. In contrast, an Ital-ian nationwide study (13) showed gender differencesfor ulcerative colitis (male–female ratio of 1.7).
During the last five decades, 20 studies on acutepancreatitis with more than 100 patients each havebeen published, showing detailed gender data distri-bution and etiology (14–33). Of all 7097 patients,55% were male and 45% female (median values).Worldwide, the main etiology was biliary tract disease(41%), followed by alcohol abuse (31.7%).
The definition of “unknown” etiology of acute pan-creatitis and “other” etiologies differed so muchamong the investigations, that no percentages can berepresentative (14–33). The percentages of patientswith biliary tract disease and alcohol abuse in ourstudy (38.3% and 33.6%) agree with the worldwidestudies.
While it has been consistently found that womenpredominate among patients with biliary acute pan-creatitis (16, 17, 24, 25, 34, 35), the gender ratio seemsto change according to two factors: the presence ofgallstones and age. Acute pancreatitis seems to occurmore frequently in men than in women with gall-stones (36). Taylor et al (35) investigated 664 patientswith gallstones, with a male–female patient ratio of1:2.8. Despite the bias towards women, a higher per-centage of men had a history of acute pancreatitis(N � 25, 14.4%) than women (N � 27, 5.5%). Interms of age, Imrie et al (16) found that more menhad biliary acute pancreatitis than women amongpatients older than 61 years. A recent survey in theCounty of Luneburg revealed that although therewere more female than male patients with biliarypancreatitis (ie, with gallstones and without cholecys-tectomy), the rate for biliary pancreatitis was higherfor male than female patients (75 vs 58.1/100,000/y),and this was especially true for the older age group(61–70 years) (37).
None of the 20 studies on acute pancreatitis (14–33), except that of Pezzilli et al (33), have dealt withgender distribution in terms of severity. Pezzilli et al(33) reported recently that male sex positively corre-lated with severity, a conclusion that is difficult toaccept. In their study, 70.9% of the patients hadbiliary etiology. This is the highest incidence in all 20studies. Our incidence was 38%, which correspondsto these other studies (14–33). Furthermore, the dis-tribution of women in all etiological groups wasskewed, since there were no women with alcoholic orother etiology and only two women in the idiopathicgroup. Thus, Pezzilli’s findings may not be represen-tative. This makes comparison difficult.
In conclusion, our prospective, community-basedstudy with a substantial number of patients showsthat gender is not an independent risk factor for theseverity of acute pancreatitis in general. There weresome exceptions: longer total hospital stay forwomen in general, higher lmrie scores, morepseudocysts, and in the idiopathic group, a longerstay on intensive care unit, and more necrosis. Partof the difference may be explained by a higher agefor women in the idiopathic group. Interestingly,Browder et al (38) found earlier a severe prognosisfor patients �60 years of age in this group. Otherpossible reasons for these differences have to beclarified in further studies.
ACUTE PANCREATITIS AND GENDER
2473Digestive Diseases and Sciences, Vol. 46, No. 11 (November 2001)

REFERENCES
1. Zarling EJ, Bernsen MB: The effect of gender on the rates ofhospitalization for gastrointestinal illnesses. Am J Gastroen-terol 92:621–623, 1997
2. Karlstadt RG: Gender differences—do they really count?Am J Gastroenterol 93:671–673, 1998
3. Balthazar EJ, Ranson JHC, Naidich DP, Megibow AJ, Cac-cavale R, Cooper MM: Acute pancreatitis: prognostic value ofCT. Radiology 156:767–772, 1985
4. Balthazar EJ, Robinson DL, Megibow AJ, Ranson JHC: Acutepancreatitis: Value of CT in establishing prognosis. Radiology174:331–336, 1990
5. Bradley III EL: A clinically based classification system foracute pancreatitis. Summary of the International Symposiumon Acute Pancreatitis, Atlanta, Georgia, September 11–13,1992. Arch Surg 128:586–590, 1993
6. Ranson JHC, Rifkind KM, Roses DF, Fink SD, Eng K, Spen-cer FC: Prognostic signs and the role of operative managementin acute pancreatitis. Surg Gynecol Obstet 139:69–81, 1974
7. Ranson JHC: Etiological and prognostic factors in humanacute pancreatitis: A review. Am J Gastroenterol 77:633–638,1982
8. Blamey SL, Imrie CW, O’Neill J, Gilmour WH, Carter DC:Prognostic factors in acute pancreatitis. Gut 25:1340–1346,1984
9. Knaus WA, Draper EA, Wagner DP, Zimmerman JE:APACHE II: a severity of disease classification system. CritCare Med 13:818–829, 1985
10. Steingart RM, Packer M, Hamm P, Coglianese MA, Gersh B,Geltman EM, Sollano J, Katz S, Moye L, Basta LL, Lewis SJ,Gottlieb SS, Bernstein V, McEwan P, Jacobson K, Brown EJ,Krikin MI, Kantrowitz NE, Pfeffer MA, for the Survival andVentricular Enlargement Investigator: Sex differences in themanagement of coronary artery disease. N Engl J Med325:226–230, 1991
11. Ayanian JZ, Epstein AM: Differences in the use of proceduresbetween women and men hospitalized for coronary heart dis-ease. N Engl J Med 325:221–225, 1991
12. Marrugat J, Sala J, Masia R, Pavesi M, Sanz G, Valle V,Molina L, Seres L, Elosua R, for the RESCATE Investigators:Mortality differences between men and women following firstmyocardial infarction. J Am Med Assoc 280:1405–1409, 1998
13. Tragnone A, Corrao G, Miglio F, Caprilli R, Lanfranchi GA,Gruppo Italiano per lo Studio del Colon e del Retto (GISC):Incidence of inflammatory bowel disease in Italy: A nationwidepopulation-based study. Int J Epidemiol 25:1044–1052, 1996
14. Lukash WM: Complications of acute pancreatitis. Unusualsequelae in 100 cases. Arch Surg 94:848–852, 1967
15. Edlund Y, Norback B, Risholm L: Acute pancreatitis, etiologyand prevention of recurrence. Follow-up study of 188 patients.Rev Surg 25:153–157, 1968
16. Imrie CW: Observations on acute pancreatitis. Br J Surg61:539–544, 1974
17. Trapnell JE, Duncan EHL: Patterns of incidence in acutepancreatitis. Br Med J 2:179–183, 1975
18. Jacobs ML, Daggett WM, Civetta JM, Vasu MA, Lawson DW,Warshaw AL, Nardi GL, Bartlett MK: Acute pancreatitis:
Analysis of factors influencing survival. Ann Surg 185:43–51,1977
19. Ranson JHC, Spencer FC: The role of peritoneal lavage insevere acute pancreatitis. Ann Surg 187:565–575, 1978
20. Madsen OG, Schmidt A: Acute pancreatitis. A study of 122patients with acute pancreatitis observed for 5–15 years. WorldJ Surg 3:345–352, 1979
21. Ong GB, Lam KH, Lam SK, Lim TK, Wong J: Acute pancre-atitis in Hong Kong. Br J Surg 66:398–403, 1979
22. Satiani B, Stone HH: Predictability of present outcome andfuture recurrence in acute pancreatitis. Arch Surg 114:711–716,1979
23. Svensson J-O, Norback B, Bokey EL, Edlund Y: Changingpattern in aetiology of pancreatitis in an urban Swedish area.Br J Surg 66:159–161, 1979
24. Corfield AP, Cooper MJ, Williamson RCN: Acute pancreatitis:A lethal disease of increasing incidence. Gut 26:724–729, 1985
25. Renner IG, Savage III WT, Pantoja JL, Renner VJ: Death dueto acute pancreatitis. A retrospective analysis of 405 autopsycases. Dig Dis Sci 30:1005–1018, 1985
26. Thomson HJ: Acute pancreatitis in north and north-east Scot-land. J R Coll Surg Edinb 30:104–110, 1985
27. Thomson SR, Hendry WS, McFarlane GA, Davidson AI: Ep-idemiology and outcome of acute pancreatitis. Br J Surg74:398–401, 1987
28. Fan ST, Choi TK, Lai CS, Wong J: Influence of age on themortality from acute pancreatitis. Br J Surg 75:463–466, 1988
29. Fan S-T, Lai ECS, Mok FPT, Lo C-M, Zheng S-S, Wong J:Prediction of the severity of acute pancreatitis. Am J Surg166:262–269, 1993
30. De Beaux AC, Palmer KR, Carter DC: Factors influencingmorbidity and mortality in acute pancreatitis; an analysis of 279cases. Gut 37:121–126, 1995
31. Lankisch PG, Burchard-Reckert S, Petersen M, Lehnick D,Schirren CA, Kohler H, Stockmann F, Peiper HJ, CreutzfeldtW: Morbidity and mortality in 602 patients with acute pancre-atitis seen between the years 1980–1994. Z Gastroenterol34:371–377, 1996
32. Uhl W, Isenmann R, Curti G, Vogel R, Beger HG, BuchlerMW: Influence of etiology on the course and outcome of acutepancreatitis. Pancreas 13:335–343, 1996
33. Pezzilli R, Billi P, Morselli-Labate AM: Severity of acutepancreatitis: Relationship with etiology, sex and age. Hepato-gastroenterology 45:1859–1864, 1998
34. Gillespie WJ: Observations on acute pancreatitis. A post-mortem review. J R Coll Surg Edinb 20:36–41, 1975
35. Taylor TV, Rimmer S, Holt S, Jeacock J, Lucas S: Sex differ-ences in gallstone pancreatitis. Ann Surg 214:667–670, 1991
36. Armstrong CP, Taylor TV, Jeacock J, Lucas S: The biliary tractin patients with acute gallstone pancreatitis. Br J Surg 72:551–555, 1985
37. Lowenfels AB, Lankisch PG, Maisonneuve P: What is the riskof biliary pancreatitis in patients with gallstones? Gastroenter-ology 119:879–880, 2000
38. Browder W, Patterson MD, Thompson JL, Walters DN: Acutepancreatitis of unknown etiology in the elderly. Ann Surg217:469–475, 1993
LANKISCH ET AL
2474 Digestive Diseases and Sciences, Vol. 46, No. 11 (November 2001)







