Embed Size (px)
Citation preview

Scand J Haematol(l979) 23, 339-347
Acute Non Lymphoid Leukaemia Following Hodgkin’s Disease
Clinical, Biological and Cytogenetic Aspects of 3 Cases
GIUSEPPE PAPA, GIULIANA ALIMENA, LUCIANA ANNINQ,
ANNA MARIA DE LUCA, LUC~A GRANATI, NICOLA PETTI & FWCO MANDELLI ANNA PAOLA ANSELMO, FABRIZIQ CICCONE,
Institute of Haematology, University of Rome, Rome, Italy
In a group of 254 patients treated for Hodgkin’s disease with a follow up period of minimum 2 years, 3 cases of acute non lymphoid leukaemia (ANLL) were observed: erythroleukaemia, myelomonocytic and myeloblastic leukaemia, respectively. The crude idcidence of leukaemia in all patients was 0.0128 and patient year risk was estimated to be 0.003652. All 3 patients had received radiation therapy and chemo- therapy. In all cases a haemopoietic dysplasia preceded ANLL. Bone marrow chromosome investigations showed an abnormal karyotype in all patients: chromosomal changes were present in 100 5% of cells and revealed a non- random distribution, the most frequent involvement being clustered t o chromosomes nos 11, 17 and 21. Hypodiploidy was prevalent and multiple structural rearrange- ments, such as markers, rings and minutes, were present in a high percentage of cells. Other changes involved chromosomes nos 5, 7 and 14. Our results are compared with other previously reported cases and possible patho- genetic implications are discussed.
Key words: acute leukaemia - cytogenetics - Hodgkin’s disease - preleukaemia
Accepted for publication August 24, 1979
Correspondence to: Giuseppe Papa, M.D., Institute of Haematology, University of Rome, Via Lancisi 3, 00161 Ro’ma, Italy
In recent years, the increasing incidence of cases of Hodgkin’s disease (HD) termi- nating in acute non lymphoid leukaemia (ANLL) has stimulated different inter- pretations (Arseneau et a1 1972, 1977, Bonadonna et a1 1973, Mauri & Quaglino 1974, Canellos et a1 1975, Rosner & Grun- wald 1975, Toland & Coltman 1975, Brody et a1 1977, Cadman et a1 1977). Most au- thors consider modern therapeutic strategies
used in the treatment of HD as the main pathogenetic factor. In fact it cannot be denied that the increased incidence of ANLL following HD occurred contem- porarily with the more intensive use of radiotherapy and chemotherapy, especially if combined.
In this paper we report the clinical and biological characteristics of 3 patients with HD developing ANLL.
0036-553W79/09033!4-09 $02.50/0 @ 1979 Munksgaard, Copenhagen
340 PAPA, ALIMENA, ANNINO, ANSELMO, CICCONE, DE LUCA et a1
MATERIAL AND METHODS
372 patients affected by HD were treated and fol- lowed up in our Institute between 1969 and 1978. We calculated cumulative patient years at risk of developing ANLL (Brody et a1 1977, Larsen & Brincker 1977) in 234 patients with a minimum follow up period of 2 years.
The patients were grouped according t o the type of treatment. Radiotherapy was always on extended fields, e.g. mantle field, inverted Y , total nodal irradiation (TNI) (Kaplan 1966); chemotherapy was based on multiple drugs, mainly MOPP (De Vita et a1 1970), PROVECIP (Mandelli et a1 1974), ABVD (Bonadoana et a1 1975).
Chromosome analyses were prepared by a di- rect technique from bone marrow aspiration and from short term cultures of peripheral blood with PHA. The chromosomes were stained by means of the GAG banding technique (Alimena et a1 1977).
Marrow culture were performed on case 1, using the technique of Pike & Robinson (1970).
Erythrokinetic studies (performed on case 1) and platelet survival studies (performed on case' 2), were performed according to Najean et a1 (1969).
The preleukaemic syndrome was defined using the criteria suggested by Linman & Bagby (1978): Abnormalities of the cells in the peripheral b l d and bone marrow, with absence d vitamin Biz and folate deficiency and no cytotoxic therapy in the previous 6 months.
The cytological type of acute leukaemia was defined according to the FAB cooperative group classification (Bennet et a1 1976).
CASE REPORTS Case I A 30-year-old woman, diagnosed in Dec 1970, as having HD, NS histological type, CS 111 B. First she received radiotherapy on involved fields (cervival and axillary nodes); 3300 rads in 2 months. From Apr 1971 tor Oct 1972, she re- ceived chemotherapy with vinblastine (VLB), chlorambucil (Cloram) and prednisone (PDN). The patient remained symptom-free until May 1973, when she relapsed in the left cervical area. At this stage she was referred to us. TNI was performed from May t o Dec 1973. An extended
spleen irradiation was given in Febr 1974. A complete remission (CR) was obtained and
the patient remained syrnptom-free until March 1977, when a serious anaemia without evidence of haemolysis or haemorrhage was detected. The bone marraw aspiration showed erythro- blastic hyperplasia with maturation defect and megaloblastic changes. Morphological and matu- ration anomalies were also present in the granu- lablasts and in the megakaryocytes. Erythro- kinetic studies showed a combination of quanti- tative and qualitative kinetic marrow abnormal- ities (Najean et a1 1975, Faille et a1 1977) sug- gesting a diagnosis of refractory anaemia (RA).
In Oct 1977 the patient's condition deteriorated, with increasing anaemia, high fewer, haernor- rhagic syndrome, gum hypertrophy. Hb 79 gA, WBC 3.9 X 1WA with 22 % blast cells and cir- culating erythroblasts; platelet count was 45 X 109/1. The bone marrow smears showed a picture of erythroleukaemia (M6).
The patient was given a mild antilcukaemic therapy with 6-mercaptopurine and hydroxiurea; no response was obtained and she died 5 months later in March 1978. Autopsy was nat performed.
Bone marrow cultures were performed during the preleukaemic phase (June 1977) and during the diagnosed leukaemic phase (Nov 1977). Ln the first series of cultures there was a reduced num- ber of clusters on the 4th d and an absence of colonies on the 12th d. In the leukaemic phase there was a complete absence of clusters and colonies both on the 4th and on the 12th d.
Chromosome analyses were performed dur- ing the overt leukaemic phase in Nov 1977. The 76 metaphases observed were abnor- mal with the presence of several clones. The majority of cells had chromosome counts from 40 to 50 and 10 out of 76 metaphases were tetraploid to near octo- ploid (150 chromosomes), with multiple fragmentations. Clones with 43-44 chro- mosomes were prevalent. In all analysed metaphases a Robertsonian translocation, t(13;14), was found. This abnormality was also present in the short term cultured lym- phocytes from peripheral blood and thus must be considered congenital.
ACUTE LEUKAEMIA IN HODGKIN’S DISEASE 341
S
G
S
G
5 11 13 la4 14 15 I 6 R
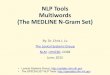
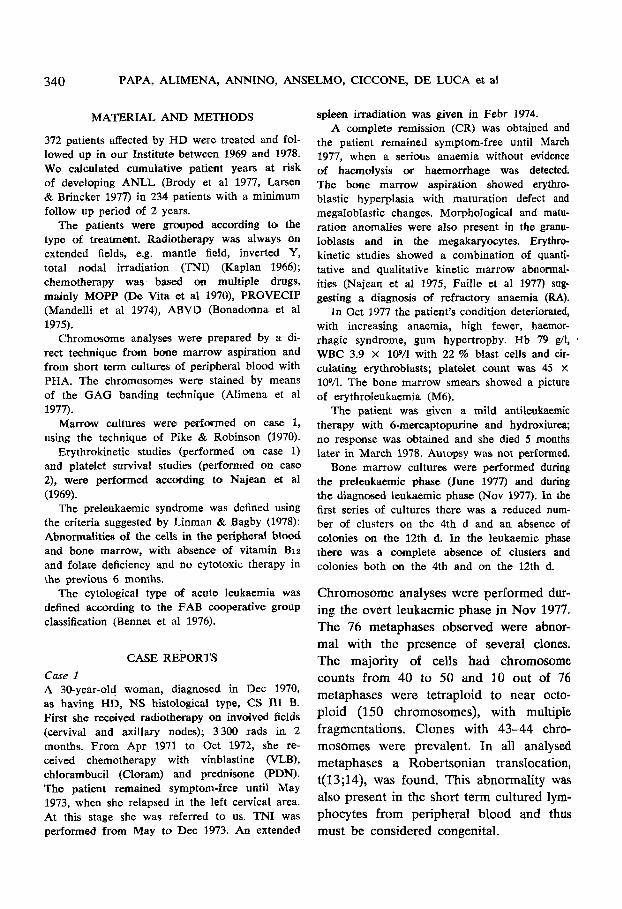
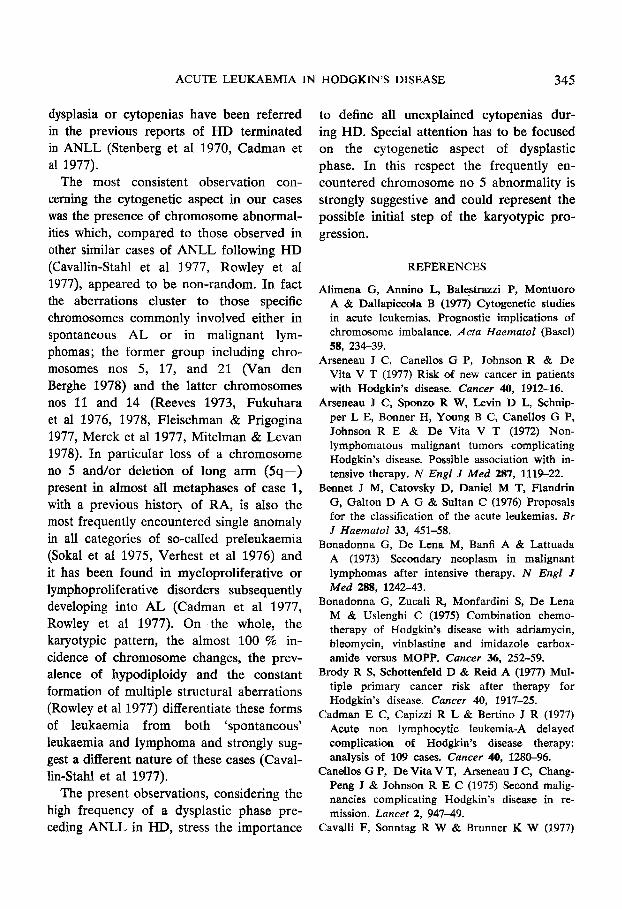
Figure 1. Partial karyatypes of case 1 showing the deleted chromosomes nos 5 and 11, the translocation t(13;14) and ring chromosomes.
The constant karyotypic changes (90 % of the cells) were: loss of a chromosome no 5 and the presence of a small meta- centric chromosome, derived probably by a deletion, de1(5)(q13;q31-33); deletion of the long arm of a chromosome no 11 del (ll)(q21); loss of chromosomes nos 17 and 21 (Figure 1). Furthermore, there were losses andor gains of chromosomes in all other groups, however not in a constant manner, even in cells with an identical number of chromosomes. 60 % of cells showed structural abnormalities including markers, ring chromosomes and minute fragments.
Case 2 A 43-year-old man diagnosed in Febr 1971, as having HD, LP histological type, CS I1 B. He first received radiotherapy on involved fields (right cervical and supraclavicular areas) 4 400
rads. From March 1971 to June 1973 he was treated with cyclophosphamide (CY) and pro- carbazine (PCB), and from Febr t o Sept 1973 with TNI. After CR, 6 cycles of MOPP were administered. In May 1974 a thrombocytopenia (20 X 109/1) did not improve on corticosteroid and androgen treatment. Platelet kinetics showed a defective production with normal platelet life span.
In May 1975 the patient was referred to our Institute with fever and haemorrhages. The bone marrow and peripheral blood examination showed a picture of acute myelo-monocytic leukaemia W4).
The patient died in July 1975 of septic shock, despite treatment with daunorubicin, cytarabine and thioguanine.
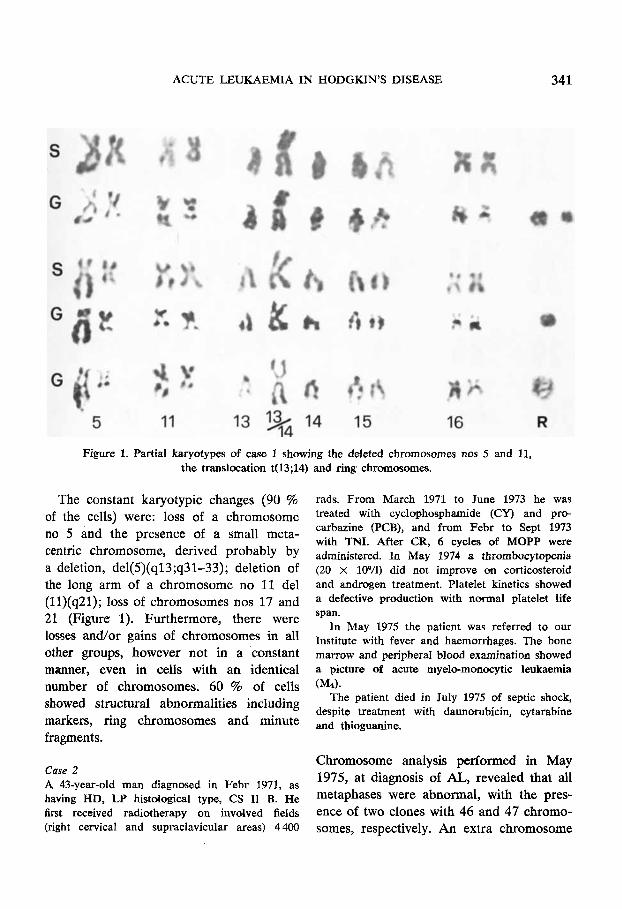
Chromosome analysis performed in May 1975, at diagnosis of AL, revealed that all metaphases were abnormal, with the pres- ence of two clones with 46 and 47 chromo- somes, respectively. An extra chromosome
342 PAPA, ALIMENA, ANNINO, ANSELMO, CICCONE, DE LUCA et a1
1
6
13
1
6
..
13
2
7
14
19
3
8
15
2 0
4 5
9 10 11 12 X
16 17 ' 18
d
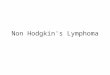
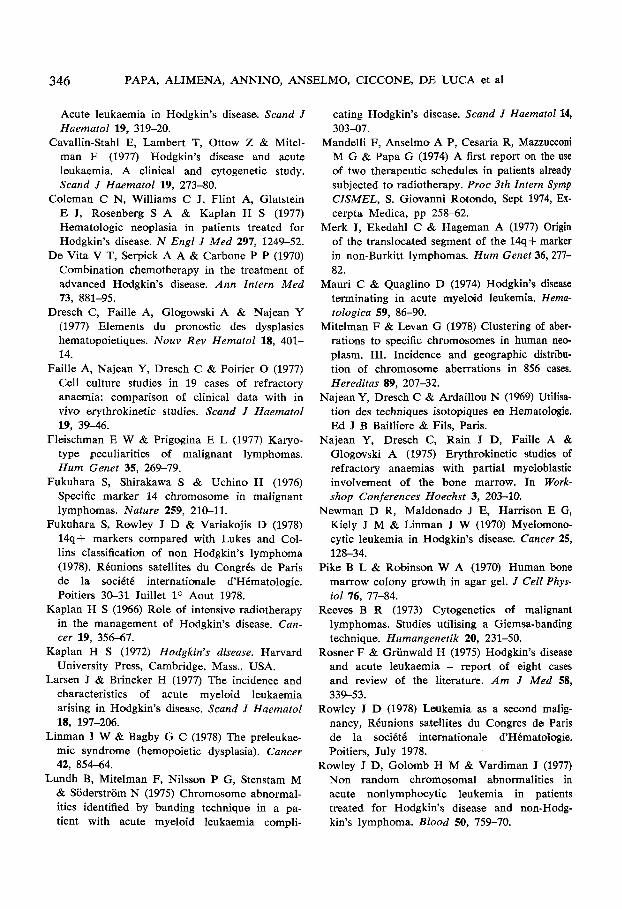
21 2 2 Y Figure 2. Bane marrow karyoltype of case 2: 46,XY,-17,+21.
2 3 4 5
a 9 10 1 1 12 X 1
7
16 17 18
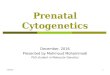
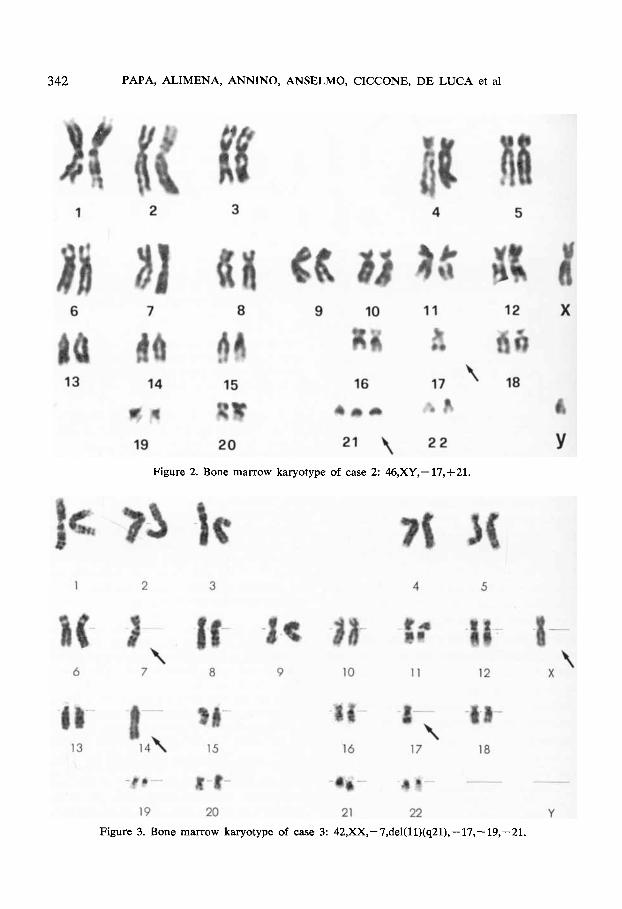
19 20 21 22 Y Figure 3. Bone marrow karyotype of case 3: 42,XX,-7,del(ll)(q21),-17,- 19,-21.
ACUTE LEUKAEMIA IN HODGKIN'S DISEASE 343
1
6
13
2
1 7
14
19 \
3
8
15
20
4 5
\ 9 10 11
18 \
16 17
1 R 21 2 2
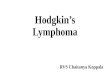
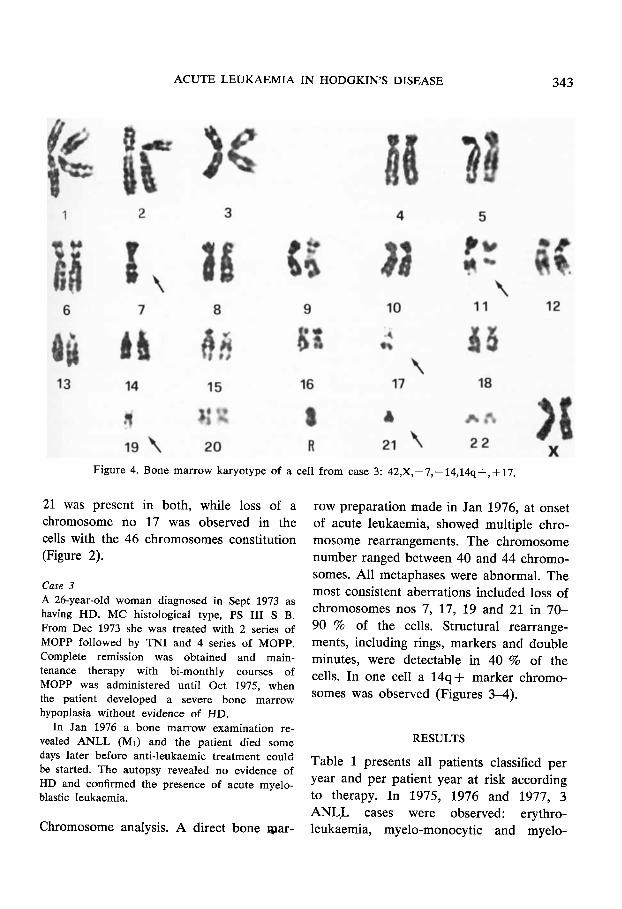
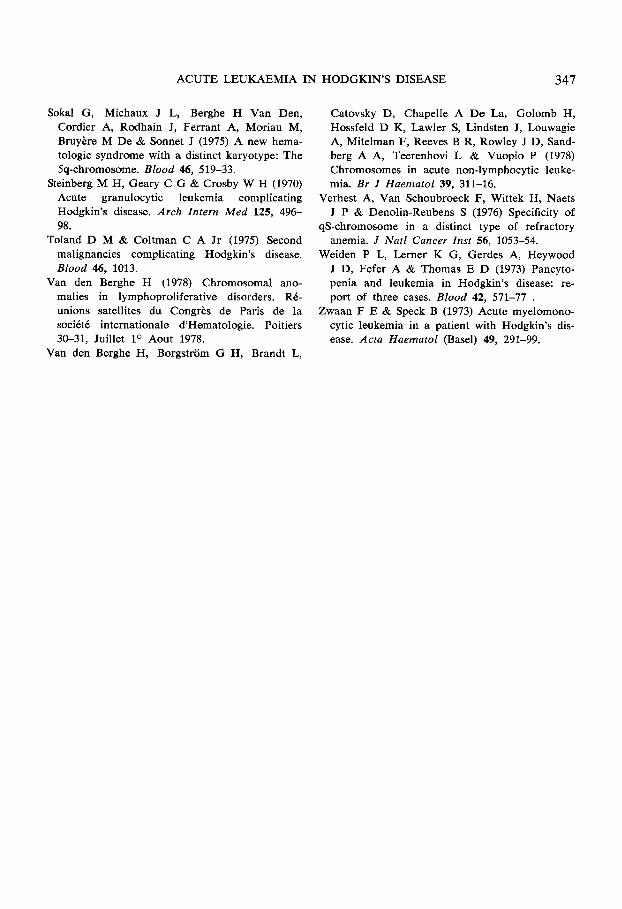
Figure 4. Bosne marrow karyo'type of a cell fro'm case 3: 42,X, -7, - 14,14q +, + 17.
21 was present in both, while loss of a chromosome no 17 was observed in the cells with the 46 chromosomes constitution (Figure 2).
Case 3 A 26-year-old woman diagnosed in Sept 1973 as having HD, MC histological type, PS 111 S B. From Dec 1973 she was treated with 2 series of MOPP followed by TNI and 4 series o€ MOPP. Complete remission was obtained and main- tenance therapy with bimonthly courses of MOPP was administered until Oct 1975, when the patient developed a severe bone marrow hypoplasia without evidence of HD.
In Jan 1976 a bone marrow examination re- vealed ANLL (MI) and the patient died some days later before anti-leukaemic treatment could be started. The autopsy revealed no evidence of HD and confirmed the presence of acute myelo- blastic leukaemia.
Chromosome analysis. A direct bone war-
12
X
row preparation made in Jan 1976, at onset of acute leukaemia, showed multiple chro- mosome rearrangements. The chromosome number ranged between 40 and 44 chromo- somes. All metaphases were abnormal. The most consistent aberrations included loss of chromosomes nos 7, 17, 19 and 21 in 70- 90 % of the cells. Structural rearrange- ments, including rings, markers and double minutes, were detectable in 40 % of the cells. In one cell a 14q+ marker chromo- somes was observed (Figures 3-4).
RESULTS
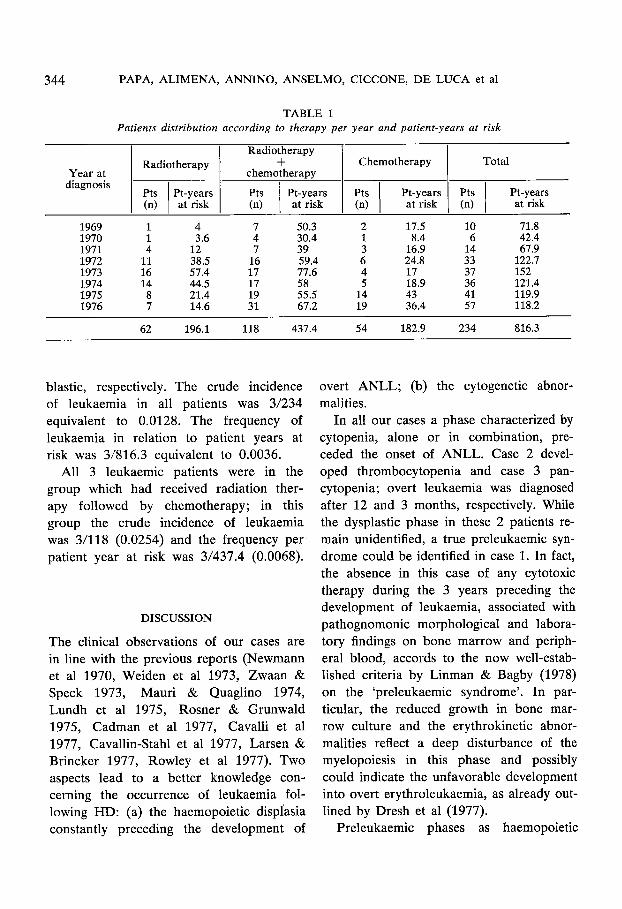
Table 1 presents all patients classified per year and per patient year at risk according to therapy. In 1975, 1976 and 1977, 3 ANLL cases were observed: erythro- leukaemia, myelo-monocytic and myelo-
344 PAPA, ALIMENA, ANNINO, ANSELMO, CICCONE, D E LUCA et a1
Year at diagnosis
Radiotherapy
chemotherapy Radiotherapy + Chemotherapy Total
Pts Pt-years (n) at risk
Pt-years Pts 1 Pt-years Pts I Pt-years at risk (n) at risk
1969 1970 1971 1972 1973 1974 1975 1976
1 4 7 50.3 2 17.5 10 71.8 1 3.6 4 30.4 1 8.4 6 42.4 4 12 7 39 3 16.9 14 67.9
11 38.5 16 59.4 6 24.8 33 122.7 16 57.4 17 77.6 4 17 37 152 14 44.5 17 58 5 18.9 36 121.4 8 21.4 19 55.5 14 43 41 119.9 7 14.6 31 67.2 19 36.4 57 118.2
62 196.1 118 437.4 54 182.9 234 816.3
blastic, respectively. The crude incidence of leukaemia in all patients was 3/234 equivalent to 0.0128. The frequency of leukaemia in relation to patient years at risk was 3/816.3 equivalent to 0.0036.
All 3 leukaemic patients were in the group which had received radiation ther- apy followed by chemotherapy; in this group the crude incidence of leukaemia was 3/118 (0.0254) and the frequency per patient year at risk was 3/437.4 (0.0068).
DISCUSSION
The clinical observations of our cases are in line with the previous reports (Newmann et a1 1970, Weiden et a1 1973, Zwaan & Speck 1973, Mauri & Quaglino 1974, Lundh et a1 1975, Rosner & Grunwald 1975, Cadman et a1 1977, Cavalli et a1 1977, Cavallin-Stahl et a1 1977, Larsen & Brincker 1977, Rowley et a1 1977). TWO aspects lead to a better knowledge con- cerning the occurrence of leukaemia fol- lowing HD: (a) the haemopoietic displasia constantly preceding the development of
overt ANLL; (b) the cytogenetic abnor- malities.
In all our cases a phase characterized by cytopenia, alone or in combination, pre- ceded the onset of ANLL. Case 2 devel- oped thrombocytopenia and case 3 pan- cytopenia; overt leukaemia was diagnosed after 12 and 3 months, respectively. While the dysplastic phase in these 2 patients re- main unidentified, a true preleukaemic syn- drome could be identified in case 1. In fact, the absence in this case of any cytotoxic therapy during the 3 years preceding the development of leukaemia, associated with pathognomonic morphological and labora- tory findings on bone marrow and periph- eral blood, accords to the now well-estab- lished criteria by Linman & Bagby (1978) on the ‘preleukaemic syndrome’. In par- ticular, the reduced growth in bone mar- row culture and the erythrokinetic abnor- malities reflect a deep disturbance of the myelopoiesis in this phase and possibly could indicate the unfavorable development into overt erythroleukaemia, as already out- lined by Dresh et a1 (1977).
Preleukaemic phases as haemopoietic
ACUTE LEUKAEMIA IN HODGKIN’S DISEASE 345
dysplasia or cytopenias have been referred in the previous reports of HD terminated in ANLL (Stenberg et a1 1970, Cadman et a1 1977).
The most consistent observation con- cerning the cytogenetic aspect in our cases was the presence of chromosome abnormal- ities which, compared to those observed in other similar cases of ANLL following HD (Cavallin-Stahl et a1 1977, Rowley et a1 1977), appeared to be non-random. In fact the aberrations cluster to those specific chromosomes commonly involved either in spontaneous AL or in malignant lym- phomas; the former group including chro- mosomes nos 5, 17, and 21 (Van den Berghe 1978) and the latter chromosomes nos 11 and 14 (Reeves 1973, Fukuhara et a1 1976, 1978, Fleischman & Prigogina 1977, Merck et a1 1977, Mitelman & Levan 1978). In particular loss of a chromosome no 5 and/or deletion of long arm (5q-) present in almost all metaphases of case 1, with a previous histon of RA, is also the most frequently encountered single anomaly in all categories of so-called preleukaemia (Sokal et a1 1975, Verhest et a1 1976) and it has been found in myeloproliferative or lymphoproliferative disorders subsequently developing into AL (Cadman et a1 1977, Rowley et a1 1977). On the whole, the karyotypic pattern, the almost 100 % in- cidence of chromosome changes, the prev- alence of hypodiploidy and the constant formation of multiple structural aberrations (Rowley et a1 1977) differentiate these forms of leukaemia from both ‘spontaneous’ leukaemia and lymphoma and strongly sug- gest a dif€erent nature of these cases (Caval- 1inStahl et a1 1977).
The present observations, considering the high frequency of a dysplastic phase pre- ceding ANLL in HD, stress the importance
to define all unexplained cytopenias dur- ing HD. Special attention has to be focused on the cytogenetic aspect of dysplastic phase. In this respect the frequently en- countered chromosome no 5 abnormality is strongly suggestive and could represent the possible initial step of the karyotypic pro- gression.
REFERENCES
Alimena G, Annino L, Balestrazzi P, Mmtuoro A & Dallapiccola B (1977) Cytogenetic studies in acute leukemias. Prognostic implications of chromosome imbalance. Acta Huematol (Basel)
Arseneau J C, Canellos G P, Johnson R & De Vita V T (1977) Risk oQ new cancer in patients with Hodgkin’s disease. Cancer 40, 1912-16.
Arseneau J C, Spnzo R W, Levin D L, Schnip- per L E, Bonner H, Young B C, Canellos G P, Johnson R E & De Vita V T (1972) Non- lymphomatous malignant tumors complicating Hodgkin’s disease. Possible association with in- tensive therapy. N Engi J Med 287, 111!+-22.
Bennet J M, Catovsky D, Daniel M T, Flandrin G, Galton D A G & Sultan C (1976) Proposals for the classification of the acute leukemias. Br J Haematol 33, 451-58.
Bonadonna G, De Lena M, Banfi A & Lattuada A (1973) Secondary neoplasm in malignant lymphomas after intensive therapy. N Engl J Med 288, 1242-43.
Bonadonna G, Zucali R, Mmfardini S, De Lena M & Uslenghi C (1975) Combination chemo. therapy of Hodgkin’s disease with adriamycin, bleomycin, vinblastine and imidazole carbox- amide versus MOPP. Cancer 36, 252-59.
Brody R S, Schottenfeld D & Reid A (1977) Mul- tiple primary cancer risk after therapy for Hodgkin’s disease. Cancer 40, 1917-25.
Cadman E C, Capizzi R L & Bertino J R (1977) Acute non lymphocytic leukemia-A delayed complication oE Hodgkin’s disease therapy: analysis of 109 cases. Cancer 40, 1280-96.
Canellos G P, De Vita V T, Arseneau J C, Chang- Peng J & Johnson R E C (1975) Second malig- nancies complicating Hodgkin’s disease in re- mission. Lancet 2, 947-49.
Cavalli F , Sonntag R W & Brunner K W (1977)
58, 234-39.
346 PAPA, ALIMENA, ANNINO, ANSELMO, CICCONE, D E LUCA et a1
Acute leukaemia in Hodgkin’s disease. Scand J Haematol 19, 319-20.
Cavallin-Stahl E, Lambert T, Ottow Z & Mitel- man F (1977) Hodgkin’s disease and acute leukaemia. A clinical and cytogenetic study. Scand J Haematol 19, 273-80.
Coleman C N, Williams C J, Flint A, Glatstein E J, Rosenberg S A & Kaplan H S (1977) Hematologic neoplasia in patients treated for Hodgkin’s disease. N Engl J Med 297, 1249-52.
De Vita V T, Serpick A A & Carboae P P (1970) Combination chemotherapy in the treatment of advanced Hodgkin’s disease. Ann Intern Med
Dresch C, Faille A, Glogowski A & Najean Y (1977) Elements du pronostic des dysplasies hematopoietiques. Nouv Rev Hematol 18, 401- 14.
Faille A, Najean Y , Dresch C & Poirier 0 (1977) Cell culture studies in 19 cases of refractory anaemia: comparison of clinical data with in vivo erythrokinetic studies. Scand J Haernatol
Fleischman E W & Prigogina E L (1977) Karyo- type peculiarities of malignant lymphomas. Hum Genet 35, 269-19.
Fukuhara S, Shirakawa S & Uchino H (1976) Specific marker 14 chromosome in malignant lymphomas. Nature 259, 210-11.
Fukuhara S, Rowley J D & Variakojis D (1978) 14q+ markers compared with Lukes and Col- lins classification of noa Hodgkin’s lymphoma (1978). RBunions satellites du Congr6s de Paris de la soci6t6 internationale d’H6matologie. Poitiers 30-31 Juillet lo Aout 1978.
Kaplan H S (1966) Role of intensive radiotherapy in the management of Hodgkin’s disease. Can- cer 19, 356-67.
Kaplan H S (1972) Hodgkin’s disease. Harvasd University Press, Cambridge, Mass., USA.
Larsen J & Brincker H (1977) The incidence and characteristics of acute myeloid leukaemia arising in Hodgkin’s disease. Scand J Haematol
Linman 5 W & Bagby G C (1978) The preleukae- mic syndrome (hemopoietic dysplasia). Cancer 42, 854-64.
Lundh B, Mitelman F, Nilsson P G, Stenstam M & Soderstrom N (1975) Chromosome abnormal- ities identified by banding technique in a pa- tient with acute myeluid leukaemia compli-
73, 881-95.
19, 39-46.
18, 197-206.
cating Hodgkin’s disease. Scand J Haematol 14, 303-07.
Mandelli F, Anselmol A P, Cesaxia R, Mauucconi M G & Papa G (1974) A first report on the use of two therapeutic schedules in patients already subjected to radiotherapy. Proc 3th Intern Symp CISMEL, S . Giovanni Rotondo, Sept 1974, Ex- cerpta Medica, pp 25842 .
Merk J, Ekedahl C & Hageman A (1977) Origin of the translocated segment of the 14q+ marker in non-Burkitt lymphomas. Hum Genet 36, 211- 82.
Mauri C & Quaglino D (1974) Hodgkin’s disease terminating in acute myeloid leukemia. Hema- tologica 59, 86-W.
Mitelman F & Levan G (1978) Clustering of aber- rations to specific chromosomes in human nee plasm. 111. Incidence and geographic distnbu- tion of chromosome aberrations in 856 cases. Hereditas 89, 207-32.
Najean Y, Dresch C & Ardaillou N (1969) Utilisa- tion des techniques isotopiques en Hematdogie. Ed J B Bailliere & Fils, Paris.
Najean Y, Dresch C, Rain J D, Faille A & Glogovski A (1975) Erythrokinetic studies of refractory anaemias with partial myeloblastic involvement of the bone marrow. In Work- shop Conferences Hoechst 3, 203-10.
Newman D R, Maldonado J E, Harrison E G, Kiely J M & Linman J W (1970) Myelomoncr- cytic leukemia in Hodgkin’s disease. Cancer 25,
Pike B L & Robinson W A (1970) Human bone marrow colony growth in agar gel. J CeIl Phys- iol 76, 77-84.
Reeves B R (1973) Cytogenetics of malignant lymphomas. Studies utilising a Giemsa-banding technique. Humangenetik 20, 231-50.
Rosner F & Griinwald H (1975) Hodgkin’s disease and acute leukaemia - report of eight cases and review of the literature. Am J Med 58, 339-53.
Rowley J D (1978) Leukemia as a second malig- nancy, RBunions satellites du Congres de Paris de la sociCt6 internationale d‘H6matologie. Poitiers, July 1978.
Rowley J D, Golomb H M & Vardiman J (1977) Non random chromosomal abnormalities in acute noalymphocytic leukemia in patients treated for Hodgkin’s disease and non-Hodg- kin’s lymphoma. Blood 50, 759-70.
128-34.
ACUTE LEUKAEMIA IN HODGKIN’S DISEASE 347
Sokal G, Michaux J L, Berghe H Van Den, Cordier A, Rodhain J, Ferrant A, Moriau M, Bruybre M De & Sonnet J (1975) A new hema- tologic syndrome with a distinct karyotype: The 5q-chromosome. Blood 46, 519-33.
Steinberg M H, Geary C G & Crosby W H (1970) Acute granulocytic leukemia complicating Hodgkin’s disease. Arch Intern Med 125, 496- 98.
Toland D M & Coltman C A Jr (1975) Second malignancies complicating Hodgkin’s disease. Blood 46, 1013.
Van den Berghe H (1978) Chromosomal ano- malies in lymphoproliferative disorders. RB- unions satellites du Congrbs de Paris de la sociCtC internationale d’Hematologie. Poitiers 30-31, Juillet lo Aout 1978.
Van den Berghe H, Borgstrom G H, Brandt L,
Catovsky D, Chapelk A De La, Golomb H, Hossfeld D K, Lawler S, Lindsten J, Louwagie A, Mitelman F, Reeves B R, Rowley J D, Sand- berg A A, Teerenhovi L & Vuopio P (1978) Chromosomes in acute non-lymphocytic leuke- mia. Br J Haematol 39, 311-16.
Verhest A, Van Schmbroeck F, Wittek H, Naets J P & Denolin-Reubens S (1976) Specificity of
qS-chromosome in a distinct type of refractory anemia. J Natl Cancer Inst 56, 1053-54.
Weiden P L, Lerner K G, Gerdes A, Heywood J D, Fefer A & Thomas E D (1973) Pancyto- penia and leukemia in Hodgkin’s disease: re- port of three cases. Blood 42, 571-77 .
Zwaan F E & Speck B (1973) Acute myelomono- cytic leukemia in a patient with Hodgkin’s dis- ease. Acta Haematol (Basel) 49, 291-99.