Embed Size (px)
Citation preview
at SciVerse ScienceDirect
Manual Therapy 17 (2012) 318e324
Contents lists available
Manual Therapy
journal homepage: www.elsevier .com/math
Original article
Acute low back pain information online: An evaluation of quality, contentaccuracy and readability of related websites
Paul A. Hendrick*, Osman H. Ahmed, Shane S. Bankier, Tze Jieh Chan, Sarah A. Crawford,Catherine R. Ryder, Lisa J. Welsh, Anthony G. SchneidersCentre for Physiotherapy Research, School of Physiotherapy, University of Otago, PO Box 56, Dunedin 9054, New Zealand
a r t i c l e i n f o
Article history:Received 22 June 2011Received in revised form20 February 2012Accepted 24 February 2012
Keywords:Acute low back painInternetHealth Information
* Corresponding author. Tel.: þ64 3 479 5428; fax:E-mail address: [email protected] (P.A. H
1356-689X/$ e see front matter � 2012 Elsevier Ltd.doi:10.1016/j.math.2012.02.019
a b s t r a c t
The internet is increasingly being used as a source of health information by the general public. Numerouswebsites exist that provide advice and information on the diagnosis and management of acute low backpain (ALBP), however, the accuracy and utility of this information has yet to be established. The aim ofthis study was to establish the quality, content and readability of online information relating to thetreatment and management of ALBP. The internet was systematically searched using Google searchengines from six major English-speaking countries. In addition, relevant national and international lowback pain-related professional organisations were also searched. A total of 22 relevant websites wasidentified. The accuracy of the content of the ALBP information was established using a 13 point guidedeveloped from international guidelines. Website quality was evaluated using the HONcode, and theFlesch-Kincaid Grade level (FKGL) was used to establish readability. The majority of websites lackedaccurate information, resulting in an overall mean content accuracy score of 6.3/17. Only 3 websites hada high content accuracy score (>14/17) along with an acceptable readability score (FKGL 6e8) with themajority of websites providing information which exceeded the recommended level for the averageperson to comprehend. The most accurately reported category was, “Education and reassurance” (98%)while information regarding “manipulation” (50%), “massage” (9%) and “exercise” (0%) were amongst thelowest scoring categories. These results demonstrate the need for more accurate and readable internet-based ALBP information specifically centred on evidence-based guidelines.
� 2012 Elsevier Ltd. All rights reserved.
1. Introduction
The internet has become a major source of health-relatedinformation and its use is expected to increase exponentially(Sambandam et al., 2007). A recent survey found that 60% ofinternet users accessed the internet to find health-related infor-mation (Atkinson et al., 2009), with factors such as convenienceand accessibility cited as key reasons (McMullan, 2006). However,a lack of quality assurance relating to web-based health informa-tion potentially means that some details may be incomplete, oreven incorrect, leading to misinformation that could delay recoveryor even precipitate harm (Dutta-Bergman, 2003).
Acute low back pain (ALBP) is one of the most commonmusculoskeletal disorders, in part due to its cyclic nature ofremission and relapse (Kent and Keating, 2005; Krismer and vanTulder, 2007; Majid and Truumees, 2008). For most patients with
þ64 3 479 8414.endrick).
All rights reserved.
non-specific ALBP the source of symptoms is unknown. The self-limiting but frequent nature of the condition means the majorityof patients do not seek specific medical attention for each episode(Majid and Truumees, 2008), but rather self-manage the conditionfrom information sourced from the community that includespersonal treatment recommendations and anecdotes (Bush et al.,1993). Thus, the internet offers a potentially important source ofhealth education for this condition.
The popularity of health information on the internet is reflectedby the increasing number of studies evaluating the quality ofhealth-related information (Starman et al., 2010; Ahmed et al.,2011). To date however, only two studies have previously evalu-ated the quality of online information relating to low back pain(LBP) (Li et al., 2001; Butler and Foster, 2003). These studies foundthat the quality of LBP information available on the internet wasgenerally poor. Since the publication of this work nearly a decadeago, a large number of international guidelines for non-specificALBP has been published (Dagenais et al., 2010) which has conse-quently resulted in a substantial increase in the available evidencefor effective management of LBP. Taking into consideration the

Table 1ALBPguide.
Checklistnumber
Description of ALBPguide management intervention Yes/nocriteriona
1 Encouragement to stay active within the limits of pain. Yes2 Medications limited to NSAIDS, muscle relaxants,
acetaminophen and opioids.Yes
3 Brief education and reassurance about back pain andits self-limiting nature.
Yes
4 Manipulation. Yes5 Bed rest to be advised only within the time limit of 2
e3 days.Yes
6 Specific back exercise. No7 Massage. No8 Physical modalities (ice, heat, traction, ultrasound and
TENS).No
9 Acupuncture. No10 Lumbar supports. No11 Injections. No12 Behavioural therapy. No13 Surgery. No
a Based upon 75% agreement of management intervention across internationalguidelines for ALBP management.
Table 2Scoring criteria for ALBPguide.
Yes (recommended clinicalintervention by guidelines)
No (clinical intervention notsupported by guidelines)
Score Descriptor Score Descriptor
2 Present and complete 1 Present and complete1 Present but incomplete 0 Not Present0 Not present �1 Present but incorrect�1 Present but incorrect
P.A. Hendrick et al. / Manual Therapy 17 (2012) 318e324 319
growth in the internet during the past decade and increasing accessto evidence-based guidelines, there is a timely need for a review ofinternet sites that provide information online for the managementof ALBP.
It is agreed that health information needs to be current, accu-rate, evidence-based, and unambiguous in order to provide the enduser with the most valid and reliable information (Lawrentschuket al., 2009). Accuracy in health information is especially impor-tant for globally prevalent conditions such as ALBP, where specificinformation available to the public is important to promote effec-tive self-management strategies. The purpose of this study was tocompile a non-exhaustive list of current websites on Google�
which contain information on the management of non-specific LBPand to evaluate the quality and content accuracy of suchwebsites inrelation to current evidence-based practice guidelines. As part ofsuch a process, the study also aimed to evaluate the managementinformation on selected LBP sites related to national and interna-tional bodies. A secondary aim was to examine the readability ofthe information and quality of the websites. The results will allowevaluation of currentwebsitemanagement information available tothe public for the management of non-specific ALBP in relation tocurrent best-practice guidelines.
2. Methodology
A cross sectional study design was chosen to evaluate thecontent and quality of online information on the internet related tothe management of ALBP. The analysis was carried out in twostages: Firstly a comprehensive checklist was developed to evaluatecontent accuracy of online ALBP information and termed the,“ALBPguide”. Secondly an extensive internet search was conductedand a selection of LBP websites from recognised professional,national and international spinal/LBP organisations were exam-ined. Website information was subsequently evaluated and scoredfor content accuracy and readability.
2.1. Content assessment (ALBPguide)
No content analysis for web-based information for themanagement of non-specific ALBP currently exists and thereforethe authors developed a 13 item checklist (ALBPguide) in order toassess the content of each website. Since these websites would besourced from a number of countries it was decided to develop theALBPguide from a synthesis of current national guidelines for non-specific ALBP, rather than specifically look at how each websitematches guidelines for the country of origin (since websites areoften sourced beyond the country of origin). A recent review of allnational guidelines for non-specific ALBP was therefore chosen asthe review document to develop the ALBPguide (Dagenais et al.,2010). A comprehensive review of the current internationalguidelines (Dagenais et al., 2010) contained in the review for non-specific ALBP management was carried out by two experiencedManipulative Physiotherapists in the research team (PH and AS). Itwas arbitrarily decided that management intervention componentsof the ALBPguide required at least half (50%) of the countriesinvolved in recent LBP guideline publication to report on thespecific management interventions. Inclusion of these manage-ment interventions in the ALBPguide required three-quarters (75%)of the international guidelines to be in agreement as to theevidence-based use of the intervention (Table 1).
Two authors (PH and AS) independently evaluated each of themanagement interventions and through subsequent consensusreached full agreement on all interventions included in the ALBP-guide. In addition, red flags detailed in the international guidelines(Dagenais et al., 2010) were evaluated by the same two authors. For
the purpose of this research it was decided to evaluate the presenceof at least 4 flags (from the evidence-based list of red flags (seeappendix 1)) (Dagenais et al., 2010). While the inclusion of red flagsis described in the results they are not scored in the ALBPguide asthey were considered part of patient assessment rather thanmanagement.
Short descriptors were created for each management itemreflecting the keymessage from the guidelines (see Table 1). Each ofthe management items for ALBP was grouped into one of twocategories (Dagenais et al., 2010). A “yes” category was determinedby an evidence-based recommendation that a management inter-vention item (e.g. manipulation) should be included in clinicalpractice. Those items which were not supported by evidence-basedrecommendations were categorised as “no” (i.e. not supported inclinical practice). The scoring system for the ALBPguide is detailed inTable 2 and had a maximum score of þ17 with scores potentiallyranging from �13 to þ17. Any information on a website relating toan item on the ALBPguide which was considered to be misinfor-mation was given a score of �1, indicating the information waspresent but incorrect. This scoring systemwas modelled on the oneused in a previous study on LBP internet information (Butler andFoster, 2003).
2.2. Search strategy
All evaluated websites were required to be in English and befreely available to the public (i.e. not require a login,membership, orrestricted registration to enter the site). It was mandatory that thecontent of the website included information relating to themanagement of ALBP. Websites were excluded if they focused onchronic LBP or general back pain information, or if the content wasnot specifically related to an acute onset of LBP. Journal articles,

Fig. 1. Search strategy flowchart.
P.A. Hendrick et al. / Manual Therapy 17 (2012) 318e324320
blogs, forums, videos, and audio links were excluded. Hyperlinks(links to other webpages) and PDFs (Portable Document Folders)that led to informationwithin the same website were followed andincluded in the analyses; however hyperlinks which led to anexternal website were excluded.
2.3. Google search
The search strategy was designed to locate websites that wouldbe easily accessible to the general public. For the purposes of thisstudy Google was used as the primary search engine as it is inter-nationally acknowledged as the most popular search engineaccounting for up to 67% of all internet searches (Bernstam et al.,2005). A systematic search of the internet was conducted usingthe following search terms “acute low back pain AND treatment ORmanagement” using the relevant Google search engine from the sixmajor English-speaking countries: Australia (www.google.com.au),Canada (www.google.ca), New Zealand (www.google.co.nz), SouthAfrica (www.google.co.za), United Kingdom (www.google.co.uk)and the United States of America (www.google.com). This proce-dure was undertaken using an advanced Google search, reportingresults in English only. The search was carried out on the 3rdFebruary 2011 using the search engines mentioned above. Fromthese searches, the first 10 relevant websites that met the inclusioncriteria were recorded, and any repeat/duplicate websites weremanually removed.
In addition, websites of major national/international organisa-tions and professional bodies involved in spinal/LBP research andmanagement were also searched. The process involved compilationof a non-exhaustive list of relevant websites and was cross-checkedby the principle researchers who are actively involved in LBPresearch (PH, AS, OA). Additional LBP sites related to national andinternational bodies which arose during the Google search stagewere also included in the study.
2.4. HONcode (information quality tool)
The HONcode is the most commonly used benchmark for healthwebsite quality (Peterlin et al., 2008; Morr et al., 2010) and iscurrently used by over 7300 websites, covering 10 million pages in102 countries. In order for a website to be approved by the HONFoundation, it must follow the HONcode principles (listed inappendix 2). If these criteria are met, the website is awardeda HONcode logowhich is displayed on thewebsite. For the purposesof this study, the item was scored as “Yes” or” No”.
2.5. Readability assessment
The FLESCH-Kincaid Grade level (FKGL) is a widely acceptedscale to evaluate readability (Paasche-Orlow et al., 2003). The FKGLcalculates a reading level using the mean sentence and wordlength. Reading grades, produced from the United States educa-tional school grades, range from 3 (lowest) to 12 (final year of highschool) (Williamson and Martin, 2010). Previous studies suggesthealth information for the general public should be ideally pre-sented at a grade level of between 6 and 8 (Van der Marel et al.,2009). Microsoft Word 2007� was used to determine the FKGLfor each website using the inbuilt readability statistics function.
2.6. Procedure
Prior to undertaking the content assessment, three members ofthe research group familiarised themselves with the ALBPguidescoring systemand a full internet searchwas then completedwithina 24 h period (3/02/11). Once all duplicates had been removed and
websites assessed, two researchers (SB and SC) independentlyscored each of the items from the ALBPguide for websiteswhichmetthe inclusion criteria. The scoring for each of the items was thencompared and if a disagreement arose, a third researcher (TJC)scored the item independently and a consensus score was reached.
2.7. Analyses
Descriptive statistics (mean and standard deviation) werecalculated for the ALBPguide, FKGL and FRES. Independent t-testswere carried out to investigate differences in ALBPguide scores forwebsites that were HON approved and those that were not. Pearsoncorrelation coefficients were conducted between ALBPguide andreading grade level (FKGL). Kappa values were calculated to eval-uate inter-rater reliability for the each of the management inter-ventions in the ALBPguide and an overall Kappa was calculated forthe ALBPguide. Microsoft Excel 2010� was used to calculatedescriptive statistics and Med Calc� was used to determine Kappascores for inter-rater reliability.
3. Results
After removing duplicates a total of 19 relevant websites waslocated from the Google search, and a further 59 websites fromprofessional organisations was screened. Only three websites fromthe professional organisations contained information relating tothemanagement of ALBP (Fig. 1), leaving a total of 22 websites to beevaluated using the ALBPguide (see Table 3).
The average ALBPguide score for all websites was 6.73 points(SD¼ 4.33), from a maximum score of 17. The highest recordedALBPguide score was 16 out of 17 (http://besthealth.bmj.com/x/index.html) and the lowest score was 0 out of 17 (http://www.spineuniverse.com/conditions/back-pain/low-back-pain/medication-and-treatment-acute-low-back-pain). The average scores for theFKGL were 9.37 (SD¼ 2.92) (Table 3). There was negativecorrelation between FKGL and ALBPguide: r¼�0.39, p< 0.05 (seeFig. 1). Of the 22 websites evaluated, 68% (15/22) contained satis-factory information about red flags (>4 flags) and 41% (9/22) wereHON-approved websites (Table 3).
3.1. Management interventions
Management interventions recommended from the guidelines(“Yes” category) scored relatively highly on each of the websites.“Education and reassurance” achieved the highest overall score onthe ALBPguide with 43/44 points (98%), while “manipulation”scored the lowest with 23/44 (52%) on the ALBPguide score.
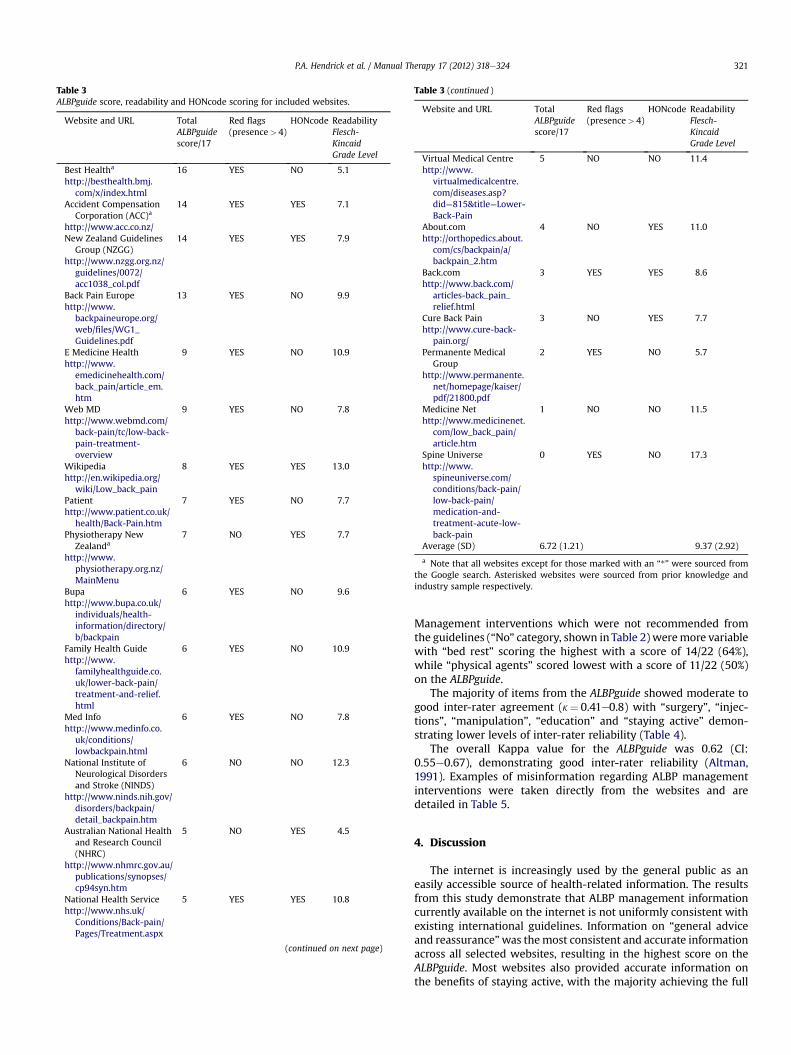
Table 3ALBPguide score, readability and HONcode scoring for included websites.
Website and URL TotalALBPguidescore/17
Red flags(presence> 4)
HONcode ReadabilityFlesch-KincaidGrade Level
Best Healtha 16 YES NO 5.1http://besthealth.bmj.
com/x/index.htmlAccident Compensation
Corporation (ACC)a14 YES YES 7.1
http://www.acc.co.nz/New Zealand Guidelines
Group (NZGG)14 YES YES 7.9
http://www.nzgg.org.nz/guidelines/0072/acc1038_col.pdf
Back Pain Europe 13 YES NO 9.9http://www.
backpaineurope.org/web/files/WG1_Guidelines.pdf
E Medicine Health 9 YES NO 10.9http://www.
emedicinehealth.com/back_pain/article_em.htm
Web MD 9 YES NO 7.8http://www.webmd.com/
back-pain/tc/low-back-pain-treatment-overview
Wikipedia 8 YES YES 13.0http://en.wikipedia.org/
wiki/Low_back_painPatient 7 YES NO 7.7http://www.patient.co.uk/
health/Back-Pain.htmPhysiotherapy New
Zealanda7 NO YES 7.7
http://www.physiotherapy.org.nz/MainMenu
Bupa 6 YES NO 9.6http://www.bupa.co.uk/
individuals/health-information/directory/b/backpain
Family Health Guide 6 YES NO 10.9http://www.
familyhealthguide.co.uk/lower-back-pain/treatment-and-relief.html
Med Info 6 YES NO 7.8http://www.medinfo.co.
uk/conditions/lowbackpain.html
National Institute ofNeurological Disordersand Stroke (NINDS)
6 NO NO 12.3
http://www.ninds.nih.gov/disorders/backpain/detail_backpain.htm
Australian National Healthand Research Council(NHRC)
5 NO YES 4.5
http://www.nhmrc.gov.au/publications/synopses/cp94syn.htm
National Health Service 5 YES YES 10.8http://www.nhs.uk/
Conditions/Back-pain/Pages/Treatment.aspx
(continued on next page)
Table 3 (continued )
Website and URL TotalALBPguidescore/17
Red flags(presence> 4)
HONcode ReadabilityFlesch-KincaidGrade Level
Virtual Medical Centre 5 NO NO 11.4http://www.
virtualmedicalcentre.com/diseases.asp?did¼815&title¼Lower-Back-Pain
About.com 4 NO YES 11.0http://orthopedics.about.
com/cs/backpain/a/backpain_2.htm
Back.com 3 YES YES 8.6http://www.back.com/
articles-back_pain_relief.html
Cure Back Pain 3 NO YES 7.7http://www.cure-back-
pain.org/Permanente Medical
Group2 YES NO 5.7
http://www.permanente.net/homepage/kaiser/pdf/21800.pdf
Medicine Net 1 NO NO 11.5http://www.medicinenet.
com/low_back_pain/article.htm
Spine Universe 0 YES NO 17.3http://www.
spineuniverse.com/conditions/back-pain/low-back-pain/medication-and-treatment-acute-low-back-pain
Average (SD) 6.72 (1.21) 9.37 (2.92)
a Note that all websites except for those marked with an “*” were sourced fromthe Google search. Asterisked websites were sourced from prior knowledge andindustry sample respectively.
P.A. Hendrick et al. / Manual Therapy 17 (2012) 318e324 321
Management interventions which were not recommended fromthe guidelines (“No” category, shown in Table 2) weremore variablewith “bed rest” scoring the highest with a score of 14/22 (64%),while “physical agents” scored lowest with a score of 11/22 (50%)on the ALBPguide.
The majority of items from the ALBPguide showed moderate togood inter-rater agreement (k¼ 0.41e0.8) with “surgery”, “injec-tions”, “manipulation”, “education” and “staying active” demon-strating lower levels of inter-rater reliability (Table 4).
The overall Kappa value for the ALBPguide was 0.62 (CI:0.55e0.67), demonstrating good inter-rater reliability (Altman,1991). Examples of misinformation regarding ALBP managementinterventions were taken directly from the websites and aredetailed in Table 5.
4. Discussion
The internet is increasingly used by the general public as aneasily accessible source of health-related information. The resultsfrom this study demonstrate that ALBP management informationcurrently available on the internet is not uniformly consistent withexisting international guidelines. Information on “general adviceand reassurance”was themost consistent and accurate informationacross all selected websites, resulting in the highest score on theALBPguide. Most websites also provided accurate information onthe benefits of staying active, with the majority achieving the full

Table 4Inter-rater reliability of the ALBPguide.
ALBPguide item # and topic Kappa score (k) (95%CI) Strength of agreement
1. Stay active 0.22 (�0.15 to 0.60) Fair2. Bed rest 0.69 (0.38e1.00) Good3. Education 0.10 (�0.16 to 0.37) Poor4. Back exercises 0.59 (0.31e0.86) Moderate5. Medication 0.46 (0.16e0.77) Moderate6. Massage 0.66 (0.34e0.98) Good7. Manipulation 0.29 (0.02e0.57) Fair8. Physical agents 0.48 (0.19e0.78) Moderate9. Acupuncture 0.62 (0.31e0.94) Good10. Lumbar support 0.66 (0.33e1.00) Good11. Injection 0.24 (�0.26 to 0.76) Fair12. Behavioural Therapy 0.62 (0.16e1.00) Good13. Surgery 0.09 (�0.19 to 0.37) PoorOverall 0.62 (0.55 to 0.69) Good
P.A. Hendrick et al. / Manual Therapy 17 (2012) 318e324322
score for this item. Of particular concern was that most websitesscored less than half of the total maximum score (17) on theALBPguide which may in part be explained by the indefinitewording of management recommendations encountered on manywebsites. Internet information scored poorly when managementinterventions shown to be non-efficacious in the guidelines were
Table 5Examples of website misinformation relating to management interventions.
Name of website Recommendationsfrom ALBPguide
Quote of incorrectinformation
National Institute ofNeurologicalDisorders andStroke (NINDS)
No physical modalities(heat, cold andelectrotherapy) areindicated.
“As soon as possible followingtrauma, patients should applya cold pack or a cold compress(such as a bag of ice or bag offrozen vegetables wrapped ina towel) to the tender spotseveral times a day for up to20 min.”
Australian NationalHealth and ResearchCouncil (NHRC)
Measures that are effectivefor relieving acute low backpain are: staying active(relieves pain better thanresting in bed), havingwritten information (it ishelpful to discuss writteninformation with your healthpractitioner) and heat wraptherapy.”
Back.com (Acute BackPain)
Lumbar supportsare not indicated.
“Use a cervical roll (a foam rollapproximately 3 inches indiameter and 18 inches long)to support the natural curvesin your neck or low back.”
Cure Back Pain Acupuncture is notindicated.
“For short term relief fromacute back pain, acupunctureis highly recommended”
Medicine.net Massage is not indicated. “The treatment of lumbarstrain consists of resting theback (to avoid re-injury),medications to relieve painand muscle spasm, local heatapplications, massage, andeventual (after the acuteepisode resolves)reconditioning exercises tostrengthen the low back andabdominal muscles.”
No physical modalities(heat, cold andelectrotherapy) areindicated.
Spine Universe Massage is not indicated. “Considering that many casesof back pain are caused bymuscle strain and overuse, itswonderful news that massageis a worthwhile treatmentoption.”
described using words such as ‘may work’ or ‘works for somepatients’.
Information retaining to physical modalities had the lowestoverall ALBPguide category score with many websites suggestingthat both heat and ice were an effective treatment for ALBP. Thisrecommendationmay be due to the historical and continuing use ofice and heat by the general public, and the fact that these physicalmodalities are readily available and commonly used by some healthprofessionals in combinationwith other forms of treatment (Frenchet al., 2006). Information regarding manipulation as a managementintervention for ALBP was not consistent across the websites.Manipulation was specifically mentioned in 15 of the 22 websites;seven of which contained “present and complete” information.Encouragingly no websites were found to contain misinformationregarding manipulation.
Website advice on medication use scored relatively highly,however many of the websites did not include complete informa-tion for all listed medications and several websites suggested “overthe counter drugs” for ALBP management (which may be due todiffering drug prescription policies across countries) (Kennedy,1996). Encouragingly, 69% of websites included information onfour or more red flags from the international guidelines (Dagenaiset al., 2010). While red flags are not a management interventionand their prevalence in ALBP sufferers is low (0.9%) (Henschke et al.,2009), their inclusion in the current study was intended toacknowledge important safety issues related to the differentialdiagnosis of non-specific ALBP (especially for the assessment ofmore severe pathologies).
It is acknowledged that assessment of internet-based healthinformation is important (Hanif et al., 2009). The strength of theALBPguide developed for this study is that it represents a synthesisof guideline evidence to analyse and appropriately grade thequality of internet-based information. This ALBPguide classifiedinterventions categorically based upon their recommendation (Yes/No) as a management intervention, whereas previous scoringsystems employed to assess LBP quality on the internet focusedonly on the quality of information related solely to interventionsrecommended at that time for themanagement of ALBP (Butler andFoster, 2003). The ALBPguide had good overall inter-reliability(k¼ 0.62), however some variation was found across manage-ment interventions (k range 0.09e0.69). Further studies are neededto validate the ALBPguide against other measures of informationquality assessment in LBP.
The quality of the website information showed that 41% ofwebsites were HON approved; a figurewhich is slightly higher thanthose assessed in a recent study of health-related websites(Starman et al., 2010). Our study found no difference (p¼ 0.35) inthe ALBPguide scores between websites that were HON approvedand those that were not HON approved. This reinforces the fact thatthe HONcode does not necessarily reflect the accuracy or quality ofthe information on the website (Peterlin et al., 2008), but serves asa mechanism to help readers understand the purpose and source ofthe information. It is also acknowledged that website information isonly useful to a patient if it is readable (Oermann andWilson, 2000;Berland et al., 2001). The readability scores in our study indicatethat a large proportion of ALBP website information may be toocomplex for mainstream users to understand (Bernstam et al.,2005), and this assertion is further supported by recent evidencethat 25% of the American population that have an education belowhigh school level use the internet to access health information (Foxand Jones, 2009).
Inconsistencies in online information regarding managementinterventions for ALBP may be as a result of differences in guidelinespecification (Murphy et al., 2006). Primarily, this is due to thediffering methods of assessing and weighting research evidence for

The HONcode principles.a
Principles Description
1 e Authority Give qualifications of authors2 e Complementarity Respect the privacy of site users3 e Confidentiality Respect the privacy of site users4 e Attribution Cite the sources and dates of medical information5 e Justifiability Justification of claims/balanced and objective claims6 e Transparency Accessibility, provide valid contact details7 e Financial disclosure Provide details of funding8 e Advertising Clearly distinguish advertising from editorial content
a
Red flags.
Age < 20 Pain at multiple sitesAge > 50 Saddle numbnessFecal incontinence Steroid useFever Structural deformityGait abnormality Systemic unwellnessHistory of cancer TraumaImmune suppression Unexplained weight lossIntravenous drug use Urinary retentionNight pain Weakness in limbsNo response to care Widespread neurological symptomsOsteoporosis
P.A. Hendrick et al. / Manual Therapy 17 (2012) 318e324 323
guidelines between countries. Adoptions of guidelines remaininconsistent across countries (Armstrong et al., 2003; Strand et al.,2005; Fullen et al., 2007) and these results are further reflected inthe website findings, whereby current practice is not necessarilyguideline based.With global access to the internet, thedevelopmentof consensus-based international guidelines for the managementALBP would help standardise best practice, however the optimalutilisation of guidelines by clinicians needs further investigation.
The number of websites from national and International spinalorganisations carrying information relating to the management ofALBP was surprisingly low. One reason for this may be that suchwebsites are designed primarily for practicing clinicians andresearchers, and they are linked directly to the guidelines for thecountry which the organisation represents. It could be arguedhowever that current, updated evidence-based guidelines for theassessment and management of ALBP would be a useful resourcefor clinicians and researchers, and potentially a valuable and trus-ted resource for patients.
4.1. Recommendations for future research
The internet is continually evolving, as are clinical practiceguidelines for ALBP (Sandvik, 1999). Future studies should focus onhow patients retrieve information relating to management infor-mation for ALBP on the internet, the potential search terms thatpatients might employ for this and, the varying and often diversesources of such information (i.e. videos, sites such as YouTube/Facebook/Twitter, blogs). Also, evaluation of the quality of acutelow back pain management information from all sources should beextensively reviewed for both quality and readability.
Although the use of internet-based education in LBP has notbeen studied in detail, empowering patients with current guidelinebased advice via a simple “back book” has been shown to be clin-ically efficacious in various LBP groups (Burton et al., 1999;Udermann et al., 2004; Coudeyre et al., 2007). A recent study alsodemonstrated that guideline based care was responsible for bothimprovements in physical functioning and for a lower utilisation ofcare (Rutten et al., 2010). The continued growth of the World WideWeb in modern society necessitates further research on thepotential role for internet-based information on clinical outcomes.
4.2. Limitations
This study represented a non-exhaustive search of websitesreadily available to the general public. Although Google was theonly search engine used, recent statistics show that Google is theleading search engine worldwide and used for over 67% of allsearches on the internet (Hitwise, 2011). A potential limitation isthat only the first 10 relevant “hits” were taken from each Googlesearch, a decision based on evidence indicating that the majority ofpeople only look at the first page of hits when searching witha search engine (Atkinson et al., 2009). The authors also recognisethat the grouping and scoring of the management interventionsemployed in this study was a pragmatic choice based upona consensus amalgamation of current national guidelines, andtherefore further validation is required in future study’s to assessthe use of this process to determine content quality of websiteinformation pertaining to LBP management. Retrieval of relevantwebsites may also have been limited from a global perspective bylimiting Google searches to English-speaking countries only.
5. Conclusion
The internet represents a crucial but under-researched source ofinformation for patientswith back pain. Internet-based information
available to thepublicwhich relates to evidence-basedmanagementof non-specific low back pain is currently limited, and readability ofsuch content is often too difficult for some people to interpret andunderstand. Development of future low back pain websites shouldbe in accordancewith evidence-basedguidelines, better targeted forthe general public and, written at an appropriate level to ensure theavailability of reliable and understandable information.
Appendix 1
Appendix 2
Table adapted from the HON website (www.hon.ch).
References
Ahmed OH, Sullivan SJ, Schneiders AG, McCrory PR. Concussion information online:evaluation of information quality, content and readability of concussion-relatedwebsites. British Journal of Sports Medicine; 2011. doi:10.1136/bjsm.2010.081620.
AltmanDG. Practical statistics formedical research. London: ChapmanandHall; 1991.Armstrong MP, McDonough S, Baxter GD. Clinical guidelines versus clinical practice
in the management of low back pain. International Journal of Clinical Practice2003;57:9e13.
Atkinson LN, Saperstein LS, Pleis J. Using the internet for health-related activities:findings from a national probability sample. Journal of Medical InternetResearch 2009;11(1):e4.
Berland GK, Elliott MN, Morales LS, Algazy JI, Kravitz RL, Broder MS, et al. Healthinformation on the internet. JAMA: The Journal of the American MedicalAssociation 2001;285(20):2612e21.
Bernstam EV, Shelton DM, Walji M, Meric-Bernstam F. Instruments to assess thequality of health information on the world wide web: what can our patientsactually use? International Journal of Medical Informatics 2005;74(1):13e9.
Burton AK, Waddell G, Tillotson KM, Summerton N. Information and advice topatients with back pain can have a positive effect: a randomized controlled trialof a novel educational booklet in primary care. Spine 1999;24:2484e91.
Bush T, Cherkin D, BarlowW. The impact of physician attitudes onpatient satisfactionwith care for low back pain. Archives of Family Medicine 1993;2(3):301e5.
Butler L, Foster NE. Back pain online: a cross-sectional survey of the quality of web-based information on low back pain. Spine 2003;28(4):395e401.
Coudeyre E, Tubach F, Rannou F, Baron G, Coriat F, Brin S, et al. Effect of a simpleinformation booklet on pain persistence after an acute episode of low back pain:a non-randomized trial in a primary care setting. PLoS One 2007;2(8):e706.
Dagenais S, Tricco AC, Haldeman S. Synthesis of recommendations for the assess-ment and management of low back pain from recent clinical practice guide-lines. The Spine Journal 2010;10(6):514e29.
Dutta-Bergman M. Trusted online sources of health information: differences indemographics, health beliefs, and health-information orientation. Journal ofMedical Internet Research 2003;5(3):e21.
P.A. Hendrick et al. / Manual Therapy 17 (2012) 318e324324
Fox S, Jones S. The social life of health information. Washington, DC: Pew Internet &American Life Project, Pewinternet.org; 2009. pp. 1e88.
French SD, Cameron M, Walker BF, Reggars JW, Esterman AJ. A Cochrane review ofsuperficial heat or cold for low back pain. Spine 2006;31(9):998e1006. 10.97/01.brs.0000214881.10814.64.
Fullen BM, Maher T, Bury G, Tynan A, Daly LE, Hurley DA. Adherence of Irish generalpractitioners to European guidelines for acute low back pain: a prospective pilotstudy. European Journal of Pain 2007;11:614e23.
Hanif F, Read JC, Goodacre JA, Chaudhry A, Gibbs P. The role of quality tools inassessing reliability of the Internet for health information. Informatics forHealth and Social Care 2009;34(4):231e43.
Henschke N, Maher CG, Refshauge KM, et al. Prevalence of and screening for seriousspinal pathology in patients presenting to primary care settings with acute lowback pain. Arthritis & Rheumatism 2009;60(10):3072e80.
Lawrentschuk N, Abouassaly R, Hackett N, Groll R, Fleshner NE. Health informationquality on the internet in urological oncology: a multilingual longitudinalevaluation. Urology 2009;74(5):1058e63.
Li L, Irvin E, Guzman J, Bombardier C. Surfing for back pain patients: the nature andquality of back pain information on the internet. Spine 2001;26(5):545e57.
Majid K, Truumees E. Epidemiology and natural history of low back pain. Seminarsin Spine Surgery 2008;20(2):87e92.
McMullan M. Patients using the Internet to obtain health information: how thisaffects the patient-health professional relationship. Patient Education andCounseling 2006;63(1e2):24e8.
Morr S, Shanti N, Carrer A, Kubeck J, Gerling MC. Quality of information concerningcervical disc herniation on the internet. The Spine Journal 2010;10(4):350e4.
Murphy AY, van Teijlingen ER, Gobbi MO. Inconsistent grading of evidence acrosscountries: a review of low back pain guidelines. Journal of Manipulative andPhysiological Therapeutics 2006;29:576e81.
Kent P, Keating J. The epidemiology of low back pain in primary care. Chiropractic &Osteopathy 2005;13(1):13.
Kennedy JG. Over the counter drugs. British Medical Journal 1996;312(7031):593e4.
Krismer M, van Tulder M. Low back pain (non-specific). Best Practice & ResearchClinical Rheumatology 2007;21(1):77e91.
Oermann MH, Wilson FL. Quality of care information for consumers on the internet.Journal of Nursing Care Quality 2000;14(4):45e54.
Paasche-Orlow MK, Taylor HA, Brancati FL. Readability standards for informed-consent forms as compared with actual readability. New England Journal ofMedicine 2003;348(8):721e6.
Peterlin BL, Gambini-Suarez E, Lidicker J, Levin M. An analysis of cluster headacheinformation provided on internet websites. Headache 2008;48(3):378e84.
Rutten GM, Degen S, Hendriks EJ, Braspenning JC, Harting J, Oostendorp RA.Adherence to clinical practice guidelines for low back pain in physical therapy:do patients benefit? Physical Therapy 2010;90(8):1111e22.
Sambandam SN, Ramasamy V, Priyanka P, Ilango B. Quality analysis of patientinformation about knee arthroscopy on the world wide web. Journal ofArthroscopic and Related Surgery 2007;23(5):509e13.
Sandvik H. Health information and interaction on the internet: a survey of femaleurinary incontinence. British Medical Journal 1999;319(7201):29e32.
Starman JS, Gettys FK, Capo JA, Fleischli JE, Norton HJ, Karunakar MA. Quality andcontent of internet-based information for ten common orthopaedic sportsmedicine diagnoses. Journal of Bone and Joint Surgery 2010;92A(7):1612e8.
Strand LI, Kvale A, Råheim M, Ljunggren AE. Do Norwegian manual therapistsprovide management for patients with acute low back pain in accordance withclinical guidelines? Manual Therapy 2005;10:38e43.
Udermann BE, Spratt KF, Donelson RG, Mayer J, Graves JE, Tillotson J. Can a patienteducational book change behavior and reduce pain in chronic low back painpatients? The Spine Journal 2004;4(4):425e35.
Van der Marel S, Duijvestein M, Hardwick JC, et al. Quality of web-based infor-mation on inflammatory bowel diseases. Inflammatory Bowel Diseases 2009;15(12):1891e6.
Williamson JML, Martin AG. Analysis of patient information leaflets provided bya district general hospital by the Flesch and Flesch-Kincaid method. Interna-tional Journal of Clinical Practice 2010;64(13):1824e31.
Web References (Ordered by position in Table 3)
BMJ Best Health. Back pain e what treatments work for short-term back pain?,http://besthealth.bmj.com/x/topic/392834/essentials.html; 2011 [last accessed03.02.11].
Accident Compensation Corporation (ACC). Acute low back pain part 2 clinicalmanagement e Issue 8, http://www.acc.co.nz/for-providers/clinical-best-practice/acc-review/WCMZ003155#P3_79; 2004a [last accessed 03.02.11].
Accident Compensation Corporation (ACC). New Zealand acute low back pain guide,http://www.nzgg.org.nz/guidelines/0072/acc1038_col.pdf; 2004b [last accessed03.02.11].
Tulder M, et al. European guidelines for the management of acute nonspecific lowback pain in primary care, http://www.backpaineurope.org/web/files/WG1_Guidelines.pdf [last accessed 03.02.11].
Shiel Jr W. Low back pain, http://www.emedicinehealth.com/back_pain/article_em.htm; 2011 [last accessed 03.02.11].
Erstad S. Low back pain e treatment overview, http://www.webmd.com/back-pain/tc/low-back-pain-treatment-overview; 2010 [last accessed 03.02.11].
Low back pain. http://en.wikipedia.org/wiki/Low_back_pain [last accessed 03.02.11].Non-specific lower back pain in adults, http://www.patient.co.uk/health/Back-Pain.
htm [last accessed 03.02.11].Low back pain e what physiotherapists can do, http://www.physiotherapy.org.nz/
Folder?Action¼Download&Folder_id¼90&File¼Pamphlet%2520-%2520Low%2520Back%2520Pain.pdf [last accessed 03.02.11].
Bupa Health Information Team 2010. Back Pain. http://www.bupa.co.uk/individuals/health-information/directory/b/backpain[last accessed 03.02.11]
Lower back pain. http://www.familyhealthguide.co.uk/lower-back-pain/treatment-and-relief.html [last accessed 03.02.11].
Medinfo: Low back pain. http://www.medinfo.co.uk/conditions/lowbackpain.html[last accessed 03.02.11].
National Institute of Neurological Disorders and Stroke. Low back pain fact sheet,http://www.ninds.nih.gov/disorders/backpain/detail_backpain.htm; 2011 [lastaccessed 03.02.11].
Information sheet 1-acute low back pain. http://www.nhmrc.gov.au/publications/synopses/cp94syn.htm [last accessed 03.02.11].
Back pain e treatment. http://www.nhs.uk/Conditions/Back-pain/Pages/Treatment.aspx [last accessed 03.02.11].
Lower Back Pain. http://www.virtualmedicalcentre.com/diseases.asp?did¼815&title¼Lower-Back-Pain [last accessed 03.02.11].
Cluett J. Backpain treatment, http://orthopedics.about.com/cs/backpain/a/backpain_2.htm; 2010 [last accessed 03.02.11].
Acute back pain. http://www.back.com/articles-back_pain_relief.html [last accessed03.02.11].
Rostocki A. Back pain, http://www.cure-back-pain.org/; 2011 [last accessed 03.02.11].The PermanenteMedical Group. Self-management for acute lowback pain, http://www.
permanente.net/homepage/kaiser/pdf/21800.pdf; 2003 [last accessed 03.02.11].Shiel Jr W. Lower back pain, http://www.medicinenet.com/low_back_pain/article.
htm [last accessed 03.02.11].Malanga G. Medication and treatment of acute low back pain, http://www.
spineuniverse.com/conditions/back-pain/low-back-pain/medication-and-treatment-acute-low-back-pain; 2009 [last accessed 03.02.11].