Embed Size (px)
Citation preview

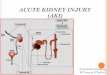
Acute Kidney Injury (AKI)
Emad A. Kelantan, MBBS
Umm Al Qura university, Makkah, K.S.A

Components
Definition.
Approach:
Hx.
Px.
Ix.s
Management & Treatment.
Case.
Extra notes.
25-Nov-12

Definition• AKI is an abrupt ( > 48 h ) deterioration in the renal
parenchymal excretory function i.e.
1. BUN …!!2. Creatinine level in the blood:
– 46 – 92 micromole/L– 0.6 – 1.2 mg/dl
3. UOP:– Oligouria if < 500 ml/24h or < 0.5 ml/kg/h × 24h– Auria if < 50 ml/24h
Azotemia Vs. Uremia?? 25-Nov-12

How to approach AKI?
1. Hx
2. Px
3. Ix.s
4. Management & treatment.
25-Nov-12

Hx DDx.
Pre- Renal Post- Decrease effective arterial volume i.e.
Hypovolemia e.g.Impaired cardiac contract. e.g.Systemic vasodilatation e.g.
Renal vasoconstriction e.g.
Large vessel pathology e.g.
Tubular (ATN) i.e.Ischemia i.e.Toxins:
• Drugs e.g.• Protein e.g.• Pigments e.g.• Crystals e.g.
CIAKI
Intrensic (AIN) i.e.Allergy e.g.Autoimmune e.g.Infection e.g.Infiltration e.g.
Small vessels pathology e.g.
Glomurulonephritis e.g.
Bladder neck e.g.
Ureteral (bilaterally) pathology e.g.
25-Nov-12

Px1. Vitals: ( What each sign indicates? )
T 39.9 C ??
BP 60/40 ??
P 20 bpm ??
O2 saturation 99% ??
RR 20 bpm ??
2. What other signs you are looking for regarding your DDx?
25-Nov-12

x.sI
What & Why ??
25-Nov-12

List of Ix.s that should be ordered in AKI
CBC.
Biochemistry.
Urine evaluation:1. UOP.
2. U/A.
3. U/E.
4. Osmolarity.
5. Sediment.
Fractional exertion of Na.
Renal U/S.
Serology if needed… ??
Renal Bx if needed… ??25-Nov-12

InterpretationIx.s
25-Nov-12

Management & Treatment• Treat underlying disorder, ? steroids if AIN.
• Avoid nephrotoxic insults; review dosing of renally cleared drugs.
• Optimize hemodynamics (both MAP & CO); may take 1–2 wks to recover from ATN
• Watch for and correct volume overload, electrolyte ( K, PO4), & acid/base status
• If obstruction is diagnosed and relieved, watch for:
– Hypotonic diuresis (2˚ buildup of BUN, tubular damage); Rx w/ IVF (e.g. 1⁄2 NS). – Hemorrhagic cystitis (rapid ∆ in size of bladder vessels); avoid by decompressing slowly.
• Indications for urgent dialysis (when condition refractory to conventional therapy)
Acid-base disturbance: acidemia Electrolyte disorder: generally hyperkalemia; occasionally hypercalcemia, tumor lysis Intoxication: methanol, ethylene glycol, lithium, salicylates Overload of volume (CHF) Uremia: pericarditis, encephalopathy, bleeding
• No benefit to dopamine (Annals 2005;142:510), diuretics (JAMA 2002;288:2547), or mannitol.
25-Nov-12

Case
25-Nov-12

Extra notesRIFLE classification BUN vs. SCr
25-Nov-12

References
• Kumar & Clark : Clinical Medicine, 7th edition.
• Pocket Medicine 4th Edition.
• FIRST AID for the CASES USMLE STEP2 CK Second Edition.
• USMLE : Internal Medicine CK 2011.
• www.Wikipedia.com
25-Nov-12

Thank youDone by .. Emad A. Kelantan on 25/11/2012
25-Nov-12