Embed Size (px)
Citation preview

1367
LETTERS
Acute Joint Dislocation-An Early Feature of Neuropathic Arthropathy To the Editor:
Neuropathic joint disease, described by Charcot in 1868 ( I ) , results from disturbance in the sensory innervation of the joint, which leads to repeated trauma, instability, and gross destruction. Joint dislocation may occur (2.3), but it has been noted only with advanced destructive changes i n the cartilage and bone. The patient with tabes dorsalis described here presents a striking exception to the usual course of neuropathic arthropathy. This individual incurred an acute total knee dislocation in the presence of only minimal degen- erative change. To our knowledge this clinical course of neuropathic arthropathy, with gross dislocation occur- ring in the early stages of the joint disease, has not been previously reported.
A 72-year-old female developed swelling and stiffness of the left knee in February 1975 and noted progressive "bowing" of the left leg. Deep tendon re-
flexes were absent from both lower extremities. Arthro- centesis of the left knee in May 1975 yielded 75 cm3 of slightly turbid, yellow fluid with a fair mucin and 180 leukocytes per mm3, 90% of which were mononuclear cells and 10% of which were segmented polymor- phonuclear leukocytes. Serum VDRL and fluorescent treponema antibody tests were positive. Spinal fluid was normal with respect to cells, protein, and serology. The patient was treated with a long-leg brace and re- ceived 4.8 X lo6 units of benzathine penicillin G . Nine months later, while pivoting on her left foot, she felt a pop in her left knee and immediately noted a marked painless swelling of that joint, which led her to seek medical attention.
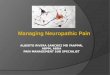
Examination revealed bilateral knee effusions with anterior dislocation of the left knee and minimal laxity of the right knee. Deep tendon reflexes and deep pain sensation were absent, and position sense was di- minished in both lower extremities. X-rays revealed bi- lateral knee effusions, mild degenerative changes, and total anterior dislocation of the left knee (Figure 1 ). A n arthrodesis was performed. Only minimal degeneration of the articular cartilage was noted at surgery.
It is likely that loss of proprioception and deep pain sensation in this patient resulted in abnormal stress on the knee joint. This stress, in combination with
Fig 1. Anteroposterior ( A ) and lateral ( B ) radiographs showing total anterior dislocation of left knee
Arthritis and Rheumatism, Val. 19, No. 6 (November-December 1976)

1368
stretching of the knee ligaments by the synovial effusion, produced gross joint dislocation. The case is unusual in that the dislocation occurred while the cartilage and bone were still relatively intact. I t emphasizes that changes in joint capsule and ligaments may at times be more significant than those in the hard tissues of the joint in the genesis of neuropathic arthropathy.
ALAN STEWART, M.D. DONALD B. KETTELKAMP, M.D. KENNETH D. BRANDT, M.D. Indiana University School of Medicine Indianapolis, Indiana 46202
REFERENCES
I . Charcot JM: Sur quelques arthropathies qui paraissent de- pendre d'une lesion cerveau ou de la moelle kpinikre. Arch Physiol Norm Pathol l:l6l, 1868
2. Eichenholtz SN: Charcot Joints. Springfield, Illinois, Thomas, 1966
3. Rodnan GP: Neuropathic joint disease, Arthritis and Al- lied Conditions. Eighth edition. Edited by J L Hollander, DJ McCarty, Jr. Philadelphia, Lea 8c Febiger, 1972, pp I 329- I339
Gold Levels in Kidney, Liver, and Spleen To the Editor:
The continued use of gold drugs in the treatment of rheumatoid arthritis has resulted in many studies of the plasma level of gold (1-3), but there are fewer re- ports of gold levels in internal organs of human subjects. One such study (4) on one subject showed that gold was distributed in a wide variety of tissues, had the greatest concentration in lymphatic tissues, and had the largest total amount in the reticuloendothelial tissues and in skin. These results broadly confirm the more extensive studies in animals (5). The gold levels detected are ex- tremely high, at least as high as the toxic levels of other heavy metals (6), and raise questions about the chemical form, toxicity, and bioavailability of the gold stores built up during therapy.
Recently we obtained samples of liver, kidney, spleen, and plasma from a white female who had re- ceived weekly 50-rng intramuscular injections of so- dium aurothiomalate (Myocrisin, May and Baker Ltd.) from 3/ 13/73 until 12/3 1 /74, when she developed an ex- foliative dermatitis of the abdomen and thighs, and therapy was discontinued. The total number of in-
Table 1. Tissue Determinations by Carbon Furnace Atomic A bsorption Spectrometry
rg/g Weight of Dry Weight No. of
Organ Organ (8) ofTissue Results RSD
Liver I I50 105.83 9 I .62 Spleen 390 51.9 9 1.85 Kidney - 112.3 9 3.57
jections was 35, i.e., a total dose of 1750 mg of Myocri- sin, equivalent to 875 mg of gold. She died on 1/13/76 following intractable gastrointestinal hemorrhage, for which she had received multiple transfusions involving the administration of 37 units (1 I . 1 L) of blood in the form of packed cells. The autopsy findings were con- gestive cardiac failure, esophageal ulceration (varices), portal hypertension, nodular noncirrhotic liver, and rheumatoid arthritis. We were able, therefore, to at- tempt to confirm the results of the previous study (4) and, in addition, to consider the effect of time on the tissue gold concentrations.
The blood level, detected using a new analytical procedure involving carbon furnace atomic absorption spectrometry (3), was 0.3 pg/ml compared to a norm of about 1.3 pg/ml of blood in subjects actually receiving gold therapy. (This latter figure varies quite widely, usu- ally falling in the range 0.5-7.0 pg/ml of plasma (1-3). We recently showed that about 96% of the gold is bound to plasma protein, so these figures are equivalent to about 0.2-2.8 pg/ml of blood.) Consideration of the length of time since gold therapy was discontinued and the effect of the blood transfusions suggests the possi- bility that some of the gold stored in the tissues may have been redissolved into the blood. A study of patients on gold therapy up to 216 days past injection reached a similar conclusion (7).
Tissue determinations, also by carbon furnace atomic absorption spectrometry (8), are presented in Table 1 .
In the previous study (4), in which the patient died while undergoing gold therapy, the liver and spleen levels were 559 and 368 pg/g dry weight respectively, and the plasma level, which was rather high compared to recent studies (1,2), was 9.9 pg/ml of plasma. Thus the ratio of liver to spleen levels is similar in both cases and, although the total levels are lower in the present study, they are extremely high even a year after the cessation of therapy. The kidney level determination is the first reported in a human subject. It demonstrates that even this organ cannot clear gold quickly and, indeed, the ratio of kidney to liver levels is similar to