Embed Size (px)
Citation preview

elttaa6icepntpnwlo
en
Iwoebe
RA
The Journal of Emergency Medicine, Vol. 35, No. 2, pp. 167–170, 2008Copyright © 2008 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/08 $–see front matter
doi:10.1016/j.jemermed.2007.06.043
ClinicalCommunications: Adults
ACUTE COLONIC PSEUDO-OBSTRUCTION: RAPID CORRECTION WITHNEOSTIGMINE IN THE EMERGENCY DEPARTMENT
Robert McNamara, MD, FAAEM and Michael J. Mihalakis, MD
Department of Emergency Medicine, Temple University School of Medicine, Philadelphia, PennsylvaniaReprint Address: Robert McNamara, MD, FAAEM, Department of Emergency Medicine, Jones Hall, 10th Floor, Temple University School
of Medicine, 3401 North Broad Street, Philadelphia, PA 19140
gssaodaaTlt
ccmudsoo
Anaco
Abstract—Ogilvie’s syndrome, now known as acute co-onic pseudo-obstruction, is characterized by massive dila-ation of large bowel in the absence of mechanical obstruc-ion. It is found in a variety of patients, although elderlynd immobile patients make up a large portion of thefflicted population. This article discusses the case of a4-year-old bedridden, paraplegic, male nursing home res-dent who presented to the Emergency Department with ahronic history of abdominal distention that acutely wors-ned on the day of his arrival. A diagnosis of acute colonicseudo-obstruction was made and 2 mg of intravenouseostigmine was administered, with resolution of the pa-ient’s condition allowing for subsequent Emergency De-artment discharge. This report discusses the utilization ofeostigmine, an acetylcholinesterase inhibitor, for patientsith colonic pseudo-obstruction. We also briefly review the
iterature on this condition and other therapeuticptions. © 2008 Elsevier Inc.
Keywords—Ogilvie’s syndrome; pseudo-obstruction;eostigmine; abdomen; elderly
INTRODUCTION
n 1948, Sir Heneage Ogilvie recounted two cases inhich, “the symptoms so strongly suggested obstructionf the distal colon by a carcinoma that laparotomy wasventually undertaken in spite of normal findings in aarium enema” (1). The theories behind this clinicalntity have continued to evolve. Current literature sug-
ECEIVED: 25 February 2007;
CCEPTED: 12 June 2007167
ests that Ogilvie’s syndrome is a product of excessiveympathetic stimulation coupled with decreased para-ympathetic impulses, leading to an adynamic ileus, not,s Ogilvie hypothesized, a result of parasympatheticveractivity (1,2). The preferred terminology of this con-ition is now colonic pseudo-obstruction. Left untreated,cute colonic pseudo-obstruction can lead to ischemiand perforation in anywhere from 3% to 15% of cases.he 50% mortality that accompanies perforation high-
ights the need for prompt diagnosis and appropriatereatment (3,4).
This article discusses the use of neostigmine to suc-essfully decompress an uncomplicated case of acuteolonic pseudo-obstruction in the emergency depart-ent. We are unaware of any prior reports describing the
se of this agent for this condition in the emergencyepartment. This therapy incorporates the current under-tanding of the pathophysiology of colonic pseudo-bstruction and provides emergency physicians with thepportunity to improve outcomes for afflicted patients.
CASE REPORT
64-year-old man was sent via ambulance from a localursing home to our Emergency Department for severebdominal distention. The nursing home staff reportedoncern about a significant increase in abdominal girthn the day of presentation. The nursing home did not

rdmfnidabhds
3bpnbtefantinf
wbmcoTt
f1tOpcc
olp2pbmabwgvwms
RptatiFlpdbiatbfaot
attadl
F
168 R. McNamara and M. J. Mihalakis
eport vomiting, fever, or abdominal pain, and also in-icated that the patient had a small non-bloody bowelovement on the day of his presentation. The history
rom the patient, tempered by his baseline dementia, wasotable for a lack of abdominal pain, nausea, or vomit-ng. In addition, his past history was significant foriabetes mellitus, hypertension, hepatitis C, meningitis,nd an unspecified delusional disorder. The patient wasedridden and paraplegic. Current medications includedaloperidol, as well as the gastrointestinal agents bisaco-yl and senna. There was no history of prior abdominalurgery, diverticular disease, or malignancy.
The vital signs were as follows: rectal temperature6.8°C, pulse rate 92 beats/min, respiratory rate 16reaths/min, and blood pressure 130/80 mm Hg. Uponhysical examination, the patient was observed to be ino distress. The skin was warm and the mucous mem-ranes were moist. Dry bibasilar crackles were noted onhe pulmonary examination, and there was trace pedaldema. The abdomen was massively distended, and dif-usely tympanitic with hypoactive bowel sounds. Nobdominal tenderness was present, and a fluid wave wasot detected. On rectal examination, the vault was notedo be cavernous without masses or evidence of fecalmpaction. A small amount of soft brown stool wasegative for blood by a guaiac test. No inguinal oremoral hernias were detected on examination.
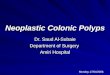
The complete blood count and serum chemistry panelere normal, with the exception of a mildly increasedlood urea nitrogen (24 mg/dL) and glucose of 145g/dL. A plain abdominal radiograph revealed signifi-
ant diffuse colonic dilatation with a maximal diameterf 15 cm in the region of the sigmoid colon (Figure 1).he patient’s prior radiographic investigations were re-
rieved from the computerized archives and a plain film
tigure 1. Pre-treatment supine abdominal radiograph.
rom 3 weeks prior demonstrated a colonic diameter of7 cm. This study had been followed by a barium enemahat did not uncover volvulus or an obstructing lesion.ld records were obtained and it was noted that theatient had been admitted for colonic distention on oc-asion, including 3 weeks prior, when treatment includedolonic decompression through colonoscopy.
Given the prior history and investigations, a diagnosisf colonic pseudo-obstruction was deemed the mostikely cause of abdominal distention. The patient waslaced on a cardiac monitor and a physician administeredmg of intravenous neostigmine. Within minutes, the
atient began to pass large amounts of gas accompaniedy small amounts of soft stool per rectum. Within 30in, the abdomen was soft, markedly reduced in size,
nd no longer tympanitic. The patient did not manifestradycardia over 1 h of observation and was dischargedith no further interventions. A repeat abdominal radio-raph was not obtained, as the clinical assessment re-ealed complete resolution of the distention. Follow-upas conducted and there was no subsequent need foredical care related to his abdominal condition in the
ucceeding 6 months.
DISCUSSION
evised from Ogilvie’s original hypothesis of parasym-athetic over-activity, the prevailing theory regardinghis syndrome of marked dilatation of the colon in thebsence of mechanical obstruction is one of altered au-onomic activity, that is, decreased parasympathetic tonen conjunction with increased sympathetic impulses (5).irst described in two cases with malignancy of the
umbar spine, other associated conditions now includeost-surgical states, immobility, neurologic disease, car-iopulmonary disease, diabetes mellitus, electrolyte im-alances, trauma, burns, and medications such as narcot-cs, tricyclics, and phenothiazines (2,6,7). The elderlynd immobile patients account for the largest group ofhese patients (6). The patient in this report, as an elderly,edridden paraplegic with diabetes, was clearly at riskor this illness. We believe that this is a novel use of thisgent in the ED for a patient with colonic pseudo-bstruction, and it resulted in successful discharge backo his chronic care facility.
When considering this condition, the first prioritiesre to exclude ischemia, perforation, or the presence of arue mechanical obstruction. In this patient, the presen-ation, diagnostic testing, and recent hospital recordsllowed the treating physicians to be secure in theiriagnosis. The absence of pain, tenderness, fever, andeukocytosis made perforation unlikely. In the absence of
his prior history and these clinical features, this patient
wu
ctvopstfitLpsbraioc
oodirpmtdti
aaaiadqdw
uwr(coc1rs
2wt
tufncftcdmima
pscstw(abtda
ncpmabtsaaap
pnmbHiAmT
Colonic Pseudo-obstruction 169
ould have required further investigation to delineate thenderlying condition.
The main differential diagnosis of importance is me-hanical obstruction of the colon. The majority of pa-ients with pseudo-obstruction will not have nausea oromiting, and a number will report the passage of stoolr flatus (8,9). Distention and tympany are to be ex-ected, but, as in this patient, massive distention withoutignificant pain or discomfort on examination suggestshe diagnosis (8–10). Plain radiography may be useful ifndings indicate volvulus, but may not differentiate be-
ween true and pseudo-obstruction (8,9). Ponec et al. andoftus et al. diagnosed pseudo-obstruction when thelain radiograph demonstrated air throughout all colonicegments including the rectosigmoid colon (5,11). Ab-asakoor et al. criticized this practice as dangerous, andecommended advanced radiographic investigation with
water-soluble contrast enema before pharmacologicntervention for all suspected cases (12). Often, a searchf old records will indicate prior evaluations for thisondition, as recurrence is common (3).
Current treatment recommendations for colonic pseudo-bstruction include a conservative pathway that includesbservation, nasogastric tube suctioning, intravenous hy-ration, electrolyte correction, discontinuing precipitat-ng medications when possible, and the placement of aectal tube or rectal examination every 6 h along withatient ambulation or bed turning. Should the aboveeasures fail, practitioners then utilize alternative
reatment strategies, including neostigmine or colonicecompression, with surgical intervention reserved forhose cases that have not responded to the aboventerventions (3).
Ischemia and perforation are responsible for most of thessociated complications of colonic pseudo-obstruction,nd a great deal of research has focused upon establishingppropriate guidelines for when, in the absence of clearndications for surgery, to initiate conservative treatments opposed to more aggressive measures such as colonicecompression and surgical intervention. The centraluestion has always been, is there a degree of colonicistention (the cecal diameter is most commonly cited) athich one must abandon conservative measures?Several authors advocate conservative therapy in all
ncomplicated cases of colonic pseudo-obstruction, evenith cecal diameters up to 18 cm (7,11,13,14). Success
ates of a conservative pathway range from 33% to 100%7–9,14–20). Others tie the risk of perforation to theecal diameter. For example, a review of over 400 casesf colonic pseudo-obstruction found no perforations at aecal diameter � 12 cm, a 7% rate for diameters of2–14 cm, and a 23% rate for � 14 cm (21). Othereports confirmed a cecal diameter of 12 cm as the
tarting level for an increasing risk of perforation (22– m5). In deciding on an initial strategy, the clinician musteigh the benefits of conservative treatment vs. the po-
ential for perforation.Citing the wide variability in cecal diameters leading
o perforation, other authorities place more importancepon the duration of dilatation in predicting the chanceor colonic rupture. For example, a 1979 study reportedo perforations in patients who were successfully de-ompressed in � 72 h despite cecal diameters rangingrom 10 to 25 cm (15). Other studies report no perfora-ions or a significantly decreased mortality if there islinical resolution within 4 days (4,21). In light of theseata indicating higher complications with delayed treat-ent, a renewed emphasis has been placed upon earlier
ntervention and the use of medications such as neostig-ine to rapidly address the syndrome and minimize
ssociated sequelae.If conservative measures fail, colonoscopic decom-
ression is generally recommended, as studies demon-trate its efficacy along with fewer complications asompared to surgical intervention (3,21,26,27). A 1989tudy found colonoscopy to be curative in 44% of pa-ients, with complications occurring in 6% of the sample,hereas surgery resulted in a complication rate of 57%
14). Surgery is then reserved for those who fail or suffercomplication of colonic decompression. Surgery has
een previously recommended as the initial approach forhose with duration of dilatation � 72 h, abdominalistention causing cardiopulmonary embarrassment and,s discussed above, a cecal diameter � 12–14 cm (28).
Numerous reports have detailed the efficacy ofeostigmine, including a double-blinded, placebo-ontrolled trial published in 1999 (5). In this study of 21atients, neostigmine had a success rate of 73%, with theost serious complications being two cases of symptom-
tic bradycardia responsive to atropine. One case ofradycardia occurred while the patient was ambulating tohe restroom approximately 30 min after treatment. Othertudies have shown similar, if not better, success ratesnd no serious complications. Clinical response gener-lly occurs within 30 min (11,29–33). Loftus et al. noteddecrease in length of stay from 11 to 4 days as com-
ared to treatment with colonoscopy (11).Typical side effects of neostigmine include abdominal
ain, salivation, vomiting, and diaphoresis. There areumerous contraindications to treatment with neostig-ine, including recent myocardial infarction, acidosis,
eta-blocker therapy, systolic blood pressure � 90 mmg, pulse � 60 beats/min, bronchospasm requiring med-
cal treatment, and creatinine � 3 mg/dL (5,11,29–33).s with other non-invasive methods, the use of neostig-ine is not recommended with evidence of perforation.he effects of the mistaken administration of neostig-
ine in a patient with mechanical obstruction have not
bocr
spdttsdghoca
Timmsa
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
170 R. McNamara and M. J. Mihalakis
een reported, but it is theorized that the administrationf this potent colonic stimulator could lead to adverseonsequences (12). The half-life of neostigmine is short,anging from 25 to 80 min (30).
Neostigmine seems to be an effective treatment withuccess rates comparable to other accepted treatmentathways such as conservative treatment, colonoscopicecompression, and surgery. The number of complica-ions noted in the neostigmine trials is low and far lesshan those noted in the colonoscopic decompression andurgical trials. As outlined above, neostigmine-inducedecompression is usually rapid, thus providing the emer-ency physician with the ability to discharge the patientome or, if admitted, to likely decrease the overall lengthf stay. If the use of neostigmine is successful, thelinician should address any correctable inciting event inn attempt to limit recurrence.
CONCLUSION
he emergency physician may have the opportunity tontervene to the patient’s benefit with the use of neostig-ine if the diagnosis of colonic pseudo-obstruction isade in the emergency department. For the appropriately
elected patient, serious complications of neostigminere few and the clinical response is rapid.
REFERENCES
1. Ogilvie H. Large intestinal colic due to sympathetic denervation: aclinical syndrome. Br Med J 1948;1:671–3.
2. Kahi CJ, Rex DK. Bowel obstruction and pseudo-obstruction.Gastroenterol Clin North Am 2003;32:1229–47.
3. Rex DK. Colonoscopy and acute colonic pseudo-obstruction. Gas-trointest Endosc Clin N Am 1997;7:499–508.
4. Johnson CD, Rice RP, Kelvin FM, Foster WL, Williford ME. Theradiographic evaluation of gross cecal distention: emphasis oncecal ileus. AJR Am J Roentgenol 1985;145:1211–7.
5. Ponec RJ, Saunders MD, Kimmey MB. Neostigmine for the treat-ment of acute colonic pseudo-obstruction. N Engl J Med 1999;341:137–41.
6. Hyatt R. Colonic pseudo-obstruction: an important complication inhospitalized elderly patients. Age Ageing 1987;16:145–52.
7. Sloyer AF, Panella VS, Demas BE, et al. Ogilvie’s syndrome:successful management without colonoscopy. Dig Dis Sci 1988;33:1391–6.
8. Bachulis BL, Smith PE. Pseudo-obstruction of the colon. Am JSurg 1978;136:66–72.
9. Gilchrist AM, Mills JO, Russell CG. Acute large-bowel pseudo-
obstruction. Clin Radiol 1985;36:401–4.0. Geelhoed GW. Colonic pseudo-obstruction in surgical patients.Am J Surg 1985;149:258–65.
1. Loftus CG, Harewood GC, Baron TH. Assessment of predictors ofresponse to neostigmine for acute colonic pseudo-obstruction.Am J Gastroenterol 2002;97:3118–22.
2. Abbasakoor F, Evans A, Stephenson BM. Neostigmine for acutecolonic pseudo-obstruction [letter]. N Engl J Med 1999;34:1622.
3. Nanni G, Garbini A, Luchetti P, Nanni G, Ronconi P, CastagnetoM. Ogilvie’s syndrome (acute colonic pseudo-obstruction): reviewof the literature (October 1948 to March 1980) and report of fouradditional cases. Dis Colon Rectum 1982;25:157–66.
4. Hart MB, Rosemurgy AS. Cecal pseudo-obstruction: early therapyshould be nonoperative. Am Surg 1989;56:43–6.
5. Baker DA, Morin ME, Tan A, Sue H. Colonic ileus. Indication forprompt decompression. JAMA 1979;241:2633–4.
6. Bullock PR, Thomas WE. Acute pseudo-obstruction of the colon.Ann R Coll Surg Engl 1984;66:327–30.
7. Koneru B, Selby R, O’Hair DP, Tzakis AG, Hakala TR, Starzl TE.Nonobstructing colonic dilatation and colon perforations followingrenal transplantation. Arch Surg 1990;125:610–3.
8. Moses Y, Weissberg D, Kaufman M, Weizbard E. Acute pseudo-obstruction of the colon. S Afr J Surg 1991;29:18–20.
9. Stratta RJ, Starling JR, D’Alessandro AM, et al. Acute colonicileus (pseudo-obstruction) in renal transplant recipients. Surgery1988;104:616–23.
0. Watson CJ, Jamieson NV, Johnston PS, et al. Early abdominalcomplications following heart and heart-lung transplantation. Br JSurg 1991;78:699–704.
1. Vanek VW, Al-Salti M. Acute pseudo-obstruction of the colon(Ogilvie’s syndrome): an analysis of 400 cases. Dis Colon Rectum1986;29:203–10.
2. Gierson ED, Storm FK, Shaw W, Coyne SK. Caecal rupture due tocolonic ileus. Br J Surg 1975;62:383–6.
3. Melzig EP, Terz JJ. Pseudo-obstruction of the colon. Arch Surg1978;113:1186–90.
4. Waldron R, Johnston J. Ogilvie’s syndrome. J R Coll Surg Edinb1983;28:388–90.
5. Wanebo HW, Mathewson C, Connolly B. Pseudo-obstruction ofthe colon. Surg Gynecol Obstet 1971;7:44–8.
6. Geller A, Peterson BT, Gostout CJ. Endoscopic decompressionfor acute colonic pseudo-obstruction. Gastroint Endosc 1996;44:144–50.
7. Jetmore AB, Timmcke AE, Gathright JB, Hicks TC, Ray JE, BakerJW. Ogilvie’s syndrome: colonoscopic decompression and analy-sis of predisposing factors. Dis Colon Rectum 1992;35:1135–42.
8. Schuffler MD, Deitch EA. Chronic idiopathic intestinal pseudo-obstruction: a surgical approach. Ann Surg 1980;192:752–61.
9. Breccia M, Girmenia C, Mecarocci S, et al. Ogilvie’s syndrome inacute myeloid leukemia: pharmacological approach with neostig-mine. Ann Hematol 2001;80:614–6.
0. De Giorgio R, Barbara G, Stanghellini V, et al. Review article: thepharmacological treatment of acute colonic pseudo-obstruction.Aliment Pharmacol Ther 2001;15:1717–27.
1. Paran H, Silverberg D, Mayo A, Shwartz I, Neufeld D, Freund U.Treatment of acute colonic pseudo-obstruction with neostigmine.J Am Coll of Surg 2000;190:315–8.
2. Stephenson BM, Morgan AR, Salaman JR, Wheeler MH. Ogilvie’ssyndrome: a new approach to an old problem. Dis Colon Rectum1995;38:424–7.
3. Turegano-Fuentes F, Munoz-Jimenez F, Del Valle-Hernandez E, etal. Early resolution of Ogilvie’s syndrome with intravenousneostigmine: a simple, effective treatment. Dis Colon Rectum
1997;40:1353–7.













![Case Report The Use of Intravenous Neostigmine in ...downloads.hindawi.com/journals/crigm/2013/796739.pdf · [] R. McNamara and M. J. Mihalakis, Acute colonic pseudo- obstruction:](https://img.pdfslide.us/doc/110x75/5f3dcf01d21a5c60af4c94e4/case-report-the-use-of-intravenous-neostigmine-in-r-mcnamara-and-m-j-mihalakis.jpg)