Embed Size (px)
DESCRIPTION
Acute Cholangitis Workup_ Laboratory Studies, Imaging Studies, Ultrasonography
Citation preview

7/10/2015 Acute Cholangitis Workup: Laboratory Studies, Imaging Studies, Ultrasonography
http://emedicine.medscape.com/article/774245workup#showall 1/4
Acute Cholangitis WorkupAuthor: Timothy M Scott, DO; Chief Editor: Barry E Brenner, MD, PhD, FACEP more...
Updated: Nov 10, 2014
Laboratory StudiesLaboratory studies include the following:
CBC: Leukocytosis: In patients with cholangitis, 79% had a WBC greater than 10,000/mL, with a mean of13.6. Septic patients may be leukopenic.Electrolyte panel with renal function may be performed.Calcium level is necessary to check if pancreatitis, which can lead to hypocalcemia, is a concern.Expect liver function test results to be consistent with cholestasis, hyperbilirubinemia (88100%), andincreased alkaline phosphatase level (78%).Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels are usually mildly elevated.Prothrombin time and activated partial thromboplastin time: Do not expect either to be elevated unlesssepsis is associated with disseminated intravascular coagulation or underlying cirrhosis exists. A coagulationprofile may be required if the patient needs operative intervention.Creactive protein level and erythrocyte sedimentation rate are typically elevated.[3]Blood cultures (2 sets): Between 20% and 30% of blood cultures are positive. Many exhibit polymicrobialinfections.Urinalysis result is usually normal.Blood type, screen, and crossmatch: With urgent operating room dispatch, patients need to have bloodavailable.Lipase: Involvement of the lower CBD may cause pancreatitis and an elevated lipase level. One third ofpatients have a mildly elevated lipase level.Pancreatic enzyme elevations suggest that bile duct stones caused the cholangitis, with or without gallstonepancreatitis.[7]Biliary cultures (not performed in the ED): Send biliary cultures if the patient has biliary drainage byinterventional radiology or endoscopy.
Imaging StudiesImaging studies are important to confirm the presence and cause of biliary obstruction and to rule out otherconditions. Ultrasonography and CT scanning are the most commonly used firstline imaging modalities.
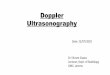
UltrasonographyUltrasonography is excellent for gallstones and cholecystitis. It is highly sensitive and specific for examining thegallbladder and assessing bile duct dilatation (see the following image). However, it often misses stones in the distalbile duct.[8]
Sonogram of dilated intrahepatic ducts.
Consider the following:
Transabdominal ultrasonography is the initial imaging study of choice.Ultrasonography can differentiate intrahepatic obstruction from extrahepatic obstruction and image dilatedducts.In one study of cholangitis, only 13% of CBD stones were observed on ultrasonography, but dilated CBD wasfound in 64%.Advantages to sonography include the ability to be performed rapidly at the bedside by the ED physician,capacity to image other structures (eg, aorta, pancreas, liver), identification of complications (eg, perforation,empyema, abscess), and lack of radiation.Disadvantages to sonography include operator and patient dependence, cannot image the cystic duct, anddecreased sensitivity for distal CBD stones.A normal sonogram does not rule out acute cholangitis.
Endoscopic Retrograde CholangiopancreatographyEndoscopic retrograde cholangiopancreatography (ERCP) is both diagnostic and therapeutic and is considered thecriterion standard for imaging the biliary system.
ERCP should be reserved for patients who may require therapeutic intervention. Patients with a high clinicalsuspicion for cholangitis should proceed directly to ERCP.
ERCP has a high success rate (98%) and is considered safer than surgical and percutaneous intervention.
Diagnostic use of ERCP carries a complication rate of approximately 1.38% and a mortality rate of 0.21%. The

7/10/2015 Acute Cholangitis Workup: Laboratory Studies, Imaging Studies, Ultrasonography
http://emedicine.medscape.com/article/774245workup#showall 2/4
major complication rate of therapeutic ERCP is 5.4%, and it has a mortality rate of 0.49%. Complications includepancreatitis, bleeding, and perforation.[9]
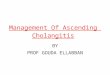
CT ScanningCT is adjunctive to and may replace ultrasonography. Spiral or helical CT improves imaging of the biliary tree. CTcholangiography uses a contrast agent that is taken up by the hepatocytes and secreted into the biliary system. Thisenhances the ability to visualize radiolucent stones and increases detection of other biliary pathology.
Dilated intrahepatic (see the image below)and extrahepatic ducts and inflammation of the biliary tree are imaged.Gallstones are poorly visualized with traditional CT scan.
CT scan of dilated intrahepatic bile ducts. Image courtesy of David Schwartz, MD, New York University Hospital.
Advantages of CT include the following:
Other pathologies that are causes or complications of cholangitis (eg, ampullary tumors, pericholecystic fluid,liver abscesses) can be imaged.Pathology that must be distinguished from cholangitis also can be observed (eg, rightsided diverticulitis,papillary necrosis, some evidence of pyelonephritis, mesenteric ischemia, ruptured appendix).Detection of biliary pathology with CT cholangiography approaches that of ERCP.
Disadvantages of CT include poor imaging of gallstones, allergic reaction to contrast, exposure to ionizing radiation,and diminished ability to visualize the biliary tree with elevated serum bilirubin level.
Magnetic Resonance CholangiopancreatographyMagnetic resonance cholangiopancreatography (MRCP) is a noninvasive imaging modality that is increasingly beingused in the diagnosis of biliary stones and other biliary pathology.
MRCP is accurate for detecting choledocholithiasis, neoplasms, strictures, and dilations within the biliary system.
Limitations of MRCP include the inability for invasive diagnostic tests such as bile sampling, cytologic testing, stoneremoval, or stenting. It has limited sensitivity for small stones (< 6 mm in diameter).
Absolute contraindications are the same as for a traditional MRI, which include the presence of a cardiacpacemaker, cerebral aneurysm clips, ocular or cochlear implants, and ocular foreign bodies. Relativecontraindications include the presence of cardiac prosthetic valves, neurostimulators, metal prostheses, and penileimplants.
The risk of MRCP during pregnancy is not known.
RadiographyIn general, abdominal films aid little in the diagnosis of acute cholangitis. Findings may include the following:
An ileus may be observed.Between 10% and 30% of gallstones have a ring of calcium and, as a result, are radiopaque.Films may show air in the biliary tree after endoscopic manipulation or if the patient has emphysematouscholecystitis, cholangitis, or a cholecysticenteric fistula.Air in the gallbladder wall indicates emphysematous cholecystitis.
Nuclear ImagingBiliary scintigraphy (hepatic 2,6dimethyliminodiacetic acid [HIDA] and diisopropyl iminodiacetic acid [DISIDA])scans are functional studies of the gallbladder.
Obstruction of the CBD causes nonvisualization of the small intestine. A HIDA scan with complete biliaryobstruction does not visualize the biliary tree.
Advantages include their ability to assess function and positive results may appear before the ducts are enlargedsonographically.
One disadvantage is that high bilirubin levels (>4.4) may decrease the sensitivity of the study. Recent eating or nofood in 24 hours also may affect the study. In addition, anatomic imaging for other structures is lacking. The studytakes several hours, so it is not recommended in critically ill or unstable patients.
ProceduresED physicians generally do not perform procedures for cholangitis (eg, ERCP and transhepatic decompression).
If an obstruction is observed, ERCP provides direct visualization and potential treatment. It is best performed after72 hours of antibiotics or after resolution of fever.
In unstable patients, a reasonable option for decompression of the biliary tract is percutaneous transhepaticcholangiogram and biliary drain. The biliary ducts are observed, even when no ductal dilatation is present.

7/10/2015 Acute Cholangitis Workup: Laboratory Studies, Imaging Studies, Ultrasonography
http://emedicine.medscape.com/article/774245workup#showall 3/4
Contributor Information and DisclosuresAuthorTimothy M Scott, DO Chief Resident, Department of Emergency Medicine, Detroit Medical Center, WayneState University School of Medicine
Timothy M Scott, DO is a member of the following medical societies: American College of EmergencyPhysicians, American Medical Association, American Osteopathic Association, Emergency MedicineResidents' Association
Disclosure: Nothing to disclose.
Coauthor(s)Adam J Rosh, MD Assistant Professor, Program Director, Emergency Medicine Residency, Department ofEmergency Medicine, Detroit Receiving Hospital, Wayne State University School of Medicine
Adam J Rosh, MD is a member of the following medical societies: American Academy of Emergency Medicine,American College of Emergency Physicians, Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
Specialty Editor BoardFrancisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center Collegeof Pharmacy; EditorinChief, Medscape Drug Reference
Disclosure: Received salary from Medscape for employment.
Chief EditorBarry E Brenner, MD, PhD, FACEP Professor of Emergency Medicine, Professor of Internal Medicine,Program Director for Emergency Medicine, Case Medical Center, University Hospitals, Case Western ReserveUniversity School of Medicine
Barry E Brenner, MD, PhD, FACEP is a member of the following medical societies: Alpha Omega Alpha,American Heart Association, American Thoracic Society, Arkansas Medical Society, New York Academy ofMedicine, New York Academy of Sciences, Society for Academic Emergency Medicine, American Academy ofEmergency Medicine, American College of Chest Physicians, American College of Emergency Physicians,American College of Physicians
Disclosure: Nothing to disclose.
AcknowledgementsEugene Hardin, MD, FAAEM, FACEP Former Chair and Associate Professor, Department of EmergencyMedicine, Charles Drew University of Medicine and Science; Former Chair, Department of Emergency Medicine,Martin Luther King Jr/Drew Medical Center
Disclosure: Nothing to disclose.
Jeffrey A Manko, MD A ssistant Professor of Emergency Medicine, Director, Emergency Medicine ResidencyProgram, Consulting Staff, Emergency Medicine Services, New York University/Bellevue Medical Center
Jeffrey A Manko, MD is a member of the following medical societies: American College of EmergencyPhysicians, Council of Emergency Medicine Residency Directors, and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
Sally Santen, MD Program Director, Assistant Professor, Department of Emergency Medicine, VanderbiltUniversity
Sally Santen, MD is a member of the following medical societies: American College of Emergency Physiciansand Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
References
1. Aron JH, Bowlus CL. The immunobiology of primary sclerosing cholangitis. Semin Immunopathol. 2009Sep. 31(3):38397. [Medline]. [Full Text].
2. Kashyap R, Mantry P, Sharma R, et al. Comparative analysis of outcomes in living and deceased donorliver transplants for primary sclerosing cholangitis. J Gastrointest Surg. 2009 Aug. 13(8):14806. [Medline].
3. van Erpecum KJ. Gallstone disease. Complications of bileduct stones: Acute cholangitis and pancreatitis.Best Pract Res Clin Gastroenterol. 2006. 20(6):113952. [Medline].
4. Rosing DK, De Virgilio C, Nguyen AT, El Masry M, Kaji AH, Stabile BE. Cholangitis: analysis of admissionprognostic indicators and outcomes. Am Surg. 2007 Oct. 73(10):94954. [Medline].
5. Kinney TP. Management of ascending cholangitis. Gastrointest Endosc Clin N Am. 2007 Apr. 17(2):289306, vi. [Medline].
6. Jabara B, Fargen KM, Beech S, Slakey DR. Diagnosis of cholangiocarcinoma: a case series and literaturereview. J La State Med Soc. 2009 MarApr. 161(2):8994. [Medline].
7. Attasaranya S, Fogel EL, Lehman GA. Choledocholithiasis, ascending cholangitis, and gallstonepancreatitis. Med Clin North Am. 2008 Jul. 92(4):92560, x. [Medline].
8. Rustemovic N, CukovicCavka S, Opacic M, et al. Endoscopic ultrasound elastography as a method forscreening the patients with suspected primary sclerosing cholangitis. Eur J Gastroenterol Hepatol. 2010Jun. 22(6):74853. [Medline].
9. Iorgulescu A, Sandu I, Turcu F, Iordache N. PostERCP acute pancreatitis and its risk factors. J Med Life.2013 Mar 15. 6(1):10913. [Medline]. [Full Text].
10. Sharma BC, Agarwal N, Sharma P, Sarin SK. Endoscopic biliary drainage by 7 Fr or 10 Fr stentplacement in patients with acute cholangitis. Dig Dis Sci. 2009 Jun. 54(6):13559. [Medline].
11. Itoi T, Kawai T, Sofuni A, et al. Efficacy and safety of 1step transnasal endoscopic nasobiliary drainage

7/10/2015 Acute Cholangitis Workup: Laboratory Studies, Imaging Studies, Ultrasonography
http://emedicine.medscape.com/article/774245workup#showall 4/4
Medscape Reference © 2011 WebMD, LLC
for the treatment of acute cholangitis in patients with previous endoscopic sphincterotomy (with videos).Gastrointest Endosc. 2008 Jul. 68(1):8490. [Medline].
12. Park TY, Choi JS, Song TJ, et al. Early oral antibiotic switch compared with conventional intravenousantibiotic therapy for acute cholangitis with bacteremia. Dig Dis Sci. 2014 Nov. 59(11):27906. [Medline].
























![Surgery cholangitis[1]](https://img.pdfslide.us/doc/110x75/55506071b4c90574428b52be/surgery-cholangitis1.jpg)

