Embed Size (px)
Citation preview
Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
1
guidelines for the diagnosis and management of patients with thoracic aortic disease proposed a standard approach to the diagnosis and treatment of AAS.3
Although clinical history and physical examination are important, imaging is essential in the diagnosis of AAS. Transesophageal echocardiography (TEE), computed tomography (CT), and magnetic resonance imaging (MRI) are the preferred imaging modalities and angiography is rarely needed.
CLASSIFICATION OF ACUTE AORTIC SYNDROMES
Historically, CAAD was the first recognized form of AAS. The classification schemes used for the classic aortic dissection were subsequently extended to include IMH and PAU.
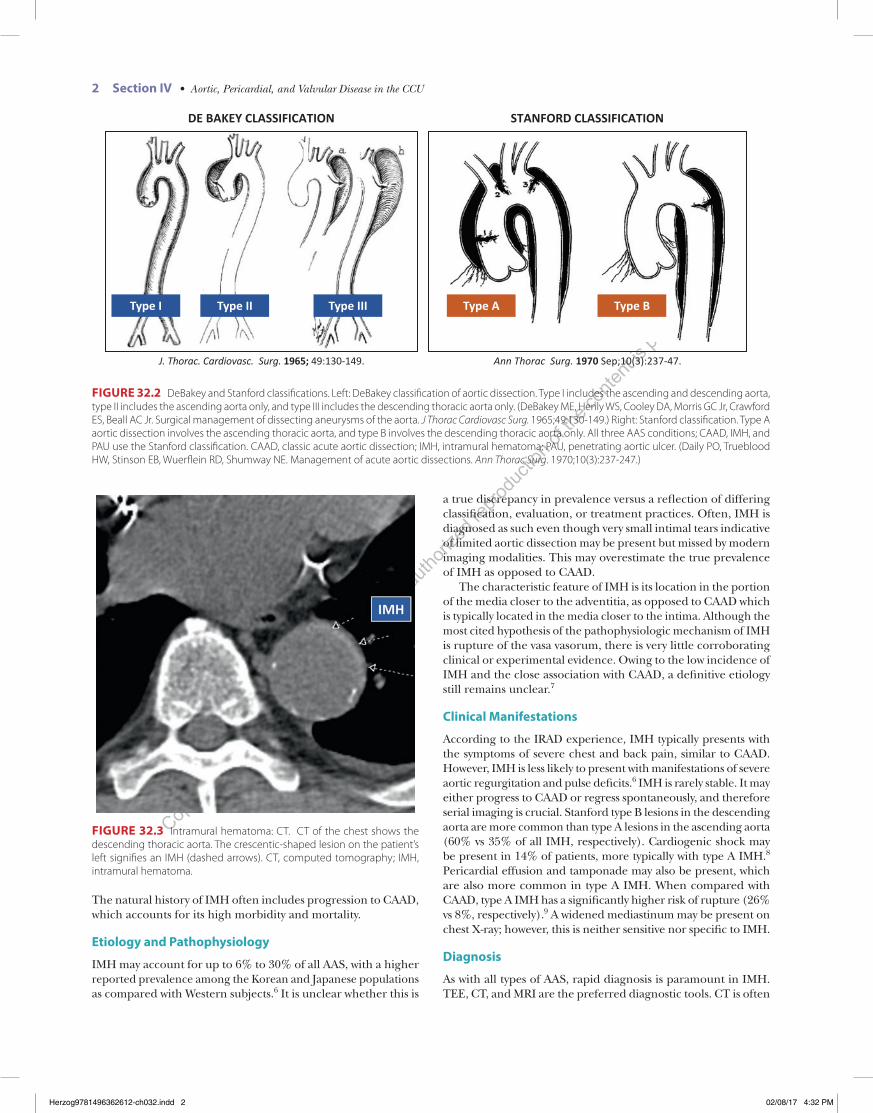
AASs are classified on the basis of the location and extent of involvement of the aorta. Two systems have been proposed, the DeBakey and the Stanford systems (Figure 32.2). The DeBakey system, which was proposed in 1965 by the Lebanese-American surgeon Michael Ellis DeBakey, divided aortic dissection into three types based on the anatomic location. Type I originates in the ascending aorta and propagates beyond the aortic arch, type II is limited to the ascending aorta only, and type III is limited to the descending aorta.4
The Stanford system, which was created by researchers at Stanford University in 1970, divides aortic dissections into two types. Type A includes any dissection that involves the ascending aorta, whereas type B dissections are limited to the descending thoracic aorta.5 The Stanford classification appears to have wider acceptance and is now used for all three AAS types: CAAD, IMH, and PAU.
INTRAMURAL HEMATOMA
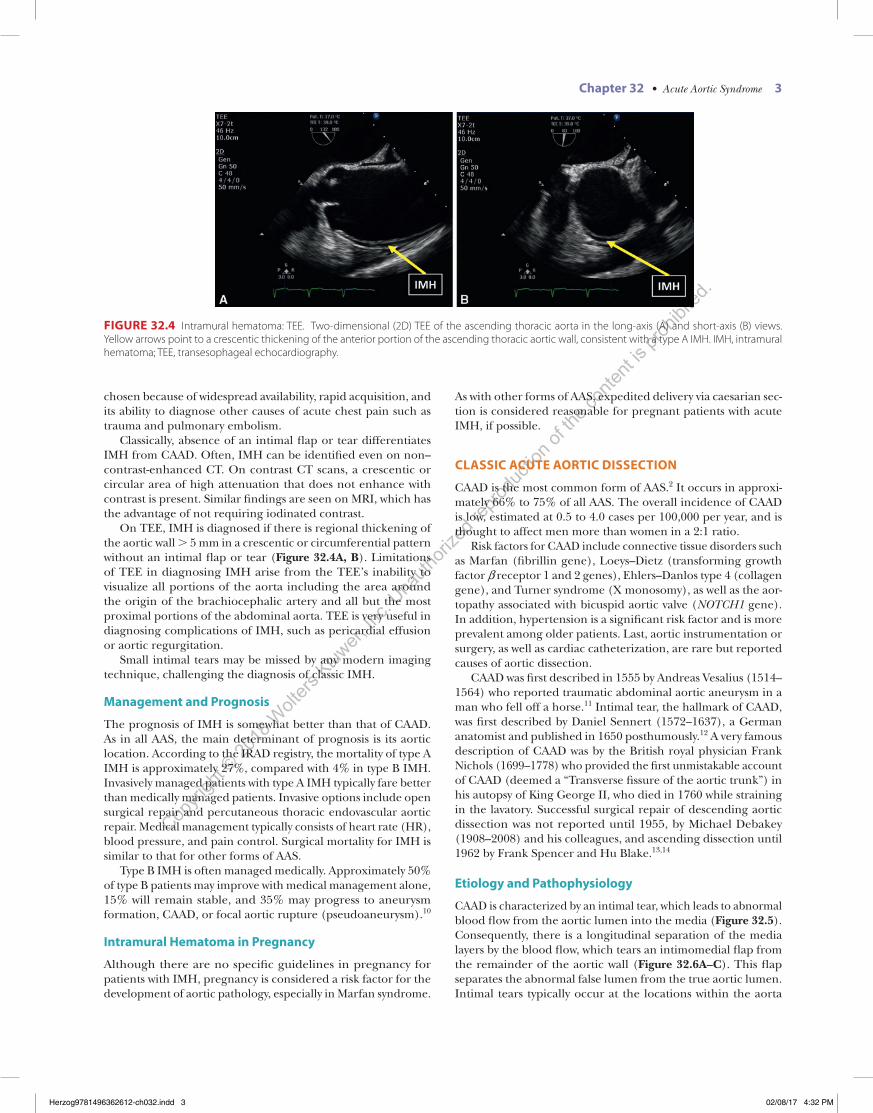
IMH is defined by crescentic or circumferential thickening of the media layer of the aortic wall. IMH is likely due to a ruptured vasa vasorum resulting in intramural bleeding but without a de-tectable intimal tear. It was first described in 1920 by the German pathologist Ernst Kruckenberg, who is also well known for his description of the so-called Kruckenberg tumors (transperito-neal ovarian metastases from stomach and colon cancers). On TEE, CT, or MRI, IMH is typically visualized as a crescentic or concentric thickening of the aortic wall > 5 mm (Figure 32.3).
AQ2
Alan F. VainribMuhamed Saric
Acute Aortic Syndrome
32
INTRODUCTION
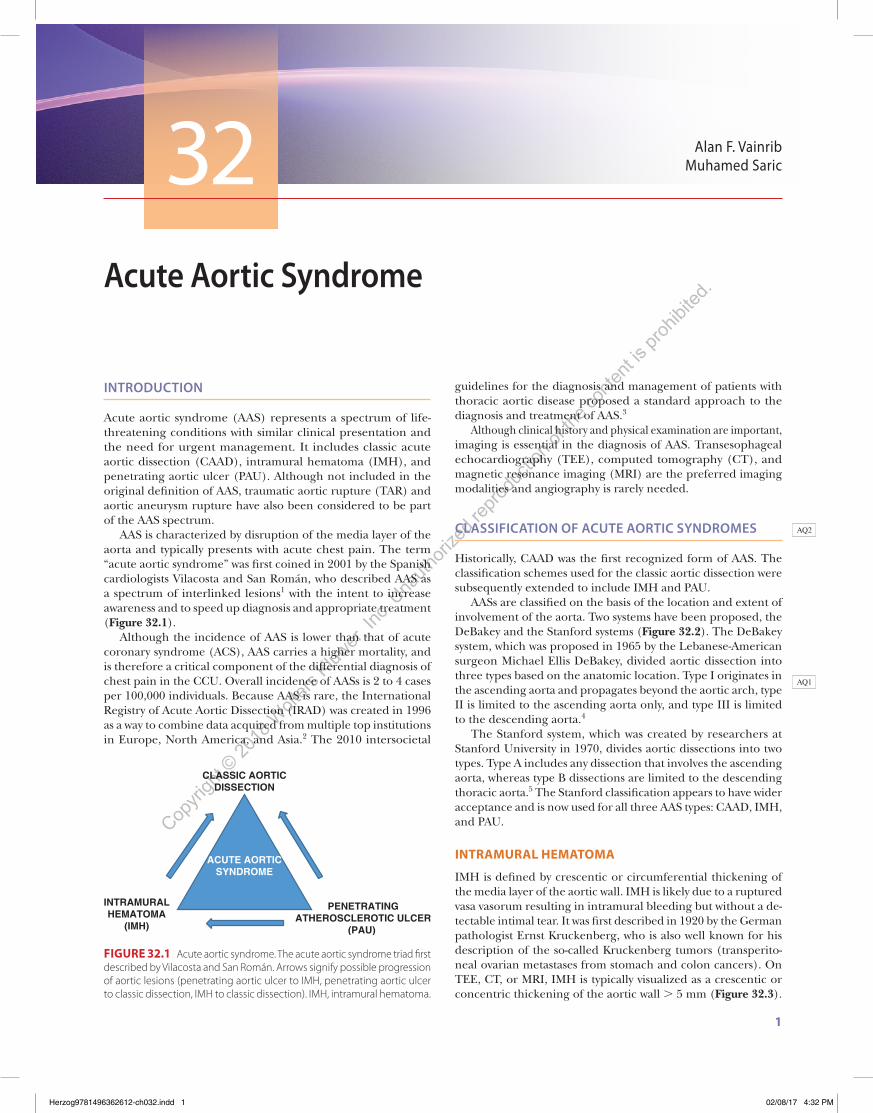
Acute aortic syndrome (AAS) represents a spectrum of life- threatening conditions with similar clinical presentation and the need for urgent management. It includes classic acute aortic dissection (CAAD), intramural hematoma (IMH), and penetrating aortic ulcer (PAU). Although not included in the original definition of AAS, traumatic aortic rupture (TAR) and aortic aneurysm rupture have also been considered to be part of the AAS spectrum.
AAS is characterized by disruption of the media layer of the aorta and typically presents with acute chest pain. The term “acute aortic syndrome” was first coined in 2001 by the Spanish cardiologists Vilacosta and San Román, who described AAS as a spectrum of interlinked lesions1 with the intent to increase awareness and to speed up diagnosis and appropriate treatment (Figure 32.1).
Although the incidence of AAS is lower than that of acute coronary syndrome (ACS), AAS carries a higher mortality, and is therefore a critical component of the differential diagnosis of chest pain in the CCU. Overall incidence of AASs is 2 to 4 cases per 100,000 individuals. Because AAS is rare, the International Registry of Acute Aortic Dissection (IRAD) was created in 1996 as a way to combine data acquired from multiple top institutions in Europe, North America, and Asia.2 The 2010 intersocietal
AQ1
ACUTE AORTICSYNDROME
CLASSIC AORTICDISSECTION
INTRAMURALHEMATOMA
(IMH)
PENETRATINGATHEROSCLEROTIC ULCER
(PAU)
FIGURE 32.1 Acute aortic syndrome. The acute aortic syndrome triad first described by Vilacosta and San Román. Arrows signify possible progression of aortic lesions (penetrating aortic ulcer to IMH, penetrating aortic ulcer to classic dissection, IMH to classic dissection). IMH, intramural hematoma.
Herzog9781496362612-ch032.indd 1 02/08/17 4:32 PM
Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
2 Section IV • Aortic, Pericardial, and Valvular Disease in the CCU
The natural history of IMH often includes progression to CAAD, which accounts for its high morbidity and mortality.
Etiology and Pathophysiology
IMH may account for up to 6% to 30% of all AAS, with a higher reported prevalence among the Korean and Japanese populations as compared with Western subjects.6 It is unclear whether this is
a true discrepancy in prevalence versus a reflection of differing classification, evaluation, or treatment practices. Often, IMH is diagnosed as such even though very small intimal tears indicative of limited aortic dissection may be present but missed by modern imaging modalities. This may overestimate the true prevalence of IMH as opposed to CAAD.
The characteristic feature of IMH is its location in the portion of the media closer to the adventitia, as opposed to CAAD which is typically located in the media closer to the intima. Although the most cited hypothesis of the pathophysiologic mechanism of IMH is rupture of the vasa vasorum, there is very little corroborating clinical or experimental evidence. Owing to the low incidence of IMH and the close association with CAAD, a definitive etiology still remains unclear.7
Clinical Manifestations
According to the IRAD experience, IMH typically presents with the symptoms of severe chest and back pain, similar to CAAD. However, IMH is less likely to present with manifestations of severe aortic regurgitation and pulse deficits.6 IMH is rarely stable. It may either progress to CAAD or regress spontaneously, and therefore serial imaging is crucial. Stanford type B lesions in the descending aorta are more common than type A lesions in the ascending aorta (60% vs 35% of all IMH, respectively). Cardiogenic shock may be present in 14% of patients, more typically with type A IMH.8 Pericardial effusion and tamponade may also be present, which are also more common in type A IMH. When compared with CAAD, type A IMH has a significantly higher risk of rupture (26% vs 8%, respectively).9 A widened mediastinum may be present on chest X-ray; however, this is neither sensitive nor specific to IMH.
Diagnosis
As with all types of AAS, rapid diagnosis is paramount in IMH. TEE, CT, and MRI are the preferred diagnostic tools. CT is often
Ann Thorac Surg. 1970 Sep;10(3):237-47.J. Thorac. Cardiovasc. Surg. 1965; 49:130-149.
DE BAKEY CLASSIFICATION STANFORD CLASSIFICATION
Type I Type II Type III Type A Type B
FIGURE 32.2 DeBakey and Stanford classifications. Left: DeBakey classification of aortic dissection. Type I includes the ascending and descending aorta, type II includes the ascending aorta only, and type III includes the descending thoracic aorta only. (DeBakey ME, Henly WS, Cooley DA, Morris GC Jr, Crawford ES, Beall AC Jr. Surgical management of dissecting aneurysms of the aorta. J Thorac Cardiovasc Surg. 1965;49:130-149.) Right: Stanford classification. Type A aortic dissection involves the ascending thoracic aorta, and type B involves the descending thoracic aorta only. All three AAS conditions; CAAD, IMH, and PAU use the Stanford classification. CAAD, classic acute aortic dissection; IMH, intramural hematoma; PAU, penetrating aortic ulcer. (Daily PO, Trueblood HW, Stinson EB, Wuerflein RD, Shumway NE. Management of acute aortic dissections. Ann Thorac Surg. 1970;10(3):237-247.)
FIGURE 32.3 Intramural hematoma: CT. CT of the chest shows the descending thoracic aorta. The crescentic-shaped lesion on the patient’s left signifies an IMH (dashed arrows). CT, computed tomography; IMH, intramural hematoma.
Herzog9781496362612-ch032.indd 2 02/08/17 4:32 PM
Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
Chapter 32 • Acute Aortic Syndrome 3
chosen because of widespread availability, rapid acquisition, and its ability to diagnose other causes of acute chest pain such as trauma and pulmonary embolism.
Classically, absence of an intimal flap or tear differentiates IMH from CAAD. Often, IMH can be identified even on non–contrast-enhanced CT. On contrast CT scans, a crescentic or circular area of high attenuation that does not enhance with contrast is present. Similar findings are seen on MRI, which has the advantage of not requiring iodinated contrast.
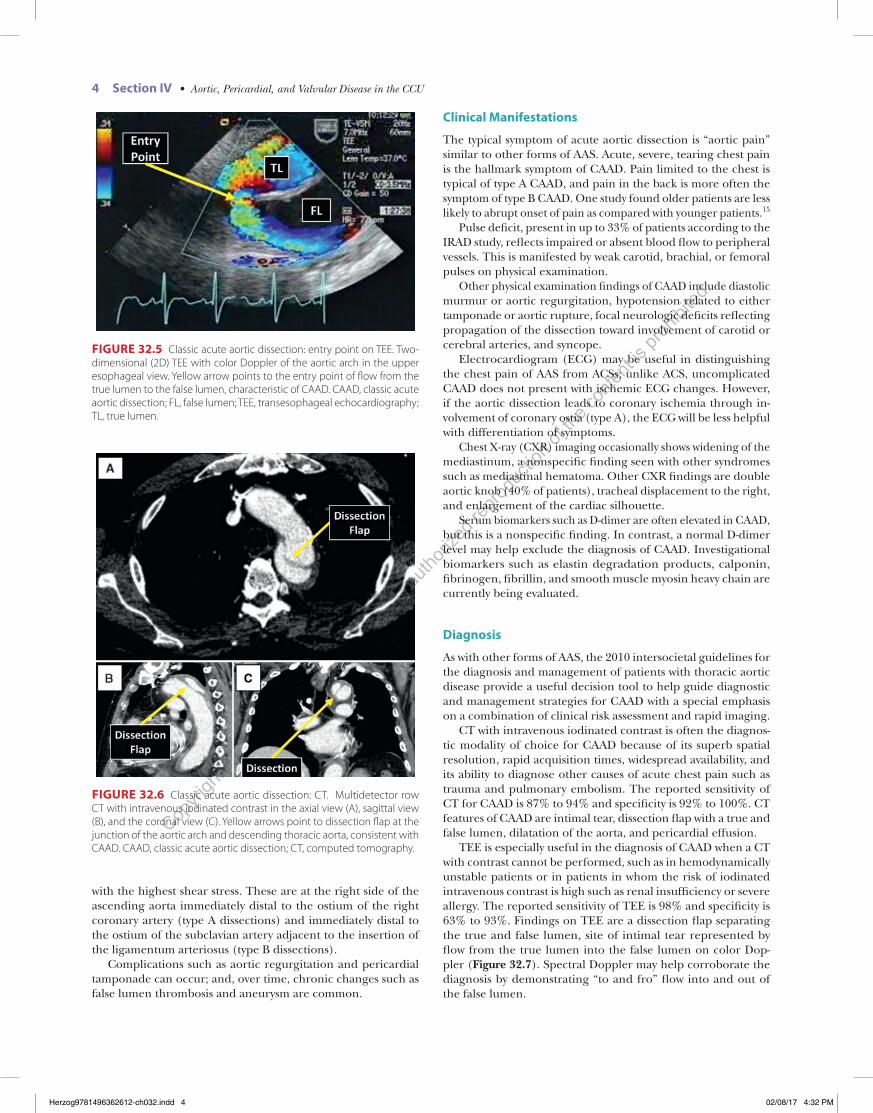
On TEE, IMH is diagnosed if there is regional thickening of the aortic wall > 5 mm in a crescentic or circumferential pattern without an intimal flap or tear (Figure 32.4A, B). Limitations of TEE in diagnosing IMH arise from the TEE’s inability to visualize all portions of the aorta including the area around the origin of the brachiocephalic artery and all but the most proximal portions of the abdominal aorta. TEE is very useful in diagnosing complications of IMH, such as pericardial effusion or aortic regurgitation.
Small intimal tears may be missed by any modern imaging technique, challenging the diagnosis of classic IMH.
Management and Prognosis
The prognosis of IMH is somewhat better than that of CAAD. As in all AAS, the main determinant of prognosis is its aortic location. According to the IRAD registry, the mortality of type A IMH is approximately 27%, compared with 4% in type B IMH. Invasively managed patients with type A IMH typically fare better than medically managed patients. Invasive options include open surgical repair and percutaneous thoracic endovascular aortic repair. Medical management typically consists of heart rate (HR), blood pressure, and pain control. Surgical mortality for IMH is similar to that for other forms of AAS.
Type B IMH is often managed medically. Approximately 50% of type B patients may improve with medical management alone, 15% will remain stable, and 35% may progress to aneurysm formation, CAAD, or focal aortic rupture (pseudoaneurysm).10
Intramural Hematoma in Pregnancy
Although there are no specific guidelines in pregnancy for patients with IMH, pregnancy is considered a risk factor for the development of aortic pathology, especially in Marfan syndrome.
As with other forms of AAS, expedited delivery via caesarian sec-tion is considered reasonable for pregnant patients with acute IMH, if possible.
CLASSIC ACUTE AORTIC DISSECTION
CAAD is the most common form of AAS.2 It occurs in approxi-mately 66% to 75% of all AAS. The overall incidence of CAAD is low, estimated at 0.5 to 4.0 cases per 100,000 per year, and is thought to affect men more than women in a 2:1 ratio.
Risk factors for CAAD include connective tissue disorders such as Marfan (fibrillin gene), Loeys–Dietz (transforming growth factor b receptor 1 and 2 genes), Ehlers–Danlos type 4 (collagen gene), and Turner syndrome (X monosomy), as well as the aor-topathy associated with bicuspid aortic valve (NOTCH1 gene). In addition, hypertension is a significant risk factor and is more prevalent among older patients. Last, aortic instrumentation or surgery, as well as cardiac catheterization, are rare but reported causes of aortic dissection.
CAAD was first described in 1555 by Andreas Vesalius (1514–1564) who reported traumatic abdominal aortic aneurysm in a man who fell off a horse.11 Intimal tear, the hallmark of CAAD, was first described by Daniel Sennert (1572–1637), a German anatomist and published in 1650 posthumously.12 A very famous description of CAAD was by the British royal physician Frank Nichols (1699–1778) who provided the first unmistakable account of CAAD (deemed a “Transverse fissure of the aortic trunk”) in his autopsy of King George II, who died in 1760 while straining in the lavatory. Successful surgical repair of descending aortic dissection was not reported until 1955, by Michael Debakey (1908–2008) and his colleagues, and ascending dissection until 1962 by Frank Spencer and Hu Blake.13,14
Etiology and Pathophysiology
CAAD is characterized by an intimal tear, which leads to abnormal blood flow from the aortic lumen into the media (Figure 32.5). Consequently, there is a longitudinal separation of the media layers by the blood flow, which tears an intimomedial flap from the remainder of the aortic wall (Figure 32.6A–C). This flap separates the abnormal false lumen from the true aortic lumen. Intimal tears typically occur at the locations within the aorta
FIGURE 32.4 Intramural hematoma: TEE. Two-dimensional (2D) TEE of the ascending thoracic aorta in the long-axis (A) and short-axis (B) views. Yellow arrows point to a crescentic thickening of the anterior portion of the ascending thoracic aortic wall, consistent with a type A IMH. IMH, intramural hematoma; TEE, transesophageal echocardiography.
Herzog9781496362612-ch032.indd 3 02/08/17 4:32 PM
Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
4 Section IV • Aortic, Pericardial, and Valvular Disease in the CCU
Clinical Manifestations
The typical symptom of acute aortic dissection is “aortic pain” similar to other forms of AAS. Acute, severe, tearing chest pain is the hallmark symptom of CAAD. Pain limited to the chest is typical of type A CAAD, and pain in the back is more often the symptom of type B CAAD. One study found older patients are less likely to abrupt onset of pain as compared with younger patients.15
Pulse deficit, present in up to 33% of patients according to the IRAD study, reflects impaired or absent blood flow to peripheral vessels. This is manifested by weak carotid, brachial, or femoral pulses on physical examination.
Other physical examination findings of CAAD include diastolic murmur or aortic regurgitation, hypotension related to either tamponade or aortic rupture, focal neurologic deficits reflecting propagation of the dissection toward involvement of carotid or cerebral arteries, and syncope.
Electrocardiogram (ECG) may be useful in distinguishing the chest pain of AAS from ACSs; unlike ACS, uncomplicated CAAD does not present with ischemic ECG changes. However, if the aortic dissection leads to coronary ischemia through in-volvement of coronary ostia (type A), the ECG will be less helpful with differentiation of symptoms.
Chest X-ray (CXR) imaging occasionally shows widening of the mediastinum, a nonspecific finding seen with other syndromes such as mediastinal hematoma. Other CXR findings are double aortic knob (40% of patients), tracheal displacement to the right, and enlargement of the cardiac silhouette.
Serum biomarkers such as D-dimer are often elevated in CAAD, but this is a nonspecific finding. In contrast, a normal D-dimer level may help exclude the diagnosis of CAAD. Investigational biomarkers such as elastin degradation products, calponin, fibrinogen, fibrillin, and smooth muscle myosin heavy chain are currently being evaluated.
Diagnosis
As with other forms of AAS, the 2010 intersocietal guidelines for the diagnosis and management of patients with thoracic aortic disease provide a useful decision tool to help guide diagnostic and management strategies for CAAD with a special emphasis on a combination of clinical risk assessment and rapid imaging.
CT with intravenous iodinated contrast is often the diagnos-tic modality of choice for CAAD because of its superb spatial resolution, rapid acquisition times, widespread availability, and its ability to diagnose other causes of acute chest pain such as trauma and pulmonary embolism. The reported sensitivity of CT for CAAD is 87% to 94% and specificity is 92% to 100%. CT features of CAAD are intimal tear, dissection flap with a true and false lumen, dilatation of the aorta, and pericardial effusion.
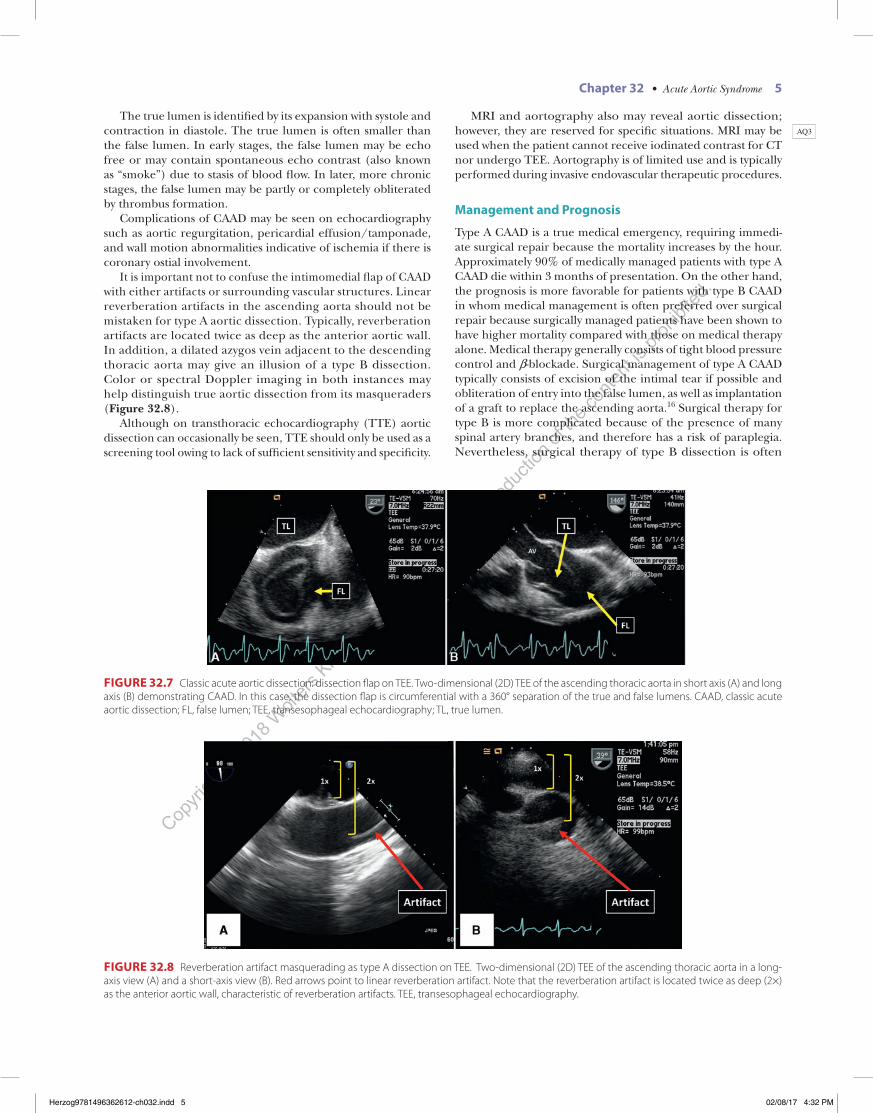
TEE is especially useful in the diagnosis of CAAD when a CT with contrast cannot be performed, such as in hemodynamically unstable patients or in patients in whom the risk of iodinated intravenous contrast is high such as renal insufficiency or severe allergy. The reported sensitivity of TEE is 98% and specificity is 63% to 93%. Findings on TEE are a dissection flap separating the true and false lumen, site of intimal tear represented by flow from the true lumen into the false lumen on color Dop-pler (Figure 32.7). Spectral Doppler may help corroborate the diagnosis by demonstrating “to and fro” flow into and out of the false lumen.
with the highest shear stress. These are at the right side of the ascending aorta immediately distal to the ostium of the right coronary artery (type A dissections) and immediately distal to the ostium of the subclavian artery adjacent to the insertion of the ligamentum arteriosus (type B dissections).
Complications such as aortic regurgitation and pericardial tamponade can occur; and, over time, chronic changes such as false lumen thrombosis and aneurysm are common.
FIGURE 32.5 Classic acute aortic dissection: entry point on TEE. Two- dimensional (2D) TEE with color Doppler of the aortic arch in the upper esophageal view. Yellow arrow points to the entry point of flow from the true lumen to the false lumen, characteristic of CAAD. CAAD, classic acute aortic dissection; FL, false lumen; TEE, transesophageal echocardiography; TL, true lumen.
FIGURE 32.6 Classic acute aortic dissection: CT. Multidetector row CT with intravenous iodinated contrast in the axial view (A), sagittal view (B), and the coronal view (C). Yellow arrows point to dissection flap at the junction of the aortic arch and descending thoracic aorta, consistent with CAAD. CAAD, classic acute aortic dissection; CT, computed tomography.
Herzog9781496362612-ch032.indd 4 02/08/17 4:32 PM
Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
Chapter 32 • Acute Aortic Syndrome 5
MRI and aortography also may reveal aortic dissection; however, they are reserved for specific situations. MRI may be used when the patient cannot receive iodinated contrast for CT nor undergo TEE. Aortography is of limited use and is typically performed during invasive endovascular therapeutic procedures.
Management and Prognosis
Type A CAAD is a true medical emergency, requiring immedi-ate surgical repair because the mortality increases by the hour. Approximately 90% of medically managed patients with type A CAAD die within 3 months of presentation. On the other hand, the prognosis is more favorable for patients with type B CAAD in whom medical management is often preferred over surgical repair because surgically managed patients have been shown to have higher mortality compared with those on medical therapy alone. Medical therapy generally consists of tight blood pressure control and b-blockade. Surgical management of type A CAAD typically consists of excision of the intimal tear if possible and obliteration of entry into the false lumen, as well as implantation of a graft to replace the ascending aorta.16 Surgical therapy for type B is more complicated because of the presence of many spinal artery branches, and therefore has a risk of paraplegia. Nevertheless, surgical therapy of type B dissection is often
The true lumen is identified by its expansion with systole and contraction in diastole. The true lumen is often smaller than the false lumen. In early stages, the false lumen may be echo free or may contain spontaneous echo contrast (also known as “smoke”) due to stasis of blood flow. In later, more chronic stages, the false lumen may be partly or completely obliterated by thrombus formation.
Complications of CAAD may be seen on echocardiography such as aortic regurgitation, pericardial effusion/tamponade, and wall motion abnormalities indicative of ischemia if there is coronary ostial involvement.
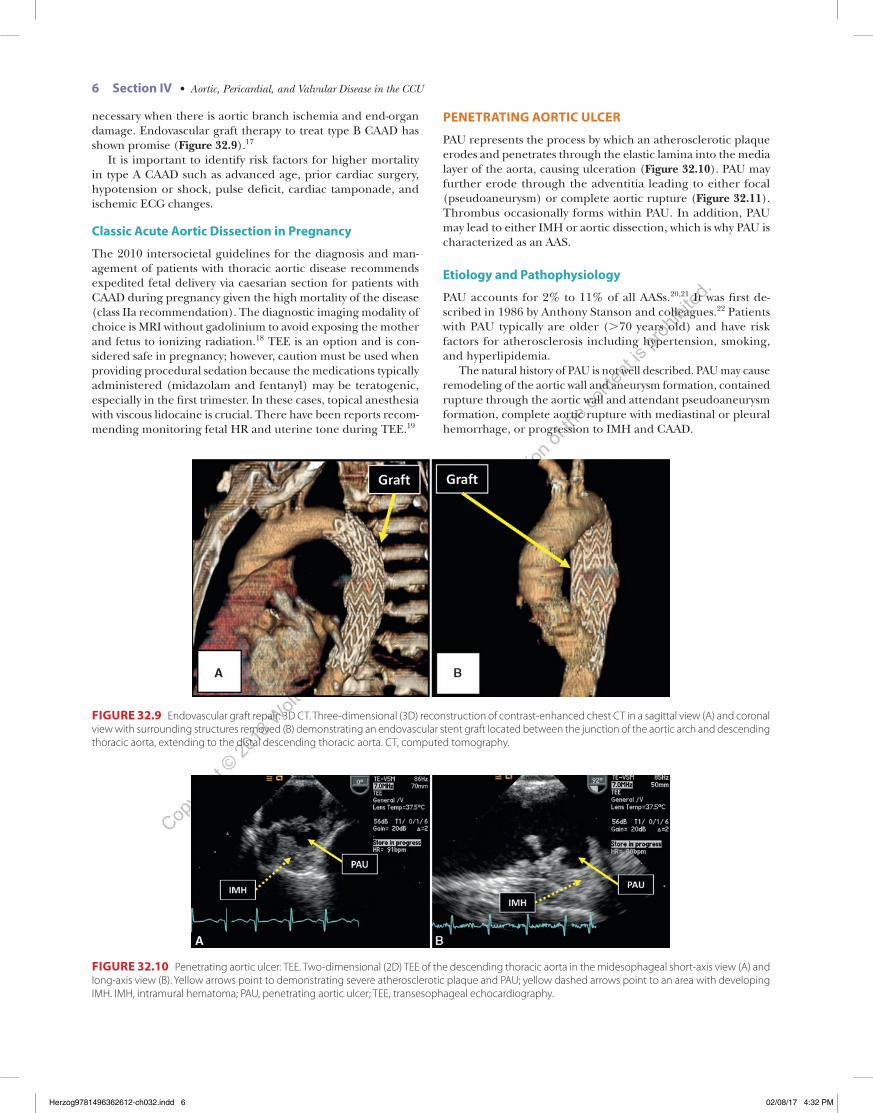
It is important not to confuse the intimomedial flap of CAAD with either artifacts or surrounding vascular structures. Linear reverberation artifacts in the ascending aorta should not be mistaken for type A aortic dissection. Typically, reverberation artifacts are located twice as deep as the anterior aortic wall. In addition, a dilated azygos vein adjacent to the descending thoracic aorta may give an illusion of a type B dissection. Color or spectral Doppler imaging in both instances may help distinguish true aortic dissection from its masqueraders (Figure 32.8).
Although on transthoracic echocardiography (TTE) aortic dissection can occasionally be seen, TTE should only be used as a screening tool owing to lack of sufficient sensitivity and specificity.
AQ3
FIGURE 32.7 Classic acute aortic dissection: dissection flap on TEE. Two-dimensional (2D) TEE of the ascending thoracic aorta in short axis (A) and long axis (B) demonstrating CAAD. In this case, the dissection flap is circumferential with a 360° separation of the true and false lumens. CAAD, classic acute aortic dissection; FL, false lumen; TEE, transesophageal echocardiography; TL, true lumen.
FIGURE 32.8 Reverberation artifact masquerading as type A dissection on TEE. Two-dimensional (2D) TEE of the ascending thoracic aorta in a long-axis view (A) and a short-axis view (B). Red arrows point to linear reverberation artifact. Note that the reverberation artifact is located twice as deep (2×) as the anterior aortic wall, characteristic of reverberation artifacts. TEE, transesophageal echocardiography.
Herzog9781496362612-ch032.indd 5 02/08/17 4:32 PM
Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
6 Section IV • Aortic, Pericardial, and Valvular Disease in the CCU
PENETRATING AORTIC ULCER
PAU represents the process by which an atherosclerotic plaque erodes and penetrates through the elastic lamina into the media layer of the aorta, causing ulceration (Figure 32.10). PAU may further erode through the adventitia leading to either focal (pseudoaneurysm) or complete aortic rupture (Figure 32.11). Thrombus occasionally forms within PAU. In addition, PAU may lead to either IMH or aortic dissection, which is why PAU is characterized as an AAS.
Etiology and Pathophysiology
PAU accounts for 2% to 11% of all AASs.20,21 It was first de-scribed in 1986 by Anthony Stanson and colleagues.22 Patients with PAU typically are older (>70 years old) and have risk factors for atherosclerosis including hypertension, smoking, and hyperlipidemia.
The natural history of PAU is not well described. PAU may cause remodeling of the aortic wall and aneurysm formation, contained rupture through the aortic wall and attendant pseudoaneurysm formation, complete aortic rupture with mediastinal or pleural hemorrhage, or progression to IMH and CAAD.
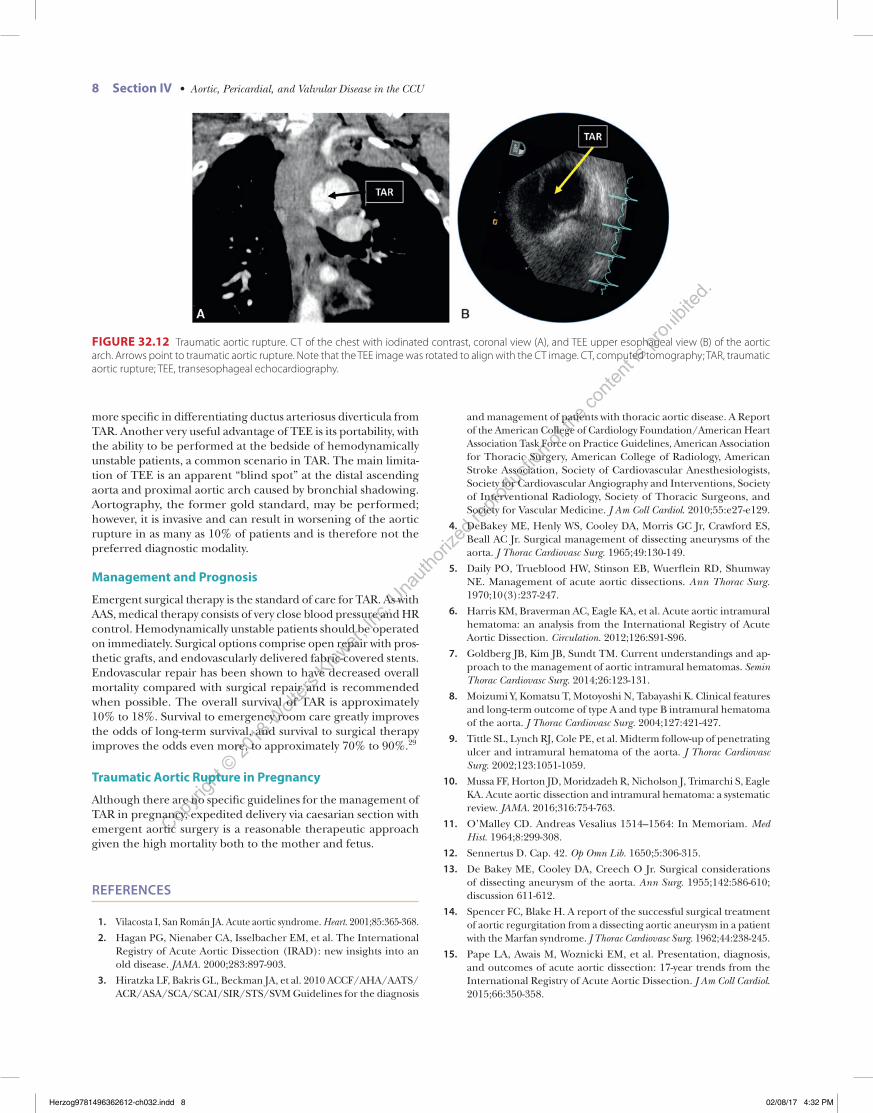
necessary when there is aortic branch ischemia and end-organ damage. Endovascular graft therapy to treat type B CAAD has shown promise (Figure 32.9).17
It is important to identify risk factors for higher mortality in type A CAAD such as advanced age, prior cardiac surgery, hypotension or shock, pulse deficit, cardiac tamponade, and ischemic ECG changes.
Classic Acute Aortic Dissection in Pregnancy
The 2010 intersocietal guidelines for the diagnosis and man-agement of patients with thoracic aortic disease recommends expedited fetal delivery via caesarian section for patients with CAAD during pregnancy given the high mortality of the disease (class IIa recommendation). The diagnostic imaging modality of choice is MRI without gadolinium to avoid exposing the mother and fetus to ionizing radiation.18 TEE is an option and is con-sidered safe in pregnancy; however, caution must be used when providing procedural sedation because the medications typically administered (midazolam and fentanyl) may be teratogenic, especially in the first trimester. In these cases, topical anesthesia with viscous lidocaine is crucial. There have been reports recom-mending monitoring fetal HR and uterine tone during TEE.19
FIGURE 32.9 Endovascular graft repair: 3D CT. Three-dimensional (3D) reconstruction of contrast-enhanced chest CT in a sagittal view (A) and coronal view with surrounding structures removed (B) demonstrating an endovascular stent graft located between the junction of the aortic arch and descending thoracic aorta, extending to the distal descending thoracic aorta. CT, computed tomography.
FIGURE 32.10 Penetrating aortic ulcer: TEE. Two-dimensional (2D) TEE of the descending thoracic aorta in the midesophageal short-axis view (A) and long-axis view (B). Yellow arrows point to demonstrating severe atherosclerotic plaque and PAU; yellow dashed arrows point to an area with developing IMH. IMH, intramural hematoma; PAU, penetrating aortic ulcer; TEE, transesophageal echocardiography.
Herzog9781496362612-ch032.indd 6 02/08/17 4:32 PM

Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
Chapter 32 • Acute Aortic Syndrome 7
TRAUMATIC AORTIC RUPTURE
Although TAR is not considered to be a part of the original AAS triad, it is a life-threatening aortic emergency with only a 15% to 20% survival.24 TAR is typically caused by deceleration injuries sustained in motor vehicle accidents (MVAs) and falls greater than 3 m.25 It is the second leading cause of death after blunt trauma, occurring in approximately 1.5% to 1.9% cases.26
Etiology and Pathophysiology
The most common site of injury in TAR is at the aortic isthmus, immediately distal to the left subclavian artery at the site of the ductus arteriosus. This location is considered to be the most vulnerable to torsional and shear forces because it is thought to be a transition zone between the semi-mobile aortic arch and the fixed descending thoracic aorta. Other possible sites of injury are the transverse arch, ascending aorta, and descending aorta proximal to the diaphragm.27 Typically, the intima and medial layers rupture first, followed by rupture of the adventitia after an unpredictable interval of time.28 Multiple tears may occur.
Clinical Manifestations
There is no specific symptom associated with TAR. Chest pain in the patient with trauma should, however, raise suspicion, especially in the presence of the “seat belt sign” (seat belt imprint on the surface of the skin). Pulse deficit and murmur of aortic regurgi-tation may be present. CXR may show a widened mediastinum, obscured aortic knob, and left hemothorax.
Diagnosis
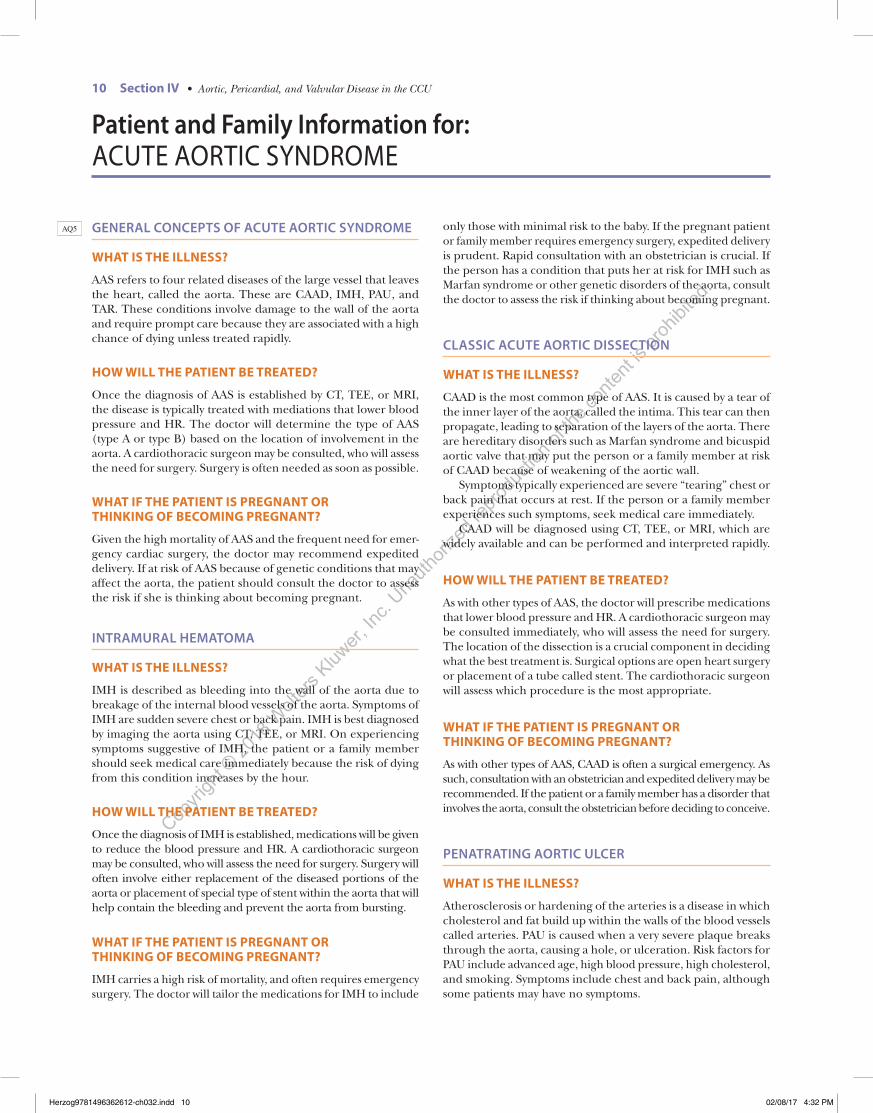
TAR is best diagnosed using either contrast-enhanced CT or TEE because both modalities have high diagnostic sensitivity and spec-ificity (Figure 32.12). Findings seen on CT include intimal flap, periaortic hematoma, luminal filling defects, pseudoaneurysm, or active extravasation of contrast from the aorta. It is important to distinguish TAR from a ductus arteriosus diverticulum, which is helped by the improved special and temporal resolution of modern multidetector row CT scanners. However, TEE may be
Clinical Manifestations
Symptoms of PAU are similar to that of other AASs. The pain associated with PAU is variable, and dependent on the location of the ulceration. Type A PAU typically presents with chest pain and type B PAU is more likely to present with back pain. Unlike IMH or CAAD, there have been reports of PAU as an incidental finding in asymptomatic patients.
Diagnosis
The diagnosis of PAU is primarily made by CT, TEE, and MRI. Aortography is not typically used for PAU because of lack of direct visualization of the aortic wall. All three techniques are able to image atherosclerotic changes, ulceration, and complications such as pseudoaneurysm, rupture, and medi-astinal and pleural hemorrhage. Identification of an ulcer crater distinguishes PAU from IMH with intraparietal. PAU lesions are typically focal as opposed to those of CAAD and IMH, which are more extensive.
Management and Prognosis
The natural history of PAU is poorly understood. On one hand, PAU is considered to be a surgical emergency with risk similar to or worse than other forms of AAS. On the other, reports have described the progression of PAU as slow, with a low prevalence of life-threatening complications.23 There is therefore equipoise regarding the optimal medical versus surgical treatment strategies. Nevertheless, surgical management of PAU with aortic grafting is considered appropriate in the presence of aortic rupture, persistent or recurrent pain, hemodynamic instability, or rapidly expanding aortic diameter.
Penetrating Aortic Ulcer in Pregnancy
Because PAU is a disease that primarily affects older people (>70 years of age), it is highly unlikely that it will occur during pregnancy. There is therefore no available guideline to direct optimal management.
AQ4
FIGURE 32.11 Penetrating aortic ulcer with rupture/pseudoaneurysm, CT. CT with intravenous iodinated contrast of the chest. Arrows point to PAU with aortic rupture and pseudoaneurysm of anterior portion of the proximal descending thoracic aorta. CT, computed tomography; PsA, pseudoaneurysm.
AQ6
Herzog9781496362612-ch032.indd 7 02/08/17 4:32 PM
Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
8 Section IV • Aortic, Pericardial, and Valvular Disease in the CCU
and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. J Am Coll Cardiol. 2010;55:e27-e129.
4. DeBakey ME, Henly WS, Cooley DA, Morris GC Jr, Crawford ES, Beall AC Jr. Surgical management of dissecting aneurysms of the aorta. J Thorac Cardiovasc Surg. 1965;49:130-149.
5. Daily PO, Trueblood HW, Stinson EB, Wuerflein RD, Shumway NE. Management of acute aortic dissections. Ann Thorac Surg. 1970;10(3):237-247.
6. Harris KM, Braverman AC, Eagle KA, et al. Acute aortic intramural hematoma: an analysis from the International Registry of Acute Aortic Dissection. Circulation. 2012;126:S91-S96.
7. Goldberg JB, Kim JB, Sundt TM. Current understandings and ap-proach to the management of aortic intramural hematomas. Semin Thorac Cardiovasc Surg. 2014;26:123-131.
8. Moizumi Y, Komatsu T, Motoyoshi N, Tabayashi K. Clinical features and long-term outcome of type A and type B intramural hematoma of the aorta. J Thorac Cardiovasc Surg. 2004;127:421-427.
9. Tittle SL, Lynch RJ, Cole PE, et al. Midterm follow-up of penetrating ulcer and intramural hematoma of the aorta. J Thorac Cardiovasc Surg. 2002;123:1051-1059.
10. Mussa FF, Horton JD, Moridzadeh R, Nicholson J, Trimarchi S, Eagle KA. Acute aortic dissection and intramural hematoma: a systematic review. JAMA. 2016;316:754-763.
11. O’Malley CD. Andreas Vesalius 1514–1564: In Memoriam. Med Hist. 1964;8:299-308.
12. Sennertus D. Cap. 42. Op Omn Lib. 1650;5:306-315.
13. De Bakey ME, Cooley DA, Creech O Jr. Surgical considerations of dissecting aneurysm of the aorta. Ann Surg. 1955;142:586-610; discussion 611-612.
14. Spencer FC, Blake H. A report of the successful surgical treatment of aortic regurgitation from a dissecting aortic aneurysm in a patient with the Marfan syndrome. J Thorac Cardiovasc Surg. 1962;44:238-245.
15. Pape LA, Awais M, Woznicki EM, et al. Presentation, diagnosis, and outcomes of acute aortic dissection: 17-year trends from the International Registry of Acute Aortic Dissection. J Am Coll Cardiol. 2015;66:350-358.
more specific in differentiating ductus arteriosus diverticula from TAR. Another very useful advantage of TEE is its portability, with the ability to be performed at the bedside of hemodynamically unstable patients, a common scenario in TAR. The main limita-tion of TEE is an apparent “blind spot” at the distal ascending aorta and proximal aortic arch caused by bronchial shadowing. Aortography, the former gold standard, may be performed; however, it is invasive and can result in worsening of the aortic rupture in as many as 10% of patients and is therefore not the preferred diagnostic modality.
Management and Prognosis
Emergent surgical therapy is the standard of care for TAR. As with AAS, medical therapy consists of very close blood pressure and HR control. Hemodynamically unstable patients should be operated on immediately. Surgical options comprise open repair with pros-thetic grafts, and endovascularly delivered fabric-covered stents. Endovascular repair has been shown to have decreased overall mortality compared with surgical repair and is recommended when possible. The overall survival of TAR is approximately 10% to 18%. Survival to emergency room care greatly improves the odds of long-term survival, and survival to surgical therapy improves the odds even more, to approximately 70% to 90%.29
Traumatic Aortic Rupture in Pregnancy
Although there are no specific guidelines for the management of TAR in pregnancy, expedited delivery via caesarian section with emergent aortic surgery is a reasonable therapeutic approach given the high mortality both to the mother and fetus.
REFERENCES
1. Vilacosta I, San Román JA. Acute aortic syndrome. Heart. 2001;85:365-368.
2. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283:897-903.
3. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis
FIGURE 32.12 Traumatic aortic rupture. CT of the chest with iodinated contrast, coronal view (A), and TEE upper esophageal view (B) of the aortic arch. Arrows point to traumatic aortic rupture. Note that the TEE image was rotated to align with the CT image. CT, computed tomography; TAR, traumatic aortic rupture; TEE, transesophageal echocardiography.
Herzog9781496362612-ch032.indd 8 02/08/17 4:32 PM

Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
Chapter 32 • Acute Aortic Syndrome 9
16. Braverman AC. Acute aortic dissection: clinician update. Circulation. 2010;122:184-188.
17. Nienaber CA, Kische S, Rousseau H, et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ Cardiovasc Interv. 2013;6:407-416.
18. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular An-giography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Catheter Cardiovasc Interv. 2010;76:E43-E86.
19. Stoddard MF, Longaker RA, Vuocolo LM, Dawkins PR. Transe-sophageal echocardiography in the pregnant patient. Am Heart J. 1992;124:785-787.
20. Hirst AE Jr, Johns VJ Jr, Kime SW Jr. Dissecting aneurysm of the aorta: a review of 505 cases. Medicine. 1958;37:217-279.
21. Eggebrecht H, Plicht B, Kahlert P, Erbel R. Intramural hematoma and penetrating ulcers: indications to endovascular treatment. Eur J Vasc Endovasc Surg. 2009;38:659-665.
22. Stanson AW, Kazmier FJ, Hollier LH, et al. Penetrating atherosclerotic ulcers of the thoracic aorta: natural history and clinicopathologic correlations. Ann Vasc Surg. 1986;1:15-23.
23. Hayashi H, Matsuoka Y, Sakamoto I, et al. Penetrating atheroscle-rotic ulcer of the aorta: imaging features and disease concept. Radiographics. 2000;20:995-1005.
24. Fabian TC, Richardson JD, Croce MA, et al. Prospective study of blunt aortic injury: multicenter trial of the American Association for the Surgery of Trauma. J Trauma. 1997;42:374-380; discussion 380-383.
25. Sanchez-Ross M, Anis A, Walia J, et al. Aortic rupture: comparison of three imaging modalities. Emerg Radiol. 2006;13:31-33.
26. Dyer DS, Moore EE, Ilke DN, et al. Thoracic aortic injury: how pre-dictive is mechanism and is chest computed tomography a reliable screening tool? A prospective study of 1,561 patients. J Trauma. 2000;48:673-682; discussion 682-683.
27. Sevitt S. The mechanisms of traumatic rupture of the thoracic aorta. Br J Surg. 1977;64:166-173.
28. Nikolic S, Atanasijevic T, Mihailovic Z, Babic D, Popovic-Loncar T. Mechanisms of aortic blunt rupture in fatally injured front-seat passengers in frontal car collisions: an autopsy study. Am J Forensic Med Pathol. 2006;27:292-295.
29. Smith RS, Chang FC. Traumatic rupture of the aorta: still a lethal injury. Am J Surg. 1986;152:660-663.
Herzog9781496362612-ch032.indd 9 02/08/17 4:32 PM
Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
10 Section IV • Aortic, Pericardial, and Valvular Disease in the CCU
only those with minimal risk to the baby. If the pregnant patient or family member requires emergency surgery, expedited delivery is prudent. Rapid consultation with an obstetrician is crucial. If the person has a condition that puts her at risk for IMH such as Marfan syndrome or other genetic disorders of the aorta, consult the doctor to assess the risk if thinking about becoming pregnant.
CLASSIC ACUTE AORTIC DISSECTION
WHAT IS THE ILLNESS?
CAAD is the most common type of AAS. It is caused by a tear of the inner layer of the aorta, called the intima. This tear can then propagate, leading to separation of the layers of the aorta. There are hereditary disorders such as Marfan syndrome and bicuspid aortic valve that may put the person or a family member at risk of CAAD because of weakening of the aortic wall.
Symptoms typically experienced are severe “tearing” chest or back pain that occurs at rest. If the person or a family member experiences such symptoms, seek medical care immediately.
CAAD will be diagnosed using CT, TEE, or MRI, which are widely available and can be performed and interpreted rapidly.
HOW WILL THE PATIENT BE TREATED?
As with other types of AAS, the doctor will prescribe medications that lower blood pressure and HR. A cardiothoracic surgeon may be consulted immediately, who will assess the need for surgery. The location of the dissection is a crucial component in deciding what the best treatment is. Surgical options are open heart surgery or placement of a tube called stent. The cardiothoracic surgeon will assess which procedure is the most appropriate.
WHAT IF THE PATIENT IS PREGNANT OR THINKING OF BECOMING PREGNANT?
As with other types of AAS, CAAD is often a surgical emergency. As such, consultation with an obstetrician and expedited delivery may be recommended. If the patient or a family member has a disorder that involves the aorta, consult the obstetrician before deciding to conceive.
PENATRATING AORTIC ULCER
WHAT IS THE ILLNESS?
Atherosclerosis or hardening of the arteries is a disease in which cholesterol and fat build up within the walls of the blood vessels called arteries. PAU is caused when a very severe plaque breaks through the aorta, causing a hole, or ulceration. Risk factors for PAU include advanced age, high blood pressure, high cholesterol, and smoking. Symptoms include chest and back pain, although some patients may have no symptoms.
AQ5 GENERAL CONCEPTS OF ACUTE AORTIC SYNDROME
WHAT IS THE ILLNESS?
AAS refers to four related diseases of the large vessel that leaves the heart, called the aorta. These are CAAD, IMH, PAU, and TAR. These conditions involve damage to the wall of the aorta and require prompt care because they are associated with a high chance of dying unless treated rapidly.
HOW WILL THE PATIENT BE TREATED?
Once the diagnosis of AAS is established by CT, TEE, or MRI, the disease is typically treated with mediations that lower blood pressure and HR. The doctor will determine the type of AAS (type A or type B) based on the location of involvement in the aorta. A cardiothoracic surgeon may be consulted, who will assess the need for surgery. Surgery is often needed as soon as possible.
WHAT IF THE PATIENT IS PREGNANT OR THINKING OF BECOMING PREGNANT?
Given the high mortality of AAS and the frequent need for emer-gency cardiac surgery, the doctor may recommend expedited delivery. If at risk of AAS because of genetic conditions that may affect the aorta, the patient should consult the doctor to assess the risk if she is thinking about becoming pregnant.
INTRAMURAL HEMATOMA
WHAT IS THE ILLNESS?
IMH is described as bleeding into the wall of the aorta due to breakage of the internal blood vessels of the aorta. Symptoms of IMH are sudden severe chest or back pain. IMH is best diagnosed by imaging the aorta using CT, TEE, or MRI. On experiencing symptoms suggestive of IMH, the patient or a family member should seek medical care immediately because the risk of dying from this condition increases by the hour.
HOW WILL THE PATIENT BE TREATED?
Once the diagnosis of IMH is established, medications will be given to reduce the blood pressure and HR. A cardiothoracic surgeon may be consulted, who will assess the need for surgery. Surgery will often involve either replacement of the diseased portions of the aorta or placement of special type of stent within the aorta that will help contain the bleeding and prevent the aorta from bursting.
WHAT IF THE PATIENT IS PREGNANT OR THINKING OF BECOMING PREGNANT?
IMH carries a high risk of mortality, and often requires emergency surgery. The doctor will tailor the medications for IMH to include
Patient and Family Information for: ACUTE AORTIC SYNDROME
Herzog9781496362612-ch032.indd 10 02/08/17 4:32 PM
Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
Chapter 32 • Acute Aortic Syndrome 11
TAR is a very dangerous condition and requires prompt medical attention. A mark across the skin of the chest due to a seat belt often is present when TAR is caused by an MVA. TAR is diagnosed using CT and TEE.
HOW WILL THE PATIENT BE TREATED?
Emergency surgery is the standard of care for TAR. The doctor may prescribe medications to lower HR and blood pressure if necessary; however, a cardiothoracic surgeon may be consulted as soon as possible. Treatment typically requires open heart surgery.
WHAT IF THE PATIENT IS PREGNANT OR THINKING OF BECOMING PREGNANT?
Because TAR is a surgical emergency, consultation with an obstetrician for early delivery is crucial.
The surgeon may recommend delivery by cesarean section at the time of surgery to repair the broken aorta.
Along with other forms of AAS, PAU is diagnosed by CT, TEE, or MRI.
HOW WILL THE PATIENT BE TREATED?
The doctor may recommend close monitoring with imaging studies, medications, or surgery.
WHAT IF THE PATIENT IS PREGNANT OR THINKING OF BECOMING PREGNANT?
PAU is typically a disease that affects older people (more than 70 years of age). It is highly unlikely that it will occur during pregnancy.
TRAUMATIC AORTIC RUPTURE
WHAT IS THE ILLNESS?
TAR describes tearing of the aorta after a chest injury. It most commonly occurs after MVAs and bad falls.
Herzog9781496362612-ch032.indd 11 02/08/17 4:32 PM
Copyri
ght ©
2018
Wolt
ers K
luwer,
Inc.
Unauth
orize
d rep
roduc
tion o
f the c
onten
t is pr
ohibi
ted.
Query LogJob ID: Herzog_165298Chapter No: 32
Query No Query Remarks
AQ1 Please clarify if CCU should be spelt coronary care unit or cardiac care unit.
AQ2 Please check whether the hierarchy of section heading levels are appropriate.
AQ3 Please note that this sentence “The true lumen is often smaller than the false lumen, and the false lumen” is incomplete. We have deleted the portion “and the false lumen.” Kindly confirm if the edit is correct.
AQ4 Please note that this sentence “Identification of an ulcer crater...intraparietal” is incomplete. Kindly provide the missing word/s.
AQ5 Please confirm whether the edit made to the sentence “If you or your family requires. . .is prudent” retains the intended meaning.
AQ6 Would you like to add descriptions for part labels A and B in the legend of Figure 32.11?
Herzog9781496362612-ch032.indd 12 02/08/17 4:32 PM





























