Embed Size (px)
Citation preview

tap_705 540..548
Acute and Subacute Effect of Rheopheresis onMicrovascular Endothelial Function in Patients Suffering
From Age-related Macular Degeneration
Marco Rossi,1 Rodolfo Puccini,2 Maria Chiara Romagnoli,3 Cinzia Di Maria,1
Paola Mattei,2 Matteo Bernini,2 Claudio Marconcini,4 and Gino Santoro1
1Department of Internal Medicine, University of Pisa, 2Nephrology Unit, Kidney Transplant and Dialysis(Section of Apheresis Treatment), and 3Ophthalmic Surgery Unit, Pisa Hospital, Pisa, and 4Ophthalmology
Unit, Pontedera Hospital, Pontedera, Italy
Abstract: This study was performed on seven patientsaffected by the atrophic form of age-related maculardegeneration (AF-ARMD). The patients under investiga-tion belonged to a larger study aimed at evaluating theefficacy of rheopheresis treatment (RT) on the visualfunction of AF-ARMD patients. Following the protocol ofthe larger study, patients received RT twice a week, everytwo weeks, for a total of ten treatments, as well as high-dose supplementation with zinc and vitamins A, E andbeta-carotene. Recruited patients underwent skin laserDoppler flowmetry coupled with skin iontophoresis of theendothelium-dependent vasodilator acetylcholine (ACh)and a test of skin post-ischemic reactive hyperemia,before and after the first RT (time 1: all seven patients)and the fifth RT (time 2: six patients). A significantlyhigher absolute (anova for repeated measures) and rela-
tive (percentage change from the baseline) skin blood fluxresponse (SBFR) to ACh iontophoresis was observedafter RT, compared to before RT at time 1 (679 � 43%and 436 � 78%, respectively; P < 0.05), as well as beforeRT at time 2 compared to before RT at time 1(683 � 74% and 436 � 78%, respectively; P < 0.05). Abso-lute and relative SBFR to ischemia did not differ eitherafter RT compared to before RT at time 1, or before RTat time 2 compared to before RT at time 1. These findingsare consistent with an acute and subacute beneficialeffect of RT on skin microvascular endothelial func-tion in the studied AF-ARMD patients. Key Words:Acetylcholine iontophoresis, Age-related macular de-generation, Laser Doppler flowmetry, Microvascularendothelial function, Rheopheresis treatment, Skinmicrocirculation.
Rheopheresis is a safe and effective application ofdouble filtration plasmapheresis for extracorporealhemorheotherapy (1–3). The elimination of a definedspectrum of hemorheologically relevant highmolecular weight proteins from human plasma, forexample fibrinogen, low-density lipoprotein choles-terol, a2-macroglobulin, immunoglobulin M (IgM),fibronectin, and von Willebrand factor (vWF)obtained by rheopheresis, causes a reduction in bloodand plasma viscosity as well as erythrocyte andthrombocyte aggregation (1,2). These effects repre-
sent the rationale for the use of rheopheresis in thetreatment of microcirculatory disorders such asischemic diabetic foot syndrome (4), critical limbischemia (5), sudden hearing loss (2), and age-relatedmacular degeneration (ARMD) (3,6–8).
ARMD is the leading cause of blindness in elderlypeople in the Western world. There are two forms ofARMD: dry ARMD and wet/exudative ARMD (9).The dry form is characterized by deposition of lipidsand proteins through Bruch’s membrane (drusen)and by the possible presence of retinal pigmentedepithelium dystrophy or atrophy, with likely progres-sive deterioration of central visual function (9). Theexudative form is characterized by proliferation ofchorio-capillaries through Bruch’s membrane (9),with rapid deterioration of central visual function.Although the pathogenesis of ARMD has not been
Received January 2009; revised March 2009.Address correspondence and reprint requests to Professor
Marco Rossi, Dipartimento di Medicina Interna, Università diPisa, Via Roma 67, 56100 Pisa, Italia. Email: [email protected]
Therapeutic Apheresis and Dialysis 13(6):540–548doi: 10.1111/j.1744-9987.2009.00705.x© 2009 The AuthorsJournal compilation © 2009 International Society for Apheresis
540

completely clarified, several epidemiologic studiesdemonstrated a positive association between ARMDand cardiovascular risk factors, such as arterial hyper-tension (10) and smoking (11), both conditionsknown to be associated with endothelial dysfunction.Recent findings showing an increase in plasma levelsof the vWF in ARMD patients (12), further suggestthat microvascular endothelial dysfunction couldcontribute to the pathogenesis of retinal microcircu-latory disorders responsible for ARMD.
This hypothesis suggests a further rationale for theuse of rheopheresis in the treatment of ARMD, basedon its hypothetical positive effect on microvascularendothelial dysfunction. In the literature, just onestudy assessed the effect of rheopheresis on theendothelial function at the level of the brachial arteryin patients suffering from sudden hearing loss (2).Another study investigated the effect of rheopheresistreatment on choroidal microcirculation in patientsaffected by early or late ARMD, using fluoresceinangiography (8). Nevertheless, to our knowledge,no study has evaluated the effect of rheopheresistreatment on microvascular endothelial function inpatients affected by ARMD. Therefore, we investi-gated the skin vasodilator response to acetylcholine(ACh) iontophoresis and to ischemia in ARMDpatients before and after rheopheresis treatments,with the aim of testing whether rheopheresis mightacutely and/or subacutely improve microvascularendothelial function in these patients.
MATERIAL AND METHODS
Study design and criteria for selection of patientsThe present pilot study belongs to a larger con-
trolled randomized study aimed at evaluating theeffect of rheopheresis treatment on visual function inpatients affected by the dry form of ARMD. Patientsrecruited in the larger study were randomizedto receive a rheopheresis treatment together witha high-dose supplementation regimen with zinc(80 mg/day), vitamin C (500 mg/day), vitamin E(400 IU/day), and beta carotene (15 mg/day), or onlya zinc and vitamins high-dose supplementationregimen. Rheopheresis treatment was performedin the first and fourth days of the week, every twoweeks, for a total of ten rheopheresis treatments.Patients recruited in the larger study were tested bin-ocularly using low-contrast letter acuity and EarlyTreatment Diabetic Retinopathy Study visual acuity,at the beginning of the study, every three monthsduring the study, and at the end of the study. At thesame time, patients underwent the following tests:biomicroscopy, tonometry, ophthalmoscopy, fluoran-
giography, optical coherence tomography of themacular region, electroretinogram, and computer-ized perimetry.
Patients were recruited in the larger study follow-ing two inclusion criteria: to be affected by a dry formof ARMD and to have a “best corrected visualacuity” between 20/30 to 20/100. Exclusion criteriaconsisted of: anemia, known disturbances in coagula-tion, systemic hypotension, collagen or neoplastic dis-eases, previous myocardial infarction, peripheralarterial diseases, infectious diseases, severe kidney orliver diseases, as well as chronic smoking. Patientswith evidence of proliferative retinopathy or rubeosiswere also excluded. The protocol of the larger studywas approved by the local ethics committee.
The present pilot study was performed in ARMDpatients who were consecutively recruited in thelarger study from March 2007 to February 2008 andwere randomized to receive rheopheresis treatmentand the high-dose supplementation regimen. Then,based on the larger study’s design, recruited patientsin the present study underwent rheopheresis treat-ment on the first and fourth days of the week, everytwo weeks, for a total of ten rheopheresis treatments.We also planned to investigate microvascular endot-helial function in the enrolled ARMD patients onehour before and one hour after the first rheopheresistreatment (time 1), as well as one hour before andone hour after the fifth rheopheresis treatment (time2). The protocol of the present pilot study wasapproved by the Local Ethics Committee.
RheopheresisRheopheresis treatment was performed using a
specialized blood and plasma therapy system(Diapact CRRT; B. Braun, Melsungen, Germany)with a polyethylene plasma separator (Plasmaflo;Asahi Kasei Kuraray Medical, Tokyo, Japan) and aspecifically designed ER-4000 Rheofilter (Asahi,Tokyo, Japan; effective surface area 2 m2).
Vascular access for the extracorporeal circuit wasestablished with two peripheral veins, and a bloodflow of about 60–80 mL/min was maintained. Afterseparation, blood was pumped at a continuous rate of60–90 mL/min through the ER-4000 Rheofilter, tar-geted high molecular weight plasma components(>600 kDa) were retained in the hollow fibers, whilesmaller plasma components were returned to thepatient. No substitution fluid was used. Continuousheparinization was used for anticoagulation. Aboutone and a half times the plasma volume of the patientwas processed in each rheopheresis treatment. Theplasma volume of each studied patient was estimated
Rheopheresis and Endothelial Function 541
© 2009 The AuthorsJournal compilation © 2009 International Society for Apheresis Ther Apher Dial, Vol. 13, No. 6, 2009

by means of the following formula: plasma volume(L) = 0.065 ¥ patient weight (kg) ¥ (1 - hematocrit(%)).
Microcirculatory investigationMicrocirculatory investigation consisted of the
measurement of the skin blood flux response to AChiontophoresis and to ischemia by means of laserDoppler flowmetry (LDF). Both tests were per-formed in a temperature controlled room (22 � 1°C),with the subject lying in a supine position, after20 min acclimatization.
Briefly, LDF is based on a laser beam that pen-etrates the skin and is partially back-scattered bymoving blood cells. According to the Doppler prin-ciple, a frequency shift occurs generating a signal thatis linearly related to red cell flux, as predicted bytheoretical and experimental models (13). In thepresent study an LDF apparatus (Periflux PF4001;Perimed, Järfälla, Sweden) with the following char-acteristics was used: wavelength 780 nm, bandwidth10–19 000 Hz, time constant 0.1 s, and samplingfrequency 32 Hz. Calibration was performed usingcolloidal latex particles whose Brownian motion pro-vides the standard value. The LDF outputs wererecorded continuously by an interfaced computer(Travelmate 202 T; Acer, Taipei, Taiwan) equippedwith Perisoft dedicated software, which allows theblood flux of the illuminated skin to be measured inconventional perfusion units (PU; 1 PU = 10 mV).
Acetylcholine iontophoresisAcetylcholine iontophoresis was performed before
and after rheopheresis, on the anterior surface of theright forearm. Iontophoresis is a procedure widelyused in clinical studies to locally transfer chargedvasoactive substances across the skin by means of asmall electric current (13). Characteristics of this pro-cedure are that it is non-invasive and avoids the sys-temic effects of the delivered vasoactive substancethat could interfere with the skin microcirculatoryresponse.
The apparatus we used in this case consisted of abattery-powered iontophoresis controller (Perijont328; Perimed) able to provide the current for AChdelivery to the skin. A drug delivery electrode withthe laser probe placed in the middle (PF 383;Perimed) and an indifferent electrode (PF 384;Perimed) were also used.The drug delivery electrodechamber was filled with 62.5 mL of 1% ACh solution,then it was attached on to the anterior surface of theright forearm by a double-sided adhesive disc. Anindifferent electrode was attached on to the anteriorsurface of the right forearm at 10 mm distance from
the drug delivery electrode, by a double-sided adhe-sive disc. Following a previous performed protocol(14,15) ACh was delivered to the skin by means ofnine iontophoretic pulses of 0.1 mA for 20 s, with a60 s interval between one pulse and the next. Basalskin blood flux was determined in PU as the mediumvalue within 5 min before iontophoresis. Maximalskin blood flux reached following each pulse ofACh iontophoresis was also determined in PU.Skin vasodilator response to ACh iontophoresis wasexpressed as the percentage change from the baselineof the maximal skin blood flux value reached follow-ing ACh iontophoresis.
Post-ischemic skin reactive hyperemiaTen minutes after ACh iontophoresis, each subject
underwent a test of skin post-ischemic reactive hype-remia on the left forearm. Skin ischemia was pro-duced by a pneumatic cuff, positioned on the leftforearm and inflated up to 30 mm Hg above the sys-tolic blood pressure of the subject. After 3 min offorearm ischemia the pneumatic cuff was thendeflated. Three minutes of occlusion were chosenbased on a previous study (16), which showed thatthree minutes of occlusion produced a significantlygreater increase in skin blood perfusion compared toperiods of 1 and 2 min occlusion. However, in our andother authors’ (16) experience, holding the ischemicconditions for more than three minutes producedbigger hyperemic responses, but at the expense ofpatient comfort. Skin blood flux was registered forfive minutes under basal conditions, during threeminutes of occlusion and for ten minutes followingthe pneumatic cuff release, using the same LDF appa-ratus used in the ACh iontophoresis test. Basalskin blood flux value was determined in PU asthe medium value within 5 min before occlusion;maximal blood flux value reached within five minutesfollowing pneumatic cuff release was determinedin PU. Skin vasodilator response to ischemia wasexpressed as the percentage change from the baselineof the highest blood flux value reached followingischemia.
Laboratory testsA 10 mL blood sample from each patient was ana-
lyzed for fibrinogen, a2-macroglobulin, vWF, IgMand total cholesterol serum levels, as well as hemo-globin blood concentration and hematocrit level,before and after rheopheresis, both at time 1 and attime 2.
Statistical analysisMicrocirculatory and laboratory data were
expressed as mean � standard error (SE) and as
M Rossi et al.542
© 2009 The AuthorsJournal compilation © 2009 International Society for ApheresisTher Apher Dial, Vol. 13, No. 6, 2009

mean � standard deviation (SD), respectively. Basalas well as maximal absolute and percentage bloodflux values obtained in response to ACh iontophore-sis or to ischemia were statistically compared usingStudent’s t-test for paired data. Skin vasodilatorresponses to ACh iontophoresis and to ischemiaobserved before rheopheresis at time 1 and beforerheopheresis at time 2 were statistically comparedusing Student’s t-test for non-paired data. Changes inthe absolute skin blood flux values following AChiontophoresis or to ischemia observed before andafter rheopheresis at time 1 were compared usinganova for repeated measures. Scheffè’s test wasapplied for multiple comparison testing when anovawas used. A P value less than 0.05 was consideredstatistically significant.
RESULTS
Studied patientsSeven patients (four males) affected by the dry
form of ARMD who fitted the inclusion and exclu-sion criteria took part in the study. The “best cor-rected visual acuity” of the diseased eye in eachpatient was 20/70, 20/100, 20/30, 20/200, 20/50 and20/70. Two patients presented with dry ARMDwith “geographic” atrophy. Patients did notreceive any treatment for their ophthalmologicdisease before their participation in this study. Thepatients’ main clinical and laboratory featuresare listed in Table 1. Three patients were affectedby arterial hypertension; one was affected byhypercholesterolemia; but no patients were affectedby diabetes. Pharmacological treatment consisted ofvalsartan, ramipril, and/or amlodipine in hyperten-sive patients, and of simvastatin in the one affected byhypercholesterolemia. Informed written consent wasobtained from each participant.All recruited patientsunderwent microcirculatory and laboratory tests at
time 1; six of them underwent microcirculatory andlaboratory tests also at time 2 of the study.
Results of microcirculatory investigation
Time 1Basal skin blood flux values did not significantly
differ before and after rheopheresis at time 1(9.8 � 5.7 PU and 9.7 � 3.4 PU, respectively; P =0.95).
Acetylcholine iontophoresis elicited a significantincrease in skin blood flux from the baseline, bothbefore rheopheresis (with a maximal skin blood fluxmean value of 38.1 � 17.2 PU, P < 0.005 from thebaseline) and after rheopheresis (with a maximal skinblood flux mean value of 65.8 � 26.1 PU, P < 0.001from the baseline).
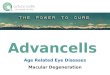
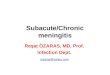
Changes in absolute skin blood flux values follow-ing Ach iontophoresis were significantly higherafter rheopheresis compared to before rheopheresis(anova for repeated measures; P < 0.001) (Fig. 1).Similarly, the skin vasodilator response to ACh ion-tophoresis, expressed as the percent change from thebaseline, was significantly higher after rheopheresiscompared to that obtained before rheopheresis(679 � 43% and 436 � 78%, respectively; P < 0.05)(Fig. 2).
Ischemia elicited a significant increase in the skinblood flux from the baseline both before rheopher-esis (with a maximal skin blood flux mean value of37.3 � 39.5 PU, P < 0.05 compared to the baseline)and after rheopheresis (with a maximal skin bloodflux mean value of 54.3 � 40.9 PU, P < 0.05 com-pared to the baseline). Changes in absolute skinblood flux values following ischemia did not signifi-cantly differ before and after rheopheresis (anovafor repeated measures) (Fig. 1). Similarly, the skinvasodilator response to ischemia, expressed as per-centage change from the baseline, did not differbefore and after rheopheresis (367 � 77% and444 � 78%, respectively; P = 0.24) (Fig. 3).
Time 2The basal skin blood flux mean values did not sig-
nificantly differ before and after rheopheresis at time2 (10.0 � 4.0 PU and 14.4 � 10.6 PU, respectively;P = 0.43). Acetylcholine iontophoresis elicited a sig-nificant increase in skin blood flux from the baselineboth before rheopheresis (with a maximal skin bloodflux mean value of 72.1 � 38.5 PU, P < 0.01 com-pared to baseline) and after rheopheresis (with amaximal skin blood flux mean value of 97.1 �54.8 PU, P < 0.05 compared to baseline).
TABLE 1. Clinical and laboratory features of the sevenpatients
Feature
Age (years) 68 � 11Sex (M/F) 4/3Body mass index 23.3 � 4.1SBP (mm Hg) 134 � 15DBP (mm Hg) 76 � 6TC serum levels (mg/dL) 204 � 52Plasma volume (mL) 2617 � 531Smoking (no/yes) No (in all seven patients)
DBP, diastolic blood pressure; F, female; M, male; SBP, systolicblood pressure; TC, total cholesterol.
Rheopheresis and Endothelial Function 543
© 2009 The AuthorsJournal compilation © 2009 International Society for Apheresis Ther Apher Dial, Vol. 13, No. 6, 2009

Changes in absolute skin blood flux values follow-ing ACh iontophoresis did not significantly differbefore and after rheopheresis (anova for repeatedmeasures). Similarly, the skin vasodilator response toACh iontophoresis expressed as the percentagechange from the baseline did not significantly differbefore and after rheopheresis (683 � 74% and880 � 222%, respectively; P = 0.28) (Fig. 2).
Ischemia elicited a significant increase in skinblood flux from the baseline both before rheopher-
esis (with a maximal skin blood flux mean value of42.8 � 44.1 PU, P < 0.05 compared to baseline) andafter rheopheresis (with a maximal skin blood fluxmean value of 36.2 � 22.4 PU, P < 0.01 compared tobaseline).
Changes in absolute skin blood flux values follow-ing ischemia did not significantly differ before andafter rheopheresis (anova for repeated measures).Similarly, the skin vasodilator response to ischemiaexpressed as percentage change from the baseline did
FIG. 1. (a) Skin blood flux values(mean � SE) observed under basal condi-tions (baseline) and following each pulse ofacetylcholine (ACh) iontophoresis beforeand after rheopheresis at time 1 of thestudy in seven patients suffering from age-related macular degeneration. p = AChiontophoresis pulse, P < 0.001 betweenbefore and after rheopheresis. (b) Skinblood flux values (mean � SE) observedunder basal conditions (baseline) and fol-lowing ischemia before and after rheopher-esis at time 1 of the study in seven patientswith age-related macular degeneration.
0
10
20
30
40
50
60
70
80
90
Baseline 1 th p 2 th p 3 th p 4 th p 5 th p 6 th p 7 th p 8 th p 9 th p
0
10
20
30
40
50
60
70
80
90
Ski
nbl
ood
flux
(PU
)S
kin
bloo
dfl
ux(P
U)
Baseline Following ischemia
Before rheopheresis
After rheopheresis
P < 0.001
Before rheopheresis
After rheopheresis
(a)
(b)
M Rossi et al.544
© 2009 The AuthorsJournal compilation © 2009 International Society for ApheresisTher Apher Dial, Vol. 13, No. 6, 2009

not significantly differ before and after rheopheresis(511 � 124% and 434 � 83%, respectively; P = 0.56)(Fig. 3).
A significantly higher skin vasodilator response toACh iontophoresis was observed before rheopher-esis at time 2 compared to the one obtained beforerheopheresis at time 1 (683 � 74% vs. 436 � 78%;P < 0.05) (Fig. 2), while skin vasodilator response toischemia obtained before rheopheresis at time 2 didnot significantly differ from that one obtained beforerheopheresis at time 1 (Fig. 3).
Results of laboratory testsThe results of the laboratory tests are reported in
Table 2. With the only exception of hematocrit leveland hemoglobin blood concentration, which did notsignificantly differ before and after rheopheresisat both times of the study, a statistically significantdecrease in the other laboratory parameters investi-gated was observed after rheopheresis compared tobefore rheopheresis, both at time 1 and time 2.
DISCUSSION
The main finding of our study is that in ARMDpatients the skin vasodilator response to ACh
Before rheopheresis
After rheopheresis
0
300
600
900
1200
Time 1 Time 2
***
Ski
n va
sodi
lato
r re
spon
se (
%)
FIG. 2. Skin vasodilator response (percent change in skin bloodflux from the baseline) (mean � SE) observed in response to ace-tylcholine iontophoresis, before and after rheopheresis, in sevenpatients suffering from age-related macular degeneration at time 1of the study, and in six patients at time 2 of the study. *P < 0.05between before and after rheopheresis at time 1, **P < 0.05between before rheopheresis at time 1 and before rheopheresis attime 2.
TABLE 2. Laboratory values (mean � SD) obtained before and after rheopheresis treatment (RT) at time 1 and time 2 ofthe study
Time 1 Time 2
Before RT After RT Before RT After RT
Fibrinogen (mg/dL) 332 � 103 113 � 32**** 387 � 70 132 � 58*****a2-Macroglobulin (mg/dL) 179 � 77 66 � 38*** 140 � 67 64 � 34**von Willebrand factor (IU/dL) 87 � 31 60 � 18* 109 � 37 49 � 18**Immunoglobulin M (mg/dL) 89 � 110 47 � 66* 59 � 39 22 � 15*Total cholesterol (mg/dL) 204 � 52 110 � 34***** 212 � 36 96 � 21*****Hemoglobin (g %) 14 � 2 14 � 1 14 � 2 13 � 2Hematocrit (%) 43 � 5 42 � 6 42 � 6 42 � 7
*P < 0.05 compared to before rheopheresis, **P < 0.01 compared to before rheopheresis, ***P < 0.005 compared to before rheopheresis,****P < 0.001 compared to before rheopheresis, *****P < 0.0005 compared to before rheopheresis.
Before Rheopheresis
After Rheopheresis
0
200
400
600
800
Time 1 Time 2 S
kin
vaso
dila
tor
resp
onse
(%
)
FIG. 3. Skin vasodilator response (percent change in skin bloodflux from the baseline) (mean � SE) observed in response toischemia, before and after rheopheresis, in seven patients sufferingfrom age-related macular degeneration at time 1 of the study, andin six of them at time 2.
Rheopheresis and Endothelial Function 545
© 2009 The AuthorsJournal compilation © 2009 International Society for Apheresis Ther Apher Dial, Vol. 13, No. 6, 2009

iontophoresis significantly increased after the firstrheopheresis treatment compared to before rheo-pheresis, while in the same patients the skin vasodi-lator response to ischemia did not significantlychange after the first rheopheresis treatment com-pared to before the same treatment. This finding isconsistent with an acute beneficial effect of rheo-pheresis treatment on skin microvascular endo-thelial function in the recruited ARMS patients. Inour patients this effect of rheopheresis was asso-ciated with a statistically significant reduction inplasma levels of fibrinogen, total cholesterol, a2-macroglobulin, IgM, and vWF. A further finding wasthat the same ARMD patients exhibited a persistentincrease in skin vasodilator response to ACh ionto-phoresis, compared to the first pre-rheopheresis test,when they underwent a second microcirculatoryinvestigation about a month later. This is consistentwith a persistent improvement in skin microvascularendothelial function in the studied ARMD patientsat the time of the second microcirculatory investi-gation, suggesting a positive subacute effect ofrheopheresis treatment on skin microvascularendothelial function.
It has been recently hypothesized that reductionin plasma levels of a defined spectrum of hemorheo-logically relevant high molecular weight proteinsinduced by rheopheresis could ameliorate endothe-lial dysfunction (2,8), with consequent beneficialeffects on different microcirculatory disorders. In aprevious study (2) a positive acute effect of rheopher-esis on endothelial dysfunction was demonstrated atthe level of the brachial artery in patients sufferingfrom sudden hearing loss; however, endothelial func-tion data obtained at the brachial artery level donot accurately reflect endothelial function at themicrovascular level (17). Microvascular endothelialfunction can be investigated at skin level by means ofLDF coupled with ACh iontophoresis. It has beendemonstrated that skin microvascular dysfunctionreflects other districts microvascular dysfunction thatcould be present in other microvascular districts,including the myocardium and the retina (18–21).Then, skin may be considered a suitable “window”for the investigation of microvascular endothelialfunction in patients affected by ARMD, a retinaldisease that is suggested to be a microvasculardisorder (8).
The LDF method used in the present study has agood sensitivity in detecting and quantifying changesin skin blood flux in response to a given stimulus (22).ACh produces endothelium-dependent vasodilata-tion in human skin microcirculation mainly through aprostanoid-dependent pathway (23). However, ACh
iontophoresis, as a unique test for the investigation ofskin endothelial function, is questionable because theextent of the skin vasodilator response to ACh couldbe influenced by the skin endothelial-independentvasoreactivity or by the skin microvascular wallcompliance (16). Iontophoresis of the endothelium-independent vasodilator sodium nitroprusside hasbeen shown to be a reliable control test in the inves-tigation of skin microvascular endothelial functionusing ACh iontophoresis (24). Unlike ACh, ischemiaelicits a skin vasodilator response through differentnon-endothelial-dependent mechanisms, includingthe accumulation of vasodilator metabolite adenos-ine in the skin (25), the relaxation of skin microvesselsmooth muscle cells (26) and the activation ofsensory nerves (22).Although recent findings suggestthat the skin vasodilator response to ischemia mayalso be partly mediated by endothelium-releasedprostaglandins (27), this represents only a potentialand secondary mechanism (22). Indeed, post-ischemic skin reactive hyperemia may represent asuitable “control” test in the investigation of skinmicrovascular endothelial function by means of AChiontophoresis.
The absence of any significant change in the skinvasodilator response to ischemia after rheopheresis,with respect to before rheopheresis, observed in thepresent study suggests that the parallel post-rheopheresis increase in skin vasodilator responseto ACh iontophoresis reflects an improved skinmicrovascular endothelial function. There is anongoing discussion regarding the underlying mecha-nisms of ARMD, thus leading to different therapeu-tic approaches. The hypothesis that choroidalmicrocirculation would be impaired in ARMD,leading to the deposition of lipids and proteins inBruch’s membrane (drusen), represented the ratio-nale for the use of rheopheresis in ARMD patients(3,6–8). According to this hypothesis, a reduction indrusen size and number was observed in a high per-centage of ARMD patients treated with rheopher-esis in a previous study (8). The new contribution ofour study with respect to the previous mentionedinvestigation (8) is the preliminary demonstrationthat rheopheresis exerts an acute and subacute ben-eficial effect on microvascular endothelial functionin patients suffering from the dry form of ARMD.This observation may represent a further rationalefor the use of rheopheresis in the treatment ofpatients suffering from ARMD, since some labora-tory (12) and clinical findings (10,11) obtainedin ARMD patients suggest the involvement ofmicrovascular endothelial dysfunction in the patho-genesis of ARMD.
M Rossi et al.546
© 2009 The AuthorsJournal compilation © 2009 International Society for ApheresisTher Apher Dial, Vol. 13, No. 6, 2009

Further studies are required to confirm the benefi-cial effect of rheopheresis on microvascular endothe-lial function in ARMD patients and to verify if theimprovement in endothelial function may be predic-tive for the final outcome of ARMD patients. A limi-tation of this study is the relatively small number ofinvestigated ARMD patients, resulting in weak sta-tistical support of the obtained data. There was not aspecific rationale for investigating only seven ARMDpatients in the present study. The small number ofstudied patients also represents a limitation of theone previous study that investigated the effect ofrheopheresis on endothelial function at the level ofthe brachial artery in patients suffering from suddenhearing loss (2). On the other hand, concordancebetween absolute and relative skin blood fluxchanges in response to ACh iontophoresis andischemia observed in our recruited ARMD patientsminimizes this potential limitation of our study. Afurther limitation of this study could be the absenceof a control group involving subjects not affected byARMD; however, the aim of this study was to evalu-ate the acute and subacute effects of rheopheresistreatments on microvascular endothelial function inARMD patients, and not to ascertain if microvascu-lar endothelial dysfunction was present in thesesubjects.
CONCLUSION
To our knowledge, this is the first reported studysuggesting a beneficial acute and subacute effect ofrheopheresis treatment on microvascular endothe-lial function in patients affected by the dry form ofARMD. Further studies are required to confirm thiseffect of rheopheresis treatment in ARMD patientsand to evaluate if the improvement in microvascularendothelial function may be predictive for the finaloutcome of ARMD patients.
Acknowledgments: We would like to thank Dr SimonaValleggi for her kind and useful help with the writtenEnglish version of this manuscript.
REFERENCES
1. Klingel R, Fassbender C, Fassbender T, Erdtracht B, Berrous-chot J. Rheopheresis: rheologic, functional, and structuralaspects. Ther Apher 2000;4:348–57.
2. Balletshofer BM, Stock J, Rittig K et al. Acute effect of Rheo-pheresis on peripheral endothelial dysfunction in patients suf-fering from sudden hearing loss. Ther Apher Dial 2005;9:385–90.
3. Pulido J, Sanders D, Winters JL, Klingel R. Clinical outcomesand mechanism of action for Rheopheresis treatment of age-
related macular degeneration (AMD). J Clin Apher 2005;20:185–94.
4. Klingel R, Mumme C, Fassbender T et al. Rheopheresis inpatients with ischemic diabetic foot syndrome: results of anopen label prospective pilot trial. Ther Apher Dial 2003;7:444–55.
5. Ferrannini M, Vischini G, Staffolani E et al. Rheopheresis invascular diseases. Int J Artif Organs 2007;30:923–9.
6. Klingel R, Fassbender C, Fischer I et al. Rheopheresis for age-related macular degeneration: a novel indication for therapeu-tic apheresis in ophthalmology. Ther Apher 2002;6:271–81.
7. Pulido JS, Sanders D, Klingel R. Rheopheresis for age-relatedmacular degeneration: clinical results and putative mechanismof action. Can J Ophthalmol 2005;40:332–40.
8. Fell AJ, Engelmann K, Richard G, Fassbender C, Wahls W,Klingel R. Rheophoresis. A systematic approach to therapy ofage-related macular degeneration (AMD)? Ophthalmologe2002;99:780–4.
9. Age-Related Eye Disease Study Research Group. The Age-Related Eye Disease Study system for classifying age-relatedmacular degeneration from stereoscopic color fundusphotographs: the Age-Related Eye Disease Study ReportNumber 6. Am J Ophthalmol 2001;132:668–81.
10. Sperduto RD, Hiller R. Systemic hypertension and age-relatedmaculopathy in the Framingham Study. Arch Ophthalmol1986;104:216–9.
11. Klein R, Klein BE, Linton KL, DeMets DL. The relation ofage-related maculopathy to smoking. The Beaver Dam EyeStudy. Am J Epidemiol 1993;137:190–200.
12. Lip PL, Blann AD, Hope-Ross M, Gibson JM, Lip GY. Age-related macular degeneration is associated with increasedvascular endothelial growth factor, hemorheology and endot-helial dysfunction. Ophthalmology 2001;108:705–10.
13. Nilsson GE, Tenland T, Oeberg PA. Evaluation of laserDoppler flowmeter for measurements of tissue blood flow.IEEE Trans Biomed Eng 1980;27:597–604.
14. Kalia YN, Naik A, Garrison J, Guy RH. Iontophoretic drugdelivery. Adv Drug Deliv Rev 2004;56:619–58.
15. Rossi M, Ricco R, Carpi A. Spectral analysis of skin laserDoppler blood perfusion signal during cutaneous hyperemiain response to acetylcholine iontophoresis and ischemia innormal subjects. Clin Hemorheol Microcirc 2004;31:303–10.
16. Rossi M, Bazzichi L, Di Maria C et al. Blunted increase ofdigital skin vasomotion following acetylcholine and sodiumnitroprusside iontophoresis in systemic sclerosis patients.Rheumatology 2008;47:1012–7.
17. Tee GB, Rasool AH, Halim AS, Rahman AR. Dependence ofhuman forearm skin postocclusive reactive hyperemia onocclusion time. J Pharmacol Toxicol Methods 2004;50:73–8.
18. Gori T, Di Stolfo G, Sicuro S et al. Correlation analysisbetween different parameters of conduit artery and microvas-cular vasodilation. Clin Hemorheol Microcirc 2006;35:509–15.
19. Shamim-Uizzaman Q, Pfenninger D, Kehrer C. Altered cuta-neous microvascular responses to reactive hyperemia in coro-nary artery disease: a comparative study with conduit vesselresponses. Clin Sci 2002;103:267–73.
20. Tur E, Yosipovitch G, Bar-On Y. Skin reactive hyperemia indiabetic patients. Diabetes Care 1991;14:958–62.
21. Jung F, Mrowietz C, Labarrere C. Primary cutaneous microan-giopathy in heart recipients. Microvasc Res 2001;62:154–63.
22. Cracowski JL, Minson CT, Salvat-Melis M, Halliwill JR. Meth-odological issues in the assessment of skin microvascularendothelial function in humans. Trends Pharmacol Sci 2006;27:503–8.
23. Holowatz LA, Thompson CS, Minson CT, Kenney WL.Mechanisms of acetylcholine-mediated vasodilatation inyoung and aged human skin. J Physiol 2005;15:965–73.
24. Morris SJ, Shore AC, Tooke JE. Responses of the skin micro-circulation to acetylcholine and sodium nitroprusside inpatients with NIDDM. Diabetologia 1995;38:1337–44.
Rheopheresis and Endothelial Function 547
© 2009 The AuthorsJournal compilation © 2009 International Society for Apheresis Ther Apher Dial, Vol. 13, No. 6, 2009

25. Roddie IC. Circulation to skin and adipose tissue. In: Geiger,SR, ed. Bethesda, MD: The Cardiovascular System, 1983;285–317.
26. Patterson GC. The role of intravascular pressure in the causa-tion of reactive hyperaemia in the human forearm. Clin Sci1956;15:17–25.
27. Binggeli C, Spieker LE, Corti R et al. Statins enhance postis-chemic hyperemia in the skin circulation of hypercholester-olemic patients. E monitoring test of endothelial dysfunctionfor clinical practice. JACC 2003;42:71–7.
M Rossi et al.548
© 2009 The AuthorsJournal compilation © 2009 International Society for ApheresisTher Apher Dial, Vol. 13, No. 6, 2009







![Uveitic macular edema: a stepladder treatment paradigm€¦ · of macular edema [1,3–4], this review will focus on uveitic macular edema specifically. Uveitic macular edema Macular](https://img.pdfslide.us/doc/110x75/5ed770e44d676a3f4a7efe51/uveitic-macular-edema-a-stepladder-treatment-paradigm-of-macular-edema-13a4.jpg)