Embed Size (px)
Citation preview

915
Research
Bull World Health Organ 2010;88:915–921C | doi:10.2471/BLT.10.076737
Introduction
Acupuncture is popular in most countries, but nowhere more than in China. Because its use is so widespread, safety is an im-portant issue that deserves close attention. Serious adverse events resulting from acupuncture, including pneumothorax, cardiac tamponade, spinal cord injury and viral hepatitis, have been identified in previous literature reviews.1–4 Prospective surveys to determine the frequency of acupuncture-related adverse events have been conducted in Germany,5,6 Norway7 and the United Kingdom of Great Britain and Northern Ireland.8,9 These studies have shown an incidence of mild, transient acupuncture-related adverse events that ranges from 6.71% to 15%. The most com-mon adverse events of this type were local pain from needling (range: 1.1–2.9%) and slight bleeding or haematoma (range: 2.1–6.1%). In a prospective observational study of 190 924 patients, the incidence of serious adverse events (death, organ trauma or hospital admission) was about 0.024%.5 Another large-scale observational study showed a rate of adverse events requiring specific treatment of 2.2% (4963 incidents among 229 230 subjects).6 Studies such as these have shown that in extremely rare cases acupuncture can lead to serious, sometimes life-threatening complications, in addition to mild and transient adverse events.
Because most reports on the safety of acupuncture have been published outside China, the objective of this article was to summarize the Chinese literature on the subject of acupuncture-related adverse events and determine the possible reasons that such events occur.
MethodsInclusion/exclusion criteriaIn December 2009 we searched the following electronic data-bases: Chinese Biomedical Literature Database (1980–2009), Chinese Journal Full-Text Database (1980–2009) and Weipu Journal Database (1989–2009). The search terms were: (acu-puncture OR needle) AND (induce OR cause OR adverse event OR adverse reaction OR side effect OR complication OR harm OR risk OR mistake OR infection OR injury OR fainting OR haemorrhage OR bleeding OR death OR pneumothorax OR pain). We searched for these terms (in Chinese) as free text in the title or abstract, and we also hand-searched the reference lists of all reports located through the electronic searches.
Case reports, case series, surveys and other observational studies were included in the review if they reported factual data on complications related to acupuncture. Review articles, transla-tions and clinical trials were excluded. The search was limited to Chinese-language papers.
Different types of acupuncture can lead to different adverse events. To present clear results, we only included reports on traditional needle acupuncture, defined as a procedure in which stainless steel filiform needles are inserted into acupoints – acu-puncture points located throughout the body that are associated with specific therapeutic effects – and manipulated in place. Other types of acupuncture, such as electroacupuncture, laser acupuncture and auricular acupuncture, were excluded.
Two authors (Zhang and Shang) independently examined the titles and abstracts of all papers found through the search to determine if they fulfilled the inclusion criteria outlined
Une traduction en français de ce résumé figure à la fin de l’article. Al final del artículo se facilita una traducción al español. الرتجمة العربية لهذه الخالصة يف نهاية النص الكامل لهذه املقالة.
Objective To systematically review the Chinese-language literature on acupuncture-related adverse events.Methods We searched three Chinese databases (the Chinese Biomedical Literature Database, 1980–2009; the Chinese Journal Full-Text Database, 1980–2009; and the Weipu Journal Database, 1989–2009) to identify Chinese-language articles about the safety of traditional needle acupuncture. Case reports, case series, surveys and other observational studies were included if they reported factual data, but review articles, translations and clinical trials were excluded.Findings The inclusion criteria were met by 115 articles (98 case reports and 17 case series) that in total reported on 479 cases of adverse events after acupuncture. Fourteen patients died. Acupuncture-related adverse events were classified into three categories: traumatic, infectious and “other”. The most frequent adverse events were pneumothorax, fainting, subarachnoid haemorrhage and infection, while the most serious ones were cardiovascular injuries, subarachnoid haemorrhage, pneumothorax and recurrent cerebral haemorrhage.Conclusion Many acupuncture-related adverse events, most of them owing to improper technique, have been described in the published Chinese literature. Efforts should be made to find effective ways of monitoring and minimizing the risks related to acupuncture.
Acupuncture-related adverse events: a systematic review of the Chinese literatureJunhua Zhang,a Hongcai Shang,a Xiumei Gaoa & Edzard Ernstb
a Research Centre of Traditional Chinese Medicine, Tianjin University of Traditional Chinese Medicine, 88 Yuquan Road, Tianjin, 300193, China.b Peninsula Medical School, University of Exeter, Exeter, England.Correspondence to Junhua Zhang (e-mail: [email protected]).(Submitted: 9 February 2010 – Revised version received: 21 July 2010 – Accepted: 4 August 2010 – Published online: 27 August 2010 )

Bull World Health Organ 2010;88:915–921C | doi:10.2471/BLT.10.076737916
Junhua Zhang et al.Review of acupuncture-related adverse events in ChinaResearch
above. The full texts of potentially rel-evant articles were retrieved for detailed assessment. Disagreements between the two authors were resolved by discussion.
Information on author, patient, acu-puncturist, acupuncture site, adverse event, treatment and outcome was extracted from the primary articles and entered into a pre-formulated spreadsheet. Acupoints were described by pinyin name (i.e. the Latinized spelling of traditional Mandarin Chinese names) and code according to a standard nomenclature developed by the World Health Organization.10,11 These data have been summarized in three tables according to the type of adverse event.
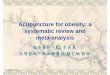
ResultsOur inclusion criteria were met by 115 articles (98 case reports and 17 case series) (Fig. 1). We noted no clear trend in the frequency of reports of acupuncture-re-lated adverse events over the past 30 years.
In total, 479 cases of acupuncture-related adverse events were reported. Patients ranged in age from 2 to 73 years. The first authors of the papers were members of medical departments, court jurisdictions and police depart-ments. Only 20% of these authors were the acupuncturists who performed the procedure that caused the adverse event. The reported acupuncture-related adverse events were classified into three categories: traumatic (Table 1, avail-able at: http://www.who.int/bulletin/volumes/88/12/10-076737), infectious (Table 2) and “other” (Table 3).
Traumatic eventsTraumatic injuries were reported in 87 articles (73 case reports and 14 case series) and totalled 296 cases. The events were classified into seven subgroups according to the type and site of the injury.
Arachnoid and spinal dura materNine cases of spinal epidural haematoma (in the cervical, thoracic and lumbar spine) were reported. No further informa-tion was provided.
Subarachnoid haemorrhage was reported in 35 patients, 3 of whom died. The others recovered after 1 to 8 weeks of treatment. One of the deceased patients had a history of hypertension and cerebral haemorrhage and died 10 days after the acupuncture. The other two patients died within 30 minutes of having undergone the acupuncture, perhaps as a result of injury to the medulla oblongata.
The acupoints most frequently in-volved in cases of subarachnoid haemor-rhage and spinal epidural haematoma were Fengchi (GB20), Yamen (GV15), Fengfu (GV16), Dazhui (GV14) and Tianzhu (BL10). In several cases, the needles were inserted to a depth of 4 to 5 cm below the skin’s surface, and such deep insertion is suspected to have led to injury.
Thoracic organs and tissuesWith a total of 201 cases, pneumotho-rax was the most frequently reported acupuncture-related adverse event. Four patients died from it and the others recov-ered after 2 to 30 days of treatment. One
patient was a 70-year-old woman with a history of chronic bronchitis, emphysema, cor pulmonale and heart failure who died from pulmonary infection, heart failure and pneumothorax. Two more women died after not receiving timely treatment for pneumothorax caused by needling at the Jianjing (GB21) and Tianding (LI17) acupoints. The fourth patient died from tension pneumothorax but no further information was provided.
The acupuncture sites in these cases were primarily in the shoulder and scapu-lar regions (64%) and in the chest (24%). In two cases, the Tianding (LI17) point in the neck area had been needled. The most frequently used acupoints were Jianjing (GB21; 30%), Feishu (BL13; 15%), Quepen (ST12; 10%) and Tiantu (CV22; 10%). Other acupoints were Ganshu (BL18), Shenshu (BL23), Ti-anding (LI17), Jiuwei (CV15), Juque (CV14), Jianzhen (SI9), Quyuan (SI13) and Dingchuan (EX-B1).
Chylothorax was reported after needling at the Feishu (BL13) point in a 21-year-old man with a malformed thoracic duct. Right ventricular injury was reported in four cases, two of which recovered after surgical treatment. The other two patients died from right ven-tricular puncture complicated by cardiac tamponade and multiorgan dysfunction syndrome. One case of aortic artery rup-ture was reported after needling at the Qi-men point (LR14) at a depth of 4 cm; the patient died within 15 minutes. Coronary artery injury with cardiac tamponade was reported in a man who treated himself for chronic bronchitis and lost the needle at the Zhongfu point (LU1).
Abdominal organs and tissuesInjuries of abdominal organs and tis-sues were reported in 16 patients, all of whom recovered after surgery. These instances included perforations of the gallbladder, of the bowels and of the stomach, frequently complicated by peritonitis. A 2-year-old boy suffered intestinal wall haematoma with intes-tinal obstruction after acupuncture treatment for diarrhoea.
The acupoints associated with such adverse events were Tianshu (ST25), Zhongwan (CV12) and Qimen (LR14). Most of the patients underwent acupunc-ture for abdominal pain, attributable mainly to appendicitis or cholecystitis. Deep needling accounted for most of the abdominal injuries.
Fig. 1. Flow diagram for systematic review of the Chinese-language literature on adverse events related to traditional needle acupuncture, 1980–2009
Records identified from database(n = 1810)
Potentially relevant articles(n = 247)
Articles assessed for eligibility(n = 141)
Included articles(n = 115)
98 case reports;17 case series
Duplicates, articles not about acupuncture(n = 1563)
Reports unrelated to adverse events,duplicates, reviews and translations
(n = 106)
Articles about acupoint injection,electroacupuncture and related measures
(n = 26)

Bull World Health Organ 2010;88:915–921C | doi:10.2471/BLT.10.076737 917
Junhua Zhang et al. Review of acupuncture-related adverse events in ChinaResearch
Neck areaSix cases of injuries in the neck region were reported, including neural injuries (4), a false aneurysm of the carotid artery (1) and thyroid haemorrhage (1). One patient died after acupuncture at the Tiantu point (CV22); the needle had been inserted to a depth of 6 cm.
EyesFive articles reported injuries to the eyes, including orbital haemorrhage (3), trau-matic cataract (1), injury of the oculomo-tor nerve (1) and retinal puncture (1). One case of optic atrophy accompanied by haemorrhage and traumatic cataract resulted in visual impairment.
The acupoints in the above cases were Jingming (SL1), Qiuhou (EX-HN7) and Chengqi (ST1). When needling acupoints in the area of the orbital cavity, bleeding is difficult to avoid, even for the experienced acu-puncturist. Deep needling can also injure the oculomotor nerve, the retina and neighbouring tissues.
Peripheral nerves, vessels and other tissuesThree cases of haemorrhage were reported after acupuncture on the cheeks and the hypoglottis. One case of calf haematoma complicated by diabetic foot was caused by needling at the Tiaokou (ST38) and Chengshan (BL57) acupoints.
Four cases of peripheral motor nerve injuries and subsequent motor dysfunc-tion were reported. Three children suffered adductor muscle fibrosis and ad-duction deformity of the thumb as a result of local vascular and muscular injuries from needling at the Hegu point (LI4).
The acupoints most frequently involved in the injuries were Taiyang (EX-HN5), Neiguan (PC6) and Hegu (LI4). Forceful needle manipulation at these points, which are quite superficial, can cause injury to peripheral nerves, capillaries and muscle fibres.
Needling site pain and broken needleFour cases of pain at the needling site were reported in two articles. An intra-abdominal lump turned out to be caused by an acupuncture needle fragment that had broken off 15 years earlier.
Infectious eventsNine cases of bacterial infection and two cases of viral infection were reported. Ta
ble
2. C
ase
repo
rts
of in
fect
ion
afte
r tra
ditio
nal n
eedl
e ac
upun
ctur
e, a
s id
entifi
ed th
roug
h a
syst
emat
ic re
view
of t
he C
hine
se-l
angu
age
liter
atur
e, 1
980–
2009
Refe
renc
eaCa
sesb (
age
in
year
s an
d se
x)Re
ason
for
acup
unct
ure
Acup
oint
(c
odec o
r site
)Ad
vers
e ev
ent
Outc
ome
Caus
ed b
y
acup
unct
ure?
Zhan
g JG
. Acu
punc
ture
cau
sed
bucc
al s
pace
abs
cess
. Med
J C
hin
Peop
le’s
Arm
ed
Polic
e Fo
rces
200
7;18
:778
.23
, mal
eTo
otha
che
Bucc
al re
gion
Bucc
al s
pace
ab
sces
sRe
cove
ryPr
obab
ly
Zhao
YJ.
Acu
punc
ture
indu
ced
tem
pora
l spa
ce a
bsce
ss. C
hin
J M
ed To
day
2003
;3:7
1.52
, mal
eTo
otha
che
Bucc
al re
gion
Tem
pora
l spa
ce
absc
ess
Reco
very
Prob
ably
Ma
JF, W
ang
KK, T
ian
ZC. A
cupu
nctu
re-in
duce
d in
fect
ion
in b
utto
cks
with
ext
ensi
ve
subc
utan
eous
tiss
ue n
ecro
sis.
Chi
n Pr
act J
Rur
al D
octo
r 199
0;2:
30–1
.45
, mal
eGl
utea
l num
bnes
sGl
utea
l reg
ion
Glut
eal a
bsce
ssRe
cove
ryCe
rtain
ly
Chen
YS,
Gao
L. B
rain
abs
cess
afte
r acu
punc
ture
in th
e he
ad. P
eopl
e’s
Mil
Surg
19
95;4
:58.
30, m
ale
Inso
mni
a, d
izzin
ess
Ceph
alic
regi
onAb
sces
s of
sca
lp,
intra
cran
ial
absc
ess
Reco
very
Certa
inly
Xu C
Z. In
tracr
ania
l inf
ectio
n ca
used
by
acup
unct
ure.
Nei
Mon
gol J
Trad
Chi
n M
ed
1990
;1:1
2.19
, mal
eHe
adac
heCe
phal
ic re
gion
Absc
ess
of s
calp
, in
tracr
ania
l ab
sces
s
Reco
very
Certa
inly
Song
QL,
Wu
TY. T
hree
ther
apeu
tic a
cupu
nctu
re e
rrors
. Clin
Misd
iag
Mist
her
2001
;14:
73.
38, m
ale
Arth
ritis
EX-L
E5Su
ppur
ative
ar
thrit
isRe
cove
ryCe
rtain
ly
Zhou
Z. S
uper
ficia
l tub
ercu
lous
abs
cess
cau
sed
by a
cupu
nctu
re in
3 c
ases
. Jiu
jiang
M
ed J
199
9;1:
47.
22–2
8, 1
mal
e &
2 fe
mal
esPs
oatic
stra
inLo
wer
bac
kTu
berc
ulou
s ab
sces
sRe
cove
ryPr
obab
ly
Liu
CR. A
cupu
nctu
re-in
duce
d te
tanu
s. C
hin
Prac
t J R
ural
Doc
tor 1
992;
4:30
.52
, fem
ale
Leg
pain
–Te
tanu
sRe
cove
ryPr
obab
lyLi
u GX
. Acu
punc
ture
cau
sed
teta
nus.
J M
ed T
heor
Pra
ct 1
991;
4:30
.52
, fem
ale
Head
ache
Ceph
alic
regi
onTe
tanu
sRe
cove
ryPr
obab
lya A
ll re
fere
nces
in th
is ta
ble
are
in C
hine
se. T
he E
nglis
h-la
ngua
ge p
aper
and
jour
nal t
itles
are
free
tran
slat
ions
. The
orig
inal
Chi
nese
-lang
uage
title
s ca
n be
obt
aine
d fro
m th
e co
rresp
ondi
ng a
utho
r.b O
nly
case
s of
trad
ition
al n
eedl
e ac
upun
ctur
e ar
e in
clud
ed. T
his
expl
ains
any
dis
crep
ancy
bet
wee
n th
e nu
mbe
r of c
ases
in th
is c
olum
n an
d th
e tit
le o
f the
cor
resp
ondi
ng re
fere
nce.
c Ref
eren
ces10
and
11.

Bull World Health Organ 2010;88:915–921C | doi:10.2471/BLT.10.076737918
Junhua Zhang et al.Review of acupuncture-related adverse events in ChinaResearch
Tabl
e 3.
Acu
punc
ture
-rel
ated
adv
erse
eve
nts
othe
r tha
n tr
aum
a an
d in
fect
ion,
as
iden
tified
thro
ugh
a sy
stem
atic
revi
ew o
f the
Chi
nese
-lan
guag
e lit
erat
ure,
198
0–20
09
Refe
renc
eaCa
sesb (
age
in
year
s an
d se
x, o
r no
. of c
ases
)
Reas
on fo
r ac
upun
ctur
eAc
upoi
nt
(cod
ec or s
ite)
Adve
rse
even
tOu
tcom
eCa
used
by
ac
upun
ctur
e?
Liu
CB. A
cupu
nctu
re-r
elat
ed s
ynco
pe in
4 c
ases
. J C
lin A
cu M
oxib
ustio
n 20
01;1
7:51
.34
, 45
& 56
, fe
mal
esLo
w b
ack
pain
; sh
ould
er p
ain
Fain
ting
Reco
very
Certa
inly
Liu
YZ. I
mpr
oper
pos
ture
cau
sed
by a
cupu
nctu
re in
2 c
ases
. Lish
izhen
Med
Mat
eria
M
ed R
es 2
007;
18:1
756.
42, f
emal
eSh
ould
er p
ain
Shou
lder
site
Fain
ting
Reco
very
Certa
inly
Shi G
P, Ch
en Z
M. A
ccid
ents
cau
sed
by a
cupu
nctu
re in
3 c
ases
. J C
lin A
cu
Mox
ibus
tion
1994
;10:
38.
57, f
emal
eSt
omac
h ac
he–
Fain
ting
Reco
very
Certa
inly
Xu G
P, Yu
an Y
M. F
irst a
id a
nd c
are
of 8
2 fa
intin
g ep
isod
es d
urin
g ac
upun
ctur
e. C
hina
He
alth
car
e In
nov
2007
;2:1
25.
82 c
ases
––
Fain
ting
Reco
very
Certa
inly
You
Y. Fa
intin
g du
ring
acup
unct
ure
in 6
0 fli
ght p
erso
nnel
. Chi
n J
Misd
iag
2007
;7:5
668–
9.60
cas
es–
–Fa
intin
gRe
cove
ryCe
rtain
ly
Zhan
g H,
Sun
S. F
aint
ing
durin
g ac
upun
ctur
e an
d its
man
agem
ent i
n 3
case
s. C
hina
. Pr
act M
ed (B
arc)
200
8;13
:137
–8.
35 &
45,
mal
es 3
0,
fem
ale
Cerv
ical
spo
ndylo
sis
Cerv
ical
site
Fain
ting
Reco
very
Certa
inly
Kang
YH.
Stro
ke a
fter a
cupu
nctu
re: fi
rst-
aid
care
and
less
on. J
ilin M
ed In
f 199
4;7:
29.
72, f
emal
eAr
m p
ain,
rh
eum
atoi
d ar
thrit
isLI
4, L
I10,
LI1
1, S
J3St
roke
Reco
very
Prob
ably
Feng
B, H
uang
YX.
Adv
erse
eve
nts
afte
r im
prop
er a
cupu
nctu
re. J
Clin
Acu
M
oxib
ustio
n 19
96;1
2:42
.65
, mal
eSt
roke
-rel
ated
he
mip
legi
aGB
20, C
V23
Stro
keRe
cove
ryPr
obab
ly
Mi J
. Rec
urre
nt c
ereb
ral h
aem
orrh
age
caus
ed b
y ac
upun
ctur
e. H
eilo
ngjia
ng J
Trad
Ch
in M
ed 1
993;
2:34
.73
, mal
eSe
quel
a of
cer
ebra
l ha
emor
rhag
eLI
4, L
I11,
ST3
6, e
tc.
Cere
bral
ha
emor
rhag
eDe
ath
Prob
ably
Song
QL,
Wu
TY. T
hree
ther
apeu
tic a
cupu
nctu
re e
rrors
. Clin
Misd
iag
Mist
her
2001
;14:
73.
58, m
ale
Sequ
ela
of c
ereb
ral
haem
orrh
age
KI1
Cere
bral
ha
emor
rhag
eDe
ath
Prob
ably
Zhou
TQ,
Zha
ng H
Y. Ac
upun
ctur
e-in
duce
d fa
tal h
aem
orrh
agic
stro
ke. X
injia
ng J
Trad
Ch
in M
ed 1
985;
4:24
–5.
59, m
ale
Sequ
ela
of s
troke
EX-H
N5, G
V20,
GB
20Ce
rebr
al
haem
orrh
age
Deat
hPr
obab
ly
Ma
ZH. A
cupu
nctu
re-in
duce
d ca
rdia
c ar
rest
. Heb
ei J
Trad
Chi
n M
ed 2
005;
27:5
89.
28, m
ale
Tic
doul
oure
uEX
-HN5
, LI4
, SJ5
Card
iac
arre
stRe
cove
ryPr
obab
lyZh
ang
CY, Z
heng
SM
, Pei
YF.
Acci
dent
al in
jury
to in
tern
al o
rgan
s ca
used
by
impr
oper
ac
upun
ctur
e in
5 c
ases
. Hei
long
jiang
J Tr
ad C
hin
Med
199
2;1:
38.
39, m
ale
Asth
ma
BL13
Shoc
kRe
cove
ryCe
rtain
ly
Wan
g L.
Acu
punc
ture
-indu
ced
petit
mal
epi
leps
y. Ch
in A
cu M
oxib
ustio
n 20
04;S
1:96
.35
, mal
eCh
eira
lgia
Pain
ful s
pot
Pykn
olep
syRe
cove
ryPr
obab
lyGa
n ZZ
. Acu
punc
ture
at T
aiya
ng p
oint
cau
sed
seve
re o
rbita
l hae
mor
rhag
e. C
hin
J Oc
ular
Trau
ma
Occu
p Ey
e Di
s 20
00;2
2:24
6.46
, fem
ale
Cold
, hea
dach
eEX
-HN5
Orbi
tal
haem
orrh
age
Reco
very
Prob
ably
Li J
S. A
cupu
nctu
re-in
duce
d fe
ver.
Chin
Acu
Mox
ibus
tion
2000
;10:
639.
52, m
ale
Sequ
ela
of b
rain
co
ncus
sion
GV20
, GB2
0, L
I11,
LI
4, e
tc.
Feve
rRe
cove
ryPr
obab
ly
Shan
g YT
. Adv
erse
eve
nts
caus
ed b
y ac
upun
ctur
e in
2 c
ases
. New
J Tr
ad C
hin
Med
20
06;3
8:76
.65
, fem
ale
Faci
ople
gia
GB14
, LI4
Coug
hRe
cove
ryPr
obab
ly46
, fem
ale
Obes
ityST
25, S
P15
Thirs
tRe
cove
ryCe
rtain
lyW
ang
SF, L
an Y
H. A
cupu
nctu
re a
t Nei
guan
poi
nt c
ause
d su
dden
aph
onia
. New
Chi
n M
ed 1
980;
11:5
87–8
.36
, fem
ale
46, m
ale
Hicc
ups
PC6
Apho
nia
Reco
very
Prob
ably
Li M
. Acu
punc
ture
at H
ouxi
poin
t cau
sed
left
low
er e
xtre
mity
num
bnes
s. J
Sha
nxi
Trad
Chi
n M
ed C
oll 1
994;
1:37
.47
, fem
ale
Scia
tica
SI3
Leg
num
bnes
s–
Prob
ably
Yang
XH,
Zha
ng G
S. L
ong-
term
acu
punc
ture
at G
uany
uan
poin
t cau
sed
sexu
al
dysf
unct
ion
in 2
men
with
obe
sity.
Chi
n J
Hum
Sex
200
9;18
:19–
20.
52, m
ale
41, f
emal
eSi
mpl
e ob
esity
CV4
Sexu
al d
ysfu
nctio
nRe
cove
ryPr
obab
ly

Bull World Health Organ 2010;88:915–921C | doi:10.2471/BLT.10.076737 919
Junhua Zhang et al. Review of acupuncture-related adverse events in ChinaResearch
All patients recovered after appropriate treatment.
Infections were mainly due to poor sterilization of acupuncture needles. Acupoints on the head became infected most often, perhaps because hair makes it difficult to implement aseptic technique. Two cases of facial abscess may have been caused by acupuncture to relieve toothache.
Other adverse eventsA total of 172 acupuncture-related adverse events that were neither due to trauma nor to infection were reported. Local allergic reactions occurred after acupuncture in four patients with an al-lergy to metal needles.
In our review, fainting was the most common adverse event associated with acupuncture, and it occurred primarily in patients receiving acupuncture for the first time. In total, 150 cases of fainting were reported. In one report of 82 cases, 60% (49) of the patients fainted during the first treatment. Of these 49 fainting spells, 83% occurred when acupuncture was being applied to the head or neck.
Stroke after acupuncture was re-ported in five patients (aged from 58 to 73 years). One case of stroke occurred in a 72-year-old woman who received acupuncture on her arm. The other four patients had a history of stroke and hyper-tension. Three patients died from cerebral haemorrhage that was considered to be causally related to the acupuncture.
Other adverse effects included cardi-ac arrest, pyknolepsy (epileptiform attacks resembling petit mal), shock, fever, cough, thirst, aphonia, leg numbness and sexual dysfunction. However, the existence of a causal link between acupuncture and these adverse events is uncertain.
DiscussionMany types of acupuncture-related ad-verse events have been identified in the Chinese literature. Injuries and infections appear to be related to inappropriate technique, whereas other types of adverse events are not. Fainting is vasovagal in origin and minor bleeding is sometimes inevitable.
Infections result primarily from poor aseptic procedure and insufficient knowledge on the part of acupuncturists, who often disinfect reusable acupuncture needles with alcohol instead of steril-izing them. The use of disposable sterile
acupuncture needles and guide tubes is strongly recommended.12
Most traumatic events are caused by improper manipulation in high-risk acupoints. The depth of needle insertion is crucial. The lung surface is about 10 to 20 mm beneath the skin in the region of the medial scapular or midclavicular line.2 This may explain the high incidence of pneumothorax during needling in this area. Other traumatic complications, such as subarachnoid haemorrhage, car-diovascular injuries or perforation of the gallbladder, can also be caused by exces-sively deep needle insertion.
The patient’s condition also needs to be considered. Cardiovascular trauma occurred most frequently in patients with cardiomegaly. Patients with abdominal pain that has no clear diagnosis are at increased risk of trauma or infection from acupuncture at abdominal acupoints. Symptomatic treatment of abdominal pain with acupuncture can also delay effective therapy. During needling at pe-ripheral acupoints on the legs, arms and face, manipulation should be carefully executed to avoid damaging nerves and blood vessels.
Some adverse events are inevitable but could be minimized through pre-ventive measures. Fainting, which is a reflex caused by vagal excitation, is the most common adverse event during acu-puncture.13 Its incidence can be reduced by preparing patients and positioning them properly; the patient should not be hungry or tired and should preferably be placed in the supine, lateral or prone position.
Of the 87 articles reporting traumatic events, 59 (70%) provided information about the acupuncturists. Of these 59 articles, 68% (40) indicated that the acupuncturists were practising in village clinics or rural hospitals when they per-formed the procedures that caused the traumatic events. All infections reported were caused by acupuncturists in rural areas. In China, acupuncturists in rural and urban hospitals have a great disparity in clinical skills. Acupuncturists practising in rural hospitals, township health centres or village clinics rarely receive formal edu-cation in medical colleges. It follows that training for the practice of acupuncture needs to be unified and improved.
Several serious adverse events were identified through a review of case re-ports,14 but very few were found in surveys7–9 or prospective observational
Refe
renc
eaCa
sesb (
age
in
year
s an
d se
x, o
r no
. of c
ases
)
Reas
on fo
r ac
upun
ctur
eAc
upoi
nt
(cod
ec or s
ite)
Adve
rse
even
tOu
tcom
eCa
used
by
ac
upun
ctur
e?
Zhan
g RM
. Mis
use
of a
cupu
nctu
re in
2 c
ases
. Jia
ngxi
J Tr
ad C
hin
Med
199
2;23
:47.
20, m
ale
Head
ache
KI1
Sper
mat
orrh
eaRe
cove
ryPr
obab
lyLa
n XL
, Du
XH. A
llerg
ic s
kin
rash
indu
ced
by a
cupu
nctu
re. J
Yun
yang
Med
Col
l 20
04;2
3:37
8.50
, mal
eCe
rvic
al s
pond
ylosi
sGB
20, e
tcSk
in ra
shRe
cove
ryCe
rtain
ly
Chen
g C.
Acu
punc
ture
cau
sed
wid
espr
ead
alle
rgic
ery
them
a. J
iang
xi J
Trad
Chi
n M
ed 1
988;
2:52
.11
, fem
ale
Coxa
rthrit
isBL
57, B
L40
Met
al a
llerg
yRe
cove
ryCe
rtain
ly
Guo
YJ. A
llerg
y to
met
al n
eedl
es in
2 c
ases
. Chi
n Ac
u M
oxib
ustio
n 20
06;2
6:30
7–8.
33 &
52,
fem
ales
Abdo
min
al p
ain
–M
etal
alle
rgy
Reco
very
Certa
inly
a All
refe
renc
es in
this
tabl
e ar
e in
Chi
nese
. The
Eng
lish-
lang
uage
pap
er a
nd jo
urna
l titl
es a
re fr
ee tr
ansl
atio
ns. T
he o
rigin
al C
hine
se-la
ngua
ge ti
tles
can
be o
btai
ned
from
the
corre
spon
ding
aut
hor.
b Onl
y ca
ses
of tr
aditi
onal
nee
dle
acup
unct
ure
are
incl
uded
. Thi
s ex
plai
ns a
ny d
iscr
epan
cy b
etw
een
the
num
ber o
f cas
es in
this
col
umn
and
the
title
of t
he c
orre
spon
ding
refe
renc
e.
c R
efer
ence
s 10
and
11.

Bull World Health Organ 2010;88:915–921C | doi:10.2471/BLT.10.076737920
Junhua Zhang et al.Review of acupuncture-related adverse events in ChinaResearch
studies.5,6 This suggests that serious acu-puncture-related adverse events are rare. Bleeding and pain during needling are re-ported less often in the Chinese-language than in the English-language literature, perhaps because practitioners in China consider such events too trivial to report. Infections (primarily hepatitis) after acu-puncture are reported frequently in the English-language literature1 but relatively rarely in the Chinese-language literature, even though non-disposable acupuncture needles are still used in China. It is pos-sible that in China acupuncture-related infections are underreported.
Of the 87 articles reporting traumatic injuries, 72 (about 70%) were authored not by the acupuncturists themselves, but by the physicians who treated the adverse events. None of the articles reporting infec-tions were authored by the acupuncturists, as opposed to 16 of the 20 (80%) reports of adverse events other than trauma or infection. Again, we suspect that under-
reporting of such events in the Chinese-language literature is much higher than in the English-language literature.
Our review has several limitations. Although our search strategy was compre-hensive, we cannot guarantee that all rel-evant articles were identified. Many of the reports lacked detail, so that cause–effect relationships are often uncertain. In the absence of a denominator (i.e. the total number of acupuncture treatments prac-tised over the study period), the reported adverse events do not lend themselves to generating incidence figures. There are 2688 hospitals of traditional Chinese medicine in China.15 If we assume, for instance, that each hospital receives 50 to 100 visits for acupuncture per day (a con-servative figure), the annual number of acupuncture treatments would total from 50 to 100 million. This would suggest that the incidence of acupuncture-related adverse events is negligible. However, the true incidence remains unknown and can-
not be accurately estimated. Collectively these factors limit the conclusiveness of our findings.
ConclusionVarious types of acupuncture-related adverse events have been reported in China. Similar events have been reported by other countries,1–9 usually as a result of inappropriate technique. Acupuncture can be considered inherently safe in the hands of well trained practitioners. How-ever, there is a need to find effective ways to improve the practice of acupuncture and to monitor and minimize the health risks involved. ■
AcknowledgementsThe authors thank YY Xu, X Zhang and WK Zheng for their help with the litera-ture search.
Competing interests: None declared.
ملخصاآلثار الضائرة املرتبطة بالوخز اإلبري: مراجعة نظامية لألدبيات الصينية
بالوخز املرتبطة الضائرة اآلثار الصينية حول اللغة أدبيات مراجعة الغرض اإلبري مراجعة نظامية
وهي صينية بيانات قواعد ثالث يف بالبحث الباحثون قام الطريقة وقاعدة 1980-2009؛ الصينية، البيولوجية الطبية األدبيات بيانات )قاعدة بيانات وقاعدة 1980-2009؛ الصينية، للمجالت الكاملة النصوص بيانات جريدة ويبو Weipu، 1989-2009(، من أجل تحديد املقاالت الواردة فيها البحث تضمن ولقد التقليدي. اإلبري الوخز سالمة حول الصينية باللغة تقارير حالة، وسلسلة للحاالت، مع مسوحات وسائر الدراسات القامئة عىل املراقبة، حال احتوائها عىل معطيات واقعية، وقد استبعدت مقاالت املراجعة،
واملقاالت املرتجمة والتجارب الرسيرية.املجودات لبت 115 مقالة معايري اإلدراج يف الدراسة )98 تقارير حالة، و17 سلسلة من الحاالت( واشتملت عىل إجاميل 479 حالة تعرضت لآلثار
اآلثار ولقد صنفت مريضا. 14 وتويف اإلبري، الوخز استخدام بعد الضائرة الضائرة املرتبطة بالوخز اإلبري إىل ثالث فئات: رضحي، ومعٍد، وأخرى. وكانت أكرث اآلثار الضائرة تكراراً عىل اإلطالق اسرتواح الصدر، واإلغامء، والنزف تحت العنكوبتية، والعدوى، بينام كانت اآلثار األكرث تفاقام هي تلك التي ارتبطت الصدر، واسرتواح العنكوبتية، تحت والنزف الوعائية، القلبية باإلصابات
وتكرار النزف الدماغي.العديد من األحداث الصينية املنشورة عىل االستنتاج احتوت األدبيات الخاصة باآلثار الضائرة املرتبطة بالوخز اإلبري، وكان أكرثها يعود إىل استخدام التقنية الخاطئة. ومن ثم، يتوجب بذل الجهود من أجل إيجاد طرق فعالة
للمراقبة والرصد وتقليص املخاطر املرتبطة بالوخز اإلبري.
Resumé
Événements indésirables liés à l’acupuncture: une évaluation systématique de la documentation chinoiseObjectif Évaluer systématiquement la documentation en langue chinoise sur les événements indésirables liés à l’acupuncture.Méthodes Nous avons fait des recherches dans trois bases de données chinoises (la base de données sur la documentation biomédicale chinoise, 1980–2009, la base de données en texte intégral du Journal chinois, 1980–2009 et la base de données de la revue Weipu, 1989–2009) afin d’identifier les articles en langue chinoise qui abordent le thème de la sécurité de l’acupuncture traditionnelle pratiquée avec des aiguilles. Les observations, les séries de cas, les enquêtes et d’autres études d’observation ont été prises en compte lorsqu’elles rapportaient des données factuelles, mais les articles, les traductions et les essais cliniques ont été exclus.Résultats Les critères d’inclusion concernaient 115 articles (98 observations et 17 séries de cas) qui signalaient au total 479 cas
d’événements indésirables après acupuncture. Quatorze patients étaient décédés. Les événements indésirables liés à l’acupuncture étaient classés en trois catégories : traumatiques, infectieux et «autres». Les événements indésirables les plus fréquents étaient le pneumothorax, l’évanouissement, l’hémorragie méningée et l’infection, les plus graves étant les lésions cardiovasculaires, l’hémorragie méningée, le pneumothorax et l’hémorragie cérébrale récurrente.Conclusion De nombreux événements indésirables liés à l’acupuncture, dont la majorité était due à une technique incorrecte, ont été décrits dans la documentation chinoise publiée. Des efforts sont indispensables afin de trouver des moyens efficaces de contrôler et de réduire les risques liés à l’acupuncture.

Bull World Health Organ 2010;88:915–921C | doi:10.2471/BLT.10.076737 921
Junhua Zhang et al. Review of acupuncture-related adverse events in ChinaResearch
Resumen
Acontecimientos adversos relacionados con la acupuntura: revisión sistemática de la bibliografía chinaObjetivo Realizar una revisión sistemática de la bibliografía en chino sobre los acontecimientos adversos relacionados con la acupuntura.Métodos Se realizaron búsquedas en tres bases de datos chinas (Biomedical Literature Database, 1980–2009; Chinese Journal Full-Text Database, 1980–2009 y Weipu Journal Database, 1989–2009) con el fin de identificar los artículos en lengua china sobre la seguridad de la acupuntura tradicional con agujas. Se incluyeron casos clínicos, series de casos, encuestas y otros estudios de observación que presentaran datos documentados, pero se excluyeron los artículos de revisión, las traducciones y los ensayos clínicos.Resultados Los criterios de inclusión se cumplieron en 115 artículos (98 casos clínicos y 17 series de casos) que, en total, informaron sobre
479 casos de efectos adversos tras la acupuntura. Catorce pacientes fallecieron. Los acontecimientos adversos relacionados con la acupuntura fueron clasificaron en tres categorías: traumáticos, infecciosos y «otros». Los acontecimientos adversos más frecuentes fueron: neumotórax, desmayo, hemorragia subaracnoidea e infección; mientras que los más graves fueron: lesiones cardiovasculares, hemorragia subaracnoidea, neumotórax y hemorragia cerebral recurrente.Conclusión En la bibliografía china publicada se han descrito muchas reacciones adversas relacionadas con la acupuntura, debidas en su mayor parte a una técnica inadecuada. Debemos esforzarnos para encontrar formas eficaces de controlar y reducir al mínimo los riesgos relacionados con la acupuntura.
References1. Norheim AJ. Adverse effects of acupuncture: a study of the literature for the
years 1981–1994. J Altern Complement Med 1996;2:291–7. doi:10.1089/acm.1996.2.291 PMID:9395661
2. Peuker ET, White A, Ernst E, Pera F, Filler TJ. Traumatic complications of acupuncture. Therapists need to know human anatomy. Arch Fam Med 1999;8:553–8. doi:10.1001/archfami.8.6.553 PMID:10575398
3. Yamashita H, Tsukayama H, White AR, Tanno Y, Sugishita C, Ernst E. Systematic review of adverse events following acupuncture: the Japanese literature. Complement Ther Med 2001;9:98–104. doi:10.1054/ctim.2001.0446 PMID:11444889
4. Ernst E, Sherman KJ. Is acupuncture a risk factor for hepatitis? Systematic review of epidemiological studies. J Gastroenterol Hepatol 2003;18:1231–6. doi:10.1046/j.1440-1746.2003.03135.x PMID:14535978
5. Endres HG, Molsberger A, Lungenhausen M, Trampisch HJ. An internal standard for verifying the accuracy of serious adverse event reporting: the example of an acupuncture study of 190,924 patients. Eur J Med Res 2004;9:545–51. PMID:15689300
6. Witt CM, Pach D, Brinkhaus B, Wruck K, Tag B, Mank S et al. Safety of acupuncture: results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forsch Komplementmed 2009;16:91–7. doi:10.1159/000209315 PMID:19420954
7. Norheim AJ, Fønnebø V. Acupuncture adverse effects are more than occasional case reports: Results from questionnaires among 1135 randomly selected doctors, and 197 acupuncturists. Complement Ther Med 1996;4:8–13. doi:10.1016/S0965-2299(96)80049-5
8. White A, Hayhoe S, Hart A, Ernst E. Adverse events following acupuncture: prospective survey of 32 000 consultations with doctors and physiotherapists. BMJ 2001;323:485–6. doi:10.1136/bmj.323.7311.485 PMID:11532840
9. Macpherson H, Scullion A, Thomas KJ, Walters S. Patient reports of adverse events associated with acupuncture treatment: a prospective national survey. Qual Saf Health Care 2004;13:349–55. doi:10.1136/qshc.2003.009134 PMID:15465938
10. A proposed standard international acupuncture nomenclature: report of a WHO scientific group. Geneva: World Health Organization; 1991.
11. WHO standard acupuncture point locations in the Western Pacific Region. Geneva: World Health Organization; 2008.
12. Guidelines on basic training and safety in acupuncture. Geneva: World Health Organization; 1999.
13. He J, Tang QF, Zhuang LX. Clinical analysis of the therapeutic effect of fainting during acupuncture and preliminary study of the mechanism. Chin Acu Moxibustion 2004;24:553–5.
14. Lao L, Hamilton GR, Fu J, Berman BM. Is acupuncture safe? A systematic review of case reports. Altern Ther Health Med 2003;9:72–83. PMID:12564354
15. Ministry of Health of the People’s Republic of China [Internet]. Beijing: Ministry of Health; 2010. Available from: http://www.moh.gov.cn [accessed 11 August 2010]. Chinese.

ABull World Health Organ 2;87:fpage–lpage | doi:10.2471/BLT.07.043125
Junhua Zhang et al. Review of acupuncture-related adverse events in ChinaResearch
Tabl
e 1.
Tra
umat
ic e
vent
s af
ter a
cupu
nctu
re, a
s id
entifi
ed th
roug
h a
syst
emat
ic re
view
of t
he C
hine
se-l
angu
age
liter
atur
e, 1
980–
2009
Body
site
and
refe
renc
eaAd
vers
e ev
ent (
no. o
f ca
sesb )
Acup
oint
(cod
ec or
site
)Ou
tcom
e
Spin
al c
ord
and
neig
hbou
ring
tissu
esBa
o LP
, Gao
CT.
Suba
rach
noid
hae
mor
rhag
e af
ter a
cupu
nctu
re a
t Fen
gchi
and
Yam
en p
oint
s in
3 c
ases
. Jilin
Med
J 1
983;
4:45
–6.
Suba
rach
noid
hae
mor
rhag
e (3
5 ca
ses)
GB20
, GV1
5,
GV16
, GV1
4, B
L10
3 de
aths
; 32
reco
verie
sBi
an F,
Zha
ng X
L, T
ian
SP. A
cupu
nctu
re a
t Fen
gchi
poi
nt c
ause
d su
bara
chno
id h
aem
orrh
age.
J Z
hang
jiako
u M
ed C
olle
ge 1
997;
14:7
3.Ch
en Y
Z, H
uang
WC.
Acu
punc
ture
at n
eck
poin
ts c
ause
d su
bara
chno
id h
aem
orrh
age.
Sha
nxi T
rad
Chin
Med
J 1
985;
1:47
–8.
Chen
MX.
Acu
punc
ture
at Y
amen
poi
nt c
ause
d su
bara
chno
id h
aem
orrh
age.
J P
ract
Int M
ed 1
987;
7:35
5.Ji
ang
TZ, C
hen
WD,
Zha
ng B
, et a
l. Su
bara
chno
id h
aem
orrh
age
in 2
cas
es a
fter a
cupu
nctu
re a
t the
nap
e. J
Anh
ui Tr
ad C
hin
Med
Col
l 199
6;15
:48.
Li L
F, Co
ng X
, Jin
QW
. Acu
punc
ture
at F
engf
u po
int c
ause
d su
bara
chno
id h
aem
orrh
age.
Chi
n Ac
u M
oxib
ustio
n 20
08;2
8:29
2.Li
u SX
. Acu
punc
ture
at F
engc
hi p
oint
cau
sed
suba
rach
noid
hae
mor
rhag
e. S
hanx
i Med
J 1
980;
9:53
.Li
u ZH
, Xia
o HP
, Liu
JS,
et a
l. Su
bara
chno
id h
aem
orrh
age
in 1
2 ca
ses
afte
r acu
punc
ture
at n
ape.
Peo
ple’
s M
il Su
rg 1
984;
12:5
1–2.
Liu
FY. A
cupu
nctu
re a
t Fen
gchi
poi
nt c
ause
d su
bdur
al h
aem
atom
a. M
ed J
Lia
onin
g 19
92;6
:25.
Mi X
H, L
i SK,
Jia
SK.
Acu
punc
ture
at Y
amen
poi
nt c
ause
d su
bara
chno
id h
aem
orrh
age.
Sha
ndon
g J
Trad
Chi
n M
ed 1
989;
8:22
.Ni
u LJ
, Zha
ng R
W. A
cupu
nctu
re-in
duce
d ha
emor
rhag
e in
the
cist
erna
mag
na. P
rac
J M
ed P
harm
200
6;23
:932
.Su
Y, C
hen
HX, C
hen
CC, e
t al.
Acup
unct
ure
at Y
amen
poi
nt c
ause
d su
bara
chno
id h
aem
orrh
age.
Sha
ngha
i J A
cu M
oxib
ustio
n 19
85;3
:22.
Wu
BS, X
u QZ
. One
dea
th fr
om s
pina
l cor
d in
jury
afte
r acu
punc
ture
at A
sh a
cupo
ints
in th
ird c
ervic
al v
erte
bra.
Chi
nJ F
oren
sic M
ed 1
990;
5:32
–3.
Yang
YD,
Shi
R, G
e SH
. Sub
arac
hnoi
d ha
emor
rhag
e ca
used
by
acup
unct
ure.
Lia
onin
g J
Trad
Chi
n M
ed 1
985;
8:37
.Yu
BR.
Acu
punc
ture
at n
ape
poin
ts c
ause
d su
bara
chno
id h
aem
orrh
age
in 7
cas
es. J
Apo
plex
y Ne
rv D
is 19
86;3
:74–
5.Zh
ou J
W. A
cupu
nctu
re a
t Fen
gchi
poi
nt c
ause
d on
e de
ath.
J S
ichua
n Tr
ad C
hin
Med
198
8;10
:52.
Li Y
Q, C
hen
GW. A
cupu
nctu
re c
ause
d ep
idur
al h
aem
orrh
age
in c
ervic
al s
pine
. Chi
n Co
mm
Doc
tors
200
3;19
:46–
7.Sp
inal
epi
dura
l hae
mat
oma
(9 c
ases
)–
9 re
cove
ries
Liu
FY. A
cupu
nctu
re a
t Fen
gchi
poi
nt c
ause
d su
bdur
al h
aem
atom
a. M
ed J
Lia
onin
g 19
92;6
:25.
Zhan
g J.
Dia
gnos
is a
nd tr
eatm
ent o
f spi
nal e
pidu
ral h
aem
atom
a ca
used
by
acup
unct
ure.
Mod
Med
Hea
lth 2
006;
22:2
924–
5.Ab
dom
inal
org
ans
and
tissu
esZh
ang
JH. A
cupu
nctu
re a
t abd
omin
al a
cupo
ints
cau
sed
4 ca
ses
of p
erito
nitis
. Chi
n Ru
ral D
octo
r 199
7;4:
20–1
.Pe
riton
itis
(2 c
ases
)–
Reco
very
Zhen
g BS
, Zha
o M
L. L
esso
ns fr
om 2
cas
es o
f gal
lbla
dder
per
fora
tion
com
plic
ated
with
bile
per
itoni
tis c
ause
d by
acu
punc
ture
. Chi
n J
Clin
198
3;3:
44.
Wu
DP, H
e RL
. Gal
lbla
dder
per
fora
tion
com
plic
ated
with
bile
per
itoni
tis, 2
cas
es c
ause
d by
acu
punc
ture
. Sha
nxi J
Trad
Chi
n M
ed 1
981;
S1:4
4.Ba
i XF.
Acup
unct
ure-
indu
ced
gallb
ladd
er p
erfo
ratio
n w
ith b
ile p
erito
nitis
. Inn
er M
ongo
lia M
ed J
199
1;11
:80.
Liu
JC, L
iu H
Y. Ga
llbla
dder
per
fora
tion,
2 c
ases
cau
sed
by a
cupu
nctu
re. C
hin
J Ba
ses
Clin
Gen
Sur
g 20
01;8
:226
.Pe
rfora
ted
gallb
ladd
er
(7 c
ases
, 5 w
ith p
erito
nitis
)ST
25, C
V12
Reco
very
Duan
QL,
Wan
g SR
. Sev
ere
com
plic
atio
ns c
ause
d by
acu
punc
ture
in 3
cas
es. H
ebei
J Tr
ad C
hin
Med
198
4;1:
36–7
.In
test
inal
per
fora
tion
(5 c
ases
, al
l with
per
itoni
tis)
–Re
cove
ry
Wan
g M
Y. Se
rious
con
sequ
ence
s of
acu
punc
ture
at a
bdom
inal
acu
poin
ts in
2 c
ases
. Peo
ple’
s. M
il Su
rg 1
985;
6:61
–2.
Zhan
g JH
. Acu
punc
ture
at a
bdom
inal
acu
poin
ts c
ause
d 2
case
s of
per
itoni
tis. C
hin
Rura
l Doc
tor 1
997;
4:20
–1.
Xiao
XT.
Gast
ric p
erfo
ratio
n ca
used
by
acup
unct
ure.
Chi
n J
Clin
198
5;1:
9.Ga
stric
per
fora
tion
(1 c
ase,
w
ith p
erito
nitis
)CV
12Re
cove
ry
Liu
WG,
Dua
n LJ
, Sun
DT.
Acup
unct
ure
at T
ians
hu p
oint
cau
sed
inte
stin
al o
bstru
ctio
n. C
hin
J In
t Tra
d W
est M
ed 1
992;
3:14
7.In
test
inal
wal
l hae
mat
oma
with
obs
truct
ion
(1 c
ase)
ST25
Reco
very

B Bull World Health Organ 2;87:fpage–lpage | doi:10.2471/BLT.07.043125
Junhua Zhang et al.Review of acupuncture-related adverse events in ChinaResearch
Body
site
and
refe
renc
eaAd
vers
e ev
ent (
no. o
f ca
sesb )
Acup
oint
(cod
ec or
site
)Ou
tcom
e
Thor
acic
org
ans
and
tissu
esCh
ang
JY. A
cupu
nctu
re a
t bac
k ac
upoi
nts
caus
ed h
aem
opne
umot
hora
x. H
ebei
J Tr
ad C
hin
Med
198
4;3:
48.
Pneu
mot
hora
x (2
01 c
ases
)GB
21, B
L13,
BL
18, B
L23,
LI1
7,
ST12
, CV2
2,
CV15
, CV1
4, S
I9,
SI13
4 de
aths
; 197
re
cove
ries
Ding
WY.
Acup
unct
ure
at c
hest
and
bac
k po
ints
cau
sed
10 c
ases
of t
raum
atic
pne
umot
hora
x. C
entra
l Pla
ins
Med
J 1
986;
4:39
.Du
JY.
Repo
rt of
10
case
s of
pne
umot
hora
x ca
used
by
acup
unct
ure.
Cen
tral P
lain
s M
ed J
198
1;2:
22.
Duan
QL,
Wan
g SR
. Les
sons
from
3 c
ases
of s
ever
e co
mpl
icat
ions
of a
cupu
nctu
re. H
ebei
J T
rad
Chin
Med
198
4;1:
36–7
.Ga
o CG
. Tw
o ca
ses
of b
ilate
ral p
neum
otho
rax
caus
ed b
y ac
upun
ctur
e. J
Pra
ct M
ed 1
984;
3:38
–9.
Hu D
R. T
raum
atic
pne
umot
hora
x ca
used
by
acup
unct
ure
in 7
cas
es. J
iang
xi J
Trad
Chi
n M
ed 1
981;
4:29
–30.
Hu Q
X, Z
hang
HY.
Acup
unct
ure
caus
ed 9
cas
es o
f tra
umat
ic p
neum
otho
rax.
Clin
Med
(Nor
thfie
ld, I
L) 1
987;
7:33
1–3.
Hu Y
A. A
cupu
nctu
re a
t che
st a
cupo
ints
cau
sed
13 c
ases
of p
neum
otho
rax:
X-r
ay d
iagn
osis
and
ana
lysis
. Nei
Mon
gol J
Trad
Chi
n M
ed 1
995;
S1:5
1.Ji
ang
DG. A
cupu
nctu
re a
t Jiu
wei
poi
nt c
ause
d pn
eum
otho
rax.
Cho
ngqi
Med
J 1
980;
6:47
.Ji
n BR
. Acu
punc
ture
at Q
uyua
ni p
oint
cau
sed
pneu
mot
hora
x. S
hang
hai J
Acu
Mox
ibus
tion
1987
;3:4
5.Ji
n PL
. Acu
punc
ture
-rel
ated
acc
iden
ts a
nd th
eir p
reve
ntio
n. C
hin
J Pr
act C
hin
Mod
Med
200
5;8:
765.
Li Y
C. C
linic
al a
nalys
is o
f 25
case
s of
acu
punc
ture
-indu
ced
pneu
mot
hora
x. C
hin
Com
m D
octo
rs 1
995;
12:3
7–8.
Li Y
Y, Ch
eng
XL. O
ne c
ase
of p
neum
otho
rax
caus
ed b
y ac
upun
ctur
e. J
Han
dan
Med
Col
l 199
7;10
:72–
3.Li
u LY
. One
cas
e of
hae
mop
neum
otho
rax
caus
ed b
y ac
upun
ctur
e. J
Cha
ngch
un U
niv T
rad
Chin
Med
200
7;23
:58.
Lu B
, Tia
n XH
. One
cas
e of
trau
mat
ic te
nsio
n pn
eum
otho
rax
caus
ed b
y ex
cess
ively
deep
acu
punc
ture
. Gui
zhou
Med
J 1
993;
17:1
25.
Ma
WT.
Anal
yses
of 1
4 ca
ses
of tr
aum
atic
pne
umot
hora
x in
duce
d by
acu
punc
ture
. Anh
ui M
ed J
199
3;14
:41.
Ma
L, Z
hang
CJ.
Clin
ical
ana
lysis
of a
cupu
nctu
re-in
duce
d pn
eum
otho
rax.
J C
lin A
cu M
oxib
ustio
n 19
97;1
3:40
.M
a BZ
. Acu
punc
ture
-indu
ced
traum
atic
pne
umot
hora
x in
one
cas
e. Q
ingh
ai M
ed J
200
7;37
:41.
Ou Q
, Ji J
C. A
cupu
nctu
re a
t sho
ulde
r acu
poin
ts c
ause
d 5
case
s of
pne
umot
hora
x. J
Trad
Chi
n Or
thop
Trau
mat
ol 1
997;
9:54
.Qi
n M
X, A
o W
H. Im
prop
er a
cupu
nctu
re c
ause
d pn
eum
otho
rax.
Clin
Misd
iag
Mist
her 2
003;
16:7
6.Ru
an K
Y, Qi
KJ,
Mou
ZC.
Acu
punc
ture
at p
oint
s in
sup
racl
avic
ular
foss
a ca
used
hyd
ropn
eum
otho
rax.
New
J Tr
ad C
hin
Med
199
2;4:
33.
Shi Y
K. L
esso
ns fr
om 3
8 ca
ses
of p
neum
otho
rax
caus
ed b
y ac
upun
ctur
e. P
eopl
e’s.
Mil
Surg
198
0;10
:53.
Song
BZ,
Xu
JS. O
ne c
ase
haem
opne
umot
hora
x ca
used
by
acup
unct
ure
at le
ft Ji
anjin
poi
nt. J
Anh
ui Tr
ad C
hin
Med
Col
l 198
7;6:
45.
Song
QL,
Wu
TY. T
hree
ther
apeu
tic e
rrors
of a
cupu
nctu
re. C
lin M
isdia
g M
isthe
r 200
1;14
:73.
Wan
g DS
. Acu
punc
ture
at e
piga
striu
m c
ause
d pl
eura
l effu
sion
. Peo
ple’
s. M
il Su
rg 1
982;
10:7
3.W
ang
YL. O
ne d
eath
from
pne
umot
hora
x ca
used
by
acup
unct
ure
at b
ilate
ral T
iand
ing
poin
ts. J
For
ensic
Med
199
9;15
:47–
8.Xi
a C.
Tre
atin
g ac
upun
ctur
e-in
duce
d ac
cide
nts.
J C
lin A
cu M
oxib
ustio
n 19
93;2
:75–
6.Ya
n ZC
. Acu
punc
ture
at T
iant
u po
int c
ause
d se
vere
pne
umot
hora
x. N
ew C
hin
Med
198
5;16
:655
.Zh
a CH
. Ide
ntifi
catio
n of
hae
mop
neum
otho
rax
afte
r acu
punc
ture
from
pie
rcin
g of
the
left
lung
. Chi
n J
Fore
nsic
Med
200
6;21
:75–
6.Zh
ang
SP. A
cupu
nctu
re c
ause
d ha
emop
neum
otho
rax.
Sha
ngha
i J A
cu M
oxib
ustio
n 19
86;4
:21.
Zhan
g CY
, Zhe
ng S
M, P
ei Y
F. Fi
ve c
ases
of a
ccid
enta
l inj
ury
of in
tern
al o
rgan
s ca
used
by
impr
oper
acu
punc
ture
. Hei
long
jiang
J Tr
ad C
hin
Med
199
2;1:
38.
Zhao
DY,
Zhan
g GL
. Clin
ical
ana
lysis
of 3
8 ca
ses
of p
neum
otho
rax
indu
ced
by a
cupu
nctu
re o
r inj
ectio
n at
acu
poin
t. Ch
in A
cu M
oxib
ustio
n 20
09;2
9:23
9–42
.Zh
eng
PD, P
ang
SH. A
cupu
nctu
re c
ause
d se
vere
hae
mop
neum
otho
rax.
J Tr
ad C
hin
Med
198
3;5:
32.
Zhu
ZH, S
hen
H. A
ccid
enta
l pne
umot
hora
x ca
used
by
acup
unct
ure
ther
apy.
Int J
Em
erg
Crit
Care
Med
200
5;2:
992–
5.Zo
ng W
J. P
neum
otho
rax
caus
ed b
y ac
upun
ctur
e in
5 c
ases
. Sha
ngha
i J A
cu M
oxib
ustio
n 19
84;1
:24.
Yang
ST.
Acup
unct
ure
at F
eish
u po
int c
ause
d ch
yloth
orax
. J C
lin A
cu M
oxib
ustio
n 19
91;4
:19.
Chylo
thor
ax (1
cas
e)BL
13Re
cove
ryHu
o SH
, Tia
n YP
, Ma
QL, e
t al.
Acup
unct
ure
caus
ed c
ardi
ac in
jury
with
pne
umot
hora
x. C
hin
J Cr
it Ca
re M
ed 2
007;
27:9
08.
Righ
t ven
tricu
lar p
unct
ure
(4 c
ases
)CV
15, 2
nd–3
th
ICR
near
ste
rnal
ed
ge; p
reco
rdia
l re
gion
; und
er ri
ght
brea
st
2 de
aths
; 2
reco
verie
sLu
o YZ
, Don
g L,
Yua
n HS
, et a
l. Ac
upun
ctur
e ca
used
pul
sus
tard
us a
nd c
ardi
ac ta
mpo
nade
. Chi
n J
Clin
Tho
rac
Card
iova
sc S
urg
2006
;13:
343.
Zhu
WT,
Li X
S, Z
hang
YT,
et a
l. Ac
upun
ctur
e ca
used
dea
th fr
om c
ardi
ac ru
ptur
e. J
For
ensic
Med
200
8;24
:312
.Xi
e JZ
, Lin
WZ.
Acu
punc
ture
cau
ses
deat
h fro
m c
ardi
ac in
jury
. Chi
n J
Inte
gr Tr
ad W
est M
ed In
t Crit
Car
e 20
03;1
:51.
Zhu
J. A
cupu
nctu
re a
t Qim
en p
oint
indu
ced
deat
h fro
m a
ortic
hae
mor
rhag
e. S
hang
hai J
Acu
Mox
ibus
tion
1990
;2:3
1.Ao
rtic
arte
ry ru
ptur
e (1
cas
e)LR
14De
ath
Gen
JQ. S
ucce
ssfu
l man
agem
ent o
f acu
punc
ture
-indu
ced
coro
nary
arte
ry in
jury
with
acu
te c
ardi
ac ta
mpo
nade
. J C
lin C
ardi
ol 2
005;
21:3
92.
Coro
nary
arte
ry p
unct
ure
with
ca
rdia
c ta
mpo
nade
(1 c
ase)
LU1
Reco
very

CBull World Health Organ 2;87:fpage–lpage | doi:10.2471/BLT.07.043125
Junhua Zhang et al. Review of acupuncture-related adverse events in ChinaResearch
Body
site
and
refe
renc
eaAd
vers
e ev
ent (
no. o
f ca
sesb )
Acup
oint
(cod
ec or
site
)Ou
tcom
e
Neck
are
aZh
u J.
Acu
punc
ture
at T
iant
u po
int c
ause
d on
e de
ath.
Jia
ngsu
J Tr
ad C
hin
Med
198
6;2:
28.
Inju
ry o
f inf
erio
r lar
ynge
al
nerv
e an
d tra
chea
(1 c
ase)
CV22
Deat
h
Gao
LW. A
cupu
nctu
re a
t Fut
u po
int c
ause
d dy
spno
ea. C
hin
J Tr
ad C
hin
Med
Pha
rm 1
989;
2:50
.Vo
cal c
ord
para
lysis
; su
bcut
aneo
us e
mph
ysem
a (1
cas
e)
LI18
Reco
very
Zhou
LZ,
Zha
o DG
, Pen
g L.
Opi
nion
s re
gard
ing
acup
unct
ure-
indu
ced
hoar
sene
ss. S
hang
hai J
Acu
Mox
ibus
tion
2005
;27:
27.
Hoar
sene
ss (1
cas
e)Na
pe a
rea
Reco
very
Yan
BX. A
cupu
nctu
re a
t bra
chia
l ple
xus
caus
ed p
hren
ic n
erve
inju
ry. S
haan
xi J
Trad
Chi
n M
ed 1
994;
15:5
13.
Inju
ry o
f phr
enic
ner
ve
(1 c
ase)
Bico
ngRe
cove
ry
Cai X
J. A
cupu
nctu
re c
ause
d th
yroi
d ca
psul
e ha
emor
rhag
e w
ith a
sphy
xia. M
ed J
Chi
n Pe
ople
’s Li
bera
tion
Arm
y 19
91;6
:494
.Th
yroi
d ha
emor
rhag
e;
infe
ctio
n (1
cas
e)Ne
ck a
rea
Reco
very
Chen
SM
. Acu
punc
ture
cau
sed
traum
atic
car
otid
arte
ry a
neur
ysm
. J Tr
ad C
hin
Med
198
0;7:
49.
Fals
e an
eury
sm o
f car
otid
ar
tery
(1 c
ase)
Neck
are
aRe
cove
ry
Eye
area
Jin
PL. A
dis
cuss
ion
of a
cupu
nctu
re-r
elat
ed a
ccid
ents
and
thei
r pre
vent
ion.
Chi
n J
Prac
t Chi
n M
od M
ed 2
005;
8:76
5.Or
bita
l hae
mor
rhag
e (3
cas
es)
SL1,
EX-
HN7
2 re
cove
ries;
1
Visu
al
impa
irmen
tXu
RZ.
Acu
punc
ture
at J
ingm
ing
poin
t cau
sed
exop
htha
lmos
: pre
vent
ion
and
coun
term
easu
res.
J C
lin A
cu M
oxib
ustio
n 20
03;1
9:22
.Ya
ng G
, Wan
g SL
. Blin
dnes
s ca
used
by
acup
unct
ure.
Tia
njin
J Tr
ad C
hin
Med
199
6;13
:6.
Yang
G, W
ang
SL. B
lindn
ess
caus
ed b
y ac
upun
ctur
e. T
ianj
in J
Trad
Chi
n M
ed 1
996;
13:6
.Tr
aum
atic
cat
arac
t (1
case
)Su
perc
iliary
ac
upoi
nts
Visu
al
impa
irmen
tXu
LH,
Liu
AH.
Ocu
lom
otor
ner
ve in
jury
cau
sed
by a
cupu
nctu
re. C
hin
J Oc
ular
Trau
ma
Occu
p Ey
e Di
s 19
97;1
9:22
6.In
jury
of o
culo
mot
or n
erve
(1
cas
e)ST
1Re
cove
ry
Liu
BS, L
i ZX,
Lei
F. A
cupu
nctu
re-in
duce
d re
tinal
det
achm
ent.
Chin
J O
cula
r Tra
uma
Occu
p Ey
e Di
s 19
88;1
:43–
4.Re
tinal
inju
ry (1
cas
e)Ey
elid
Reco
very
Perip
hera
l ner
ves
and
bloo
d ve
ssel
sDi
ng X
Y, Li
u SY
. Acc
iden
t due
to c
linic
al a
cupu
nctu
re. C
hin
Acu
Mox
ibus
tion
2008
;28:
817–
8.Le
g, h
aem
orrh
age;
dia
betic
fo
ot (1
cas
e)ST
38, B
L57
–
Xia
C. T
reat
ing
acup
unct
ure-
indu
ced
acci
dent
. J C
lin A
cu M
oxib
ustio
n 19
93;2
:75–
6.Ch
eeks
, hae
mat
oma
(1 c
ase)
ST5
Reco
very
Han
LX. A
cupu
nctu
re a
t Lia
nqua
n po
int c
ause
d su
blin
gual
fold
hae
mat
oma.
Sha
ngha
i J A
cu M
oxib
ustio
n 19
94;1
3:10
7.Hy
pogl
ottis
, hae
mat
oma
(2 c
ases
)CV
23Re
cove
ryW
ang
NR. A
cupu
nctu
re a
t Lia
nqua
n po
int c
ause
d su
blin
gual
hae
mat
oma.
J C
lin A
cu M
oxib
ustio
n 19
96;7
:89.
Ou L
S, L
iu D
C, T
ian
LY, e
t al.
Acup
unct
ure
at H
egu
poin
t cau
sed
thum
b ad
duct
ion
defo
rmity
in 1
2 ch
ildre
n. J
Anh
ui Tr
ad C
hin
Med
Col
l 198
9;8:
40.
Addu
ctio
n de
form
ity o
f th
umb
(3 c
ases
)LI
4Re
cove
ry
Wan
g SF
. Acu
punc
ture
at T
aiya
ng p
oint
cau
sed
adve
rse
reac
tions
from
impr
oper
man
ipul
atio
n in
2 c
ases
. Cen
tral P
lain
s M
ed J
198
2;3:
135.
Inab
ility
to c
lose
eye
(1 c
ase)
EX-H
N5Re
cove
ryW
ang
SF. A
cupu
nctu
re a
t Tai
yang
poi
nt c
ause
d ad
vers
e re
actio
ns fr
om im
prop
er m
anip
ulat
ion
in 2
cas
es. C
entra
l Pla
ins
Med
J 1
982;
3:18
5.In
abilit
y to
shu
t mou
th
(1 c
ase)
EX-H
N5Re
cove
ry
Wan
g L.
Acu
punc
ture
at N
eigu
an p
oint
indu
ced
hand
mus
cle
cont
ract
ure.
Sha
ngha
i J A
cu M
oxib
ustio
n 19
91;2
:45.
Palm
ar m
uscl
e co
ntra
ctur
e (2
cas
es)
PC6
Reco
very
Need
ling
site
Feng
B, H
uang
YX.
Adv
erse
eve
nts
caus
ed b
y im
prop
er a
cupu
nctu
re. J
Clin
Acu
Mox
ibus
tion
1996
;12:
42.
Pain
(4 c
ases
)SI
3, L
I11,
han
d ac
upoi
nts
Reco
very
Shi G
P, Ch
en Z
M. A
nalys
is o
f 3 a
ccid
ents
cau
sed
by a
cupu
nctu
re. J
Clin
Acu
Mox
ibus
tion
1994
;10:
38.
Li S
L, C
ui X
M. F
ract
ured
acu
punc
ture
nee
dle
caus
ed in
tra-a
bdom
inal
lum
p. S
hang
hai J
Acu
Mox
ibus
tion
1992
;3:3
2.Br
oken
nee
dle
(1 c
ase)
–Re
cove
rya A
ll re
fere
nces
in th
is ta
ble
are
in C
hine
se. T
he E
nglis
h-la
ngua
ge p
aper
and
jour
nal t
itles
are
free
tran
slat
ions
. The
orig
inal
Chi
nese
-lang
uage
title
s ca
n be
obt
aine
d fro
m th
e co
rresp
ondi
ng a
utho
r.b O
nly
case
s of
trad
ition
al n
eedl
e ac
upun
ctur
e ar
e in
clud
ed. T
his
expl
ains
any
dis
crep
ancy
bet
wee
n th
e nu
mbe
r of c
ases
in th
is c
olum
n an
d th
e tit
le o
f the
cor
resp
ondi
ng re
fere
nce.
c Ref
eren
ces10
,11 .

![Acupuncture for Treatment of Erectile Dysfunction: A Systematic … · 2019-08-20 · acupuncture with or without heating [moxibustion]), electro-stimulating, acupoint injection,](https://img.pdfslide.us/doc/110x75/5ece85c4ae338d6707679f9c/acupuncture-for-treatment-of-erectile-dysfunction-a-systematic-2019-08-20-acupuncture.jpg)