Embed Size (px)
DESCRIPTION
chinese medicine research
Citation preview

Acupuncture for depression (Review)
Smith CA, Hay PPJ
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2009, Issue 2
http://www.thecochranelibrary.com
Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Acupuncture versus medication, Outcome 1 Reduction in severity of depression. . . . 18
Analysis 1.2. Comparison 1 Acupuncture versus medication, Outcome 2 Improvement in depression. . . . . . . 20
Analysis 2.1. Comparison 2 Acupuncture versus wait list control, Outcome 1 Reduction in severity of depression. . 20
Analysis 2.2. Comparison 2 Acupuncture versus wait list control, Outcome 2 Improvement in depression. . . . . 21
Analysis 3.1. Comparison 3 Acupuncture versus non-specific acupuncture, Outcome 1 Reduction in severity of
depression. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Analysis 3.2. Comparison 3 Acupuncture versus non-specific acupuncture, Outcome 2 Improvement in depression. . 22
Analysis 4.1. Comparison 4 Acupuncture plus medication versus medication, Outcome 1 Reduction in severity of
depression. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Analysis 4.2. Comparison 4 Acupuncture plus medication versus medication, Outcome 2 Improvement in depression. 23
Analysis 5.1. Comparison 5 Acupuncture plus medication versus acupuncture plus placebo, Outcome 1 Reduction in
severity of depression. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Analysis 5.2. Comparison 5 Acupuncture plus medication versus acupuncture plus placebo, Outcome 2 Improvement in
depression. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
24WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
24HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
24CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
24DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
25SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
25INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iAcupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Acupuncture for depression
Caroline A Smith1, Phillipa PJ Hay2
1Centre for Complementary Medicine Research, The University of Western Sydney, Penrith South DC, Australia. 2Mental Health
School of Medicine , Building 3 , Penrith South, Australia
Contact address: Caroline A Smith, Centre for Complementary Medicine Research, The University of Western Sydney, Locked Bag
1797, Penrith South DC, New South Wales, 1797, Australia. [email protected]. (Editorial group: Cochrane Depression,
Anxiety and Neurosis Group.)
Cochrane Database of Systematic Reviews, Issue 2, 2009 (Status in this issue: Unchanged)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
DOI: 10.1002/14651858.CD004046.pub2
This version first published online: 19 July 2004 in Issue 3, 2004.
Last assessed as up-to-date: 16 March 2004. (Help document - Dates and Statuses explained)
This record should be cited as: Smith CA, Hay PPJ. Acupuncture for depression. Cochrane Database of Systematic Reviews 2004,
Issue 3. Art. No.: CD004046. DOI: 10.1002/14651858.CD004046.pub2.
A B S T R A C T
Background
There is interest from the community in the use of self help and complementary therapies for depression. This review examined the
currently available evidence supporting the use of acupuncture to treat depression.
Objectives
To examine the efficacy and adverse effects of acupuncture for depression.
Search strategy
The following databases were searched: Cochrane Central Register of Controlled Trials (CENTRAL) MEDLINE (1966 to Sept 2003)
EMBASE (1980 to Sept 2003) PSYCINFO (1874 to Sept 2003) the Database of Abstracts of Reviews of Effectiveness (DARE)
CISCOM, CINAHL (January 1980 to Sept 2003). The following terms were used: depression, depressive disorder, dysthymic disorder
and acupuncture.
Selection criteria
Inclusion criteria included all published and unpublished randomised controlled trials comparing acupuncture with sham acupuncture,
no treatment, pharmacological treatment, other structured psychotherapies (cognitive behavioural therapy, psychotherapy or coun-
selling), or standard care. The following modes of treatment were included: acupuncture, electro acupuncture or laser acupuncture.
The subjects included adult men and women with depression defined by clinical state description, or diagnosed by the Diagnostic and
Statistical Manual (DSM-IV), Research Diagnostic Criteria (RDC), or the International Classification of Disease (ICD).
Data collection and analysis
Meta analysis was performed using relative risk for dichotomous outcomes and weighted mean differences for continuous outcomes,
with 95% confidence intervals. Primary outcomes were reduction in the severity of depression, measured by self rating scales, or by
clinician rated scales; and an improvement in depression defined as remission vs no remission.
Main results
Seven trials comprising 517 subjects met the inclusion criteria. Five trials (409 subjects) included a comparison between acupuncture
and medication. Two other trials compared acupuncture with a wait list control or sham acupuncture. Subjects generally had mild
1Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

to moderate depression. There was no evidence that medication was better than acupuncture in reducing the severity of depression
(WMD 0.53, 95%CI -1.42 to 2.47), or in improving depression, defined as remission versus no remission (RR1.2, 95%CI 0.94 to
1.51).
Authors’ conclusions
There is insufficient evidence to determine the efficacy of acupuncture compared to medication, or to wait list control or sham
acupuncture, in the management of depression. Scientific study design was poor and the number of people studied was small.
P L A I N L A N G U A G E S U M M A R Y
Acupuncture for depression
In clinical depression people often report a lack of interest in life and normally enjoyed activities, accompanied by other symptoms
including weight loss/over-eating, feelings of uselessness, sleep disturbance, self neglect and social withdrawal, insomnia/hypersomnia,
loss of energy, low self esteem and poor concentration. Depression is widely experienced in our communities. There are studies indicating
a preference for treatment with self-help and complementary therapies for depression. This review examined the efficacy and adverse
effects of acupuncture in treating depression. Based on the findings from seven trials of low quality, there is insufficient evidence to
determine whether acupuncture is effective in the management of depression.
B A C K G R O U N D
Clinical depression is a syndrome characterised by a number of
behavioural, cognitive and emotional features. Depressed patients
often exhibit signs of dysphoric mood, loss of interest in normally
enjoyable things, self neglect and social withdrawal, poor appetite
or overeating, insomnia or hypersomnia, fatigue or loss of energy,
low self esteem, poor concentration or difficulty making decisions,
and feelings of hopelessness.
Depression is recognised as a major public health problem, which
has a substantial impact on individuals and to society. Depres-
sive disorders are common in the general population. In Aus-
tralia, 5.8% of Australian adults experience a depressive disorder
(Andrews 1999). The rate of depression among women is two to
three times that of men (Myer 1984). The World Health Organ-
isation has described depression as an “unseen burden” (Murray
1996). The Global Burden of Disease study reported that when
measured by Disability Adjusted Life Years (DALY), unipolar ma-
jor depression ranked fourth in 1990, and would rise to second by
2020, in terms of the overall burden of all diseases in the world. In
terms of disability alone, defined as a restriction or lack of ability
to perform an activity in the manner or range considered normal
(WHO 1980), unipolar depression ranked first in 1990, affecting
51 million people and contributing 10.7% of the total years lived
with disability from all causes (Murray 1996). It has been demon-
strated in the community that those who suffer depressive disor-
ders experience reduced physical and mental functioning, similar
to patients with chronic diseases such as diabetes (Hays 1995 and
Wells 1989). Mood disorders have, in addition, been shown to
have a greater impact on quality of life compared with conditions
such as hypertension and cardiac disease (Spitzer 1995).
The majority of depressed patients are managed in primary care
and do not require hospitalisation. This illness has considerable
financial costs to health services and to society. The cost of de-
pression in the United States has been estimated at $43 billion per
year (Greenberg 1993).
In primary care depression is most frequently treated with an-
tidepressants (Goldman 1999). In addition, there are a range of
psychological interventions, including cognitive behaviour thera-
pies, interpersonal therapy, psychotherapy and counselling. Sur-
veys in Australia have shown that Australians report a preference
for self-help and complementary therapies for depression (Jorm
1997, Jorm 2000). In an Australian survey, it has been estimated
that 49% of adults have used some form of complementary ther-
apy, and a fifth have consulted a complementary practitioner (
MacLennan 1996). In the United States, results from a survey in-
dicate that people who are depressed have a higher use of comple-
mentary therapies (Kessler 2000).
Acupuncture has a long history of use in China and Japan. Tradi-
tional Chinese medicine theory describes a state of health main-
tained by a balance of energy in the body. Acupuncture involves
the insertion of fine needles into different parts of the body to
correct the imbalance of energy in the body. There are a range of
styles of acupuncture from traditional/classical acupuncture, au-
ricular acupuncture, trigger point acupuncture, and single point
acupuncture. Traditional Chinese Medicine (TCM) and Classical
2Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Acupuncture is based on the Chinese philosophical ideas of Yin
and Yang and the Five Elements which form the basis of Chinese
medical theory. These theories form the basis for explaining dis-
ease and physiological function. A westernised medical application
of acupuncture involves the use of acupuncture administered in
relation to mainstream, and using trigger points, segmental points
and commonly used formula points. Medical acupuncture may
involve the application of acupuncture based on the principles of
neurophysiology and anatomy, and the exclusion of TCM princi-
ples and philosophy. Auricular therapy involves the use of the ear
to make a diagnosis and subsequent needling to points on the ear.
Conventional science suggests acupuncture works by neurologi-
cal, neurohormonal and psychological mechanisms. In relation to
depression, there is some evidence from animal experiments sug-
gesting acupuncture or electroacupuncture (EA) is capable of ac-
celerating the synthesis and release of serotonin (5-HT) and nore-
pinephrine (NE) in the central nervous system (Han 1986).
The rationale of treatment will determine the needling details (for
example selection or points, number of needles used) or method
of stimulation (for example use of electro-acupuncture (involves
passing a pulsed current through body tissues via acupuncture
needles), laser acupuncture (the use of low power laser to stimulate
the acupuncture point) and acupressure (the application of finger
pressure). It is possible that these different styles of acupuncture
may differ in their effectiveness, although there is little research
examining this question. Similarly, the design of the acupuncture
control in acupuncture research can range from invasive to non-
invasive procedures and wait list controls, and the design may
influence the placebo or non specific needling effects arising from
the control group design.
Acupuncture is not entirely free of adverse side effects. In a sur-
vey of acupuncture practitioners in Australia, minor reactions to
acupuncture treatment such as nausea and vomiting, fainting and
increased pain were reported (Bensoussan 2000). Acupuncture
practitioners experienced an average of one adverse effect reported
every eight to nine months of practice, or one adverse event for
every 633 consultations. It has been concluded that acupuncture
is a safe intervention in the hands of a competent practitioner (
Vincent 2001).
This review has examined the currently available evidence assessing
the efficacy and adverse effects of acupuncture for the treatment
of depression.
O B J E C T I V E S
To examine the efficacy and adverse effects of acupuncture for
depression.
1. To determine whether acupuncture is more effective than sham
acupuncture and no treatment with treating depression and im-
proving quality of life
2. To assess the efficacy of acupuncture versus standard treatment
(defined as medication, psychological intervention) with treating
depression and improving quality of life.
3. To determine the adverse effects of acupuncture compared with
sham acupuncture, no treatment and standard treatment (defined
as medication, psychological intervention) with the treatment of
depression.
M E T H O D S
Criteria for considering studies for this review
Types of studies
All published and unpublished randomised controlled trials com-
paring acupuncture with placebo (control acupuncture), no treat-
ment, pharmacological treatment, other structured psychothera-
pies (cognitive behavioural therapy, psychotherapy or counselling),
or standard care.
Types of participants
Adults with depression defined by clinical state description, or
diagnosed by the Diagnostic and Statistical Manual (DSM-IV,
APA 1994), or the Research Diagnostic Criteria (RDC, Spitzer
1977), or the International Classification of Disease (ICD, WHO
1993).
Types of interventions
Active group: classical acupuncture, electro acupuncture, laser
acupuncture versus
Control group: placebo-control (sham interventions, minimal
acupuncture, non-invasive control, electro-acupuncture), no treat-
ment (waiting list, treatment as usual), or pharmacological treat-
ment (standard medication to treat depression) or structured psy-
chotherapies (cognitive behavioural therapy, psychotherapy, coun-
selling) or other standard care as defined by the country-specific
health care setting.
Types of outcome measures
For inclusion data on at least one primary outcome needed to be
included.
Primary outcomes:
Reduction in the severity of depression, measured by self-rating
scales such as the Beck Depression Inventory (Beck 1961), or
by clinician-rated scales, such as the Hamilton Rating Scale for
Depression (Hamilton 1960).
Improvement in depression measured as a dichotomous outcome,
remission vs no remission. The authors recognise that subjective
3Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

assessment may give rise to a source of bias. If a difference was
found in this outcome, greater reliance was given to the validated
scales.
Secondary outcomes:
Quality of life indices (such as the Short Form 36 Health Status
questionnaire (Ware 1994))
Change in use of medication or use of other support systems
Adverse side effects
Acceptability of acupuncture, electro acupuncture or laser
acupuncture (assessed by questioning participants in the trial, or
satisfaction measures).
Short-term outcomes reported at the end of the trial intervention
as well as long-term outcomes were pooled where available.
Search methods for identification of studies
See: Collaborative Review Group search strategy.
Electronic Searches:The Cochrane Depression, Anxiety & Neuro-
sis Review Group Register (CCDANCTR-Studies) was searched
using the following terms: Diagnosis = Depressi* or Dysthymi*
and Intervention = Acupuncture
The following databases were searched using the following items:
depression, depressive disorder, dysthymic disorder and acupunc-
ture. Cochrane Central Register of Controlled Trials (CEN-
TRAL) MEDLINE (1966 to September 2003) EMBASE (1980
to September 2003) PSYCINFO (1874 to September 2003) the
Database of Abstracts of Reviews of Effectiveness (DARE) CIS-
COM (database of the Research Council for Complementary
Medicine), CINAHL (January 1980 to September 2003). Assis-
tance was sought from the Chinese Cochrane Centre to search
Chinese databases.
The reference lists of selected journals were inspected for more
published reports and for citations of unpublished randomised
controlled trials.
Data collection and analysis
Study selection
Translation of relevant Chinese language papers was made. Ab-
stracts of trials were evaluated for their appropriateness for inclu-
sion based on trial design and meeting the criteria of the type of
intervention by CS and PH. Where there was uncertainty about
inclusion of the study, the full text was retrieved. The original au-
thor was contacted for further information if necessary. Reasons
for excluding trials have been stated.
Data extraction
Following an assessment for inclusion, the methodology of the
trial was assessed. Data were extracted on patients, methods, in-
terventions, outcomes and results. The data were extracted onto
hard copy data sheets. Data extraction and quality assessment was
made by CS and PH. Missing data or clarification on the study
were sought from the respective authors.
Quality assessment
The methodological quality of the trials was assessed using the
criteria in the Cochrane Handbook describing the relationship
between allocation concealment and bias. Criteria for assessing
bias are described as:
A Low risk of bias (adequate allocation concealment)
B Moderate risk of bias (some doubt about results)
C High risk of bias (inadequate allocation concealment) (Clarke
2000).
A was used to indicate a trial which had a high level of quality in
which all the criteria were met;
B was used to indicate that one or more criteria were partially met
or if it was unclear if all the criteria were met, and
C was used if one or more criteria were not met (Clarke 2000).
Trials were included if they met the criteria A, B or C.
Included trials were assessed according to the following five main
criteria:
(1) adequate concealment of treatment allocation (e.g. opaque
sealed numbered envelopes);
(2) method of allocation to treatment (e.g. by computer randomi-
sation, random number tables);
(3) adequate documentation of how exclusions were handled after
treatment allocation - to facilitate intention to treat analysis;
(4) adequate blinding of outcome assessment, and
(5) losses to follow-up (trials with losses greater than 25%)
Data analysis
Data were entered directly from the data sheets into the Review
Manager software (Revman 2002) with double data entry per-
formed by PH. Where data were not presented in a suitable format
for data entry, or if data were missing, additional information was
sought from the trialists by personal communication in the form
of a letter or telephone call.
An intention to treat analysis enhances the quality of the trial,
and efforts were made to obtain additional data from the authors.
Statistical analysis was performed using the Review Manager (
Revman 2002) software. For dichotomous data, relative risks and
95% confidence intervals (CIs), were calculated. Weighted mean
difference (WMD) and 95% CIs for continuous data were calcu-
lated.
We tested for statistical heterogeneity between trials using a stan-
dard chi squared test. In the presence of significant heterogeneity,
a random effects meta-analysis was used. Causes of heterogeneity
were examined by pre specified subgroup analysis and sensitivity
analysis. The sensitivity analysis aimed to explore the influence of
high quality trials defined by random allocation (defined as ’A’)
versus moderate quality trials (defined as ’B’) and high quality
trials (defined as ’A’) versus low quality trials (defined as ’C’), if
sufficient trials were included.
Pre-specified subgroup analysis examined the effects of different
styles of acupuncture (for example classical/traditional acupunc-
4Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ture versus single point therapy, or auricular acupuncture). Other
subgroup analyses planned to explore the effects of treatment in
people with different diagnoses (for example, major depression
and dysthymia), and in people of different ages (less <65 years and
> 65 years). Data were not reported to allow these other sub-group
analyses.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies; Characteristics of ongoing studies.
A total of nine randomised controlled trials were identified. Seven
trials met the inclusion criteria, and two trials were excluded. The
Agelink 2003 trial was excluded because data describing cardio-
vascular outcomes only were reported. The Chang-du 1994 trial
was excluded because included subjects had experienced a stroke
(DSM IV criteria specify the exclusion of symptoms clearly due
to a medical condition).
Allen 1998
Thirty-four women in the United States with clinical depression
were recruited to this trial. Women were randomised into three
groups; acupuncture designed to treat depression (n=14), a non-
specific acupuncture group (n=12) which involved acupuncture to
treat a pattern of disharmony unrelated to depression, and a wait
list control (n=12). The intervention was carried out over eight
weeks, and was followed by women in the non-specific acupunc-
ture and wait list control group receiving acupuncture for eight
weeks. Acupuncture was administered by four trained and board
certified acupuncturists. No details were reported on the acupunc-
ture points used. Women were treated twice a week for the first
four weeks, followed by once weekly sessions for four weeks. Base-
line characteristics were presented on the subjects. Four women
(11%) dropped out from the study. An intention to treat analysis
was not performed.
Han 1986
Sixty-six men and women aged 18-55 years were recruited to this
trial from the Beijing University Mental Health Institute, China.
Inclusion criteria were ICD-10 and a score of greater than 20 on
the Hamilton Depression Rating Scale. Subjects were randomised
to receive electro-acupuncture (n=30) or maprotiline (n=31). Elec-
tro-acupuncture was administered for 45 minutes, six times a
week, over six weeks. A variety of acupuncture points were used
in the trial to treat Heart, Liver and Kidney deficiency. The nee-
dle depth was described, and electro-stimulation was given for 45
minutes. De qi (needling sensation) was obtained. The medicated
group received daily medication, with doses ranging from 75-250
mg, for six weeks. Subjects completed the Hamilton Depression
Rating Scale. Baseline characteristics were not presented by study
group. Five subjects (8%) did not complete the trial.
Luo 1985
Forty-seven men and women were recruited to this trial, un-
dertaken in China. Subjects were randomised to receive electro-
acupuncture (n=27) or amitriptyline (n=20). Two acupuncture
points were stimulated, Baihui and Yintang. Needles were stimu-
lated using electro-acupuncture for 60 minutes. Subjects received
six sessions a week for five weeks. Needles were inserted to a depth
of eight fen. Electro-stimulation was given until a twitch was vis-
ible. The frequency of stimulation was 80-90 beats per minute.
Subjects taking their medication received an average dose of 142
mg per day. There was no loss to follow up reported.
Luo 1988
Two hundred and forty one men and women were recruited
from 10 psychiatric hospitals in China. Subjects were randomised
to receive electro-acupuncture plus placebo tablets (n=133) or
amitriptyline (n=108). Two acupuncture points were stimulated,
Baihui and Yintang. Needles were stimulated using electro-
acupuncture for 45 minutes. The current was 3-5mA at a fre-
quency of 2Hz. Subjects received six sessions a week for six weeks.
Subjects taking their medication received an initial dose of 25 mg
three times a day, which was increased to 150mg three times a day.
Subjects completed the Hamilton Depression Rating Scale. There
was no loss to follow up reported.
Luo 1998
Twenty nine men and women were recruited from the Bei-
jing Medical University in China. Subjects were randomised to
one of three groups to receive electro-acupuncture plus placebo
tablets (n=8), or amitriptyline (n=11), or electro-acupuncture
and amitriptyline (n=10). Two acupuncture points were stimu-
lated, Baihui and Yintang. Needles were stimulated using electro-
acupuncture for 45 minutes, the current was 3-5mA at a frequency
of 2Hz. Subjects received six sessions a week for six weeks. Needles
were inserted to a depth of 2-3 cm. A twitch sensation was ob-
tained. The treatment session took 45 minutes, although the time
of retention was not specified. Treatments were administered six
days, for six weeks. No other co-interventions were administered.
No details on the practitioner background were reported. The only
information presented on the dosage for the amitriptyline group
was that the dose averaged 175mg per day. For those in the com-
bined treatment group, a dose of 150mg per day was reported.
Subjects completed the Hamilton Depression Rating Scale. There
was no loss to follow up reported.
Roschke 2000
Seventy German men and women, aged 20-70 years, with a clini-
cal diagnosis of depression were randomised to mianserin (90-120
mg/day) (n=24), mianserin (90-120 mg/day) plus verum acupunc-
ture (n=22), manserin (90-120 mg/day) plus placebo acupunc-
ture(n=24). Manual acupuncture was applied three times a week
over four weeks, and administered by two clinicians experienced
in traditional Chinese medicine. The duration of treatment was
5Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

30 minutes. Acupuncture was administered bi-laterally at points
Bladder 15, Bladder 17, Bladder 18, Heart 7, Pericardium 6, Stom-
ach 40, Spleen 5, Spleen 6, and Lung 1. Electrical resistance was
used to determine point location. Needles were inserted to a depth
of a few millimetres and needles removed after a few minutes.
Acupuncture was performed by two experienced acupuncturists.
No further details were provided. The treatment used a standard-
ised whole body acupuncture treatment applied three times a day,
over four weeks, with each treatment lasting 30 minutes. For the
placebo group, needles were inserted at non-acupuncture points.
To measure depression the Global Assessment Scale, Melancho-
lia scale, and Clinical Global Impressions Scale were used. Mean
self reported and dosage of medication were calculated. Baseline
characteristics were presented on the participants. There were no
losses to follow up.
Xiujuan 1994
Forty one men and women were recruited from in-patient and
out-patient care at a University Hospital in China. Subjects were
randomised to receive acupuncture (n=20) or standard medical
care using amitriptyline (n=21). Acupuncture points Governor
vessel 24, Governor vessel 20, Governor vessel 14, Governor ves-
sel 12, Conception vessel 17, Conception vessel 14, Gall bladder
20, Pericardium 6 were used. Additional acupuncture points were
used depending on the Chinese medical diagnosis. For stagnation
of Liver qi Stomach 23, Spleen 6 and Liver 3 were used. For stag-
nation of Liver blood Colon 4, Liver 3, Spleen 10 were used. For
Spleen and Heart deficiency Heart 7, Pericardium 7, Spleen 6 and
Stomach 36 were used. For Spleen and Kidney yang deficiency
Kidney 3, Spleen 6, Stomach 36 and Conception vessel 4 were
used. Needles were inserted bi-laterally, and stimulated manually,
except for Governor vessel 24 and Governor vessel 20, which were
stimulated using electro acupuncture (frequency 80-100/second).
Treatment was administered six days a week over six weeks. The
control group took 25 mg of amitriptyline on the first day, and
the dose was increased by 25-50 mg each day up to 150 mg. In the
second week the dose was adjusted according to response and side
effects, but ranged from 150 mg to 300 mg daily. The Hamilton
Rating Scale for Depression was used to collect data once a week
over six weeks. Data were also available on patients cured. No data
were presented on baseline characteristics. There were no losses to
follow up.
Risk of bias in included studies
ALLOCATION CONCEALMENT
The Allen 1998 trial was given a score of A. Han 1986, Luo 1985,
Luo 1988, Luo 1998, Roschke 2000 and Xiujuan 1994 trials were
given a score of B, as the allocation concealment was unclear.
METHOD OF CONCEALMENT
Central randomisation was undertaken in the Allen 1998 trial.
The method of allocation was not reported for the Han 1986,
Luo 1985, Luo 1988, Luo 1998, Roschke 2000 and Xiujuan 1994
trials.
BLINDING
In the Allen 1998 trial the patient, therapist (valid acupuncture
points were used but the therapists were blind to the experimental
hypotheses) and outcome assessor were blind. It was unclear if the
analyst was blind.
In the Roschke 2000 trial, it was unclear if subjects were blind
to their acupuncture group; although the authors reported that
subjects were blind to their acupuncture group allocation, this
was not verified with data. It was not feasible for the acupuncture
therapist to be blind. The outcome analyst was reported to be
blind in the trial, but it was unclear if the analyst was blind in the
Roschke 2000 trial.
In the Luo 1985, Han 1986 and Xiujuan 1994 trials, trial subjects
and the therapist were not blind. It was unclear if the outcome
assessor and analyst were blind to study group allocation.
In the Luo 1988 and Luo 1998 trials, full details on who was blind
was not reported.
INTENTION TO TREAT ANALYSIS
An intention to treat analysis was mentioned and performed in
the Roschke 2000, Xiujuan 1994 and Luo 1985, Luo 1988 and
Luo 1998 trials. An intention to treat analysis was not undertaken
in the Allen 1998 and Han 1986 trials.
LOSSES TO FOLLOW UP
There were no losses reported in the Roschke 2000, Luo 1985,
Luo 1988, Luo 1998 and Xiujuan 1994 trials. In the Allen 1998
trial, four women (11%) dropped out and one was included in
the analysis. Reasons for dropout included pregnancy, moving in-
terstate, discomfort with the treatment. One woman dropped out
because she did not lose weight, which she believed she would do
from receiving pharmacological treatment. In the Han 1986 trial,
five subjects (8%) were lost to follow up.
Effects of interventions
An overall seven trials were included in the meta analysis. The
trials contained a total of 517 subjects.
ACUPUNCTURE VERSUS MEDICATION
Reduction in severity of depression
Five studies (409 participants) reported on a reduction in the sever-
ity of depression using the Hamilton depression rating scale (Han
1986, Luo 1985, Luo 1988, Luo 1998 and Xiujuan 1994). Overall
there was no significant difference between groups (WMD 0.53
95%CI -1.42 to 2.47). Borderline heterogeneity was identified
in the meta-analysis and was explored through pre-specified sub-
group analysis by style of acupuncture. A comparison was made
between electro-acupuncture (Luo 1985, Luo 1988 and Luo 1998)
and a classical acupuncture approach (Han 1986 and Xiujuan
1994). In the meta-analysis of style of acupuncture, no difference
6Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

was found between groups of electro-acupuncture (WMD -0.36,
95%CI -3.19 to 2.46), similarly no significant difference in the
severity of depression was found in the two trials using classical
acupuncture. The style of acupuncture did not explain the hetero-
geneity.
Improvement in depression
Four studies (375 participants) reported on this outcome and were
included in the meta-analysis (RR 1.20, 95 % CI 0.94 to 1.51).
No differences were found between groups in any of the four trials
(Luo 1985 RR 1.48, 95% CI 0.67 to 3.27; Luo 1988 RR 1.17,
95% CI 0.9 to 1.51; Xiujuan 1994 RR 0.88, 95% CI 0.32 to
2.42; and Roschke 2000 RR 4.36, 95% CI 0.53 to 36.12).
Adverse effects
Limited data were reported on adverse effects. Han 1986 re-
ported on adverse effects for the acupuncture group only. Sleep
disturbances were reported by 10% of subjects, headaches by 7%
and tiredness by 7% of subjects. Adverse effects relating to dry
mouth, constipation, heartburn, sleepiness and headaches were
reported by the medicated group, although data were not pre-
sented. Luo 1988 reported that adverse effects in the amitriptyline
group were significantly greater than in the acupuncture group.
Luo 1998 reported 138 adverse events in the acupuncture group,
with headaches (n=26), palpitations (n=16) and dryness of the
mouth (n=16) the most common adverse effects. In the medicated
group, 342 subjects reported slight adverse effects, with palpita-
tions (n=43), dryness of the mouth (n=42), and physical tiredness
(n=38) most commonly reported.
No other outcome measures were reported.
ACUPUNCTURE VERSUS WAIT LIST CONTROL
One study reported two outcomes for this comparison (Allen
1998).
Reduction in severity of depression
Allen 1998 reported on the mean change in Hamilton Depression
Rating scores from baseline to eight weeks. No significant differ-
ence was found between groups (WMD -5.60, 95% CI -13.25 to
2.05).
Improvement in depression
Allen 1998 included 23 participants. In this study improvement
was defined as full remission. The outcome assessor was blind
in data collection. No significant difference between groups was
found (RR 2.29, 95% CI 0.55 to 9.49).
ACUPUNCTURE VERSUS NON SPECIFIC ACUPUNC-
TURE
A comparison was made in the Allen 1998 trial between the
acupuncture specific group to treat depression and a non-specific
acupuncture treatment group. Two outcomes were reported.
Reduction in severity of depression
A greater mean reduction in depression scores was found among
participants in the acupuncture specific group compared with the
non-specific acupuncture group (WMD -8.80, 95% CI -15.03 to
2.57).
Improvement in depression
No significant difference was found in the numbers reporting full
remission between groups (RR.4.58, 95% CI 0.63 to 33.36).
ACUPUNCTURE PLUS MEDICATION VERSUS MEDICA-
TION
Two studies undertook this comparison (Roschke 2000 and Luo
1998). Two outcomes were reported.
Reduction in severity of depression
In the study of 21 subjects receiving acupuncture in addition to
medication (Luo 1998), the subjects receiving medication alone
reported a greater reduction in the severity of depression (WMD
3.1, 95% CI 1.04 to 5.16).
Improvement in depression
One study (Roschke 2000) of 46 subjects found no significant
difference between these two groups (RR 4.36, 95% CI 0.53 to
36.12).
ACUPUNCTURE PLUS MEDICATION VERSUS
ACUPUNCTURE PLUS PLACEBO
Two studies undertook this comparison (Roschke 2000 and Luo
1998). Two outcomes were reported.
Reduction in severity of depression
In the Luo 1998 trial of 28 subjects, no significant difference was
found in the severity of depression (WMD 1.4, 95% CI -0.92 to
3.72).
Improvement in depression
In the Roschke 2000 trial of 46 subjects, no significant difference
was found between the two groups for an improvement in depres-
sion (RR 0.55, 95% CI 0.19 to 1.56).
A sensitivity analysis based on the allocation criteria was not per-
formed, because only one trial (Allen 1998) met the criteria of
“A”.
D I S C U S S I O N
There is a lack of well designed randomised controlled trials to eval-
uate the role of acupuncture in treating depression. Acupuncture
has not been subjected to rigorous scientific study, and overall the
number of people studied was small. The results should therefore
be interpreted with caution. The majority of studies were of poor
methodological quality or inadequately reported. Internal validity
was poor in relation to selection of participants. For many studies
the lack of blinding in relation to outcome assessors and analyst
may have introduced a source of bias, as well as the subjective
bias from poorly defined criteria for the outcome “improvement
in depression”. The varying doses of medication reported in the
Luo trials suggest that the doses may not have been therapeutically
effective, or that the timing of assessment was too early.
Seven trials involving 517 participants were included in the meta-
analysis. The first comparison of acupuncture and medication in-
volved six trials, and included two outcomes. Five trials involv-
7Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ing 409 participants were included in the first meta-analysis of
acupuncture and medication, and found no difference between
acupuncture and medication for reduction in severity of depres-
sion. However, the methodological quality of these five trials was
not high, details of randomisation were unclear, no power anal-
yses were reported and details of the acupuncture were not fully
reported. The style of acupuncture was explored in pre-specified
sub-group analyses. This variable did not explain the borderline
heterogeneity found. None of the trials included in this compari-
son were designed specifically to test equivalence. Due to the small
number of trials, the conclusions from the subgroup analysis and
sensitivity analysis were limited. Four trials involving 375 partic-
ipants were included in the second meta-analysis of acupuncture
and medication, and found no difference in improvement in de-
pression. The methodological quality of these four trials was low.
Though each of the four trials undertook an intention to treat anal-
ysis, and there were no losses to follow-up, they did not report on
the method of randomisation concealment and allocation, and in-
complete reporting on blinding suggests that the potential for bias
exists. The quality and available evidence from these randomised
controlled trials suggests that there is insufficient evidence relating
to the efficacy of acupuncture in relation to medication.
There was insufficient evidence to determine whether acupunc-
ture is more effective than a wait list control, non-specific or sham
acupuncture control, or whether acupuncture plus medication is
more effective than acupuncture plus placebo, because these com-
parisons involved only single studies and small numbers.
There are many styles of acupuncture, including traditional Chi-
nese medicine as used by Allen, and those using formula acupunc-
ture points as in the Luo trials. As illustrated in this review, there
is also wide variation in the mode of stimulation, duration of
needling, number of points used, depth of needling and needle
stimulation and duration of the trial. It is important for any future
trials of acupuncture to treat depression to report the basis for the
acupuncture treatment and needling as described in the STRICTA
guideline (MacPherson 2001). These trials also demonstrate va-
riety in the clinical setting from which subjects are recruited and
the inclusion and exclusion criteria used. Overall, trials reported
on one or two clinical outcomes only, and data on adverse effects,
acceptability of the intervention and quality of life measures were
scarce.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
There is insufficient evidence to determine the efficacy of acupunc-
ture compared to medication in the treatment of depression, based
upon the methodological quality of these trials. There are insuffi-
cient data to demonstrate whether acupuncture is more effective
than a wait list control, non-specific or sham acupuncture control,
or whether acupuncture plus medication is more effective than
acupuncture plus placebo. Recommendations for practice cannot
be made until further high quality research has been undertaken.
Implications for research
Further randomised controlled trials are required to evaluate the
effectiveness of acupuncture in the treatment of depression. All
future randomised trials must be adequately powered and should
consider other outcome measures as described in this review, in
addition to clinical outcomes. Greater attention should be given
to methodological design including randomisation, blinding of
practitioners (where appropriate), outcome assessors and analysts.
There is also a need to improve the quality and reporting of fu-
ture trials. In particular, attention could be given to reporting or
analysis of the person providing the intervention, their length of
training and length of experience, and the rationale for the style
of acupuncture used.
Future studies may need to consider the use of comparative de-
signs using medication or structured psychotherapies (cognitive
behavioural therapy, psychotherapy, counselling) or standard care,
due to the ethics of administering this intervention to this study
population. Future studies should also give consideration to in-
cluding long-term evaluation of effectiveness and adverse effects
of acupuncture.
A C K N O W L E D G E M E N T S
The reviewers would like to acknowledge the CCDAN team for
the assistance with the preparation of the review, including the
Trials Search Coordinator for assistance in developing the search
strategy, the editors, co-editors and other staff within the team and
the Chinese Cochrane Centre for their assistance with searching
databases for trials published in the Chinese literature. To Michael
Arnold for his contribution with the protocol development.
8Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

R E F E R E N C E S
References to studies included in this review
Allen 1998 {published data only}∗ Allen JB, Schnyer RN, Hitt SK. The efficiacy of acupuncture in
the treatment of major depression in women. Psychological Science
1998;9(5):397–401.
Han 2002 {published data only}∗ Han C, Li XW, Luo HC. Comparative study of electro-acupuncture
and maprotiline in treating depression. Combined Chinese/WesternJournal 2002;22(7):512–4.
Luo 1985 {published data only}
Luo HC, Yunkui J, Zhan L. Electro-acupuncture versus amitriptyline
in the treatment of depressive states. Journal of Traditional Chinese
Medicine 1985;5(1):3–8.
Luo 1988 {published data only}∗ Luo HC, Shen YC, Jia YK, Zhou D. Clinical study of electro-
acupuncture on 133 patients with depression in comparison with
tricyclic amitriptyline. Chinese Journal of Modern Developments in
Traditional Medicine 1988;8(2):77–80.
Luo 1998 {published data only}
Luo H, Meng F, Jia Y, Zhao X. Clinical research on the therapeutic
effect of the electro-acupuncture treatment in patients with depres-
sion. Psychiatry and Clinical Neurosciences 1998;52:338–40.
Roschke 2000 {published data only}∗ Roschke J, Wolf C, Muller MJ, Wagner P, Mann K, Grozinger M,
et al.The benefit from whole body acupuncture in major depression.
Journal of Affective Disorders 2000;57:73–81..
Xiujuan 1994 {published data only}∗ Xiujuan Y. Clinical observation on needling extrachannel points in
treating mental depression. Journal of Traditional Chinese Medicine1994;14(1):14–8.
References to studies excluded from this review
Agelink 2003 {published data only}∗ Agelink MW, Sanner D, Elch H, Pach J, Bertling R, Lemmer W,
et al.Does acupuncture influence cardiac autonomic nervous system
in patients with minor depression or anxiety disorders. Fortschritteder Neurologie und Psychiatrie 2003;71:141–9.
Chang-du 1994 {published data only}∗ Chang-du L, Yong H, Ying-kun L, Ka-ming H, Zhen-ya J. Treat-
ing post stroke depression with “mind refreshing antidepressive”:
acupuncture therapy: a clinical study of 21 cases. International Jour-nal of Clinical Acupuncture 1994;5(4):389–93.
References to ongoing studies
Allen {published data only (unpublished sought but not used)}
Acupuncture in the treatment of depression. Ongoing study Set
1997.
Additional references
Andrews 1999
Andrews G, Hall W, Teeson M, Henderson S. The mental health ofAustralians. Canberra, AU: Mental Health Branch, Commonwealth
Department of Health and Aged Care, 1999.
APA 1994
American Psychiatric Association. Diagnostic and statistical manual
of mental disorders. 4th Edition. Washington, DC: American Psy-
chiatric Association, 1994.
Beck 1961
Beck AT, Ward CH, Medelson M, Mock J, Erbaugh J. An inventory
for measuring depression. Archives of General Psychiatry 1961;4:561–
71.
Bensoussan 2000
Bensoussan A, Myers SP, Carlton AL. Risk associated with the practice
of traditional Chinese medicine: an Australian Study. Archives ofFamily Medicine 2000;9(10):1071–8.
Clarke 2000
Clarke M, Oxman AD. Cochrane Reviewer’s Handbook 4.1 (updated
June 2000). In: Review Manager (Revman) (Computer program) .Version 4.1. Oxford: The Cochrane Collaboration, 2000.
Goldman 1999
Goldman LS, Nielsen NH, Champion HC. Awareness, diagnosis
and treatment of depression. Journal of General Internal Medicine1999;14(9):569–89.
Greenberg 1993
Greenberg PE, Stiglin LE, Finkelstein SN, Berndt ER. The economic
burden of depression in 1990. Journal of Clinical Psychiatry 1993;
54:405–18.
Hamilton 1960
Hamilton M. A rating scale for depression. Journal of Neurosurgery& Psychiatry 1960;23:56–62.
Han 1986
Han JS. Electroacupuncture: an alternative to antidepressants for
treating effective diseases. International Journal of Neuroscience 1986;
29:79–92.
Hays 1995
Hays RD, Wells KB, Sherbourne CD, Rogers W, Spritzer K. Func-
tioning and well-being outcomes of patients with depression com-
pared with chronic general medical illnesses. Archives of General Psy-chiatry 1995;52:11–9.
Jadad 1996
Jadad A, Moore A, Carrol D, Jenkinson C, Reynolds DJ, Gavaghan
DJ, et al.Assessing the quality of reports of randomized clinical trials:
Is blinding necessary?. Controlled Clinical Trials 1996;17(1):1–12.
Jorm 1997
Jorm AF, Korten AE, Jacomb PA, Christensen H, Rodgers B, Pollitt
P. Mental health literacy: a survey of the public’s ability to recognise
mental disorders and their belief about the effectiveness of treatment.
Medical Journal of Australia 1997;166:182–86.
Jorm 2000
Jorm AF, Medway J, Christensen H, Korten AE, Jacomb PA, Rodgers
B. Public beliefs about the helpfulness of interventions for depression:
effects on actions taken when experiencing anxiety and depression
symptoms. Australia and New Zealand Journal of Psychiatry 2000;34:
619–26.
9Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kessler 2000
Kessler RC, Soukup J, Davis RB. The use of complementary and
alternative therapies to treat anxiety and depression in the Unites
States. American Journal of Psychiatry 2000;158:289–94.
MacLennan 1996
MacLennan AH, Wilson DH, Taylor AW. Prevalence and cost of
alternative medicine in Australia. Lancet 1996;347:569–73.
MacPherson 2001
MacPherson H, White A, Cummings M, Jobst K, Rose K, Niemt-
zow R. Standards for reporting interventions in controlled trials of
acupuncture: the STRICTA group.. Complementary Therapies in
Medicine 2001;9(4):246–9.
Murray 1996
Murray CJ, Lopez AD. The global burden of disease. Geneva: World
Health Organisation and Harvard University Press, 1996.
Myer 1984
Myers J, Weissman MM, Tischler GL, Holzer CE 3rd, Leaf PJ, Or-
vaschel H, et al.Six-month prevalence of psychiatric disorders in three
communities 1980 to 1982. Archives of General Psychiatry 1984;41:
959–67.
Revman 2002
The Cochrane Collaboration. Review Manager (RevMan)
(Computer program) Version 4.2 for Windows. Oxford: The
Cochrane Collaboration, 2002.
Spitzer 1977
Spitzer RL, Endicott J, Robins E. Research Diagnostic Criteria (RDC)
for a selected group of functional disorders. 3rd Edition. New York,
NY: Biometric Research, 1977.
Spitzer 1995
Spitzer RL, Kroenke K, Linzer M, Hahn SR, Williams JB, deGruy
FV 3rd, et al.Health-related quality of life in primary care patients
with mental disorders. Results from the PRIME-MD 1000 Study.
JAMA 1995;274:1511–7.
Vincent 2001
Vincent C. The safety of acupuncture. BMJ 2001;323:4467–8.
Ware 1994
Ware JE, Kosinski M, Keller SD. SF36 physical and mental healthsummary scales: a users manual. Boston, MA: Health Institute, New
England Medical Centre, 1994.
Wells 1989
Wells KB, Stewart A, Hays RD, Burnam MA, Rogers W, Daniels M,
et al.The functioning and well being of depressed patients: results
from the Medical Outcomes Study. JAMA 1989;262:914–9.
WHO 1980
World Health Organisation. International classification of impair-
ments, disabilities and handicaps: a manual of classification relatingto the consequence of disease. Geneva: World Health Organisation,
1980.
WHO 1993
World Health Organisation. The ICD-10 Classification of mentaland Behavioural Disorders. Diagnostic Criteria for Research. Geneva:
World Health Organisation, 1993.∗ Indicates the major publication for the study
10Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Allen 1998
Methods Single blind randomised controlled trial (it remains possible that the acupuncture therapists developed
some awareness between the treatments). Randomisation was computer generated and was undertaken
centrally . The patient, therapist and outcome assessor were blind. It was unclear if the analyst was blind.
Four women dropped out (13%). An intention to treat analysis was performed.
Participants Thirty eight women aged 18 to 45 were recruited in the United States. Inclusion criteria were major
depression as described by DSM IV. Exclusion criteria: dysthymia or chronic depression, history of
psychosis or mania, substance abuse, current treatment, endocrine abnormalities, history of central nervous
system lesions or any medical condition causing depression, pregnancy, suicide potential.
Interventions Women were randomly allocated to acupuncture, non specific acupuncture and a wait list control for
eight weeks. The non specific acupuncture and wait list control then received acupuncture. The eight
week intervention involved two sessions a week for the first four weeks, followed by one session a week
thereafter.
Outcomes Subjects completed the Hamilton Rating Scale for Depression (HRSD), and Beck Depression Inventory
at baseline, 8 and 16 weeks.
Notes A power calculation was not reported.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
Han 2002
Methods Acupuncture versus standard medication. No details could be obtained from the author on how the
allocation sequence was generated and the method of concealment. The study participant and therapist
were not blind and it was unclear if the outcome assessor, and analyst were blind to the study group.
Participants Sixty six men and women aged 18-55 years were recruited to the trial from the Beijing University mental
health institute, China. Inclusion criteria were ICD 10 and a score of greater than 20 on the Hamilton
Depression Scale. Exclusion criteria were not specified.
Interventions Subjects were randomly allocated to receive electro-acupuncture or maprotiline. Electro-acupuncture
was administered for 45 minutes, six times a week over six weeks. The medicated group received daily
medication with doses ranging from 75-250 mg, for six weeks.
11Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Han 2002 (Continued)
Outcomes Subjects completed the Hamilton depression rating scale, self rating scale for depression, clinical global
impression scale and Ashberg rating scale for side effects. Outcome measurements were collated at baseline,
14, 28 and 24 days from trial entry.
Notes A power calculation was not reported. Complete follow up was obtained. Intention to treat analysis was
performed.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Luo 1985
Methods Electro acupuncture versus amitriptyline. No details were provided on randomisation and blinding. There
was no loss to follow up reported and an intention to treat analysis was performed.
Participants Forty seven men and women were recruited to the trial. Subjects scored 20 or more on the Hamilton
Rating Scale. No exclusion criteria were specified.
Interventions Two acupuncture points were stimulated Baihui and Yintang. Needles were stimulated using electro
acupuncture. Subjects received 6 sessions a week for 5 weeks. Subjects taking their medication received
an initial dose of 25mg 3 times a day for one week. The treatment dose was then increased to an average
dose of 142mg.
Outcomes The Hamilton Rating scale, Clinical Global Impression Chart, and the Rating scale for side effects
(ASBERG) were interviewed by two psychiatrists at the beginning and end of the trial.
Notes A power calculation was not performed. There were no losses to follow up. An intention to treat analysis
was performed.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
12Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Luo 1988
Methods Electro acupuncture versus amitriptyline. No details were provided on randomisation. No details were
reported on blinding. There was no loss to follow up reported and an intention to treat analysis was
performed.
Participants Two hundred and forty one men and women were recruited from 3 psychiatric hospitals in China. Subjects
scored 20 or more on the Hamilton Rating Scale. No exclusion criteria were specified. Subjects were aged
32-64 years.
Interventions Two acupuncture points were stimulated Baihui and Yintang. Needles were stimulated using electro
acupuncture. Subjects received 6 sessions a week for 6 weeks. Subjects taking their medication received an
initial dose of 25mg 3 times a day for one week. The treatment dose was then increased to 50 mg three
times a day.
Outcomes The Hamilton Rating scale, Clinical Global Impression Chart, and the Rating scale for side effects
(ASBERG) were completed at the start and end of the trial.
Notes A power calculation was not performed. There were no losses to follow up. An intention to treat analysis
was performed.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Luo 1998
Methods Electro acupuncture versus amitriptyline versus electro acupuncture and amitriptyline. No details were
provided on randomisation. Outcome assessors were blind to the study group, no other details were
provided. There was no loss to follow up reported and an intention to treat analysis was performed.
Participants Twenty nine men and women were recruited to the trial. Subjects were recruited from a closed ward at
the Beijing Medical University Hospital. All participants were drug free for the week before commencing
the trial. Subjects scored 20 or more on the Hamilton Rating Scale. No exclusion criteria were specified.
Mean age was 36 years and the mean course of depression was 7.9 years.
Interventions Two acupuncture points were stimulated Baihui and Yintang. Needles were stimulated using electro
acupuncture for 45 minutes, the current was 3-5mA at a frequency of 2Hz. Subjects received 6 sessions a
week for 6 weeks. Subjects taking their medication received an average dose of 161 mg per day.
Outcomes The Hamilton Rating scale, Clinical Global Impression Chart, and the Rating scale for side effects
(ASBERG).
Notes A power calculation was not performed. There were no losses to follow up. An intention to treat analysis
was performed.
13Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Luo 1998 (Continued)
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Roschke 2000
Methods Single blind placebo controlled trial. No details could be obtained from the author on how the allocation
sequence was generated and the method of concealment. The study participant and therapist were not
blind and it was unclear if the analyst was blind. The outcome assess ors were blind. No data was provided
to verify if subjects were blind to being allocated to acupuncture or placebo acupuncture.
Participants Seventy inpatients aged 20-70 years, in Germany were randomised to the trial. Patients were eligible if
diagnosed with clinical depression equating to DSM IV and a score of greater than 18 on the Hamilton
depression scale. Patients were excluded if suicidal, a diagnosis of schizophrenia or bipolar affective disorders
, or delusions. Patients with coagulation disease, wound healing disease, emphysematous thorax, abnormal
blood cell count, serious liver and kidney disease and epilepsy were excluded. Subjects were aged 20-70
years.
Interventions Subjects were randomised to three study groups. Mianserin (90-120 mg/day, Mianserin (90-120 mg/day)
plus verum acupuncture, Mianserin (90-120 mg/day) plus placebo acupuncture). Up to 20 mg/day
diazepam was allowed if required. Acupuncture was applied three times a week over four weeks.
Outcomes The Global assessment scale, Melancholia scale, Clinical global impressions scale were used to assess
depression. Mean dosage of medication was collected and a self report of improvement.
Notes A power calculation was not performed. There were no losses to follow up. An intention to treat analysis
was performed.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
14Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Xiujuan 1994
Methods Single blind randomised controlled trial of acupuncture compared with standard treatment amitriptyline.
It was unclear as to how the allocation sequence was generated and if there was adequate concealment
of the allocation sequence. Subjects and the therapist were not blind and it was unclear if the outcome
assessor and analyst were blind to study group allocation.
Participants Forty one men and women with clinical depression and the Hamilton Depression scale were recruited to
the trial from in and out patient clinics at the Beijing Medical university, China. No exclusion criteria
were reported.
Interventions Subjects were randomised to receive acupuncture or standard medical care using amitriptyline. Acupunc-
ture points Governor Vessel 24, 20, 14, 12, Conception Vessel 17, 14, Gall Bladder 20, Pericardium 6.
Additional acupuncture points were used depending on the Chinese medical diagnosis. For stagnation
of Liver qi Stomach 23, Spleen 6 and Liver 3 were used. For stagnation of liver blood Colon 4, Liver
3, Spleen 10 were used. For spleen and heart deficiency Heart 7, Pericardium 7, Spleen 6 and Stomach
36 were used. For Spleen and Kidney yang deficiency Kidney 3, Spleen 6, Stomach 36 and Conception
vessel 4 were used. Needles were inserted bi laterally and stimulated manually except for Governor Vessel
24 and 20 which were stimulated using electro acupuncture (frequency 80-100/second). Treatment was
administered for 6 days over 6 weeks. The control group tool 25 mg of amitriptyline on the first day,
the dose was increased by 25-50 mg each day up to 150 mg. In the second week the dose was adjusted
according to response and side effects but ranged from 150 mg to 300 mg daily.
Outcomes The Hamilton Rating Scale for Depression was used to collect data once a week over 6 weeks. Data was
also available on patients cured.
Notes Follow up was complete. There was no power assessment, intention to treat analysis was not mentioned
but was performed.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Characteristics of excluded studies [ordered by study ID]
Agelink 2003 In this trial of depression and anxiety , no clinically meaningful data were reported. Data were reported on cardio-
vascular outcomes.
Chang-du 1994 In this trial of trial of acupuncture, subjects had experienced a stroke. The inclusion criteria specified by DSM IV
specifies exclusions of symptoms that are clearly due to a medical condition.
15Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Characteristics of ongoing studies [ordered by study ID]
Allen
Trial name or title Acupuncture in the treatment of depression
Methods
Participants 150 men and women meeting the criteria for major depression
Interventions Participants will be randomised to acupuncture or a wait list control
Outcomes Efficacy and safety of acupuncture, with a 18 month follow up on clinical outcomes
Starting date Set 1997
Contact information [email protected]
Notes
16Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. Acupuncture versus medication
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Reduction in severity of
depression
5 409 Mean Difference (IV, Random, 95% CI) 0.53 [-1.42, 2.47]
1.1 Electro-acupuncture 3 307 Mean Difference (IV, Random, 95% CI) -0.36 [-3.19, 2.46]
1.2 Classical acupuncture
trials
2 102 Mean Difference (IV, Random, 95% CI) 2.08 [-0.52, 4.67]
2 Improvement in depression 4 375 Risk Ratio (M-H, Random, 95% CI) 1.20 [0.94, 1.51]
Comparison 2. Acupuncture versus wait list control
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Reduction in severity of
depression
1 23 Mean Difference (IV, Random, 95% CI) -5.6 [-13.25, 2.05]
2 Improvement in depression 1 23 Risk Ratio (M-H, Random, 95% CI) 2.29 [0.55, 9.49]
Comparison 3. Acupuncture versus non-specific acupuncture
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Reduction in severity of
depression
1 23 Mean Difference (IV, Random, 95% CI) -8.80 [-15.03, -2.57]
2 Improvement in depression 1 23 Risk Ratio (M-H, Random, 95% CI) 4.58 [0.63, 33.36]
Comparison 4. Acupuncture plus medication versus medication
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Reduction in severity of
depression
1 21 Mean Difference (IV, Random, 95% CI) 3.10 [1.04, 5.16]
2 Improvement in depression 1 46 Risk Ratio (M-H, Random, 95% CI) 4.36 [0.53, 36.12]
17Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 5. Acupuncture plus medication versus acupuncture plus placebo
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Reduction in severity of
depression
1 18 Mean Difference (IV, Random, 95% CI) 1.40 [-0.92, 3.72]
2 Improvement in depression 1 46 Risk Ratio (M-H, Random, 95% CI) 0.55 [0.19, 1.56]
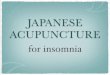
Analysis 1.1. Comparison 1 Acupuncture versus medication, Outcome 1 Reduction in severity of depression.
Review: Acupuncture for depression
Comparison: 1 Acupuncture versus medication
Outcome: 1 Reduction in severity of depression
Study or subgroup Treatment Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
1 Electro-acupuncture
Luo 1985 27 12.8 (10.5) 20 14.2 (8.3) 10.3 % -1.40 [ -6.78, 3.98 ]
Luo 1988 133 8.3 (8.07) 108 10.4 (11.4) 26.3 % -2.10 [ -4.65, 0.45 ]
Luo 1998 8 11.6 (2.54) 11 9.9 (2.3) 29.5 % 1.70 [ -0.52, 3.92 ]
Subtotal (95% CI) 168 139 66.2 % -0.36 [ -3.19, 2.46 ]
Heterogeneity: Tau2 = 3.63; Chi2 = 5.10, df = 2 (P = 0.08); I2 =61%
Test for overall effect: Z = 0.25 (P = 0.80)
2 Classical acupuncture trials
Han 2002 30 11.73 (6.13) 31 9.89 (6) 22.1 % 1.84 [ -1.21, 4.89 ]
Xiujuan 1994 20 15.5 (6.74) 21 12.8 (9.27) 11.7 % 2.70 [ -2.24, 7.64 ]
Subtotal (95% CI) 50 52 33.8 % 2.08 [ -0.52, 4.67 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.08, df = 1 (P = 0.77); I2 =0.0%
Test for overall effect: Z = 1.57 (P = 0.12)
Total (95% CI) 218 191 100.0 % 0.53 [ -1.42, 2.47 ]
Heterogeneity: Tau2 = 2.05; Chi2 = 7.09, df = 4 (P = 0.13); I2 =44%
Test for overall effect: Z = 0.53 (P = 0.60)
-10 -5 0 5 10
Favours treatment Favours control
18Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Review: Acupuncture for depression
Comparison: 1 Acupuncture versus medication
Outcome: 1 Reduction in severity of depression
Study or subgroup Treatment Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
1 Electro-acupuncture
Luo 1985 27 12.8 (10.5) 20 14.2 (8.3) 10.3 % -1.40 [ -6.78, 3.98 ]
Luo 1988 133 8.3 (8.07) 108 10.4 (11.4) 26.3 % -2.10 [ -4.65, 0.45 ]
Luo 1998 8 11.6 (2.54) 11 9.9 (2.3) 29.5 % 1.70 [ -0.52, 3.92 ]
Subtotal (95% CI) 168 139 66.2 % -0.36 [ -3.19, 2.46 ]
Heterogeneity: Tau2 = 3.63; Chi2 = 5.10, df = 2 (P = 0.08); I2 =61%
Test for overall effect: Z = 0.25 (P = 0.80)
-10 -5 0 5 10
Favours treatment Favours control
Review: Acupuncture for depression
Comparison: 1 Acupuncture versus medication
Outcome: 1 Reduction in severity of depression
Study or subgroup Treatment Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
2 Classical acupuncture trials
Han 2002 30 11.73 (6.13) 31 9.89 (6) 22.1 % 1.84 [ -1.21, 4.89 ]
Xiujuan 1994 20 15.5 (6.74) 21 12.8 (9.27) 11.7 % 2.70 [ -2.24, 7.64 ]
Subtotal (95% CI) 50 52 33.8 % 2.08 [ -0.52, 4.67 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.08, df = 1 (P = 0.77); I2 =0.0%
Test for overall effect: Z = 1.57 (P = 0.12)
-10 -5 0 5 10
Favours treatment Favours control
19Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.2. Comparison 1 Acupuncture versus medication, Outcome 2 Improvement in depression.
Review: Acupuncture for depression
Comparison: 1 Acupuncture versus medication
Outcome: 2 Improvement in depression
Study or subgroup Treatment Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Luo 1985 12/27 6/20 8.9 % 1.48 [ 0.67, 3.27 ]
Luo 1988 72/133 50/108 84.5 % 1.17 [ 0.90, 1.51 ]
Roschke 2000 5/20 6/21 5.4 % 0.88 [ 0.32, 2.42 ]
Xiujuan 1994 4/22 1/24 1.2 % 4.36 [ 0.53, 36.12 ]
Total (95% CI) 202 173 100.0 % 1.20 [ 0.94, 1.51 ]
Total events: 93 (Treatment), 63 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 2.14, df = 3 (P = 0.54); I2 =0.0%
Test for overall effect: Z = 1.48 (P = 0.14)
0.1 0.2 0.5 1.0 2.0 5.0 10.0
Favours control Favours treatment
Analysis 2.1. Comparison 2 Acupuncture versus wait list control, Outcome 1 Reduction in severity of
depression.
Review: Acupuncture for depression
Comparison: 2 Acupuncture versus wait list control
Outcome: 1 Reduction in severity of depression
Study or subgroup Treatment Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Allen 1998 12 -11.7 (7.3) 11 -6.1 (10.9) 100.0 % -5.60 [ -13.25, 2.05 ]
Total (95% CI) 12 11 100.0 % -5.60 [ -13.25, 2.05 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.43 (P = 0.15)
-10 -5 0 5 10
Favours treatment Favours control
20Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.2. Comparison 2 Acupuncture versus wait list control, Outcome 2 Improvement in depression.
Review: Acupuncture for depression
Comparison: 2 Acupuncture versus wait list control
Outcome: 2 Improvement in depression
Study or subgroup Treatment Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Allen 1998 5/12 2/11 100.0 % 2.29 [ 0.55, 9.49 ]
Total (95% CI) 12 11 100.0 % 2.29 [ 0.55, 9.49 ]
Total events: 5 (Treatment), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.14 (P = 0.25)
0.1 0.2 0.5 1.0 2.0 5.0 10.0
Favours control Favours treatment
Analysis 3.1. Comparison 3 Acupuncture versus non-specific acupuncture, Outcome 1 Reduction in severity
of depression.
Review: Acupuncture for depression
Comparison: 3 Acupuncture versus non-specific acupuncture
Outcome: 1 Reduction in severity of depression
Study or subgroup Treatment Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Allen 1998 12 -11.7 (7.3) 11 -2.9 (7.9) 100.0 % -8.80 [ -15.03, -2.57 ]
Total (95% CI) 12 11 100.0 % -8.80 [ -15.03, -2.57 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.77 (P = 0.0057)
-10 -5 0 5 10
Favours treatment Favours control
21Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.2. Comparison 3 Acupuncture versus non-specific acupuncture, Outcome 2 Improvement in
depression.
Review: Acupuncture for depression
Comparison: 3 Acupuncture versus non-specific acupuncture
Outcome: 2 Improvement in depression
Study or subgroup Treatment Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Allen 1998 5/12 1/11 100.0 % 4.58 [ 0.63, 33.36 ]
Total (95% CI) 12 11 100.0 % 4.58 [ 0.63, 33.36 ]
Total events: 5 (Treatment), 1 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.50 (P = 0.13)
0.1 0.2 0.5 1.0 2.0 5.0 10.0
Favours control Favours treatment
Analysis 4.1. Comparison 4 Acupuncture plus medication versus medication, Outcome 1 Reduction in
severity of depression.
Review: Acupuncture for depression
Comparison: 4 Acupuncture plus medication versus medication
Outcome: 1 Reduction in severity of depression
Study or subgroup Treatment Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Luo 1998 10 13 (2.5) 11 9.9 (2.3) 100.0 % 3.10 [ 1.04, 5.16 ]
Total (95% CI) 10 11 100.0 % 3.10 [ 1.04, 5.16 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.95 (P = 0.0032)
-10 -5 0 5 10
Favours treatment Favours control
22Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.2. Comparison 4 Acupuncture plus medication versus medication, Outcome 2 Improvement in
depression.
Review: Acupuncture for depression
Comparison: 4 Acupuncture plus medication versus medication
Outcome: 2 Improvement in depression
Study or subgroup Treatment Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Roschke 2000 4/22 1/24 100.0 % 4.36 [ 0.53, 36.12 ]
Total (95% CI) 22 24 100.0 % 4.36 [ 0.53, 36.12 ]
Total events: 4 (Treatment), 1 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.37 (P = 0.17)
0.1 0.2 0.5 1.0 2.0 5.0 10.0
Favours treatment Favours control
Analysis 5.1. Comparison 5 Acupuncture plus medication versus acupuncture plus placebo, Outcome 1
Reduction in severity of depression.
Review: Acupuncture for depression
Comparison: 5 Acupuncture plus medication versus acupuncture plus placebo
Outcome: 1 Reduction in severity of depression
Study or subgroup Treatment Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Luo 1998 10 13 (2.5) 8 11.6 (2.5) 100.0 % 1.40 [ -0.92, 3.72 ]
Total (95% CI) 10 8 100.0 % 1.40 [ -0.92, 3.72 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.18 (P = 0.24)
-10 -5 0 5 10
Favours treatment Favours control
23Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.2. Comparison 5 Acupuncture plus medication versus acupuncture plus placebo, Outcome 2
Improvement in depression.
Review: Acupuncture for depression
Comparison: 5 Acupuncture plus medication versus acupuncture plus placebo
Outcome: 2 Improvement in depression
Study or subgroup Treatment Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Roschke 2000 4/22 8/24 100.0 % 0.55 [ 0.19, 1.56 ]
Total (95% CI) 22 24 100.0 % 0.55 [ 0.19, 1.56 ]
Total events: 4 (Treatment), 8 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.13 (P = 0.26)
0.1 0.2 0.5 1.0 2.0 5.0 10.0
Favours treatment Favours control
W H A T ’ S N E W
Last assessed as up-to-date: 16 March 2004.
31 October 2008 Amended Converted to new review format.
H I S T O R Y
Protocol first published: Issue 1, 2003
Review first published: Issue 2, 2005
17 March 2004 New citation required and conclusions have changed Substantive amendment
C O N T R I B U T I O N S O F A U T H O R S
Caroline Smith conceptualised and took the lead in writing the protocol and review, performed initial searches of databases for trials,
was involved in selecting trials for inclusion, performed data extraction and quality assessment of the included trials, was responsible
for statistical analysis and interpretation of the data.
Phillipa Hay was involved with selecting trials for inclusion, performed data extraction and quality assessment of the included trials,
interpretation of the data and commented on drafts of the protocol and review.
24Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D E C L A R A T I O N S O F I N T E R E S T
None
S O U R C E S O F S U P P O R T
Internal sources
• The University of South Australia, James Cook University, Australia.
External sources
• No sources of support supplied
I N D E X T E R M S
Medical Subject Headings (MeSH)
∗Acupuncture Therapy; Depression [∗therapy]; Randomized Controlled Trials as Topic
MeSH check words
Female; Humans; Male
25Acupuncture for depression (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.






![Back pain: Therapy for chronic low back pain Depression ......[O= alleviate pain / treat symptoms of mild depression]? CAM therapy chiropractic acupuncture “physical therapy” nonsurgical](https://img.pdfslide.us/doc/110x75/5f4f34548b8ffe6fa7196196/back-pain-therapy-for-chronic-low-back-pain-depression-o-alleviate-pain.jpg)