Embed Size (px)
Citation preview

Research ArticleAcupuncture and Related Therapies for Obesity:A Network Meta-Analysis
Yanji Zhang ,1 Jia Li ,1,2,3 GuoyanMo,4 Jing Liu,1
Huisheng Yang,5 Xianglin Chen ,1 Hui Liu ,1 Teng Cai ,1 Xian Zhang ,1
Xiangmin Tian ,1 Zhongyu Zhou ,2,3 andWei Huang 2,3
1College of Acupuncture and Orthopedics, Hubei University ofChinese Medicine/Hubei Provincial Collaborative Innovation Center of Preventive Treatment byAcupuncture and Moxibustion, Wuhan, China
2Department of Acupuncture, Hubei Provincial Hospital of Traditional Chinese Medicine, Wuhan, China3Hubei Province Academy of Traditional Chinese Medicine, Wuhan, China4China Key Laboratory of TCM Resource and Prescription, Hubei University of Chinese Medicine,Ministry of Education, Wuhan, China
5Institute of Acupuncture and Moxibustion of China Academy of Chinese Medical Sciences, Beijing, China
Correspondence should be addressed to Zhongyu Zhou; [email protected] andWei Huang; [email protected]
Received 21 August 2018; Accepted 9 September 2018; Published 30 September 2018
Academic Editor: Mariangela Rondanelli
Copyright © 2018 Yanji Zhang et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Obesity is a worldwide public health problem. Currently, increasing evidence suggests acupuncture and related therapies areeffective for obesity. This network meta-analysis (NMA) was performed to compare the effectiveness of different acupuncture andrelated therapies. We searched potential randomized controlled trials (RCTs) in three international databases. Thirty-four trialsinvolving 2283 participants were included. Pairwise meta-analysis showed that acupuncture and related therapies were superior tolifestyle modification and placebo in reducing weight and body mass index (BMI). Based on decreases in body weight, resultsfrom NMA showed that acupoint catgut embedding (standard mean difference [SMD]: 1.26; 95% credible interval [95% CI],0.46–2.06), acupuncture (SMD: 2.72; 95% CrI, 0.06–5.29), and combination of acupuncture and related theories (SMD: 3.65; 95%CrI, 0.96–6.94) were more effective than placebo. Another NMA result indicated that acupoint catgut embedding (SMD: 0.63;95% CI, 0.25–1.11), acupuncture (SMD: 1.28; 95% CrI, 0.43–2.06), combination of acupuncture and related therapies (SMD: 1.44;95% CrI, 0.64–2.38), and electroacupuncture (SMD: 0.60; 95% CrI, 0.03–1.22) were superior to lifestyle modification in decreasingBMI. Combination of acupuncture and related therapieswas ranked the optimalmethod for both reducingweight andBMI. Furtherstudies will clarify which combination of acupuncture and related therapies is better.
1. Introduction
Obesity, a worldwide public health problem, is described asan adiposity-based chronic disease [1]. Currently, guidelinesrecommended using body mass index (BMI) to classifyindividuals as having obesity (BMI ⩾30 kg/m2) [2]. Based onthe survey conducted previously, the standardized prevalencerates for obesity in adult were 34.9% in United States and17.7% in China [3, 4]. Moreover, it is associated with otherhealth concerns, such as insulin resistance, type 2 diabetes
mellitus, cardiovascular disease, and cancer, which increasedindividuals and societies’ medical burden [5].
Lifestyle modification, pharmacotherapy, and bariatricsurgery are considered the mainstay of therapy for obesity[2]. Although diet and exercise play an essential role in theweight management, their precise mode of action remainscontroversial [6]. Five long-term medicines (naltrexone-bupropion, phentermine-topiramate orlistat, lorcaserin, andliraglutide) have been approved by US Food and DrugAdministration (FDA) for the treatment of obesity [7]. The
HindawiEvidence-Based Complementary and Alternative MedicineVolume 2018, Article ID 9569685, 20 pageshttps://doi.org/10.1155/2018/9569685

2 Evidence-Based Complementary and Alternative Medicine
latest research suggested that phentermine-topiramate wasassociated with the highest possibility of achieving at least 5%weight loss [7]. However, little is known about the long-termsafety profile of pharmacotherapy for weight loss. The effec-tiveness of bariatric procedures for treating obesity has beenreported in several randomized controlled trials (RCTs) [8–10]. Nevertheless, the evidence on cardiovascular disease andmortality remains to be validated [11]. Therefore, it is neces-sary to explore other forms of alternative therapies which areboth safe and effective in preventing gaining weight.
In reviewing the literature, it became evident that acu-puncture and related therapies have been wildly used for obe-sity treatment. As mentioned in the meta-analysis, combina-tion of acupuncture and lifestyle modification is more effec-tive compared with lifestyle modification alone [12]. Resultsof Yeh’s research suggested that ear acupoint stimulation hadremarkable improvements in the anthropometric parametersof Body Weight (BW), BMI, and so on [13]. In addition,another systematic review performed in 2015 has also shownthat clinical efficacy of acupoint catgut embedding therapywas better than that of the control group for simple obesity[14]. However, a major problem is that whether acupunctureor acupuncture-related therapies alone or combined therapyis more effective than lifestyle modification managementremains disputable.
By using the technique of network meta-analysis (NMA),both direct and indirect randomized data can be analyzed,and recommended rankings of different treatments can beprovided [15, 16]. Therefore, we conducted this Bayesian net-work meta-analysis to analyse both direct and indirect com-parisons of acupuncture and related methods for treatingobesity. In this paper, changes in BW, BMI, and the rates ofcomplications of included studies were analyzed.
2. Methods
Our research was conducted following the Preferred Report-ing Items for Systematic Reviews andMeta-Analyses for Net-work Meta-Analysis (PRISMA-NMA) checklist [17] (seeAppendix 1).
2.1. Data Sources and Search Strategy. Three electronic inter-national databases (PubMed/Medline, Embase, and the Co-chrane Library) were searched for potential RCTs (random-ized controlled trials). We identified articles published frominitiation to December 2017 with a limit to studies of RCTand without limitations on language or the form they are
published in. The complete search strategies are shown inAppendix 2.
2.2. Study Selection. Two researchers (XC and HL) inde-pendently identified irrelevant research based on titles andabstracts. Additionally, full-text articles were scanned bythese two researchers to identify eligible studies. All disagree-ments were resolved by consensus and adjudged by a thirdreviewer (TC) if necessary. In case of duplicate citations, themost updated studies were selected for data extraction.
2.3. Inclusion and Exclusion Criteria. The studies included intheNMAmet the following criteria: (1) the study designmustbe a randomized controlled clinical trial (RCT); (2) patientsdiagnosed with simple obesity irrespective of ages and sex asstudy subjects; diagnostic criteria must be clear and inclusionand exclusion criteria were explicit; (3) at least one of thefollowing efficacy outcomes or safety endpoints was included:BW, BMI, and adverse events; (4) participants in the experi-mental group have received acupuncture and related treat-ments (specifically, classical body acupuncture; electroacu-puncture auricular acupoint stimulation; acupoint catgutembedding and warming acupuncture) alone or in combina-tion; (5) English or Chinese language studies.
The following were excluded: (1) self-control and non-RCTs; (2) preclinical studies, systematic reviews, case reports,and meta-analyses; (3) reports without sufficient and clearoriginal data; (4) participants having received other forms ofacupuncture such as transcutaneous electrical nerve stimu-lation or laser acupuncture; (5) duplicate studies and studiesreporting the same results.
2.4. Data Collection and Quality Assessment. According toa standard data collection sheet, two investigators (TC andXZ) independently extracted the following data: (1) maincharacteristics of included randomized controlled trials (i.e.,year of publication, type of intervention, patients charac-teristics, types of outcome, and reported adverse events);(2) details of acupuncture and related interventions (i.e.,frequency and duration of acupuncture sessions, names ofacupuncture points used, and retention time); (3) clinical out-come (i.e., summaries of mean, standard difference, andsample size between treatment groups). In some trials, thechange between baseline and after treatmentwas failed to pre-sent. Using the methods recommended in the CochraneHandbook for Systematic Reviews of Interventions (version5.1) [18], the missing data was estimated using the followingformula:
𝑋𝑐ℎ𝑎𝑛𝑔𝑒 = 𝑋𝑝𝑜𝑠𝑡−𝑡𝑟𝑒𝑎𝑡𝑚𝑒𝑛𝑡 − 𝑋𝑏𝑎𝑠𝑒𝑙𝑖𝑛𝑒 (1)
𝑆𝐷𝑐ℎ𝑎𝑛𝑔𝑒 = √(𝑆𝐷𝑏𝑎𝑠𝑒𝑙𝑖𝑛𝑒)2 + (𝑆𝐷𝑝𝑜𝑠𝑡−𝑡𝑟𝑒𝑎𝑡𝑚𝑒𝑛𝑡)2 − 2 × 𝑟 × 𝑆𝐷𝑏𝑎𝑠𝑒𝑙𝑖𝑛𝑒 × 𝑆𝐷𝑝𝑜𝑠𝑡−𝑡𝑟𝑒𝑎𝑡𝑚𝑒𝑛𝑡 (2)
where r is a correlation coefficient with a value of 0.5[19]. For each included RCT, two researches (XT and XC)
independently assessed their risk of bias by the CochraneCollaboration tool [20]. Bias risks of each study were assessed

Evidence-Based Complementary and Alternative Medicine 3
from six aspects: random sequence generation, allocationconcealment, blinding of participants and investigators,blinding of outcome assessment, incomplete outcome dataaddressed, and selective outcome reporting, while ranked inhigh risk, low risk, and unclear risk.
2.5. Statistical Analysis. Firstly, standard pairwise meta-anal-ysis was initially performed using the Review Manager(Version 5.3, Cochrane Collaboration, Oxford, UK). Wecalculated I-square (I2) test to assess heterogeneity amongRCTs [21]. To be specific, when there was I2 > 50%, they wereanalysed using a random effects model; otherwise, a fixedeffect model was chosen. Subgroup analyses were conductedaccording to the type of acupuncture treatment and the treat-ment of control group. Mean difference (MD) with 95% con-fidence intervals (CI) was used to analyze continuous data.We generated forest plots to illustrate the relative strengthof curative effects.
Second, to indirectly compare the effectiveness amongtreatments of acupuncture and related therapies, we did arandom effects model NMAwithin a Bayesian framework, byusingWinBUGS (Version 1.4.3,MRCBiostatisticsUnit, Cam-bridge, UK) [22, 23]. Models were computed with MarkovchainMonte Carlo (MCMC) simulation methods, using fourchains with overdispersed initial values. We utilized theMarkov chains for 50,000 simultaneous iterations after thefirst 20000 iterations were discarded because they may havean influence on the arbitrary value. In this process, the con-vergence of the model was assessed by the Brooks-Gelman-Rubin (BGR) method; a value of potential scale reductionfactor (PSRF) close to 1 indicated the better convergence [24].The continuous outcome was measured by a standard meandifference (SMD) with a 95% credible intervals (CrI) for in-direct comparisons.
Finally, plot of surface under the cumulative rankingcurve (SUCRA) was generated using the STATA software(Version 13.0; Stata Corporation, College Station, Texas,USA), which indicated the probability of each interventionof being ranked best [25]. In our study, higher SUCRA scoresmean the higher rank of the treatment [15]. A Z value and itscorresponding p-value were calculated, and an R value lessthan 0.05 indicated a statistically significant difference.
3. Results
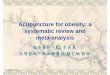
3.1. Study Search. Weperformed this research onDec 26 2017.As shown in Figure 1, a total of 1050 records were initiallyidentified from the databases. 675 studies left after duplicateswere removed. 577 recordswere excluded after carefully scan-ning titles and abstracts. Finally, 34 trials with 2283 partici-pants were included in our NMA [26–59], covering 8 groups,manual acupuncture; electroacupuncture; auricular acupointstimulation; acupoint catgut embedding; pharmacotherapy;warming acupuncture; lifestyle modification; placebo.
3.2. StudyDescription. Main characteristics of includedRCTswere shown in Table 1. The participants were from Australia[28], the United States [26], Turkey [46], Korea [51], Iran
[36], Egypt [48], and China. Age of participants ranged from15 to 70 years, while the sample size of the studies rangedfrom 12 to 86. Among the included RCTs, there were onefour-arm trials, 5 three-arm trials, and 28 two-arm trials.Fourteen studies compared acupuncture to placebo. Tenstudies compared acupuncture to lifestyle intervention. Sixstudies compared combined therapies to acupuncture alone.Details about acupuncture points used, retention time, fre-quency, and duration of acupuncture sessions were shown inTable 2. In these research, 30 articles [26–30, 32, 34–38, 41–59] reported the weight loss, while 25 articles reported thechange in BMI. The details of mean, standard difference(SD), and sample size between different groups for eligiblestudies are summarized in Appendix 3. The Cochrane risk ofbias assessment was presented in Table 3. Furthermore, thenetwork plot of included comparisons was shown in Figure 2.
3.3. Pairwise Meta-Analyses
3.3.1. Body Weight. A direct pairwise meta-analysis showedthat acupuncture and related therapies showed a greater BWreduction than lifestyle modification (MD: 1.66; 95% Confi-dence interval, 0.63to2.70) and placebo (MD: 1.15; 95% CI,0.67to1.63). When compared to acupuncture, combinationof acupuncture and related theories showed a marginallystronger effect in weight loss (MD: 1.56; 95% CI, 0.07to3.05).There was no statistically significant difference betweencombination of acupuncture and related theories and phar-macotherapy in their effectiveness in BW (MD: 2.44; 95%CI,-1.98to6.86). (Table 4)
BMI. As for the comparison in reducing BMI, acupunctureand related therapies were found to be marginally superiorto lifestyle modification (MD: 1.17; 95% CI, 0.09to2.26) andplacebo (MD: 0.57; 95%CI, 0.40to0.74).The remaining directcomparisons did not show significant differences (Table 4).
3.4. Network Meta-Analysis
3.4.1. Body Weight. The NMA showed that all treatmentsother than acupuncture combined lifestyle modification weremore efficacious than lifestyle modification. Three treat-ments were significantly more effective than placebo. Specif-ically, acupoint catgut embedding (SMD: 1.26; 95% credibleinterval, 0.46to2.06), acupuncture (SMD: 2.72; 95% CrI,0.06to5.29), and combination of acupuncture and relatedtherapies (SMD: 3.65; 95% CrI, 0.96to6.94). Furthermore,moxibustion with warming needle was associated with asignificantly improvement than lifestyle modification (SMD:-5.24; 95% CrI, -10.15to-0.55) (Table 5).
3.4.2. BMI. Four treatments showed superiority overplacebo, including acupoint catgut embedding (SMD: 1.31;95% CrI, 0.36to2.06), acupuncture (SMD: 1.94; 95% CrI,0.83to3.00), combination of acupuncture and related theories(SMD: 3.65; 95% CrI, 0.96to6.94), and electroacupuncture(SMD: 1.28; 95% CrI, 0.43to2.11). Four treatments weresignificantly more effective than lifestyle modification,including acupoint catgut embedding (SMD: 0.63; 95% CI,

4 Evidence-Based Complementary and Alternative Medicine
Records identified through database searching
(n = 1050)Sc
reen
ing
Incl
uded
Elig
ibili
tyId
entifi
catio
n
Recordsa�er duplicates removed(n =675)
Records excluded a�er readingtitles and abstracts (n = 577)
Full-text articles assessedfor eligibility
(n =98)
Full-text articles excluded, withreasons(n =63)
Duplicates(n =8)Non-RCTs(n=23)Non-Acupuncture(n=12)Obesity with complications(n = 8)Not included outcome (n = 7)Other(n = 6)
Studies included in quantitative synthesis
(meta-analysis)(n =34)
Figure 1: PRISMA flow chart.
AAS
ACE
AR+LMAcupuncture
Combined theories
EA
LM
Pharmacotherapy
Placebo
WA
AAS
ACE
AR+LMAcupuncture
Combined theories
EA
LMPharmacotherapy
Placebo
BMIBody weight
Figure 2: Network plot. BMI: body mass index; LM: lifestyle modification; AAS: auricular acupoint stimulation; EA: electroacupuncture;ACE: acupoint catgut embedding; WA: warming acupuncture; AR: acupuncture and related therapies; combined therapies: combination ofacupuncture and related therapies.

Evidence-Based Complementary and Alternative Medicine 5
Table1:Maincharacteris
ticso
fincludedrand
omized
controlledtrials.
Stud
yID
andCou
ntry
Samples
izeR
/AAge:m
ean(SD)o
rrange
R/A
Interventio
nCon
trol
Adversee
ventsreported
R/A
Type
ofou
tcom
es
Allisonetal.[17]1995,USA
35/34
19-7
0AAS
Placebo
Redn
ess,pain,bleeding
BW,
Hsu
etal.[18]2
005,Taiwan
24/22
41.5(11.2
)/41.0(10.0)
EALM
Ecchym
osis(2),a
bdom
inal
discom
fort(1)
/Non
eBW
,BMI
Richards
etal.[19]1998,Au
stralia
28/32
44.1(11.7
)/43.0(13.6)
AAS
Placebo
intercurrent
illnessand
discon
tinued(1)/N
one
BW
Hee
tal.[20]
2008,C
hina
40/40
18-5
0Com
binedtherapies#
Pharmacotherapy
NR
BW,B
MI
Lietal.[21]2
006,Ch
ina
26/30
16.00(1.3
8)/16
.00(1.9
5)EA
LMNR
BMI
29/30
15.00(2.04
)/16.00(1.9
5)AAS
Tong
etal.[22]2
011,Ch
ina
76/42
35.08(9.3
1)/34.60
(8.55)
Acup
uncture
Placebo
Adversee
ventsV
AS
BMI
Hsu
etal.[23]2
009,Taiwan
23/22
40.0(10.5)/39.4
(13.6)
AAS
Placebo
Minor-in
flammation(1),
mild
tend
erness(7)/mild
tend
erness(2)
BW,B
MI
Hsie
hetal.[24]2
010,Taiwan
26/26
18-2
0AAS
Placebo
NR
BMI
Hsie
hetal.[25]2
011,Taiwan
27/28
18-2
0AAS
Placebo
NR
BWAb
dietal.[26]2
012,Iran
86/83
37.29(1.0
)/38.73(
1.1)
AAS
Placebo
Non
eBW
,BMI
Darband
ietal.[27]
2012,Iran
43/43
37.57(9.2
6)/37.6
5(9.7
1)AR+
LMPlacebo
Non
eBW
,BMI,
Hee
tal.[28]
2012,C
hina
30/30
18-54
AR+
LMLM
NR
BW,B
MI
Lien
etal.[29]2
012,Taiwan
24/23
39.2(11.6
)/40
.7(9.7)
AAS
Placebo
Dizziness(1)
/Non
eBW
,BMI
Darband
ietal.[30]
2014,Iran
20/20
38.0(0.9)/38.0(1.3)
EAPlacebo(EA
)Non
eBW
,BMI
20/20
39.0(1.8)/37.9(1.5)
AAS
Placebo(AAS)
Yehetal.[31]2
015,Taiwan
36/34
29.9(7.7)/32.8(9.5)
EAPlacebo
NR
BMI
Chen
etal.[32]2
007,Ch
ina
40/40
43.1(13.6)/44
.6(10.3)
ACE
Acup
uncture
NR
BW,B
MI
Huang
etal.[33]2
011,Ch
ina
30/30
NR
ACE
EANR
BW,B
MI
Tang
etal.[34]2
009,Ch
ina
33/32
21-54/22-55
Com
binedtherapies
EANR
BW,B
MI

6 Evidence-Based Complementary and Alternative Medicine
Table1:Con
tinued.
Stud
yID
andCou
ntry
Samples
izeR
/AAge:m
ean(SD)o
rrange
R/A
Interventio
nCon
trol
Adversee
ventsreported
R/A
Type
ofou
tcom
es
Shietal,[35]
2006
,China
40/42
17-49/18-51
Com
binedtherapies
EANR
BW,B
MI
Hsu
etal.[36]2
005,Taiwan
22/20
40.0(11.5
)/41.3(9.9)
EALM
mild
Ecchym
osis(3),
abdo
minal
discom
fort(1)
/Non
eBW
,BMI
Guceletal.[37]2
012,Tu
rkey
20/20
34.6±6.
3/36.8±7.
8Ac
upun
cture
Placebo
NR
BW,B
MI
Dengetal.[38]2
014,Ch
ina
30/30
32(7)/33(7)
Com
binedtherapies
Acup
uncture
NR
BW30/30
32(7)/33(8)
ACE
Hassanetal.[39]2
014,Eg
ypt
21/30
45.00(9.32
)/43.47(9.59)
AR+
LMLM
NR
BW,B
MI
Hee
tal.[40]
2014,C
hina
28/28
NR
Com
binedtherapies
Acup
uncture
NR
BW,B
MI
Wangetal.[41]2
013,Ch
ina
45/45
31(10)/32(12)
EAAc
upun
cture
NR
BMI
Sujung
etal.[42]2
014,SouthKo
rea
22/15
34.7(11.9
)/42.7(10.2)
AAS
Placebo
NR
BW,B
MI
Buetal.[43]2
007,Ch
ina
32/23
32.1(1.1)/33.4(1.3)
Com
binedtherapies
Acup
uncture
NR
BW,B
MI
Shietal.[44]
2005,C
hina
36/32
19∼58
/18∼56
WA
EANR
BWYang
etal.[45]2
010,Ch
ina
31/30
18∼42
/18∼48
AR+
LMLM
NR
BW
Cabiogluetal.[46]2
005,Tu
rkey
22/12
39.8(5.3)/43.3(4.3)
EAPlacebo
NR
BW22/21
39.8(5.3)/42.7(3.9)
LM
Cabiogluetal.[47]2
006,Tu
rkey
20/15
42.1(4.4)/41.8
(4.6)
EAPlacebo
NR
BW20/15
42.1(4.4)/42.9(4.3)
LM
Cabiogluetal.[48]2
008,Tu
rkey
20/15
40.55(
5.30)/41.47(4.61)
EAPlacebo
NR
BW20/23
40.55(
5.30)/42.91(4.02)
LMDarband
ietal.[49]
2013,Iran
42/44
36.50(9.26)/36.48
(8.69)
AR+
LMPlacebo
NR
BW,B
MI
Fogartye
tal.[50]
2015,A
ustralia
19/16
>18AR+
LMPlacebo
NR
BMI
BW:bod
yweight;BM
I:bo
dymassind
ex;L
M:lifesty
lemod
ificatio
n;AAS:auric
ular
acup
oint
stimulation;
EA:electroacup
uncture;AC
E:acup
oint
catgut
embedd
ing;WA:w
armingacup
uncture;AR:
acup
uncture
andrelatedtherapies;#com
binatio
nof
acup
unctureandrelatedtherapies.

Evidence-Based Complementary and Alternative Medicine 7
Table2:Descriptio
nsof
theincludedacup
uncturea
ndrelatedtherapies.
Stud
yID
(Cou
ntry)
Styleo
facupu
ncture
Nam
esof
acup
uncturep
ointsu
sed
Retentiontim
eFrequency&
duratio
nof
Acup
uncturesessio
nsAllisonetal.1995,USA
AAS
NR
2-3m
in3sessions
daily
for12we
eks
Hsu
etal.200
5,Taiwan
EA
Qiai(R
EN9),Shu
ifen(RE
N9)
Shuidao(ST
28),Siman(K
14)
Zusanli(S
T26),Fenglon
g(ST
40)
Sang
injao(SP
6)
40min
2sessions
weeklyfor6
weeks
Richards
etal.1998,
Austr
alia
AAS
Shenmen(TF4
),Stom
ach(CO4)
15-20m
in2sessions
daily
for4
weeks
Hee
tal.2008,C
hina
Com
binedtherapies#
Eara
cupressure:
Shenmen(TF4
),Neifenm
i(CO18),
Pi(C
O13),Wei(C
O14),
Sanjiao(CO17),Dachang
(CO7),
Naodian
Body
acup
uncture:
Tianshu(ST
25),Guanyuan(RN
4)Sanyinjiso(SP
9),Fenglon
g(ST
40)
Zusanli(S
T36)
Eara
cupressure:3days
Body
acup
uncture:3
0min
Eara
cupressure:1sessionevery3
days
with
atotalof
10sessions
Body
acup
uncture:Th
efirst5
days
oftre
atment1
time,5days
after
treatment1,1
mon
th,for
acou
rseo
ftre
atment.
Lietal.200
6,Ch
ina
EA
Sang
injao(SP
6),T
ianshu
(ST2
5)Zu
sanli(S
T36),Q
uchi(LI11
)Feng
long
(ST4
0),N
eitin
g(ST
44)
Zhon
gwan(C
V12),Pishu(BL
20)
Shenshu(BL
23),Qihai(C
V6)
Yinlingquan(SP
9),
Shangjux
u(ST
37)T
aichon
g(LR
3)
10min
1sessio
ndaily
with
atotalof
60sessions,2
days
restin-betwe
en10
sessions
AAS
Hun
gerp
oint
Pizhixia(AT4
)Sh
enmen(TF4
),Sh
enshangxian(TG
2P)
Sanjiao(CO17),Pi(C
O13)
Wei(C
O14),Fei(C
O14)
Kou(CO1),D
achang
(CO7)
Zhichang
xidu
an(H
X2)
15-20m
in1sessio
ndaily
with
atotalof
10sessions
for10we
eks,2dayrest
in-betwe
en10
sessions
Tong
etal.2011,Ch
ina
Acup
uncture
Zhon
gwan(C
V12),Zh
ongji(C
V3)
Daheng(SP
15),Xiaw
an(C
V10)
Shim
en(C
V5),T
ianshu
(ST2
5)Liangqiu(ST3
4),Z
usanli(ST
36)
Yinlingquan(SP
9)
30min
1sessio
neveryo
ther
dayfora
total
of5we
eksw
ith12
sessions
Hsu
etal.200
9,Taiwan
AAS
Hun
gerp
oint,Shenm
enpo
int(T
F4)
Stom
achpo
int(C
O4),
Endo
crinep
oint(C
O18)
3days
2sessions
weeklyfora
totalof6
weeksw
ith12
sessions
Hsie
hetal.2010,Taiwan
AAS
NR
2/3d
ays
1sessio
nwe
eklyfor10sessions
Hsie
hetal.2011,Taiwan
AAS
NR
NR
1sessio
nwe
eklyfora
totalofeight
weeks

8 Evidence-Based Complementary and Alternative Medicine
Table2:Con
tinued.
Stud
yID
(Cou
ntry)
Styleo
facupu
ncture
Nam
esof
acup
uncturep
ointsu
sed
Retentiontim
eFrequency&
duratio
nof
Acup
uncturesessio
ns
Abdi
etal.2012,Iran
AAS
Shenmen(TF4
),Stom
ach(CO4)
Hun
gerp
oint
Mou
th(C
O1)
Centre
ofear(HX1),Sanjiao(CO17)
3days
Twicea
week
fora
totalof6
weeks
Darband
ietal.2012,Iran
AAS
Shenmen(TF4
),Stom
ach(CO4)
Hun
gerp
oint
Mou
th(C
O1)
Centre
ofear(HX1),Sanjiao(CO17)
3days
Twicea
week
fora
totalof6
weeks
Hee
tal.2012,C
hina
AAS
Hun
gerp
oint
Stom
ach(CO4)
Spleen(C
O14),LargeIntestin
e(CO7)
Endo
crine(CO18),Sh
enmen(TF4
)3d
ays
3tim
esad
ayfor4
weeks
Lien
etal.2012,Taiwan
AAS
Shenmen
point(T
F4),Stom
ach
point(C
O4)
Hun
gerp
oint,E
ndocrin
epo
int(C
O18)
NR
3sessio
nwe
eklywith
atotalof
12sessions
for4
weeks
Placebo
Shenmen
point(T
F4),Stom
ach
point(C
O4)
Hun
gerp
oint,E
ndocrin
epo
int(C
O18)
NR
3sessions
weeklywith
atotalof
12sessions
for4
weeks
Darband
ietal.2014,Iran
EA
Tianshu(ST-25),Weidao(GB2
8)Zh
ongw
an(REN
12),Shuifen(RE
N9)
Guanyuan(RE
N4),Sanyinjiao(SP
6)Quchi(LI11),Fenlong
(ST4
0)Qihai(REN
6),Y
inlin
gquan(SP9
)
20min
2sessions
weeklyfora
totalof6
weeks
AAS
Shenmen
(TF4
),Stom
ach(C
O4)
Hun
gerp
oint,M
outh
(CO1)
Centero
fear
(HX1),Sanjiao(C
O17)
3days
2sessions
weeklyfora
totalof6
weeks
Yehetal.2015,Taiwan
EASh
enmen
(TF4
),Stom
achCO4)
Endo
crine(CO18)
Hun
gerp
oint
20min
NR
Chen
etal.200
7,Ch
ina
ACE
Liangqiu(ST3
4),Z
hong
wan(C
V12)
Tianshu(ST
25),Shuifen(CV
9)Feng
long
(ST4
0)Awe
ek1sessio
nwe
eklywith
atotalof
30sessions
for4
weeks
Acup
uncture
Liangqiu(ST3
4),Z
hong
wan(C
V12)
Tianshu(ST
25),Shuifen(CV
9)Feng
long
(ST4
0)45
min
Thefi
rst5
days
are1
times
aday,
and1tim
eafter5
days,1
mon
this1
course
oftre
atment.
Huang
etal.2011,Ch
ina
ACE
One
setisT
ianshu
(ST2
5)Zh
ongw
an(C
V12),Guanyuan(CV
4)Zu
sanli(S
T36),W
eishu(BL
21)
Ashixue
24ho
ur1sessio
nwe
eklywith
atotalof
7sessions
for6
0days
EA
Zhon
gwan(C
V12),Tianshu(ST
25)
Daheng(SP
15),Shuifen(CV
9)QIhai(C
V6),G
uanyuan(CV
4)Zu
sanli(S
T36),A
shixue
30min
3sessions
weeklywith
atotalof
12sessions
for6
0days

Evidence-Based Complementary and Alternative Medicine 9Ta
ble2:Con
tinued.
Stud
yID
(Cou
ntry)
Styleo
facupu
ncture
Nam
esof
acup
uncturep
ointsu
sed
Retentiontim
eFrequency&
duratio
nof
Acup
uncturesessio
ns
Tang
etal.200
9,Ch
ina
Com
binedtherapies
EA:
Zhon
gwan(C
V12),Xiaw
an(C
V10)
Guanyuan(CV
4),T
ianshu
(ST2
5)Shuifen(CV
9),Sanyinjiao(SP
6)Zu
sanli(S
T36),X
uehai(S
P10)
Xinshu
(BL15),G
eshu
(BL17)
Pishu(BL
20)
ACE:
Zhon
gwan(C
V12),Tianshu(ST
25)
Qihai(C
V6),T
ianshu
(ST2
5)Liangqiu(ST3
4),Z
usanli(ST
36)
Gon
gsun
(SP4
),Xinshu
(BL15)
Pishu(BL
20)
EA:30m
in
EA:Th
efirst3
days
are1
times
aday,
and1tim
eafte
r3days,15days
is1
course
oftre
atment.
ACE:Afte
rthe
firstacup
oint
catgut
embedd
ingfor3
consecutivetim
es,
theintervalisb
uriedforthe
second
timea
fter15days,and
the
acup
unctureisp
erform
edforthe
third
timea
fterthe
endof
the
treatmentp
eriod.
EA
Zhon
gwan(C
V12),Xiaw
an(C
V10)
Guanyuan(CV
4),T
ianshu
(ST2
5)Shuifen(CV
9),Sanyinjiao(SP
6)Zu
sanli(S
T36),X
uehai(S
P10)
Xinshu
(BL15),G
eshu
(BL17)
Pishu(BL
20)
30min
Thefi
rst3
days
are1
times
aday,
and1tim
eafte
r3days,15days
is1
course
oftre
atment.
Shietal.2006
,China
Com
binedtherapies
Zhon
gwan(C
V12),Xiaw
an(C
V10)
Qihai(C
V6),Z
hong
ji(CV
3)Tianshu(ST
25),Daheng(SP
15)
Liangm
en(ST2
1),
Huaroum
en(ST2
4)Shuidao(ST
28),Quchi(C
V6)
Zhigou
(TE6
),Hegu(LI4)
Liangqiu(ST3
4),Z
usanlli(ST3
6)Sh
angjux
u(ST
37),Feng
long
(ST4
0)Sanyinjiao(SP
6),G
ongsun
(SP4
)Neitin
g((ST4
4)
30min
EA:Th
efirst3
days
are1
times
aday,
and1tim
eafte
r3days,15days
is1
course
oftre
atment.
ACE:
Afte
rthe
firstacup
oint
catgut
embedd
ingfor3
consecutivetim
es,
theintervalisb
uriedforthe
second
timea
fter15days,and
the
acup
unctureisp
erform
edforthe
third
timea
fterthe
endof
the
treatmentp
eriod.
EA
Zhon
gwan(C
V12),Xiaw
an(C
V10)
Qihai(C
V6),Z
hong
ji(CV
3)Tianshu(ST
25),Daheng(SP
15)
Liangm
en(ST2
1),
Huaroum
en(ST2
4)Shuidao(ST
28),
Quchi(C
V6)
Zhigou
(TE6
),Hegu(LI4)
Liangqiu(ST3
4),Z
usanlli(ST3
6)Sh
angjux
u(ST
37),Feng
long
(ST4
0)Sanyinjiao(SP
6),G
ongsun
(SP4
)Neitin
g((ST4
4)
30min
Thefi
rst3
days
are1
times
aday,
and1tim
eafte
r3days,15days
is1
course
oftre
atment.
Hsu
etal.200
5,Taiwan
EA
Qihai(REN
-6),Shuifen(REN
-9)
Shuidao(ST-28),Siman
(K-14)
Zusanli(ST
-26),Fenglon
g(ST
-40)
Sang
injao(SP-6)
40min
2sessions
weeklywith
atotalof
12sessions
for6
weeks

10 Evidence-Based Complementary and Alternative Medicine
Table2:Con
tinued.
Stud
yID
(Cou
ntry)
Styleo
facupu
ncture
Nam
esof
acup
uncturep
ointsu
sed
Retentiontim
eFrequency&
duratio
nof
Acup
uncturesessio
ns
Guceletal.2012,Tu
rkey
Acup
uncture
Hegu(LI4),Shenm
en(H
T7)
Zusanli(S
T36),N
eitin
g(ST
44)
Sanyinjiao(SP
6)20
min
2sessions
weeklywith
atotalof
10sessions
for5
weeks
Dengetal.2014,Ch
ina
Com
binedtherapies
Zhon
gwan
(CV12),Xiaw
an(C
V10)
Qihai(C
V6),G
uanyuan(
CV4)
Huaroum
en(ST24),Wailin
g(S
T26)
Daheng(SP15),Tianshu(ST25)
Yinjiao(C
V7),Z
higou(TE6)
Zusanll(ST
36)
NR
Acup
uncture:1
sessionevery3
days
with
atotalof
21sessions
for4
weeks,3days
restbetweenevery
session
Acup
oint
catgut
Embedd
ing:1sessio
nwe
eklywith
atotalof3
sessions
for3
weeks
Acup
uncture
Zhon
gwan
(CV12),Xiaw
an(C
V10)
Qihai(C
V6),G
uanyuan(
CV4)
Huaroum
en(ST24),Wailin
g(S
T26)
Daheng(SP15),Tianshu(ST25)
30min
1sessio
nevery3
days
with
atotalof
21sessions
for4
weeks,3days
rest
betweeneverys
essio
n
Acup
oint
catgut
embedd
ing
Zhon
gwan
(CV12),Tianshu(ST25)
Yinjiao(C
V7),Z
higou(TE6)
Guanyuan(
CV4),Z
usanli(ST36)
NR
1sessio
nwe
eklywith
atotalof
3sessions
for3
weeks
Hassanetal.2014,Eg
ypt
AR
NR
NR
NR
Hee
tal.2014,C
hina
AR
NR
NR
NR
acup
uncture
Tianshu(ST2
5),Liang
men(ST2
1)Daheng(SP15),Z
usanli(ST3
6)Sanyinjiao(SP
6),Q
uchi
(LI11
)Zh
igou
(SJ6),Zh
ongw
an(RN12)
Qihai(RN06
)
30min
1sessio
ndaily
with
atotalof
21sessions
for3
weeks
Wangetal.2013,Ch
ina
EA
Neitin
g(ST
44),Sh
angjux
u(ST
37)
Xiaju
xu(ST3
9),Fenglon
g(ST
40)
Tianshu(ST
25),Zu
sanli(S
T36)
Quchi(LI11
)
30min
1sessio
nevery2days
with
atotalof
12sessions
for3
weeks
Acup
uncture
Neitin
g(ST
44),Sh
angjux
u(ST
37)
Xiaju
xu(ST3
9),Fenglon
g(ST
40)
Tianshu(ST
25),Zu
sanli(S
T36)
Quchi(LI11
)
30min
1sessio
nevery2days
with
atotalof
12sessions
for3
weeks
Sujung
etal.2014,South
Korea
AAS
Shen-m
en(TF4
),Stom
ach(CO4)
Spleen(C
O13),Hun
gerp
oint
Endo
crine(C0
18)
NR
1sessio
nwe
eklywith
atotalof
8sessions
for8
weeks

Evidence-Based Complementary and Alternative Medicine 11
Table2:Con
tinued.
Stud
yID
(Cou
ntry)
Styleo
facupu
ncture
Nam
esof
acup
uncturep
ointsu
sed
Retentiontim
eFrequency&
duratio
nof
Acup
uncturesessio
ns
Buetal.200
7,Ch
ina
Com
binedtherapies
Acup
uncture:
Tianshu(ST
25),Guanyuan(CV
4)Zu
sanli(S
T36),Fenglon
g(ST
40)
Sanyinjiao(SP
6)AAS:
Shenmen(TF4
),En
docrine(C0
18)
Spleen(C
O13),Stom
ach(CO4)
Dachang
(CO7),Sanjiao(CO17
)Naodian
Acup
uncture:3
0min
eara
cupressure:1day
1sessio
neveryd
aywith
atotalof
10sessions
for6
weeks,1w
eekrest
in-betwe
en10
sessions.
Acup
uncture
Tianshu(ST
25),Guanyuan(CV
4)Zu
sanli(S
T36),Fenglon
g(ST
40)
Sanyinjiao(SP
6)30
min
1sessio
neveryd
aywith
atotalof
10sessions
for6
weeks,1w
eekrest
in-betwe
en10
sessions.
Shietal.2005,C
hina
Warmingacup
uncture
Zhon
gwan(C
V12),Shuifen(CV
9)Qihai(C
V6),Z
hong
ji(CV
3)Tianshu(ST
25),Shuidao(ST
28)
Neigu
an(PC6
),Hegu(LI4)
Xuehai(SP10),Z
usanli(ST
36)
Feng
long
(ST4
0),Sanyinjiao(SP
6)
40min
1sessio
neveryd
aywith
atotalof
15sessions
for4
weeks
EA
Zhon
gwan(C
V12),Shuifen(CV
9)Qihai(C
V6),Z
hong
ji(CV
3)Tianshu(ST
25),Shuidao(ST
28)
Neigu
an(PC6
),Hegu(LI4)
Xuehai(SP10),Z
usanli(ST
36)
Feng
long
(ST4
0),Sanyinjiao(SP
6)
40min
1sessio
neveryd
aywith
atotalof
15sessions
for4
weeks
Yang
etal.2010,Ch
ina
AR
Zhon
gwan(C
V12),Tianshu(ST
25)
Guanyuan(CV
4),Z
usanli(ST
36)
Feng
long
(ST4
0),Y
inlin
gquan(SP
9)Sanyinjiao(SP
6),P
ishu(BL
20)
Weishu(BL
21),Ashixue
30min
1sessio
ndaily
with
atotalof
15sessions
for7
weeks,3days
rest
betweeneverys
essio
n
Cabiogluetal.200
5,Tu
rkey
EA
Body
points:
Hegu(LI
4),T
ianshu
(ST25)
Quchi(LI11),Z
usanli(ST
36)
Neitin
g(ST
44
30min
Body
EAwas
perfo
rmed
everyday,
andEA
was
perfo
rmed
everyo
ther
day
Cabiogluetal.200
6,Tu
rkey
EABo
dypo
ints:
Quchi(LI11),Z
usanli(ST
36)
Neitin
g(ST
44)
30min
Body
EAapplicationwas
perfo
rmed
daily
for2
0days,and
EAwas
appliedto
each
earo
nalternating
days

12 Evidence-Based Complementary and Alternative Medicine
Table2:Con
tinued.
Stud
yID
(Cou
ntry)
Styleo
facupu
ncture
Nam
esof
acup
uncturep
ointsu
sed
Retentiontim
eFrequency&
duratio
nof
Acup
uncturesessio
ns
Cabiogluetal.200
8,Tu
rkey
EA
Body
points:
Hegu(LI
4),Q
uchi(LI11)
Tianshu(ST
25)Zusanli(ST
36)
Taito
ng(Liv3),N
eitin
g(ST
44)
30min
Body
EAapplicationwas
perfo
rmed
daily
for2
0days,and
EAwas
appliedto
each
earo
nalternating
days
Darband
ietal.2013,Iran
AR
Inrerventio
ngrou
p:Tianshu(ST
25),Weidao(GB28)
Zhon
gwan(RN12),Shuifen(RN
9)Guanyuan(RN
4),Sanyinjiao(SP
6)Ex
cessgrou
p:Quchi(LI11),Fenglon
g(ST
40)
Deficiency
grou
p:Qihai(RN6),Y
inlin
gquan(SP
9)
20min
Twotre
atmennt
perw
eekfora
total
of6we
eks(12
treatments)
Fogartye
tal.2015,
Austr
alia
AR
Hegu(LI
4),Q
uchi(LI11)
Zusanli(S
T36),Neitin
g(ST
44)
Taicho
ng(LR3)
Auric
ular
acup
uncture:
Shenmen(TF4
)
NR
NR
LM:lifesty
lemod
ificatio
n;AAS:auric
ular
acup
oint
stimulation;
EA:electroacup
uncture;AC
E:acup
oint
catgut
embedd
ing;WA:w
armingacup
uncture;AR:
acup
unctureandrelatedtherapies;#com
binatio
nof
acup
unctureandrelatedtherapies.

Evidence-Based Complementary and Alternative Medicine 13
Table3:Risk
ofbias
assessment.
Stud
yRa
ndom
sequ
ence
generatio
nAllo
catio
nconcealm
ent
Blinding
ofparticipants
andinvestigators
Blinding
ofou
tcom
eassessment
Incompleteo
utcome
dataaddressed
Selectiveo
utcome
repo
rting
Allisonetal.1995,USA
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Hsu
etal.200
5,Taiwan
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Richards
etal.1998,Au
stralia
Unclear
risk
Lowris
kHighris
kLo
wris
kLo
wris
kUnclear
risk
Hee
tal.2008,C
hina
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Lietal.200
6,Ch
ina
Lowris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Tong
etal.2011,Ch
ina
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Hsu
etal.200
9,Taiwan
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Hsie
hetal.2010,Taiwan
Unclear
risk
Unclear
risk
Highris
kLo
wris
kHighris
kUnclear
risk
Hsie
hetal.2011,Taiwan
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Abdi
etal2012,Iran
Unclear
risk
Unclear
risk
Highris
kLo
wris
kHighris
kUnclear
risk
Darband
ietal2012,Iran
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Hee
tal2012,Ch
ina
Unclear
risk
Unclear
risk
Highris
kLo
wris
kUnclear
risk
Unclear
risk
Lien
etal2012,Taiwan
Lowris
kLo
wris
kHighris
kLo
wris
kHighris
kUnclear
risk
Darband
ietal2014,Iran
Lowris
kLo
wris
kHighris
kLo
wris
kLo
wris
kUnclear
risk
Yehetal.2015,Taiwan
Lowris
kLo
wris
kHighris
kLo
wris
kHighris
kUnclear
risk
Chen
etal.200
7,Ch
ina
Lowris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Huang
etal.2011,Ch
ina
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Tang
etal.200
9,Ch
ina
Highris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Shietal,2006
,China
Lowris
kUnclear
risk
Highris
kLo
wris
kUnclear
risk
Unclear
risk
Hsu
etal.200
5,Taiwan
Lowris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Guceletal.2012,Tu
rkey
Lowris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Dengetal.2014,Ch
ina
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Hassanetal.2014,Eg
ypt
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Hee
tal.2014,C
hina
Lowris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Wangetal.2013,Ch
ina
Highris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Sujung
etal.2014,SouthKo
rea
Lowris
kLo
wris
kHighris
kLo
wris
kLo
wris
kUnclear
risk
Buetal.200
7,Ch
ina
Lowris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Shietal.2005,C
hina
Lowris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Yang
etal.2010,Ch
ina
Highris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Cabiogluetal.200
5,Tu
rkey
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Cabiogluetal.200
6,Tu
rkey
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Cabiogluetal.200
8,Tu
rkey
Unclear
risk
Unclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Darband
ietal.2013,Iran
Lowris
kUnclear
risk
Highris
kLo
wris
kLo
wris
kUnclear
risk
Fogartye
tal.2015,A
ustralia
Unclear
risk
Lowris
kHighris
kLo
wris
kLo
wris
kUnclear
risk

14 Evidence-Based Complementary and Alternative Medicine
Table 4: Pairwise meta-analyses.
Comparison Pairwise OR (95% CI) Number of patients Number of studies Heterogeneity testI2 (%) p value
Body weightAR vs. LM 1.66(0.63 to 2.70) 496 10 55 0.02AR vs. placebo 1.15(0.67 to 1.63) 833 14 65 0.0004Combines therapies vs. PHA 2.44(-1.98 to 6.86) 80 1 - -Acupuncture vs. related therapies 0.25(0.00 to 0.49) 413 6 0 0.73Combines therapies vs. acupuncture 1.56(0.07 to 3.05) 378 6 99 <0.00001
BMIAR vs. LM 1.17(0.09 to 2.26) 314 6 74 0.002AR vs. placebo 0.57(0.40 to 0.74) 830 12 63 0.002Combines therapies vs. PHA 0.48(-0.90 to 1.86) 80 1 - -Acupuncture vs. related therapies 0.13(-0.06 to 0.32) 325 5 0 0.8Combines therapies vs. acupuncture 0.77(-0.37 to 1.92) 158 4 88 <0.00001
BMI: body mass index; LM: lifestyle modification; PHA: pharmacotherapy; AR: acupuncture and related therapies.
0.25to1.11), acupuncture (SMD: 1.28; 95% CrI, 0.43to2.06),combination of acupuncture and related theories (SMD: 1.44;95% CrI, 0.64to2.38), and electroacupuncture (SMD: 0.60;95% CrI, 0.03to1.22). Also, the combination of acupunctureand related theories and acupuncture alone were bothsuperior to the acupuncture combined lifestyle modificationin their ability to reduce body mass index (SMD = -1.76, 95%CrI =−2.96 to −0.62; SMD = −1.59, 95% CrI = −2.71to −0.34)(Table 5).
3.5. Ranking
3.5.1. Body Weight. Ranking of the different treatment meth-ods was displayed Figure 3. The results suggested that, onthe aspect of weight loss, combination of acupuncture andrelated therapies was ranked the optimal method, the best,(88.7%), followed by moxibustion with warming needle(87.8%), manual acupuncture (70.5%), acupoint catgut em-bedding (ACE,62.1%), auricular acupoint stimulation (AAS,48.3%), electro acupuncture (EA,46.3%), pharmacotherapy(41.9%), acupuncture combined lifestyle modification (AR+LM,31.2%), placebo acupuncture/sham acupuncture (16.8%),and lifestylemodification (LM,6.4%)whichwas ranked as theworst.
3.5.2. BMI. The results suggested that, on the aspect of BMI,combination of acupuncture and related therapies was rankedthe optimal method, the best, (90.2%), followed by manualacupuncture (83.3%), pharmacotherapy (64.7%), acupointcatgut embedding (58.6%), auricular acupoint stimulation(55.7%), electroacupuncture (52.1%), placebo acupuncture/sham acupuncture (25.1%), acupuncture combined lifestylemodification (16.9%), and lifestylemodification (3.4%)whichwas ranked as the worst.
3.6. Inconsistency Assessment
3.6.1. Body Weight. The Z test illustrates the inconsistencyof the NMA specifically (Appendix 4). For the inconsistencytest outcome of BW, 95% CI of 8 loops was included 0,
which reflected that no significant inconsistency was found.However, another 2 loops (ACE-Acupuncture-Combinedtherapies; ACE-Combined theories-EA) were found statisti-cal inconsistency between direct and indirect comparisons.
3.6.2. BMI. For the inconsistency test outcome of body massindex, 95% CI of all loops (acupuncture -combined theories-EA; acupuncture-EA-placebo; AR+LM -EA- LM-placebo;ACE-acupuncture-EA; AAS-EA-LM; AAS-AR+LM-LM-placebo; AAS-EA-placebo) were included 0, which reflectedthat no significant inconsistency was found.
3.7. Safety. Ten RCTs [26–28, 31, 32, 35, 36, 38, 39, 45] report-ed adverse events, while nomajor complicationswere noticedin all included studies. Three included studies [35, 36, 39]reported that no adverse effects were noted in both exper-imental group and placebo group. In one included RCT,there were two patients reporting mild ecchymosis and oneabdominal discomfort case reported as adverse events afterelectroacupuncture treatment; no case was reported in thelifestyle modification group [27]. In another study, there wereseven subjects in group auricular acupoint stimulation andtwo subjects in group placebo had mild tenderness [32].
4. Discussion
The aim of this study was to identify the efficacy and safety ofacupoint stimulation therapy for obesity. In this NMA, theassociation of each acupuncture and related therapies withrelative weight loss was compared by the combination ofdirect and indirect evidence from 34 RCTs in 2283 obese pa-tients.
This study has three key findings. First, ranking graphsof the primary outcome suggested that the combination ofacupuncture and related therapies was the most effectivein losing weight and improving BMI. Second, comparedwith placebo or sham acupuncture, combination of acu-puncture-related therapies, manual acupuncture, acupoint

Evidence-Based Complementary and Alternative Medicine 15
Table5:Re
sults
ofnetworkmeta-analyses.
Body
weight
AAS
-1.11
(-4.01,1.71)
ACE
0.72
(-0.93,2.37
)1.8
2(-1.0
8,4.84)
AR+
LM-1.45(
-4.11,1.28)
-0.36(-1.8
2,1.3
1)-2.16
(-4.94,0.61)
Acup
unct
ure
-2.40(-5.16,0.35)
-1.28(-2.96,0.39
)-3
.09
(-5.
97,-
0.33
)-0.92(-2.34,0.30)
Com
bine
dth
eori
es-0.07(
-1.85,1.74)
1.05(-1.3
5,3.48)
-0.77(-2.61,1.03)
1.38(-0.77,3.57)
2.33
(0.17
,4.5
6)EA
1.80
(0.2
1,3.
41)
2.90
(0.16
,5.7
2)1.0
9(-0.27,2.39
)3.
26(0
.65,
5.88
)4.
18(1
.62,
6.83
)1.8
5(0
.37,
3.37
)LM
0.06
(-5.43,5.46)
1.11(-3.79,6.23)
-0.67(-6.27,4.70)
1.47(-3.37,6.35)
2.39
(-2.25,7.16
)0.11(-5.02,5.13
)-1.76
(-7.18,3.51)
Phar
mac
othera
py1.2
6(0
.46,
2.06
)2.37
(-0.43,5.18
)0.54
(-0.93,2.03)
2.72
(0.0
6,5.
29)
3.65
(0.9
6,6.
34)
1.33(
-0.36,2.96)
-0.55(
-2.02,0.90)
1.20(-4.13,6.63)
Plac
ebo
-3.47(
-8.46,1.3
5)-2.31
(-7.6
9,2.72)
-4.18
(-9.2
2,0.67)
-1.99(-7.32,2.93)
-1.04(-6.34,3.96)
-3.40(-8.10,1.06)
-5.2
4(-
10.15
,-0.
55)
-3.50(-10.48,3.39)
-4.72(-9.7
7,0.07)
WA
BMI
AAS
-0.08(-1.5
4,1.4
2)AC
E0.96
(-0.08,2.00)
1.03(-0.58,2.66)
AR+
LM-0.64(-1.4
8,0.35)-0.54(-1.8
8,0.84)
-1.5
9(-
2.71
,-0.
34)
Acup
unct
ure
-0.81(-1.77,0.12)
-0.71(-2.20,0.70)
-1.7
6(-
2.95
,-0.
62)
-0.16
(-1.0
1,0.43)
Com
bine
dth
eori
es0.04
(-0.68,0.78)
0.12
(-1.2
0,1.4
5)-0.92(-1.8
8,0.08)
0.67
(-0.11,
1.34)
0.84
(0.19
,1.5
8)EA
1.31(
0.36
,2.3
0)1.4
0(-0.18,2.96)
0.34
(-0.36,1.15
)1.9
4(0
.83,
3.00
)2.
12(1
.07,
3.23
)1.2
8(0
.43,
2.11
)LM
-0.31
(-2.14,1.55)
-0.21(-2.34,1.8
7)-1.26(-3.21,0.79)
0.33
(-1.4
6,2.01)
0.51
(-1.0
6,2.09)
-0.35(
-2.10
,1.39
)-1.62(-3.54,0.31
)Ph
arm
acot
hera
py0.
63(0
.25,
1.11)
0.72
(-0.71,2.15
)-0.32
(-1.2
8,0.69)
1.28
(0.4
3,2.
05)
1.44
(0.6
4,2.
38)
0.60
(0.0
3,1.2
2)-0.66(-1.5
8,0.26)
0.95
(-0.85,2.78)
Plac
ebo
BMI:bo
dymassind
ex;LM:lifesty
lemod
ificatio
n;AAS:auric
ularacup
ointstimulation;EA
:electroacup
uncture;AC
E:acup
ointcatgutem
bedd
ing;WA:w
arminga
cupu
ncture;A
R:acup
uncturea
ndrelatedtherapies;
combinedtherapies:combinatio
nof
acup
unctureandrelatedtherapies.

16 Evidence-Based Complementary and Alternative Medicine
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 9 10
1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 9 10
1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 9 10
AAS(48.3) ACE(62.1) AR+LM(31.2) Acupuncture(70.5)
Combined theories(88.7) EA(46.3) LM(6.4) PHA(41.9)
PLA(16.8) WA(87.8)
Cum
ulat
ive P
roba
bilit
ies
RankGraphs by Treatment
(a) Body weight
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
0.2
.4.6
.81
1 2 3 4 5 6 7 8 9 1 2 3 4 5 6 7 8 9 1 2 3 4 5 6 7 8 9
1 2 3 4 5 6 7 8 9 1 2 3 4 5 6 7 8 9 1 2 3 4 5 6 7 8 9
1 2 3 4 5 6 7 8 9 1 2 3 4 5 6 7 8 9 1 2 3 4 5 6 7 8 9
AAS(55.7) ACE(58.6) AR+LM(16.9)
Acupuncture(83.3) Combined theories(90.2) EA(52.1)
LM(3.4) PHA(64.7) PLA(25.1)
Cum
ulat
ive P
roba
bilit
ies
RankGraphs by Treatment
(b) Body mass index
Figure 3: Surface under the cumulative ranking curves. LM: lifestyle modification; AAS: auricular acupoint stimulation; EA: electroacupunc-ture; ACE: acupoint catgut embedding; WA:warming acupuncture;AR: acupuncture and related therapies; combined therapies: combinationof acupuncture and related therapies; PLA: placebo; PHA: pharmacotherapy.

Evidence-Based Complementary and Alternative Medicine 17
catgut embedding, auricular acupuncture therapy, and elec-troacupuncture are all associated with higher odds of achiev-ing weight loss. Third, combination of acupuncture and re-lated therapies, manual acupuncture, pharmacotherapy, acu-point catgut embedding, auricular acupoint stimulation, andelectroacupuncture were superior to lifestyle intervention.
Lifestyle modification, like diet intervention and physicalactivity, is recommended as safe and effective way to loseweight [60]. Results of direct and indirect evidence suggestacupuncture and related theories had significant benefi-cial effects in dealing with obesity compared with lifestylemodification. Both experimental and clinical data prove theefficacy of acupuncture for obesity [61]. Experimental datasuggests that acupuncture exerts beneficial effects on weightloss [62, 63]. The majority of clinical evidence suggests thatacupuncture and related therapies reduced more weight thansham control group [26, 28, 31, 32], which are consistent withour results. Previous animal studies have observed that theexpression of obesity-related peptides was upregulated in thehypothalamus after acupuncture treatment, which inducedless food intake and weight loss [62, 64, 65]. Similarly, sig-nificant decreases in plasma leptin level were observed afterEA treatment in obese patients [46]. With regard to insulinlevel, several experimental studies reported that EA canimprove insulin sensitivity [66, 67]. However, results fromclinical trials regarding insulin levels are controversial.Cabioglu MT reported that EA increased insulin level com-pared with control group [56], but Gucel F indicated thatacupuncture decreased insulin level [46]. As to effects onlipid metabolism, acupuncture was reported to be effectivein decreasing total cholesterol (TC), triglycerides (TG) andLDL-C concentrations [68, 69] of obese rat. Significantdecreases in TC [55], TG [35], and LDL-C [55] were observedwhereas no changes in HDL-C [55] levels were observed inclinical trials. Furthermore, experimental studies suggest thatthere was significant decrease in serum TNF𝛼 after EA [70].Except for the noted mechanisms, EA can also induce whiteadipose tissue (WAT) browning via increasing uncouplingprotein-1 (UCP1) gene expression [71].
This NMA has several attractive advantages. We focusedon simple obesity patients without complication, which de-creased the heterogeneity and improve the quality of thisstudy. In addition, we compared acupuncture and acupunc-ture-related therapieswith the first-line treatment for obesity-lifestyle modification with a Bayesian framework. The ranktest of effectiveness provides data to favour acupunctureand acupuncture-related therapies. Lastly, we conducted acomprehensive search and included all eligible studies. Wecompared five different acupuncture treatments (manual acu-puncture; electro acupuncture; auricular acupoint stimula-tion; acupoint catgut embedding; moxibustion with warmingneedle) in the clinical effectiveness in treating patients withobesity.
However, this study has several limitations. First, wefailed to evaluate the safety of each acupoint stimulationtherapy due to the limited data in primary studies. Futuretrials should report adverse events clearly to improve thequality of study design. Second, unaddressed concerns stillexist regarding the long-term effects of using acupuncture
and acupuncture-related therapies on weight management ina clinical setting. The duration of acupuncture sessions andfollow-up duration of most included trials ranging fromfour weeks to twelve weeks. Further clinical evaluation ofacupuncture for obesity with longer follow-up appears war-ranted. Third, blinding of patients and researches was notapplied among included studies and the included trials weremainly conducted in China, which may lead to publicationbias [72]. Fourth, included study in our NMA lack of researchcompares the effectiveness between acupuncture, pharma-cotherapy, and different types of combination of acupuncture.Further confirmatory comparative effectiveness trials shouldcompare different types of combination of acupuncture. Ex-cept one study compared acupuncture and pharmacotherapy[29], additional research is needed to further explore. Finally,we use R-value to estimate the changes in standard deviations(SD), which might enlarge the SD compared with the origi-nals values.
Overall, our results indicate that combination of acu-puncture and related therapies ranks as the optimal methodfor reducing both weight and BMI. Further studies will clarifywhich combination of acupuncture and related therapies isbetter.
Data Availability
All data used to support the findings of this study are includedwithin the supplementary information files.
Conflicts of Interest
All authors declare that they have no potential conflicts ofinterest.
Authors’ Contributions
Yanji Zhang, Jia Li, and Guoyan Mo contributed equally tothis work. Wei Huang, Zhongyu Zhou, and Yanji Zhang con-tributed to study design. Xianglin Chen, Hui Liu, and TengCai contributed to study selection. Xiangmin Tian, Teng Cai,Xian Zhang, and Xianglin Chen contributed to data collec-tion and quality assessment. Figures 1–3 were prepared byJia Li and Jing Liu. Tables 1–5 were prepared by Guoyan Mo.Appendices 1–4 were prepared by Jia Li. Huisheng Yang andTeng Cai were responsible for technical and language sup-port. All authors have read and approved the final manu-script.
Acknowledgments
This research was supported by the National Nature ScienceFoundation of China (nos. 81674081 and 81804165), 2015Special Project in the TCM State Industry Administrationof Traditional Chinese Medicine of the People’s Republic ofChina (no. 201507003), Young Elite Scientist Sponsors HipProgram by CAST (no. 2017QNRC001), Hubei University ofTraditional ChineseMedicineAcupuncture andMoxibustion

18 Evidence-Based Complementary and Alternative Medicine
Research Team Project (no. 2017ZXZ004), and Science andTechnology Program of Hubei, China (no. 2016CFB221).
Supplementary Materials
Appendix 1: the PRISMA-NMA checklist treatment groupsfor included studies in a network meta-analysis. Appendix2: search strategies for RCTs on acupuncture for obesity.Appendix 3: summaries of mean, standard difference, andsample size between treatment groups for included studiesin a network meta-analysis. Appendix 4: inconsistency test.(Supplementary Materials)
References
[1] World Health Organization, “Fact Sheet Obesity and Over-weight 2013,” [WWW document], http://www.who.int/media-centre/factsheets/fs311/en/#, (accessed August 2014).
[2] W. T. Garvey, J. I. Mechanick, E. M. Brett et al., “American asso-ciation of clinical endocrinologists and American college ofendocrinology comprehensive clinical practice guidelines formedical care of patients with obesity,” Endocrine Practice, vol.22, pp. 1–203, 2016.
[3] C. L. Ogden, M. D. Carroll, B. K. Kit, and K. M. Flegal, “Pre-valence of childhood and adult obesity in the United States,2011-2012,”e Journal of the AmericanMedical Association, vol.311, no. 8, pp. 806–814, 2014.
[4] W. Xu, H. Zhang, S. Paillard-Borg, H. Zhu, X. Qi, and D.Rizzuto, “Prevalence of overweight and obesity among Chineseadults: Role of adiposity indicators and age,” Obesity Facts, vol.9, no. 1, pp. 17–28, 2016.
[5] J. Cawley and C. Meyerhoefer, “The medical care costs of obe-sity: an instrumental variables approach,” Journal of Health Eco-nomics, vol. 31, no. 1, pp. 219–230, 2012.
[6] R. Dalle Grave, S. Calugi, andM. El Ghoch, “Lifestyle modifica-tion in the management of obesity: Achievements and chal-lenges,” Eating andWeight Disorders, vol. 18, no. 4, pp. 339–349,2013.
[7] R. Khera, M. H. Murad, A. K. Chandar et al., “Association ofpharmacological treatments for obesity withweight loss and ad-verse events a systematic review and meta-analysis,” Journal ofthe American Medical Association, vol. 315, no. 22, pp. 2424–2434, 2016.
[8] P. R. Schauer, S. R. Kashyap, K. Wolski et al., “Bariatric sur-gery versus intensive medical therapy in obese patients withdiabetes,” e New England Journal of Medicine, vol. 366, no.17, pp. 1567–1576, 2012.
[9] S. Ikramuddin, J. Korner, W.-J. Lee et al., “Roux-en-Y gastricbypass vs intensive medical management for the control oftype 2 diabetes, hypertension, and hyperlipidemia: the diabetessurgery study randomized clinical trial,” e Journal of theAmerican Medical Association, vol. 309, no. 21, pp. 2240–2249,2013.
[10] L. O. Reis, W. J. Favaro, G. C. Barreiro et al., “Erectile dysfunc-tion and hormonal imbalance in morbidly obese male is re-versed after gastric bypass surgery: a prospective randomizedcontrolled trial,” International Journal of Andrology, vol. 33, no.5, pp. 736–744, 2010.
[11] V. L. Gloy, M. Briel, D. L. Bhatt et al., “Bariatric surgery versusnon-surgical treatment for obesity: a systematic review and
meta-analysis of randomised controlled trials,” British MedicalJournal, vol. 347, no. 5, 2013.
[12] S. Fang, M. Wang, Y. Zheng, S. Zhou, and G. Ji, “Acupunc-ture and lifestyle modification treatment for obesity: a meta-analysis,” American Journal of Chinese Medicine, vol. 45, no. 02,pp. 1–16, 2017.
[13] T.-L. Yeh, H.-H. Chen, T.-P. Pai et al., “The effect of auricularacupoint stimulation in overweight and obese adults: a system-atic review and meta-analysis of randomized controlled trials,”Evidence-Based Complementary and Alternative Medicine, vol.2017, Article ID 3080547, 16 pages, 2017.
[14] T. Guo, Y. Ren, J. Kou, J. Shi, S. Tianxiao, and F. Liang, “Acu-point catgut embedding for obesity: systematic review andmeta-analysis,” Evidence-Based Complementary and AlternativeMedicine, vol. 2015, Article ID 401914, 20 pages, 2015.
[15] A. Chaimani, J. P. T. Higgins, D.Mavridis, P. Spyridonos, andG.Salanti, “Graphical tools for network meta-analysis in STATA,”PLoS ONE, vol. 8, no. 10, 2013.
[16] G. Salanti, C. Del Giovane, A. Chaimani, D. M. Caldwell, J. P.Higgins, and Y. Tu, “Evaluating the quality of evidence from anetwork meta-analysis,” PLoS ONE, vol. 9, no. 7, 2014.
[17] B.Hutton,G. Salanti, D.M.Caldwell et al., “ThePRISMAexten-sion statement for reporting of systematic reviews incorporat-ing network meta-analyses of health care interventions: Check-list and explanations,” Annals of Internal Medicine, vol. 162, no.11, pp. 777–784, 2015.
[18] The Cochrane Collaboration, “Cochrane handbook for sys-tematic reviews of interventions,” 2011, http://www.cochrane.org/training/cochrane-handbook.
[19] K. R. Abrams, C. L. Gillies, and P. C. Lambert, “Meta-analysis ofheterogeneously reported trials assessing change frombaseline,”Statistics in Medicine, vol. 24, no. 24, pp. 3823–3844, 2005.
[20] J. P. T. Higgins, D. G. Altman, P. C. Gøtzsche et al., “The Co-chrane Collaboration’s tool for assessing risk of bias in rando-mised trials,” British Medical Journal, vol. 343, no. 24, 2011.
[21] J. P. T. Higgins, S. G. Thompson, J. J. Deeks, and D. G. Altman,“Measuring inconsistency in meta-analyses,” British MedicalJournal, vol. 327, no. 7414, pp. 557–560, 2003.
[22] A. E. Ades, M. Sculpher, A. Sutton et al., “Bayesian methods forevidence synthesis in cost-effectiveness analysis,” Pharma-coEconomics, vol. 24, no. 1, pp. 1–19, 2006.
[23] G. Lu and A. E. Ades, “Combination of direct and indirect evi-dence in mixed treatment comparisons,” Statistics in Medicine,vol. 23, no. 20, pp. 3105–3124, 2004.
[24] G. van Valkenhoef, G. Lu, B. de Brock, H. Hillege, A. E. Ades,andN. J.Welton, “Automatingnetworkmeta-analysis,”ResearchSynthesis Methods, vol. 3, no. 4, pp. 285–299, 2012.
[25] G. Salanti, A. E. Ades, and J. P. A. Ioannidis, “Graphicalmethodsand numerical summaries for presenting results frommultiple-treatment meta-analysis: an overview and tutorial,” Journal ofClinical Epidemiology, vol. 64, no. 2, pp. 163–171, 2011.
[26] D. B. Allison, K. Kreibich, and S. Heshka, “A randomised place-bo-controlled clinical trial of an acupressure device for weightloss,” International Journal of Obesity and Related MetabolicDisorders, vol. 19, no. 9, pp. 653–658, 1995.
[27] C.-H. Hsu, K.-C. Hwang, C.-L. Chao, J.-G. Lin, S.-T. Kao, andP. Chou, “Effects of electroacupuncture in reducing weight andwaist circumference in obese women: a randomized crossovertrial,” International Journal of Obesity, vol. 29, no. 11, pp. 1379–1384, 2005.

Evidence-Based Complementary and Alternative Medicine 19
[28] D. Richards and J. Marley, “Stimulation of auricular acupunc-ture points in weight loss,” Australian Family Physician, vol. 2,no. 27, pp. S73–S77, 1998.
[29] L. He, X.-L. Gao, H.-X. Deng, and Y.-X. Zhao, “Effects of acu-puncture on body mass index and waist-hip ratio in the patientof simple obesity,” Chinese Acupuncture &Moxibustion, vol. 28,no. 2, pp. 95–97, 2008 (Chinese).
[30] L. Li and Z.-Y. Wang, “Clinical therapeutic effects of body acu-puncture and ear acupuncture on juvenile simple obesity andeffects on metabolism of blood lipids,” Chinese Acupuncture &Moxibustion, vol. 26, no. 3, pp. 173–176, 2006.
[31] J. Tong, J. X. Chen, Z. Q. Zhang et al., “Clinical observation onsimple obesity treated by acupuncture,”Chinese Acupuncture &Moxibustion, vol. 31, no. 8, pp. 679–701, 2011.
[32] C.-H.Hsu, C.-J.Wang, K.-C. Hwang, T.-Y. Lee, P. Chou, andH.-H.Chang, “The effect of auricular acupuncture in obesewomen:a randomized controlled trial,” Journal of Women’s Health, vol.18, no. 6, pp. 813–818, 2009.
[33] C. H. Hsieh, “The effects of auricular acupressure on weightloss and serum lipid levels in overweight adolescents,”AmericanJournal of Chinese Medicine, vol. 38, no. 4, pp. 675–682, 2010.
[34] C. H. Hsieh, T.-J. Su, Y.-W. Fang, and P.-H. Chou, “Effects ofauricular acupressure on weight reduction and abdominal obe-sity in asian young adults: a randomized controlled trial,”American Journal of Chinese Medicine, vol. 39, no. 3, pp. 433–440, 2011.
[35] H. Abdi, P. Abbasi-Parizad, B. Zhao et al., “Effects of auricularacupuncture on anthropometric, lipid profile, inflammatory,and immunologic markers: a randomized controlled trialstudy,”e Journal of Alternative and Complementary Medicine,vol. 18, no. 7, pp. 668–677, 2012.
[36] M. Darbandi, S. Darbandi, M. G. Mobarhan et al., “Effects ofauricular acupressure combined with low-Calorie diet on theleptin hormone in obese and overweight iranian individuals,”Acupuncture in Medicine, vol. 30, no. 3, pp. 208–213, 2012.
[37] W. He, Z. Zhou, J. Li, L. Wang, B. Zhu, and G. Litscher, “Auricu-lar acupressure plus exercise for treating primary obesewomen:a randomized controlled clinical trial,” Medical Acupuncture,vol. 24, no. 4, pp. 227–232, 2012.
[38] C. Y. Lien, L. L. Liao, P. Chou, and C. H. Hsu, “Effects of auric-ular stimulation on obese women: a randomized, controlledclinical trial,” European Journal of Integrative Medicine, vol. 4,no. 1, pp. e45–e53, 2012.
[39] M. Darbandi, S. Darbandi, A. A. Owji et al., “Auricular or bodyacupuncture: Which one is more effective in reducing abdo-minal fat mass in Iranian men with obesity: A randomizedclinical trial,” Journal of Diabetes and Metabolic Disorders, vol.13, no. 1, 2014.
[40] M.-L. Yeh, N.-F. Chu,M.-Y. F. Hsu, C.-C.Hsu, andY.-C. Chung,“Acupoint stimulation on weight reduction for obesity: a ran-domized sham-controlled study,” Western Journal of NursingResearch, vol. 37, no. 12, pp. 1517–1530, 2015.
[41] F. Chen, S. Wu, and Y. Zhang, “Effect of acupoint catgut em-bedding on TNF-alpha and insulin resistance in simple obesitypatients,” Acupuncture Research, vol. 32, no. 1, pp. 49–52, 2007.
[42] L.-C. Huang and W.-Y. Pan, “Comparation of effect and cost-benefit analysis between acupoint catgut-embedding and elec-troacupuncture on simple obesity,” Chinese Acupuncture &Moxibustion, vol. 31, no. 10, pp. 883–886, 2011.
[43] C.-L. Tang, D.-C. Dai, G.-F. Zhao, W.-F. Zhu, and L.-F. Mei,“Clinical observation on electroacupuncture combined with
catgut implantation at acupoints for treatment of simple obesityof heart and spleen deficiency type,” Chinese Acupuncture &Moxibustion, vol. 29, no. 9, pp. 703–707, 2009.
[44] Y. Shi, L.-S. Zhang, C. Zhao, and C.-Q. He, “Comparison oftherapeutic effects of acupuncture-cuppingplus acupoint catgutembedding and electroacupuncture on simple obesity of stom-ach and intestine excess-heat type,” Chinese Acupuncture &Moxibustion, vol. 26, no. 8, pp. 547–550, 2006.
[45] C.-H. Hsu, K.-C. Hwang, C.-L. Chao, H.-H. Chang, and P.Chou, “Electroacupuncture in obese women: A randomized,controlled pilot study,” Journal of Women’s Health, vol. 14, no.5, pp. 434–440, 2005.
[46] F. Gucel, B. Bahar, C. Demirtas, S. Mit, and C. Cevik, “Influenceof acupuncture on leptin, ghrelin, insulin and cholecystokininin obese women: a randomised, sham-controlled preliminarytrial,” Acupuncture in Medicine, vol. 30, no. 3, pp. 203–207, 2012.
[47] L. Deng, Z. Lun, X. Ma, and J. Zhou, “Clinical observation onregulating the three energizer by acupoint catgut embeddingcombined with abdominal acupuncture in treating abdomi-nal obesity: a randomized controlled trial,” World Journal ofAcupuncture - Moxibustion, vol. 24, no. 4, pp. 29–34, 2014.
[48] N. E. Hassan, S. A. El-Masry, S. M. Elshebini et al., “Compar-ison of three protocols: Dietary therapy and physical activity,acupuncture, or laser acupuncture in management of obesefemales,” Macedonian Journal of Medical Sciences, vol. 7, no. 2,pp. 191–197, 2014.
[49] J. He, X. Zhang, Y. Qu et al., “Effect of combined manual acu-puncture andmassage on body weight and body mass index re-duction in obese and overweight women: a randomized, short-term clinical trial,” Journal of Acupuncture andMeridian Studies,vol. 8, no. 2, pp. 61–65, 2015.
[50] Y. L. Wang, X. Cao, Z. C. Liu, and B. Xu, “Observation on thetherapeutic effect of electroacupuncture on simple obesity ofgastrointestinal heat pattern/syndrome,”World Journal of Acu-puncture - Moxibustion, vol. 23, no. 2, pp. 1–5, 2013.
[51] S. Yeo, K. S. Kim, and S. Lim, “Randomised clinical trial of fiveear acupuncture points for the treatment of overweight people,”Acupuncture in Medicine, vol. 32, no. 2, pp. 132–138, 2014.
[52] T.W. Bu, X. L. Tian, S. J. Wang et al., “Comparison and analysisof therapeutic effects of different therapies on simple obesity,”Chinese Acupuncture &Moxibustion, vol. 27, no. 5, pp. 337–340,2007.
[53] Y. Shi, L.-S. Zhang, C. Zhao, and X.-Y. Zuo, “Controlled studyof needle warming therapy and electroacupuncture on simpleobesity of spleen deficiency type,” Chinese Acupuncture &Moxibustion, vol. 25, no. 7, pp. 465–467, 2005.
[54] J.-J. Yang, H.-J. Xing, H.-L. Xiao, Q. Li, M. Li, and S.-J. Wang,“Effects of acupuncture combined with diet adjustment andaerobic exercise on weight and waist-hip ratio in simple obesitypatients,”Chinese Acupuncture &Moxibustion, vol. 30, no. 7, pp.555–558, 2010.
[55] M. T. Cabıoglu and N. Ergene, “Electroacupuncture therapy forweight loss reduces serum total cholesterol, triglycerides, andLDL cholesterol levels in obese women,” American Journal ofChinese Medicine, vol. 33, no. 4, pp. 525–533, 2005.
[56] M. T. Cabioglu andN. Ergene, “Changes in levels of serum insu-lin, C-peptide and glucose after electroacupuncture and diettherapy in obese women,” American Journal of Chinese Medi-cine, vol. 34, no. 3, pp. 367–376, 2006.
[57] M. T. Cabioglu, N. Gundogan, and N. Ergene, “The efficacyof electroacupuncture therapy for weight loss changes plasma

20 Evidence-Based Complementary and Alternative Medicine
lipoprotein A, Apolipoprotein A and Apolipoprotein B levels inobese women,” American Journal of Chinese Medicine, vol. 36,no. 6, pp. 1029–1039, 2008.
[58] S. Darbandi, M. Darbandi, and P. Mokarram, “Effects of bodyelectroacupuncture on plasma leptin concentrations in obeseand overweight people in Iran: a randomized controlled trial,”Alternative erapies in Health and Medicine, vol. 19, no. 2, pp.24–31, 2013.
[59] S. Fogarty, L. Stojanovska,D.Harris, C. Zaslawski,M. L.Mathai,and A. J. McAinch, “A randomised cross-over pilot study inves-tigating the use of acupuncture to promote weight loss andmental health in overweight and obese individuals participatingin a weight loss program,” Eating and Weight Disorders, vol. 20,no. 3, pp. 379–387, 2015.
[60] W. T. Garvey, J. I. Mechanick, E. M. Brett et al., “American asso-ciation of clinical endocrinologists and American college ofendocrinology comprehensive clinical practice guidelines formedical care of patients with obesity: Executive summary,”Endocrine Practice, vol. 22, no. 7, pp. 842–884, 2016.
[61] M. Belivani, C. Dimitroula, N. Katsiki, M. Apostolopoulou, M.Cummings, andA. I. Hatzitolios, “Acupuncture in the treatmentof obesity: a narrative review of the literature,” Acupuncture inMedicine, vol. 31, no. 1, pp. 88–97, 2013.
[62] D.-R. Tian, X.-D. Li, F. Wang et al., “Up-regulation of the ex-pression of cocaine and amphetamine-regulated transcriptpeptide by electroacupuncture in the arcuate nucleus of diet-induced obese rats,” Neuroscience Letters, vol. 383, no. 1-2, pp.17–21, 2005.
[63] N. Tian, F. Wang, D.-R. Tian et al., “Electroacupuncture sup-presses expression of gastric ghrelin and hypothalamic NPY inchronic food restricted rats,” Peptides, vol. 27, no. 9, pp. 2313–2320, 2006.
[64] F. Wang, D. R. Tian, P. Tso, and J. S. Han, “Arcuate nucleus ofhypothalamus is involved in mediating the satiety effect of elec-troacupuncture in obese rats,” Peptides, vol. 32, no. 12, pp. 2394–2399, 2011.
[65] Z. Liu, F. Sun, J. Su et al., “Study on action of acupuncture onventromedial nucleus of hypothalamus in obese rats,” Journal ofTraditional Chinese Medicine, vol. 21, no. 3, pp. 220–224, 2001.
[66] J.-G. Lin, W.-C. Chen, C.-L. Hsieh et al., “Multiple sources ofendogenous opioid peptide involved in the hypoglycemic re-sponse to 15 Hz electroacupuncture at the Zhongwan acupointin rats,” Neuroscience Letters, vol. 366, no. 1, pp. 39–42, 2004.
[67] Y. Higashimura, R. Shimoju, H. Maruyama, and M. Kurosawa,“Electro-acupuncture improves responsiveness to insulin viaexcitation of somatic afferent fibers in diabetic rats,”AutonomicNeuroscience: Basic and Clinical, vol. 150, no. 1-2, pp. 100–103,2009.
[68] S. Wang, Q. Li, Y. She et al., “Effect of electroacupuncture onmetabolism of lipids in rats of obesity induced by sodiumglutamate,” Chinese Acupuncture & Moxibustion, vol. 25, no. 4,pp. 269–271, 2005.
[69] S. J. Wang, H. Z. Xu, and H. L. Xiao, “Effect of high-frequen-cy electroacupuncture on lipid metabolism in obesity rats,”Acupuncture Research, vol. 33, no. 3, pp. 154–158, 2008.
[70] H. Yang, Y. Li, L. Cheng, and J.-S. He, “Effect of electroacupunc-ture and diet adjusting on insulin resistance in rats withnutrition obesity,” Journal of Chinese Integrative Medicine, vol.5, no. 5, pp. 546–549, 2007.
[71] W. Shen, Y. Wang, S.-F. Lu et al., “Acupuncture promotes whiteadipose tissue browning by inducing UCP1 expression on DIO
mice,” BMC Complementary and Alternative Medicine, vol. 14,no. 1, pp. 54–59, 2014.
[72] M. J. Page, J. P. Higgins, G. Clayton et al., “Empirical evidenceof study design biases in randomized trials: systematic reviewof meta-epidemiological studies,” PLoS ONE, vol. 11, no. 7, pp.5–9, 2016.

Stem Cells International
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Disease Markers
Hindawiwww.hindawi.com Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwww.hindawi.com Volume 2013
Hindawiwww.hindawi.com Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwww.hindawi.com Volume 2018
PPAR Research
Hindawi Publishing Corporation http://www.hindawi.com Volume 2013Hindawiwww.hindawi.com
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwww.hindawi.com Volume 2018
Journal of
ObesityJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwww.hindawi.com Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwww.hindawi.com Volume 2018
Diabetes ResearchJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Research and TreatmentAIDS
Hindawiwww.hindawi.com Volume 2018
Gastroenterology Research and Practice
Hindawiwww.hindawi.com Volume 2018
Parkinson’s Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwww.hindawi.com
Submit your manuscripts atwww.hindawi.com