Embed Size (px)
Citation preview

Active Versus Passive Euthanasia: An Attributional Analysis’
DAVID B. SUGAR MAN^ University of New Hampshire
The present study investigates the way in which observers judged physicians who engaged in various acts of euthanasia. These acts varied over two dimensions: volun- tary versus nonvoluntary (on the patient’s part) and active versus passive (on the physician’s part). Vignettes about a patient who was severely burned in an apartment fire were read by 632 subjects (199 men and 433 women). The vignettes varied the physician’s actions and whether the patient requested to die or not. After reading one vignette, participants responded to a 19-item questionnaire to assess the moral evalua- tion, responsibility, and professional conduct ofthe physician. The results indicated no significant differences in the perception of the physician involved in voluntary or nonvoluntary euthanasia. The physician was perceived more negatively, held more responsible, and perceived as acting outside the standards of the medical profession in situations of active euthanasia in contrast to passive euthanasia. The data also sug- gested that the temporal relationship ofthe physician’s behavior to the patient’s death affected the perception of the physician’s responsibility and professional conduct.
With recent advances in medical technoogy, the issue of euthanasia has increasingly become a concern of medical practitioners, philosophers, and the public in general. Wilson( 1975) reported findings from the Harris and Gallup surveys suggesting that in 1973, the public viewed euthanasia more favorably than in the late 1940s and the early 1950s. However, these surveys and subsequent research (Devins, 1980-1981; Hart, 1978-1979; Klopfer & Price, 1978-1979; Nagi & Lazerine, 1982; Singh, 1979; Steininger & Colsher, 1978-1979) have primarily focused on attitudes toward euthanasia in general or towards one or two specific forms of the act (e.g., active vs. passive euthanasia). The present study attempts to more clearly delineate the attitudes which surround the various forms of euthanasia.
A number of writers (Foot, 1977; Maguire, 1973; Rachels, 1975,1980) have suggested that an act of euthanasia may be categorized along two dimensions. The first dimension, the patient’s wishes, may take one of three forms. An act of euthanasia can be voluntary in that patients have clearly expressed their
‘The author wishes to thank Ellen S. Cohn, Rodney G. Triplet, Marc D. Hiller, and Rebecca
*Requests for reprints should be sent to David B. Sugarman, Department of Psychology, M . Warner for comments on earlier drafts of this paper.
Rhode Island College, Providence, RI 02908.
60
Journal of Applied Social Psychology, 1986, 16, 1, pp. 60-76. Copyright @ 1986 by V. H. Winston &Sons, Inc. All rights reserved.

EUTHANASIA 61
wishes to die through verbal statements or documents such as “living wills.” On the other hand, an act of euthanasia may be nonvoluntary(Rachels, 1980) when patients are not able to express their wishes (i.e., coma) and did not make any type of prior disclosure of their wishes known (e.g., living wills). Finally, euthanasia may be defined as involuntary when the patients’ deaths are produced against their wishes. The present discussion focuses only on the former two forms of this dimension because involuntary euthanasia simply may be perceived as murder (Rachels, 1980).
The second dimension along which acts of euthanasia may be classified involves whether the act was one of commission or omission. The former situation, usually referred to as active euthanasia, involves some direct action (e.g., lethal injection, shooting) by an actor to bring about the death of another individual who is in extreme pain and/ or in an extremely critical state of health or terminal condition. The actor is attempting intentionally to bring about the patient’s death through a known interference with the patient’s biological functioning or life support system. In contrast, a death that is due to an act of omission often is labelled as passive euthanasia. This situation arises when an actor may facilitate the death of a person by refraining from any action or treatment which might otherwise prolong the patient’s life. The patient’s biological functioning ceases but not as a result of direct interven- tion. One clear example of passive euthanasia is the issuance of “Do not resuscitate” (DNR) orders by physicians to indicate that a patient is to be allowed to die (not resuscitated) if he or she should suffer cardio-pulmonary arrest.
An attributional analysis may be used to examine the way a lay-person may perceive these situations. According to Kelley (1972), the lay-person attempts to infer causal relationships between events in an attempt to bring predict- ability and control to his or her world. To act as a heuristic in this task, Kelley proposed the notion of causal schema which represent a lay-person’s under- standing of the manner in which two or more causes (the patient’s deteriorat- ing health and the physician’s action or inaction) may interact to produce a specific effect, that is, the patient’s death. In the evaluation of an actor’s contribution to a specific outcome, an observer must assess the degree to which causes external t o the actor may have contributed to the observed event. If the perceived contribution of external factors is considerable, the actor’s perceived contribution is lessened. This discounting principle has clear application to the analysis of different forms of euthanasia.
An analysis of the voluntary-nonvoluntary distinction suggests that observers would attribute less responsibility t o a physician (actor) for a patient’s death if the patient requests that such actions be taken. In situations of nonvoluntary euthanasia, actors are required to act based upon their own value systems without any input from those of patients. Even though in a

62 DAVID B. SUGARMAN
comatose state, some patients may not want to be allowed to die. When the wishes of the patients have been made explicit, the actor’s behavior may be perceived as being in agreement with the patient’s self-determination. Es- sentially, the physician becomes an agent of the patient. The requests of the patient to die act as an external justification for the actor’s behavior and consequently mitigate the actor’s responsibility for the act.
A similar type of analysis can be done with the distinction between active and passive euthanasia. With active euthanasia, the patient’s death can be viewed as the result of a single cause, the physician’s actions. Essentially, the medical condition of the patient is causally irrelevant t o the death of the patient. For example, Wilson (1975, pp. 38-40) reported a number of cases of physicians or family members who killed handicapped or seriously ill patients even though the patients were not terminally ill.
Passive euthanasia does not involve one single cause; rather it involves both the physician’s action and the concomitant deterioration of the patient’s physical condition. Because ofthe presence of multiple causes for the patient’s death, this suggests that lay-people will utilize what Kelley (1972) referred to as a multiple necessary causal schema. This posits that both causes are required to be present in order for the effect to occur. Consequently, the patient’s death results from the joint presence of the cardio-pulmonary arrest and the absence of treatment. Neither cause necessarily produces death inde- pendent of the other in all cases. This suggests that the actor’s behavior is not the only potential cause of the patient’s death. The presence of a second cause permits an observer to discount the actor’s contribution to the outcome or effect; the patient’s death may be perceived as primarily resulting from a deterioration of the patient’s medical status. This discounting is impossible in the circumstances involving active euthanasia because the actor’s behavior will result in the patient’s death regardless of the patient’s medical situation. This suggests that the actor involved in an act of passive euthanasia will be perceived as less responsible for the patient’s death than if it were an instance of active euthanasia. Therefore, observers should make a strong distinction between an act of commission and an act of omission (see Fincham & Jaspars, 1980).
Rachels (1975) has suggested an alternate interpretation of the passive- active euthanasia distinction. He posited that the act of killing and the act of letting die were morally equivalent because equivalent motives (reduction of patient’s suffering) and outcomes (the patient’s death) characterized each of these acts. Consequently, one would expect that an act which limits the period of a person’s suffering would be more highly valued in contrast to one which requires a person to linger. This limitation of suffering hypothesis would predict that those cases which quickly foster the patient’s death (i.e., active
EUTHANASIA 63
euthanasia) would be perceived as more highly valued than a n act of passive euthanasia which might not release the patient rapidly from severe pain.
Two issues arise from this analysis. The first issued involves the situation in which there is a decay in the patient’s physical condition but an attempt to save the life of the patient was made (i.e., cardio-pulmonary resuscitation). In order to assess a physician’s act of euthanasia, it is necessary that a control scenario be used in which the same outcome results but actions were taken to inhibit this outcome. Previous studies (Devins, 1980-1981; Hart, 1978-1979; Klopfer& Price, 1978-1979; Nagi& Lazerine, 1982; Singh, 1979; Steininger& Colsher, 1978-1979) d o not offer this contrast. Because the physician’s attempl at CPR may be perceived as a means of preventing the patient’s death (inhibitory cause), it is hypothesized that the physician will be perceived as less responsible for the outcome than in any of the euthanasia conditions.
The !second issue involves the distinction between the various forms of passive euthanasia. One way of differentiating between these acts is the temporal ordering of the physician’s action in regard to the patient’s death. In the DNR order example cited previously, the physician’s action preceded the patient’s physical deterioration and cardio-pulmonary arrest. However, it is also possible that the patient’s condition may deteriorate prior t o the physi- cian’s decision to engage in an act of euthanasia. For example, patients may suffer respiratory failure and require the aid of machinery to mantain their lives. The doctor’s action of taking the patient off the respirator would then follow the patient’s medical deterioration. This argument suggests that the temporal priority of the physician’s actions might be related to the evaluation of the physician’s behavior and perceived responsibility and would predict that when the doctor’s actions are more temporally distal from the patient’s death, less reponsibility will be attributed to the doctor.
A second perspective on the distinction between types of passive euthanasia was offered by the President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research (1983). I t posited that the distinction is actually between withholding treatment (e.g., DNR order) and withdrawing treatment (e.g., turning off a respirator). The Commission argued that while a thin moral line separated these two acts of omission, the physician should be biased to act conservatively. They suggest that all avail- able medical procedures should be employed in an attempt to bring about an improvement in the patient’s medical condition. Consequently, it is preferable to implement a procedure, assess its impact on the patient’s medical status, and terminate its usage if no improvement occurs than not t o implement the procedure at all. This withdrawal-withholding hypothesis suggests that the employment of a DNR order would be perceived more negatively than the termination of the use of a respirator.
64 DAVID B. SUGARMAN
The present study attempts to examine the attributions which observers made regarding a physician involved in various forms of acts of euthanasia. The first manipulated factor was whether the patient requested to be allowed to die. This variable compared conditions in which the patient requested to be permitted to die(vo1untary euthanasia) versus conditions in which the patient only requested pain killers or never regained consciousness to offer any request (nonvoluntary euthanasia). The second independent factor examined the effect of the active-passive distinction on the observer’s attributions. This factor compared four manners of the patient’s death: lethal injection (active euthanasia), turning off respirator (passive euthanasia-proximal action), DNR order (passive euthanasia-distal action), and CPR failure (control).
Method
Subjects
A total of 632 subjects (1 99 men and 433 women) participated in the present study in order to fulfill a laboratory requirement for their General Psychology course. The mean age of the sample was 18.34 years (sd 1.88). A vast majority of the participants indicated that they were single (98.4%). The distribution of the participants’ religious affiliations was: Catholic, 54.8%; Protestant, 32.7%; Jewish, 2.5%; and other, 10.0%. Eight subjects were dropped from the study because of missing data. Consequently, analysis was performed on the data of 624 participants.
Design
The present study involved a 3 x 4 factorial design. The first factor of the design was the patient’s wishes regarding his death. In the unconscious condi- tion, the patient never fully became conscious and was unable to make his wishes known. In the pain-killer condition, the patient did become conscious and requested that the medical staff increase his medication for the pain that he was suffering. The patient then lapsed back into an unconscious state. In the death-request condition, the patient also regained consciousness but requested that he be allowed to die before becoming unconscious again. The second factor involved the manner by which the patient died. In the CPR- failure (control) condition, the patient suffered a cardio-pulmonary arrest and the staff attempted to save him but failed. In the DNR-order (passive-distal) condition, the physician wrote on the patient’s medical chart that no attempt would be made to resuscitate the patient if the patient was to suffer a cardio- pulmonary arrest. The patient subsequently suffered an arrest and was not resuscitated. The third or respirator-off (passive-proximal) condition had the
EUTHANASIA 65
patient’s lungs fail to function placing him in pulmonary arrest and required his being placed on a respirator. The doctor then terminated treatment by turning. off the respirator which resulted in the patient’s death. The final lethal-injection (active) condition involved the physician inducing an emboli by injecting air into the patient causing the patient’s death.
Dependent Measures
Attributional measures. Participants were asked to report their degree of agreement or disagreement with 19 statements about the doctor and the patient portrayed in the vignette. Each item was assessed on a 9-point Likert- type scale. Value “1” was anchored as “strongly disagree”; value “3,” “dis- agree”; value “5,” “neutral”; value “7,” “agree”; and value “9,” “strongly agree.” The specific items are presented in Table 1. In addition, two items desgned to be manipulation checks were included. These items were the degree to which the observers perceived that the patient wanted to die and that the doctor’s actions were an act of omission. The direction of these items was counterbalanced and the order of presentation was randomized.
Demographic information. Each participant was asked to indicate gender, age, year in college, political and religious affiliation, marital status, and type of residential community.
Procedure
Subjects were tested in large groups rangingfrom about 20 to 60 individals. The experimenter introduced himself and explained to the participants that they were going to be asked their opinions about the issue of euthanasia. Participants were informed that they were to respond to the items in the packet of questionnaires sequentially and without referring back to earlier answers. Participants were told that at one point in the questionnaire they would be asked to read a story and answer questions regarding this story. They were also requested to read the story carefully and not to return to it while answering the questions. Each participant initially answered the demo- graphic information questionnaire. All of the participants read one of the 12 vignettes adapted from a case study presented by Veatch (1977, pp. 342-343). These vignettes related a story about a man in his sixties who suffers burns over 701% of his body in an apartment fire. The patient was reported to have no family and no friends. Because of the severity of the burns, he was in excruciat- ing pain and his prognosis was very uncertain. In each of the vignettes, the patient does die. The attributional measures followed the vignette. After all of the participants in the group completed the questionnaire, they were debriefed.
66 DAVID B. SUGARMAN
Results
Manipulation Checks
In order to assess the impact of the experimental manipulations, two items were employed as manipulation checks. The item for checking the manner of death manipulation was the participant’s degree of agreement with the state- ment, “The action which the doctor took with regard to the patient was an act of omitting or failing to include treatment.” Participants’ responses were analyzed in a four-group analysis of variance design using the manner of death as the between-group factor. The results indicated a significant effect (F(3,626) = 31.54, p < .OOl). Participants perceived that the DNR Order condition ( M 5.35) and theTurned Off Respirator condition(M ~ 4 . 3 6 ) to be acts of omission while the CPR failed ( M = 3.1 1) and Lethal Injection ( M = 3.55) conditions were not.
The second manipulation check assessed the impact of the patient’s wishes variable. A three-group analysis of variance on the participants’ agreement with the statement “The patient wanted to die” revealed a significant effect (F(2,629) = 1 5 1 . 9 4 , ~ < ,001). The pattern of means for this effect indicated that participants showed higher agreement when the patient did request t o be allowed to d ie (M 8.09) than in either the Painkiller Request condition(M 5.38) or Unconscious condition ( M = 5.17). These findings suggested that both manipulations were effective.
Data Reduction
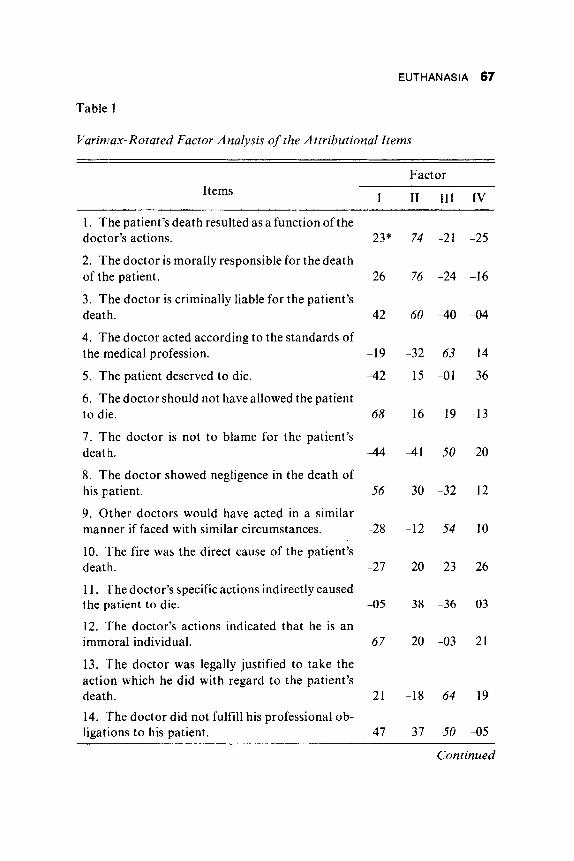
Prior to the analysis of between-group differences, the 19 responsibility items were factor analyzed using a Varimax rotation. This analysis resulted in four unrotated factors with eigenvalues greater than I .O, which accounted for 59.8% of the variance (see Table I) . Items which had a factor loading with an absolute magnitude of S O or greater were judged as loading highly on a specific factor. Rotation of the factors resulted in a decrease of the percent of accounted variance to 48.4%.
Six items loaded highly on the first factor. That factor included two types of items. The first type focused on the specific act taken by the physician. This included defining the action as an act of murder, and noting that the doctor exhibited negligent behavior and that he should not have allowed the patient to die. The second variable type involved the evaluation of the physician based upon this action. These included the physician’s immorality and lack of hu- manity and whether he should be punished for his actions. Overall, the factor may be interpreted as the moral evaluation of the physician and his actions. A reliability analysis of these moral evaluation items revealed an alpha coeffi- cient of .87. Higher scores denoted high negative moral evaluations.
EUTHANASIA 67
Table I
Variwax-Rotated Factor Analysis of the Attributional Items
Factor
I I1 I11 IV Items
1. The patient’s death resulted as a function of the doctor’s actions.
2. The doctor is morally responsible for the death of the patient.
3. The doctor is criminally liable for the patient’s deatlh.
4. The doctor acted according to the standards of the medical profession.
5 . The patient deserved to die.
6. The doctor should not have allowed the patient to die.
7. The doctor is not t o blame for the patient’s death.
8. The doctor showed negligence in the death of his patient.
9. Other doctors would have acted in a similar manner if faced with similar circumstances.
10. The fire was the direct cause of the patient’s death.
11. ‘The doctor’s specific actions indirectly caused the patient to die.
12. The doctor’s actions indicated that he is an immoral individual.
13. ‘The doctor was legally justified to take the action which he did with regard to the patient’s death. 14. ‘The doctor did not fulfill his professional ob- ligations to his patient.
23* 74 -21 -25
26 76 -24 -16
42 60 4 0 -04
-19 -32 63 I4
4 2 15 -01 36
68 16 -19 -13
4 4 4 1 50 20
56 30 -32 12
-28 -12 54 10
-27 20 23 26
-05 38 -36 03
67 20 -03 21
-21 -18 64 19
47 37 -50 -05
Continued
68 DAVID B. SUGARMAN
Table 1 . (continued)
Factor Items I I1 I11 IV
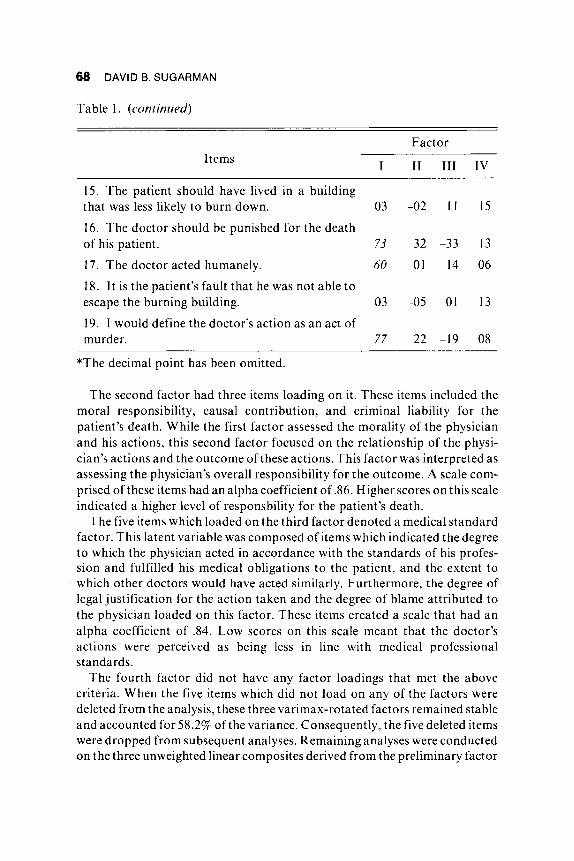
15. The patient should have lived in a building that was less likely to burn down. 03 -02 11 15
16. The doctor should be punished for the death of his patient. 73 32 -33 13
17. The doctor acted humanely. -60 -01 14 06
18. It is the patient’s fault that he was not able to escape the burning building. 03 -05 01 13
19. I would define the doctor’s action as an act of murder. 77 22 -19 08
*The decimal point has been omitted.
The second factor had three items loading on it. These items included the moral responsibility, causal contribution, and criminal liability for the patient’s death. While the first factor assessed the morality of the physician and his actions, this second factor focused on the relationship of the physi- cian’s actions and the outcome of these actions. This factor was interpreted as assessing the physician’s overall responsibility for the outcome. A scale com- prised of these items had an alpha coefficient of 26. Higher scores on this scale indicated a higher level of responsbility for the patient’s death.
The five items which loaded on the third factor denoted a medical standard factor. This latent variable was composed of items which indicated the degree to which the physician acted in accordance with the standards of his profes- sion and fulfilled his medical obligations to the patient, and the extent to which other doctors would have acted similarly. Furthermore, the degree of legal justification for the action taken and the degree of blame attributed to the physician loaded on this factor. These items created a scale that had an alpha coefficient of .84. Low scores on this scale meant that the doctor’s actions were perceived as being less in line with medical professional standards.
The fourth factor did not have any factor loadings that met the above criteria. When the five items which did not load on any of the factors were deleted from the analysis, these three varimax-rotated factors remained stable and accounted for 58.2% of the variance. Consequently, the five deleted items were dropped from subsequent analyses. Remaining analyses were conducted on the three unweighted linear composites derived from the preliminary factor
EUTHANASIA 69
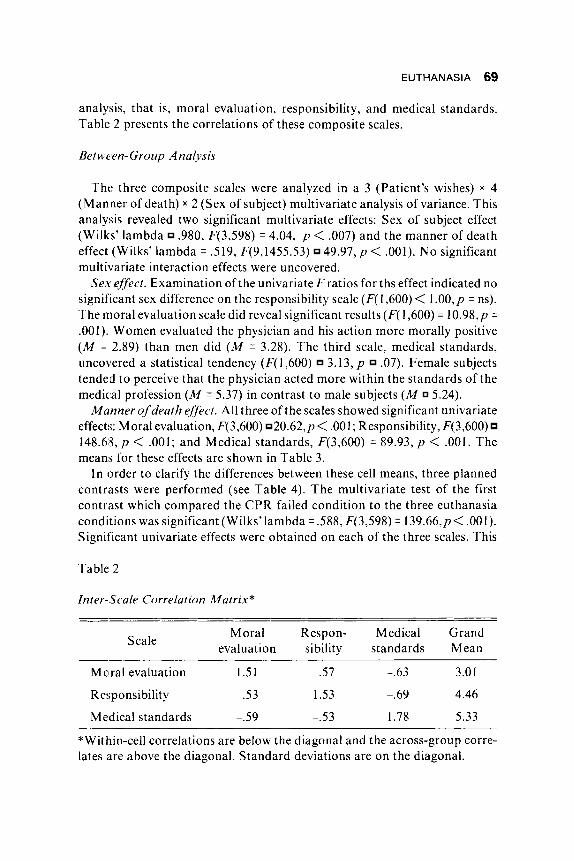
analysis, that is, moral evaluation, responsibility, and medical standards. Table 2 presents the correlations of these composite scales.
Between- Group Analysis
The three composite scales were analyzed in a 3 (Patient’s wishes) x 4 (Manner of death) x 2 (Sex of subject) multivariate analysis of variance. This analysis revealed two significant multivariate effects: Sex of subject effect (Wilks’ lambda .980, F(3,598) = 4.04, p < .007) and the manner of death effect (Wilks’ lambda = .519, F(9,1455.53) 4 9 . 9 7 , ~ < .001). No significant multivariate interaction effects were uncovered.
Sex ejfect. Examination of the univariate F ratios for ths effect indicated no significant sex difference on the responsibility scale (F( 1,600) < 1 .OO,p = ns). The moral evaluation scale did reveal significant results (F( 1,600) = 1 0 . 9 8 , ~ = .001). Women evaluated the physician and his action more morally positive ( M = 2.89) than men did ( M = 3.28). The third scale, medical standards, uncovered a statistical tendency (F(1,600) 3.13, p .07). Female subjects tended to perceive that the physician acted more within the standards of the medical profession ( M = 5.37) in contrast to male subjects ( M 5.24).
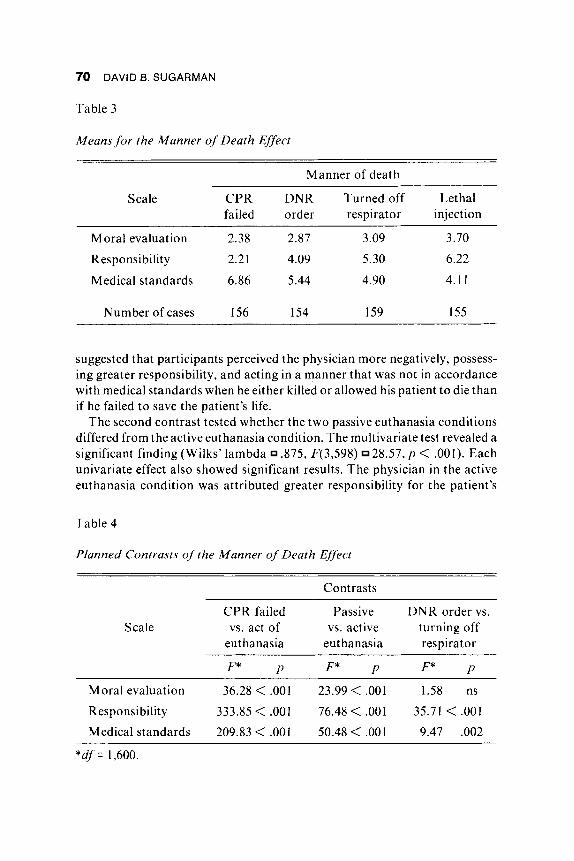
Manner of death effect. All three of the scales showed significant univariate effects: Moral evaluation, F(3,600) 20.62,p< ,001; Responsibility, F(3,600) 148.68, p < .001; and Medical standards, F(3,600) = 89.93, p < . O O l . The mean’s for these effects are shown in Table 3.
In order to clarify the differences between these cell means, three planned contrasts were performed (see Table 4). The multivariate test of the first contrast which compared the CPR failed condition to the three euthanasia conditions was significant (Wilks’lambda = ,588, F(3,598) = 139.66,p< ,001). Significant univariate effects were obtained on each of the three scales. This
Table 2
Inter-Scale Correlation Matrix*
Moral Respon- Medical Grand evaluation sibility standards Mean Scale
Mclral evaluation 1.51 .57 -.63 3.01
Responsibility .53 1.53 -.69 4.46
Medical standards p.59 -.53 1.78 5.33
*Within-cell correlations are below the diagonal and the across-group corre- lates are above the diagonal. Standard deviations are on the diagonal.
70 DAVID B. SUGARMAN
Table 3
Means for the Manner of Death Effect
Manner of death
Scale CPR DNR Turned off Let ha1 failed order respirator injection
~ ~~
Moral evaluation 2.38 2.87 3.09 3.70
Responsibility 2.21 4.09 5.30 6.22
Medical standards 6.86 5.44 4.90 4.1 1
Number of cases I56 154 159 155
suggested that participants perceived the physician more negatively, possess- ing greater responsibility, and acting in a manner that was not in accordance with medical standards when he either killed or allowed his patient to die than if he failed to save the patient’s life.
The second contrast tested whether the two passive euthanasia conditions differed from the active euthanasia condition. The multivariate test revealed a significant finding (Wilks’ lambda 2375, F(3,598) 28.57, p < .001). Each univariate effect also showed significant results. The physician in the active euthanasia condition was attributed greater responsibility for the patient’s
Table 4
Planned Contrasts of the Manner of Death Effect
Contrasts
CPR failed Passive DNR order vs. Scale vs. act of vs. active turning off
euthanasia euthanasia respirator
F* P F* P F* P
Moral evaluation 36.28 < ,001 23.99 < .001 1.58 ns
Responsibility 333.85 < ,001 76.48 < ,001 35.71 < .001
Medical standards 209.83 < .001 50.48 < ,001 9.47 .002
*df = 1,600.

EUTHANASIA 71
death and was evaluated more negatively than the physician in the passive euthanasia conditions. In addition, an act of active euthanasia was perceived as being less in line with perceived medical standards than passive euthanasia was.
The final contrast between the two passive euthanasia conditions was significant (Wilks’ lambda .935, F(3,598) 1 3 . 8 3 , ~ < .001). No effect was present for the moral evaluation scale; however, the other two scales showed significant results. Subjects attributed greater responsibility and lower per- ceived compliance with medical standards when the doctor’s actions were more proximal to the patient’s death (Respirator condition) than when the doctor’s actions were distal to the patient’s death (DNR order condition).
Supplemental analyses. Even though the main effect for patient’s wishes was nonsignificant (Wilks’ lambda .099, F(6,l 196) = 1 . 0 3 , ~ = .401), it was hypothesized that the voluntary euthanasia condition should differ from the two nonvoluntary conditions. This planned contrast was tested and revealed a very marginal multivariate effect (Wilks’ lambda = .990, F(3,598) 1 . 0 3 , ~ = . I 12). At the univariate level, neither the moral evaluation scale (F( 1,600) = 2.03, p ,155) nor the responsibility scale (F( 1,600) < 1 .O, p = ns) showed a significant effect. The medical standards scale did show a strong statistical tendency (F( 1,600) = 3 . 8 0 , ~ .052). When the patient requested to be allowed to die, the physician’s actions were perceived as being more in compliance with medi- cal standards ( M 5.50) than if the patient never made this type of request (Painkiller requested condition, M 5.26; Unconscious condition, M 5.23).
In order to rule out two alternative hypotheses, the three composite scales were examined for differences on the basis of religious affiliation and resi- dential community. A three-group (Catholic, Protestant, and other religions) MANOVA was performed on the three scales. Because of the small number of Jewish participants, their data was combined with the other affiliation data. The multivariate level test (Wilks’ lambda = .983, F(6,1236) = 1 . 7 8 , ~ = .loo) did not show a significant effect; however, a significant univariate effect was found for the moral evaluation scale (F(2,620) 3.92, p = .020). Catholic participants perceived the doctor more negatively on this scale(M ~ 3 . 1 7 ) than either the Protestant participants ( M 2.87) or the participants who affiliated with another religion ( M 2.71). A similar multivariate analysis of the community of residence factor (Urban, Rural, and Suburban) shows neither a multivariate effect (Wilks’ lambda .997, F(6,1240) < 1.00, p = ns) or any univariate effects.
Discussion
The present study examined the attributions which observers would infer about a physician who engaged in various forms of euthanasia. Several hy-
72 DAVID B. SUGARMAN
potheses were proposed and tested. It was predicted that although acts of euthanasia may not be viewed negatively in absolute terms, they will be perceived more negatively in contrast to acts of failing to succeed at saving a patient. The results clearly supported this hypothesis. Observers perceived that when the physician was associated with an act of euthanasia, he was attributed more responsibility for the patient’s death, a more severe moral evaluation, and greater discrepancy with the perceived standards of the medi- cal profession. The observers appeared to view the physician’s behavior more positively if it coincided with the traditional physician’s role of attempting to return the patient to his or her normal level of functioning (Parson, 1951, 1975).
A second hypothesis was that observers would have perceived acts of voluntary euthanasia more favorably than acts of nonvoluntary euthanasia. This hypothesis obtained almost no support. Physicians were perceived to be behaving more in agreement with perceived medical standards when they engaged in an act of voluntary euthanasia in contrast to involuntary eutha- nasia. This tentatively suggested that observers perceived that one of the professional standards which doctors employ is that of respect for persons or the right to self-determination of the patient. However, one has to be careful in interpreting this finding given the marginality of the effect.
Two related factors may be contributing to the marginality of this finding. The first involves the relationship between voluntary euthanasia and suicide. The very act of requesting to die may be perceived as irrational, which creates doubts about the patient’s capacity (i.e., the ability to make a particular health care decision). Second, observers may be discountng the patient’s wish to die as a temporary aberration. Once again, the patient’s capacity to make this decision is questioned because at the present time, he is undergoing extreme pain and may be confused due to the medical problem. However, the Presi- dent’s Commission for the Study of Ethical Problems in Medicine and Bio- medical and Behavioral Research (1982) has rejected these positions. The Commission argued that when the wishes of the patient are in opposition to prevailing medical practices, this does not prove patient incapacity.
The distinction between passive and active euthanasia offered two compet- ing hypotheses. The discounting hypothesis posited that the presence of contributing medical deterioration in the passive euthanasia condition would result in more positive evaluations of the physician in contrast to the active euthanasia situation. O n the other hand, the limitation of suffering hypothesis suggested the reverse effect. The findings supported the discounting hy- pothesis. Physicians were evaluated more negatively, given greater responsi- bility, and perceived as acting outside the boundaries of medical practices when they engaged in an act of active euthanasia. This supports Nagi and Lazerine’s (1 982) finding that although clerics generally disapproved of the
EUTHANASIA 73
direct inducement of death, they were more accepting of the indirect induce- ment of death.
The recent President’s Commission (1983) has offered conclusions coincid- ing with these data. Their report suggested that one essential reason for this passive-active distinction is that with an act of commission, the potential for patient survival is eliminated. In situations involving acts of omission, the patient’s death is not a foregone conclusion (cf. the case of Karen Ann Quinlan). This permits the actor to perceive the disease process as the cause of the death in the passive euthanasia situation. Interestingly, the report noted that this is a “very comforting formulation” for the physician (1983, p. 68).
Two competing hypotheses were offered in the examination of various forms of passive euthanasia. The data supported the temporal ordering hypothesis rather than the withholding-withdrawal hypothesis. The physician was perceived as less responsible for the patient’s death and as behaving more in line with medical standards when he wrote the DNR order than when he disconnected the respirator. This conclusion has to be made tentatively because the DNR order and respirator off conditions d o confound the distal- proximal and withdrawl-withholding distinctions. Even though these distinc- tions may offer divergent predictions, the confounding may have resulted in an overpowering of one of the effects. More controlled studies to separate these two perspectives are required.
In addition to the factors tested, a number of other variables may contribute to one’s perception of an act of euthanasia. First, the physician may have acted unilaterally, as in the present study, may have consulted an advisory board (e.g., institutional ethics committee) for aid in making a decision, may have sought probate court intervention, or may have acted as a representative of the patient. Mynatt and Sherman (1975) have noted that a diffusion of responsibility results when group decisions are placed into effect. Conse- quently, if the doctor’s behavior were the result of a group’s advice or decision, less responsibility would have been attributed to the specific actor.
Second, the patient’s medical symptoms and prognosis will affect one’s perception of a specific act of euthanasia. If the patient’s perceived life quality (i.e., the degree of pain, dependency, and physical and mental disability) and/ or perceived life quantity (i.e., life expectancy) are relatively poor, the acceptability of euthanasia should increase. For example, Crane (1975) noted that physicians are more likely to treat actively a terminal adult patient who suffers from mild physical disabilities than one who suffers from severe disabilities.
A third issue which places a number of limitations on the generalizability of the present findings is that these findings represent the attributions of observers who are biased to focus on the actor’s behavior (Jones & Nisbett, I97 1 ; Ross, 1977). An assessment of health care professionals’ perceptions

74 DAVID B. SUGARMAN
of these various forms of euthanasia may exhibit the employment of more sophisticated implicit theories. This results from their professional socializa- tion and their everyday confrontations with the personal, ethical, legal, and medical issues surrounding the act of euthanasia.
Granted the limitations of the present study, the applicability of these findings should be noted. First, although college students are a nonrepresen- tative sample of the total adult population, they d o represent the population from which future health care professionals will be selected. Consequently, understanding the way by which students view the issues surrounding eutha- nasia permits health care educators t o challenge these perceptions. This reinforces the recent emphasis on the instruction of medical ethics and similar areas to health care professionals, especially physicians (President’s Commis- sion, 1982). One may argue that the present study participants tended to focus on the concrete aspects of the situation (e.g., the physician’s behavior) and ignored the more abstract issues such as patient self-determination or quality of life versus quantity of life issues.
The second implication involves the broader question of public attitude toward euthanasia. Based on earlier research (Devins, 1980-1981; Hart, 1978-1979; Singh, 1979; Wilson, 1975), it would appear that at least some forms of euthanasia were being perceived as more acceptable than others. However, the present data leads one to infer that the issue of euthanasia has not reached a level that it is perceived as equally acceptable as attempting to save a person’s life, even though this action may prolong the patient’s suffering.
In conclusion, the present study shows that individuals d o make fine distinctions between various acts of euthanasia. First, observers more posi- tively evaluated a physician who attempted but failed to save a patient than a physician who engaged in an act of euthanasia. Second, an act of commission which results in a patient’s death was perceived more negatively than if the act involved an omission. Third, it appeared that the form of the physician’s omission which resulted in the patient’s death affected evaluations.
References
Crane, D. (1975). Decisions to treat critically ill patients: A comparison of social versus medical considerations. Milbank Memorial Fund Quarterly1 Health & Society, 53, 1-34.
Devins, G. M. (1980-1981). Contributions of health and demographic status to death anxiety and attitudes toward voluntary passive euthanasia. Omega, Journal of Death and Dying, 11(4), 293-302.
Fincham, F. D., & Jaspars, J. (1980). Attribution of responsibility: From
EUTHANASIA 75
man-the-scientist to man-the-lawyer. In L. Berkowitz (Ed.), Advances in exerimentalsocialpsychology (Vol. 13, pp. 81-138). NeivYork: Academic Press.
Foot, P. (1977). Euthanasia. Philosophy and Public Affairs, 6, 85-1 12. Hart, E. J . ( I 978-1979). The effect of death anxiety and mode of“case study”
presentation on shifts of attitude toward euthanasia. Omega, Journal of Death and Dying, 9(3), 239-244.
Jones, E. E., & Nisbett, R. E. (1971). The actor and observer: Divergent perceptions ofthecauses of behavior. In E. E. Jones, D. E. Kanouse, H. H. Kelley, R. E. Nisbett, S. Valins, & B. Weiner (Eds.), Attribution: Perceiv- ing the causes of behavior (pp. 79-95). Morristown, NH: General Learning Press.
Kelley, H. H. (1972). Causal schemata and the attribution process. In E. E. Jones, D. E. Kanouse, H. H. Kelley, R. E. Nisbett, S. Valins, & B . Weiner (Eds.), Attribution: Perceiving the causes of behavior (pp. 151-174). Mor- ristown, NJ: General Learning Press.
Klopfer, F. J . , & Price, W. F. (1978-1979). Euthanasia acceptance as related to afterlife beliefs and other attitudes. Omega, Journal of Death and Dying, 9(3), 245-253.
Maguire, D. (1973). Death by Choice. Garden City: Doubleday. Mynatt, C., & Sherman, S. J. (1975). Responsibility attribution in groups and
individuals: A direct test of the diffusion of responsibility hypothesis. Journal of Personality and Social Psychology, 32(6), 11 11 -1 118.
Nagi, M. H., & Lazerine, N. G. (1982). Death education and attitudes toward euthanasia and terminal illness. Death Education, 6( I), 1-1 5.
Parsons, T. (1951). The social system. Glencoe, 1L: Free Press. Parsons, T. (1975). The sick role and the role of the physician reconsidered.
Milbank Memorial Fund Quarterly f Health & Society, 53, 257-278. President’s Commission for the Study of Ethical Problems in Medicine and
Biomedical and Behavioral Research. (1982). Making health care deci- sions. Washington, DC: U.S. Government Printing Office.
President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. (1983). Deciding to forego life- sustaining treatment. Washington, DC: U.S. Government Printing Office.
Rachels, J. (1975). Active and passive euthanasia. New England Journal of Medicine, 292(2), 78-80.
Rachels, J . (1980). Euthanasia. In T. Regan (Ed.), Matters of life and death (pp. 28-66). Philadephia, PA: Temple University Press.
Ross, L. D. (1977). The intuitive psychologist and his shortcomings: Distor- tions in the attribution process. In L. Berkowitz (Ed.), Advances in exper- imental social psychology (Vol. 10, pp. 174-22 I) . New Y ork: Academic Press.

76 DAVID 6. SUGARMAN
Singh, B. K . (1979). Correlates of attitudes toward euthanasia. Social Biol- ogy, 26(3), 247-254.
Steininger, M., & Colsher, S. (1978-1979). Correlates of attitudes about “the right to die” among 1973 and 1976 high school and college students. Omega, Journal of Death and Dying, 9(4), 355-368.
Veatch, R . M . (1977). Case studies in medical ethics. Cambridge, MA: Har- vard University Press.
Wilson, J . B. (1975). Death by decision. Philadelphia, PA: Westminster Press.